
Opioid overdose: An opportune time to link individuals to treatment?
Rates of opioid-related overdose have increased in recent years. Active outreach to patients following an overdose might help to engage and retain individuals in treatment, which can ultimately help prevent further opioid-related overdose and fatality. The current study described initial outcomes of an assertive outreach method for opioid use disorder patients who had a recent nonfatal overdose, revealing its potential for enhancing treatment engagement and retention.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Opioid-related overdose rates have substantially increased in recent years. In the U.S., opioids were involved in about 450,000 deaths between 1999 to 2018 and emergency department visits for nonfatal opioid overdose events increased 30% from 2016 to 2017. Nonfatal opioid overdose is a key predictor of subsequent overdose events, and multiple non-fatal overdoses are linked to increased risk of a future fatal overdose. As the number of individuals presenting to the emergency department for nonfatal opioid overdose rises, opportunities present for intervention and treatment. According to cognitive motivation theories, nonfatal overdose might enhance a patient’s readiness for change because major life events are thought to enhance motivation for changing unhealthy behaviors. Medications like buprenorphine, methadone, and naltrexone are first line treatments for opioid use disorder, often combined with behavioral therapies, and can help prevent repeated overdose. However, relatively few individuals actively seek out treatment after an overdose and new interventions are needed to boost motivation for and engagement in opioid use disorder treatment. The current study tested an assertive outreach method for identifying opioid use disorder patients with a recent nonfatal overdose event, and described individuals’ treatment engagement and retention after receiving outreach.
HOW WAS THIS STUDY CONDUCTED?
The authors conducted a pilot study of a novel intervention for facilitating outreach, and described primary outcomes of treatment engagement and retention 30 and 90 days after enrollment among a single group of non-fatal opioid overdose patients. Participants were recruited from two emergency medical departments in Texas, including the Memorial Hermann Hospital’s emergency department, and the Houston Fire Department’s emergency medical services agency. Following the overdose event, patients rated their readiness (on a scale ranging from one to 10) to change (i.e., readiness to start an opioid use disorder treatment and recovery program) and were added to a surveillance system. Individuals rating their readiness as three or higher were eligible to participate. Of the 251 individuals added to the surveillance system, 103 were located and received a next-day home-based outreach visit. The outreach team included a peer recovery coach and a licensed paramedic. Motivational interviewing was used during home-based visits to inform and motivate patients’ readiness for treatment; interview topics addressed substance use history, the most recent overdose, and options for treatment and recovery. Ultimately, 34 individuals were receptive to outreach, eligible to participate, and enrolled in the study.
Patients who agreed to participate in the treatment program (1) completed a baseline medical assessment to confirm opioid use disorder diagnosis, (2) underwent rapid induction (i.e., starting the patient on medication and finding the patient’s ideal daily dose over the course of a few days) of buprenorphine (e.g., Suboxone, Subutex) with an emergency medicine doctor within ~24 hours of enrolling in the study, and (3) enrolled in a more permanent outpatient medication treatment clinic by a social worker. Although treatment started with buprenorphine, participants were able to switch to methadone or naltrexone (e.g., Vivitrol) at the discretion of their outpatient clinic. Throughout the study, participants were offered three optional counseling sessions per week, including individual meetings with an addiction counselor, group meetings with a peer recovery coach, and science-based opioid use disorder educational groups. Peer recovery specialists and social workers actively linked participants to free/stable housing, employment, and health insurance if needed.
All services provided as part of the study were free to participants. Participation in the program was evaluated via self-report questionnaires and program attendance records. Follow-up telephone calls were made at least weekly, and primary outcomes were assessed 30- and 90-days post study enrollment. Enrolled participants were all non-incarcerated English-speaking adults (average age: 38 years), who had misused opioids within the past 30 days, experienced a recent overdose, and were not already enrolled in opioid use disorder treatment. The majority of participants were white (62%) homeless (77%) men (56%) without health insurance (79%), who primarily used heroin (59%) and reported a high level of readiness for treatment (~9.6 out of 10).
WHAT DID THIS STUDY FIND?
Only a minority of those approached enrolled in treatment.
Of the individuals who completed an outreach visit (n = 103), 33% expressed interest in starting the treatment program and were enrolled. The majority of participants who did not enroll in the program chose not to participate because they denied having an opioid use problem (n = 50).
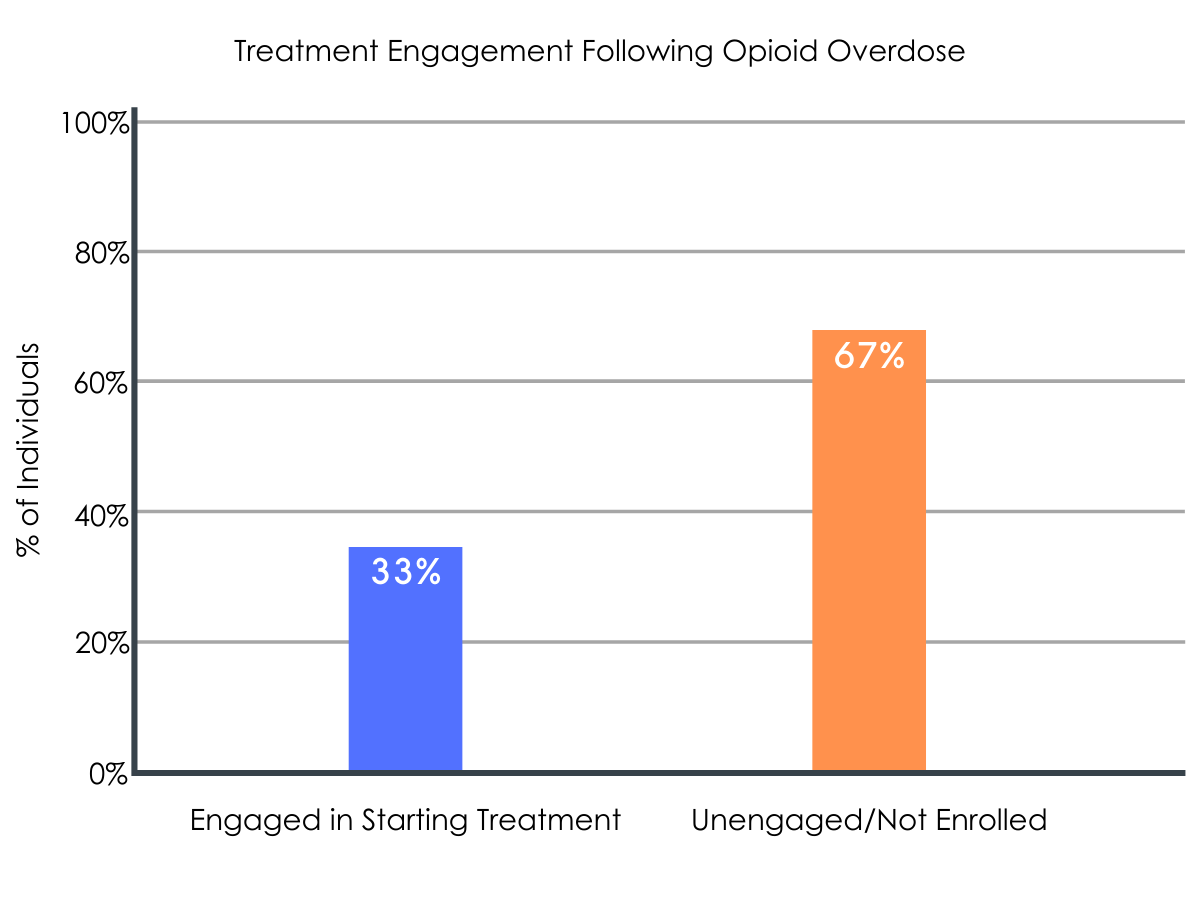
Figure 1.
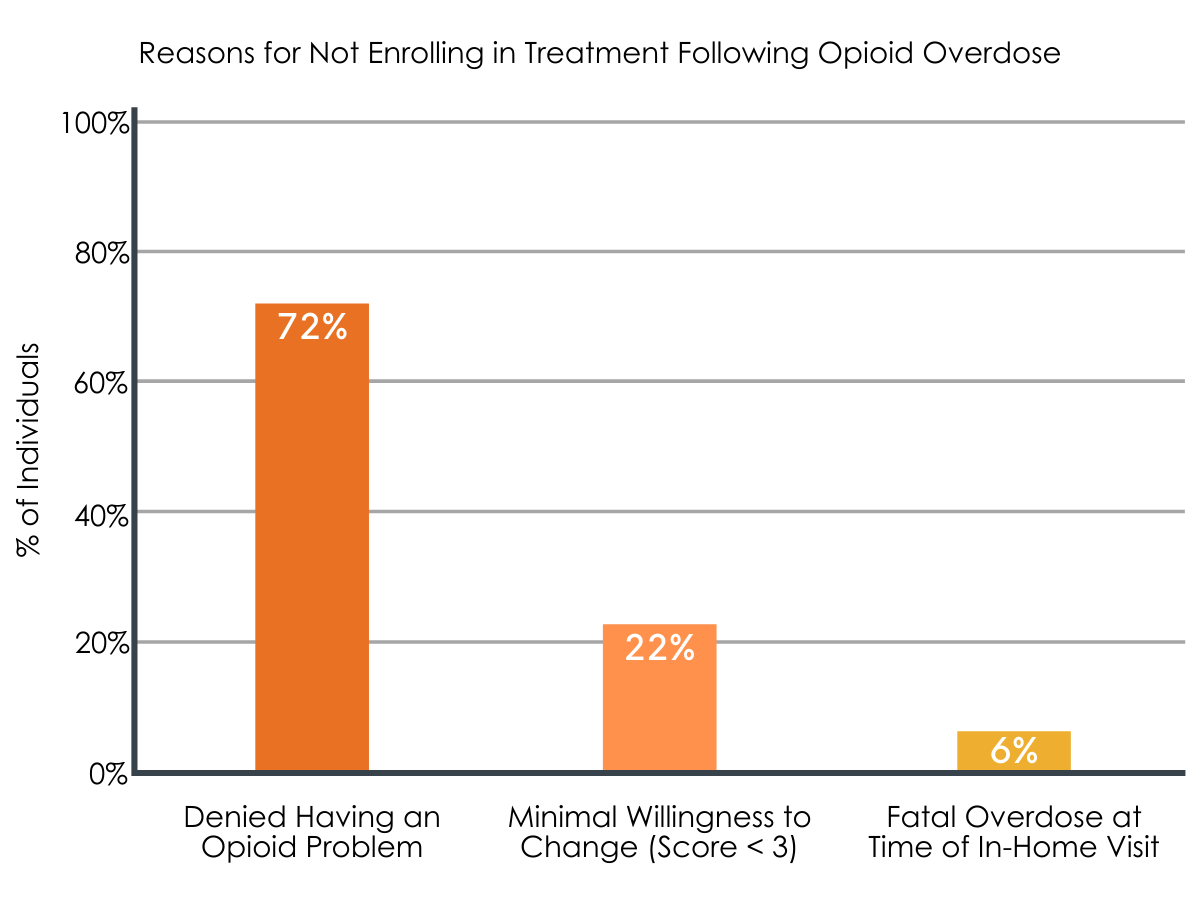
Figure 2.
Treatment engagement decreased over time.
Of the 34 individuals who enrolled in the treatment program, 30 patients were still actively engaged in treatment at the 30-day follow-up, and 19 patients remained engaged at the 90-day follow-up.
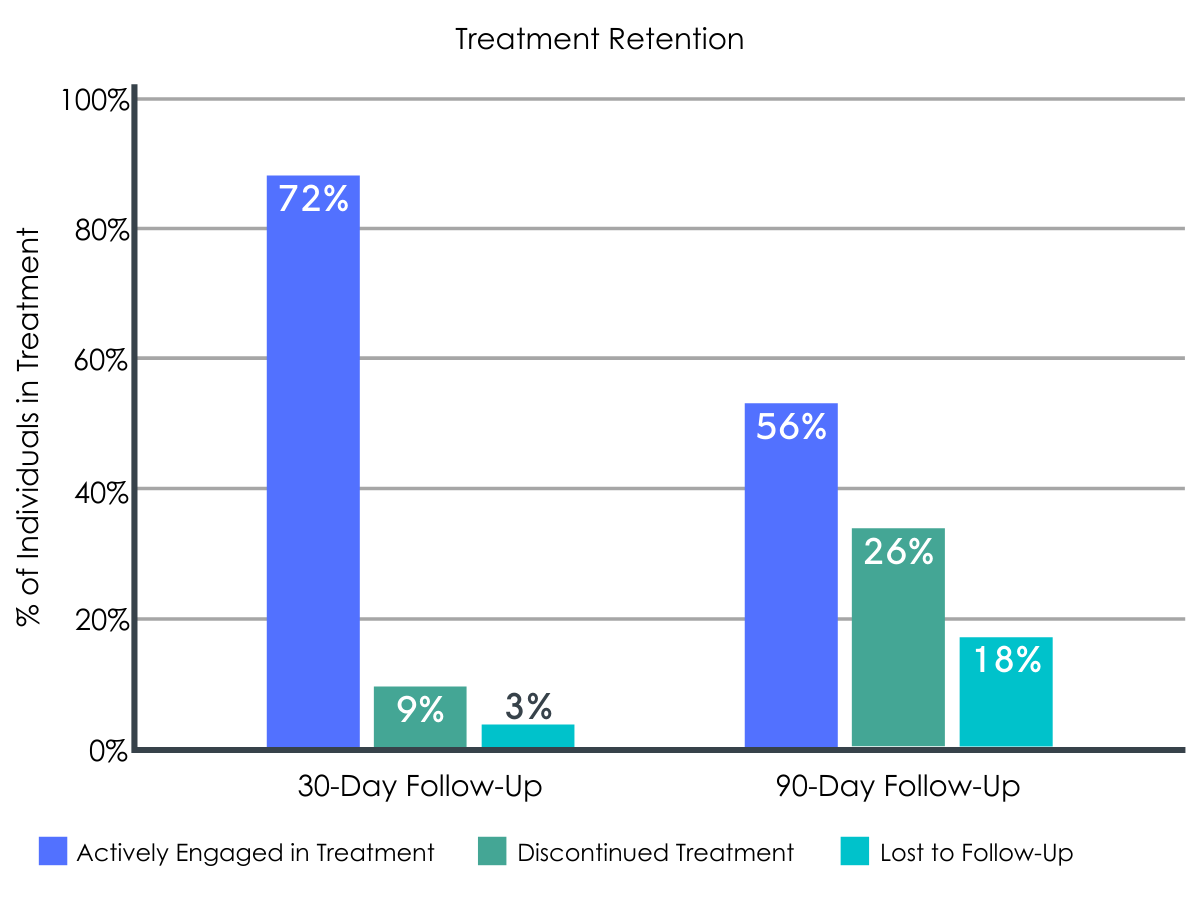
Figure 3.
Descriptive opioid outcomes were encouraging.
Among actively engaged participants, no subsequent nonfatal or fatal overdoses occurred over the 90-day study period. Additionally, only three participants were identified as having a momentary opioid relapse.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Opioid use disorder medication treatment is shown to significantly reduce overdose risk, but getting patients engaged in medication treatment can prove difficult. This study suggests that assertive outreach interventions may be promising strategies for boosting treatment engagement and retention among non-fatal opioid overdose patients.
Although the engagement rate was low (1/3 enrolled), this study suggests active outreach may help engage individuals in treatment who are highly motivated for change, but who otherwise might not do so. Among those who decided to enroll in the study, willingness to start a treatment and recovery program was very high (on average, 9/10). Although motivation was high, it can quickly diminish, so providing an outreach intervention like this one can ultimately facilitate treatment access and allow individuals to more readily take advantage of a “reachable moment”. Importantly, a large proportion of individuals who were given the opportunity for treatment, but decided not to participate, reportedly denied having an opioid problem, suggesting that assertive outreach, even when systematic and using motivational interviewing approaches, may not be sufficient for immediately engaging those who are not yet ready for change. While somewhat counterintuitive, more directive approaches, when delivered empathically, may be better at linking individuals to recovery support – future studies should investigate the effectiveness of directive-empathic linkages relative to motivational-reflective linkages. Nonetheless, individuals who refused treatment in this study were not followed up over time, and it is therefore unclear whether or not the intervention had a delayed effect on treatment seeking. Additional research is needed to see if interventions like this one facilitate awareness around the idea of treatment and later affect motivation to change and/or seek treatment among those who initially decide against it.
The majority of participants were still engaged in treatment at the 30-day follow-up, suggesting that patients generally recognized the benefits of the program. However, 90-day follow-up revealed that only about one-half of patients remained active in treatment. Although these treatment retention rates are generally consistent with outcomes of prior studies, research suggests that mortality rates are nine times higher during the first four weeks after discontinuing opioid use disorder medication treatment, and two times higher thereafter. Furthermore, less than six months of medication treatment can increase risk of relapse, increase use of serious opioid-related acute care and risk of overdose after discontinuation. In support of this prior research, the current study found low rates of relapse and overdose among those who were actively engaged and remained in treatment. Therefore, educating patients about the risks of treatment drop out and developing intervention techniques for continued care may be important for ongoing engagement and long-term recovery. Continuing care may be particularly important for those experiencing homelessness, a cohort making up the majority of the current study’s sample. Homelessness is shown to increase risk of overall mortality and to increase risk of opioid-specific fatal overdose. Providing additional treatment and recovery resources that assist individuals with obtaining insurance, housing, and employment might help to support this vulnerable population. For example, recovery housing is shown to benefit the substance use outcomes of homeless populations.
Given the relationship between nonfatal overdose events and subsequent overdose fatalities, as well as the limited number of individuals who actively seek treatment on their own after an overdose, intensive multidimensional interventions like this one are necessary to ultimately reduce opioid overdose rates and successfully address the opioid epidemic. Thankfully, a larger body of research has started to emerge, aimed at developing and testing ways to capitalize on patient motivation after a drug related harm or consequence.
- LIMITATIONS
-
- Although the surveillance system used to identify individuals who experienced an overdose in this study offers a convenient method of outreach, a significant proportion of individuals could not be reached due to a transient lifestyle. Fifty-nine percent of the individuals in this surveillance system had invalid addresses or could not be located, suggesting that outreach inside the emergency department, prior to discharge, might present an ideal time for conducting outreach among more transient populations.
- The sample size was relatively small and there was no comparison group. Understanding the effects of this intervention above and beyond the effects of individual motivation and the overdose event itself is essential for determining the true effectiveness of assertive outreach, and calls for controlled clinical trials. Furthermore, the authors did not report the number of individuals that ultimately switched from buprenorphine to methadone or naltrexone. Examining the influence of medication type is essential for interpreting treatment retention and requires further study in the context of this intervention.
- Relapse was assessed using weekly reports from recovery coaches. However, patients may not have disclosed relapse to recovery coaches and these rates might therefore be lower than actual relapse rates. Furthermore, the authors did not detail the participant’s outpatient clinics, which may or may not require abstinence as part of their program regulations. Given that overdose rates were only assessed for those who were still engaged in treatment at follow-up, overdose rates may be higher when considering those who dropped out of treatment or were lost to follow-up. Additional research is needed to see if this intensive intervention affects overdose and relapse rates controlling for these factors.
BOTTOM LINE
- For individuals and families seeking recovery: This study suggests that intensive outreach after opioid overdose may be a promising strategy to engage and retain individuals in medication treatment programs. Interventions like if proven effective, could be important for addressing the opioid epidemic. Overdose events increase risk of a future fatal overdose, but opioid use disorder medication treatment (e.g., buprenorphine) can help to prevent these overdoses. Nonetheless, engaging patients in treatment can be difficult when left to their own devices and individuals might experience barriers to treatment access. Given that individuals may be more willing to start treatment after an overdose, starting access to buprenorphine treatment more immediately in the emergency department (ED) or providing active outreach and linkage to treatment at the time of overdose after leaving the ED can ultimately help motivate individuals to begin their path to recovery. Although additional research is needed to determine if this intervention benefits treatment engagement and retention compared to less intensive interventions (or no intervention), it is unlikely that such interventions are detrimental to overdose patients who are at increased risk for fatal overdose. Development of novel interventions for overdose patients will ultimately help guide the best approaches to reduce overdose and related deaths.
- For treatment professionals and treatment systems: This pilot study suggests that intensive outreach and linkage to treatment/recovery services after an opioid overdose event may be a promising method to engage and retain individuals in medication treatment programs. It is well known that opioid use disorder medication treatment (e.g., buprenorphine) can help to prevent opioid overdose, but engaging patients in treatment can be difficult, particularly among those who experience increased barriers to treatment access. Cognitive motivation theories suggest that non-fatal overdose might enhance a patient’s willingness to change maladaptive behaviors (i.e., it is a “reachable moment” where people are more receptive to messages about positive health behavior change). Therefore, active outreach and linkage to treatment at the time of overdose can ultimately help motivate treatment engagement and retention. Given the small sample size and lack of a control group in this study, additional research is needed to determine whether or not assertive interventions like this one can significantly benefit treatment engagement and retention relative to less intensive interventions, or no intervention. However, it is unlikely that such interventions are detrimental to overdose patients who are at increased risk for fatal overdose. Development of novel interventions for overdose patients will ultimately help guide the best approaches to reduce opioid overdose and related deaths.
- For scientists: This preliminary non-randomized pilot study suggests that intensive outreach and linkage to treatment/recovery services following an opioid overdose event may be a useful mechanism for engaging and retaining individuals in medication treatment programs, to ultimately reduce risk of recurrent overdose. Given the role of pharmacotherapy in reducing opioid overdose risk, as well as the difficulty of engaging patients in medication treatment programs, randomized controlled trials, or quasi-experiments with one or more comparison conditions, are needed to determine whether or not assertive interventions like this one can significantly benefit treatment engagement and retention relative to less intensive interventions, or no intervention. Identifying the influence of medication type (buprenorphine vs. methadone vs. naltrexone), sociodemographic factors, and comorbid disorders on assertive outreach effectiveness is also essential for determining the best approaches in different overdose populations. Development of novel interventions and comprehensive treatment programs for overdose patients that support mental/physical health and psychosocial wellbeing can ultimately help reduce opioid-related morbidity and mortality.
- For policy makers: Studies like this help us to identify novel interventions for linking opioid use disorder patients to treatment, which can ultimately help reduce overdose and related deaths. Opioid-related overdose has become a substantial problem around the world. Although opioid use disorder medications (e.g., buprenorphine, methadone) are effective at reducing overdose risk, relatively few individuals actively seek out treatment after an overdose event. Therefore, timely and intensive interventions like this one, are important and potentially lifesaving. Utilizing patient motivation after an overdose event, the authors found that assertive intervention may be a promising strategy to engage and retain patients in treatment. Additional funding for randomized controlled trials will help to disentangle the effects of assertive outreach, independent of patient motivation or likelihood of treatment seeking pre-intervention, and can ultimately help address the opioid overdose epidemic by offering novel intervention techniques that enhance treatment seeking, engagement, and retention to reduce opioid-related morbidity and mortality.
CITATIONS
Langabeer, J., Champagne-Langabeer, T., Luber, S. D., Prater, S. J., Stotts, A., Kirages, K., … & Chambers, K. A. (2020). Outreach to people who survive opioid overdose: Linkage and retention in treatment. Journal of Substance Abuse Treatment, 111, 11-15. doi: 10.1016/j.jsat.2019.12.008
