A recovery framework to measure addiction medication outcomes
For individuals with opioid use disorder, FDA approved medications reduce opioid use and overdose risk. Outcomes beyond substance use in medication research – quality of life and reduction of psychological symptoms, for example – can help inform treatment and public health messaging and recommendations. This study compared effects of extended-release, injectable naltrexone to daily, oral buprenorphine on life satisfaction.
There is substantial research showing that opioid use disorder medications reduce opioid use, overdose risk, and overdose mortality. While opioid use is associated with other functional outcomes, studies that specifically include outcomes beyond substance use–quality of life, reduction of psychological symptoms, or social determinants of health, for example–can help inform treatment and public health messaging and recommendations. At the same time, researchers have not yet reached agreement on what measures other than reduced substance use best capture recovery progress and on what time scale, although a growing consensus favors some combination of standardized measures and patient centered outcomes.
Life satisfaction provides one potential way to measure a general sense of well-being in recovery. Life satisfaction has been defined as the degree to which people evaluate the overall quality of life based on the factors that matter most to them. Although not specific to a particular time or domain of life, life satisfaction is associated with positive health outcomes such as longer life expectancy, better disease tolerance, and fewer mental disorders. Low self-reported life satisfaction is associated with higher risk of suicide, among other negative health outcomes.
Individuals with opioid use disorder seeking treatment have a low life satisfaction compared to the general population. There is relatively little research on opioid use disorder medications, such as naltrexone, methadone, and buprenorphine, and life satisfaction. One study suggests that higher life satisfaction is associated with increased likelihood of prolonged abstinence among individuals with substance dependence. Another short-term 3-month trial showed an increase in life satisfaction among individuals treated with buprenorphine compared to the control group. However, participants emphasized that their lives were still not good, only somewhat better than before. This study conducted in Norway employs a measure of life satisfaction in comparing extended-release (injectable) naltrexone (also known by the brand name Vivitrol) to daily, oral buprenorphine (also known by the brand name Suboxone) in treating opioid use disorder.
HOW WAS THIS STUDY CONDUCTED?
This paper presents secondary outcomes from a trial conducted in Norway from November 2012 to July 2016 that compared monthly, injectable (XR) naltrexone to daily sublingual buprenorphine-naltrexone for the treatment of opioid use disorder. An earlier paper by the researchers reported that the trial found XR-naltrexone was equally effective as buprenorphine-naltrexone in terms of retention and abstinence from illicit opioids during a 12-week trial. An earlier secondary analysis of the same data found that XR naltrexone was more effective than buprenorphine-naltrexone in preventing relapses -defined as 4 consecutive weeks when any opioid (other than buprenorphine) was used or 7 consecutive days when any opioid (other than buprenorphine).
The first stage of this study was a 12-week, randomized control “open label” trial (“open label” means that participants knew which medication they were taking). Upon qualifying for the study, patients completed medically supervised withdrawal (i.e., detoxification) if necessary and were randomized to one of two treatment conditions. After 12 weeks, participants were given the choice of whether to continue on the medication that they were randomized to or switch to the other medication. By this point in the study, all but five participants in the buprenorphine group either dropped out or decided to switch to XR naltrexone. No participants switched from XR naltrexone to buprenorphine. As a result, the study researchers adapted their design for the second phase of the trial and compared the group that switched to naltrexone (“switchers”) to the group that continued naltrexone (“continuers”) for the remaining 26 weeks of the trial.
The researchers measured life satisfaction using the section from the Temporary Satisfaction with Life Scale that evaluates life satisfaction in the present. They administered the survey at the start of the study (“baseline”) and every four weeks through both the 12-week randomized, control trial and the 36-week comparison study. The researchers used the European Addiction Severity Index to assess the number of days that participants used illicit opioids, satisfaction with civil status, satisfaction with living arrangements, and satisfaction with leisure time.
The researchers created statistical models to estimate the strength of the association between 1) life satisfaction and opioid use (adjusted for age and gender); 2) between life satisfaction and satisfaction with living arrangements, civil status, and leisure time; and 3) life satisfaction and years of opioid use. They used another type of statistical model to evaluate whether there were well-defined sub-groups within the study population that followed distinct life satisfaction trajectories.
The study was open to men and women 18 to 60 years of age who met DSM IV criteria of opioid dependence. People were excluded from participation if they met the criteria for DSM IV alcohol dependence, were pregnant or breast-feeding, or met the criteria for a serious mental or somatic illness that could interfere with study participation. Men represented 73 percent of the study participants and the average age was 36.1 years old. On average, participants had been using illicit opioids for 7.6 years.
WHAT DID THIS STUDY FIND?
Receiving XR naltrexone associated with more life satisfaction.
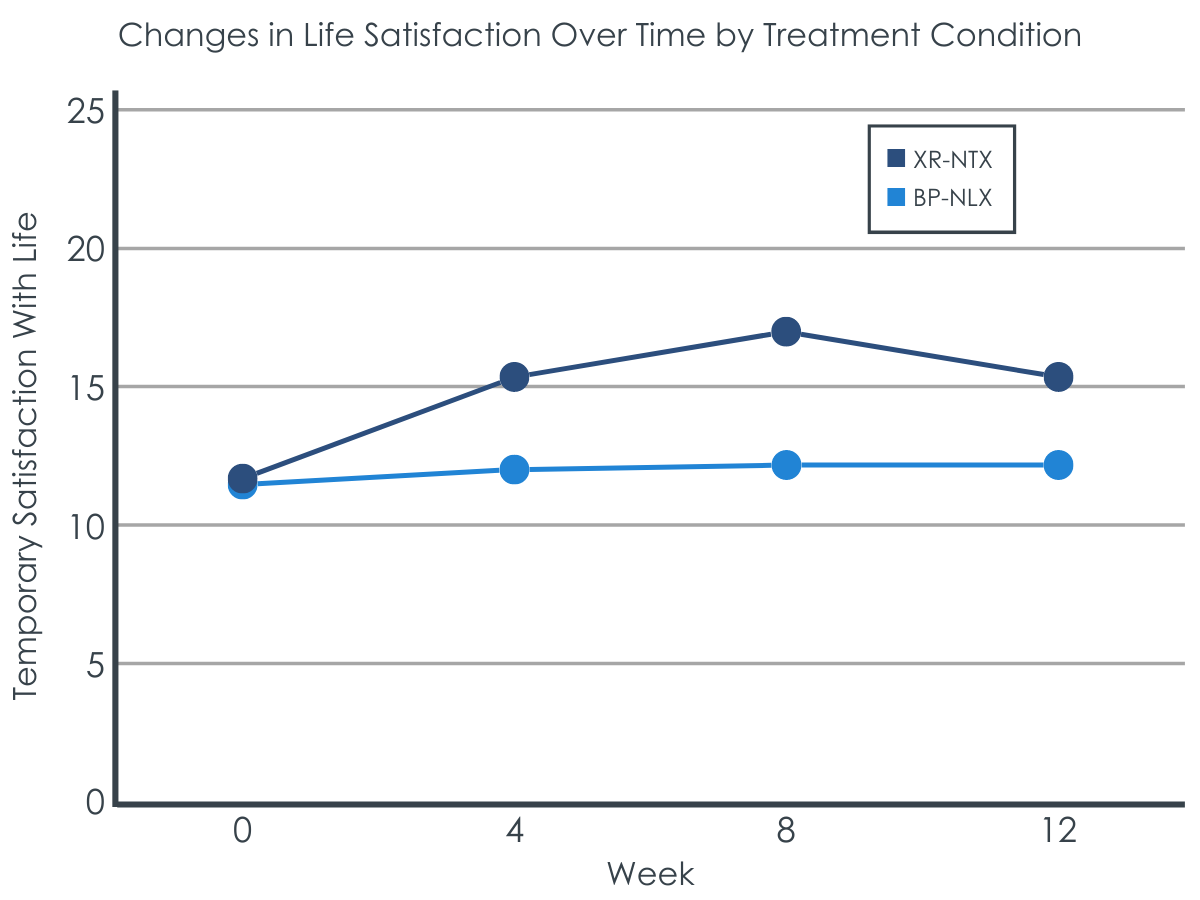
At baseline, both groups had similar life satisfaction scores. At weeks 4 and 8, the life satisfaction score of the XR naltrexone group increased more than the buprenorphine group. The two groups were similar by the end of the 12-week treatment period.
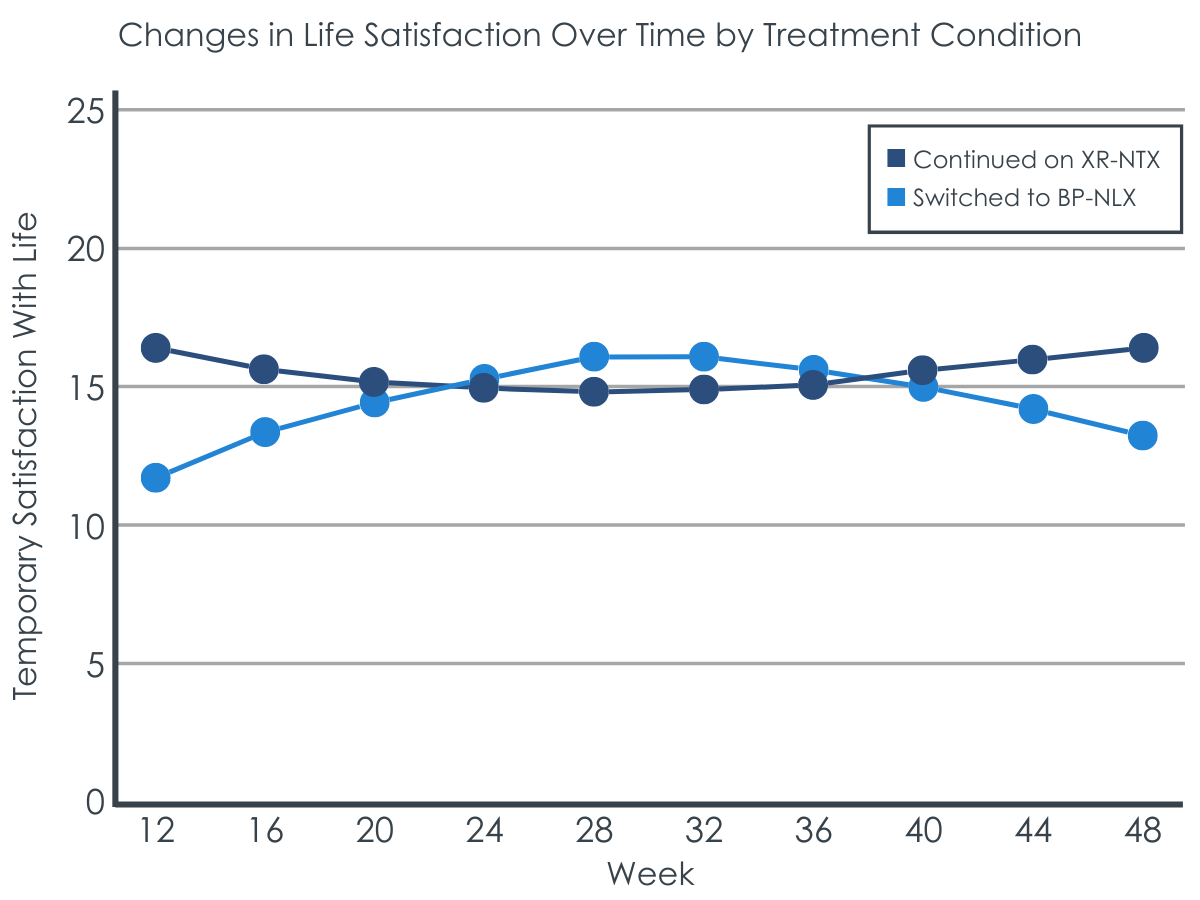
During the 32-week follow-up, the group that switched from buprenorphine to XR naltrexone had a greater increase in life satisfaction than those who continued on XR naltrexone. Throughout this follow-up period, though, those continuing on XR naltrexone had either better or similar life satisfaction compared to those who switched onto XR naltrexone. This suggests those randomly assigned to buprenorphine during the initial treatment phase were not doing as well on life satisfaction but were able to somewhat catch up to those assigned to XR naltrexone and continued on that medication during follow-up.
More opioid use was associated with lower life satisfaction.
During the 12-week trial, frequent use of opioids (more than 20 days a month) was associated with lower life satisfaction scores across all participants, whether they received buprenorphine or XR naltrexone. However, at week 12, life satisfaction was similar for all participants, regardless of the number of times they used each month. In other words, people who were not using opioids or only used opioids a few days a month showed a small increase in life satisfaction from baseline to week 12, while people who used frequently had lower life satisfaction scores most weeks during the trial, but similar life satisfaction scores to other participants at week 12.
Participants starting out low on life satisfaction increased slightly at first, but changed little thereafter.
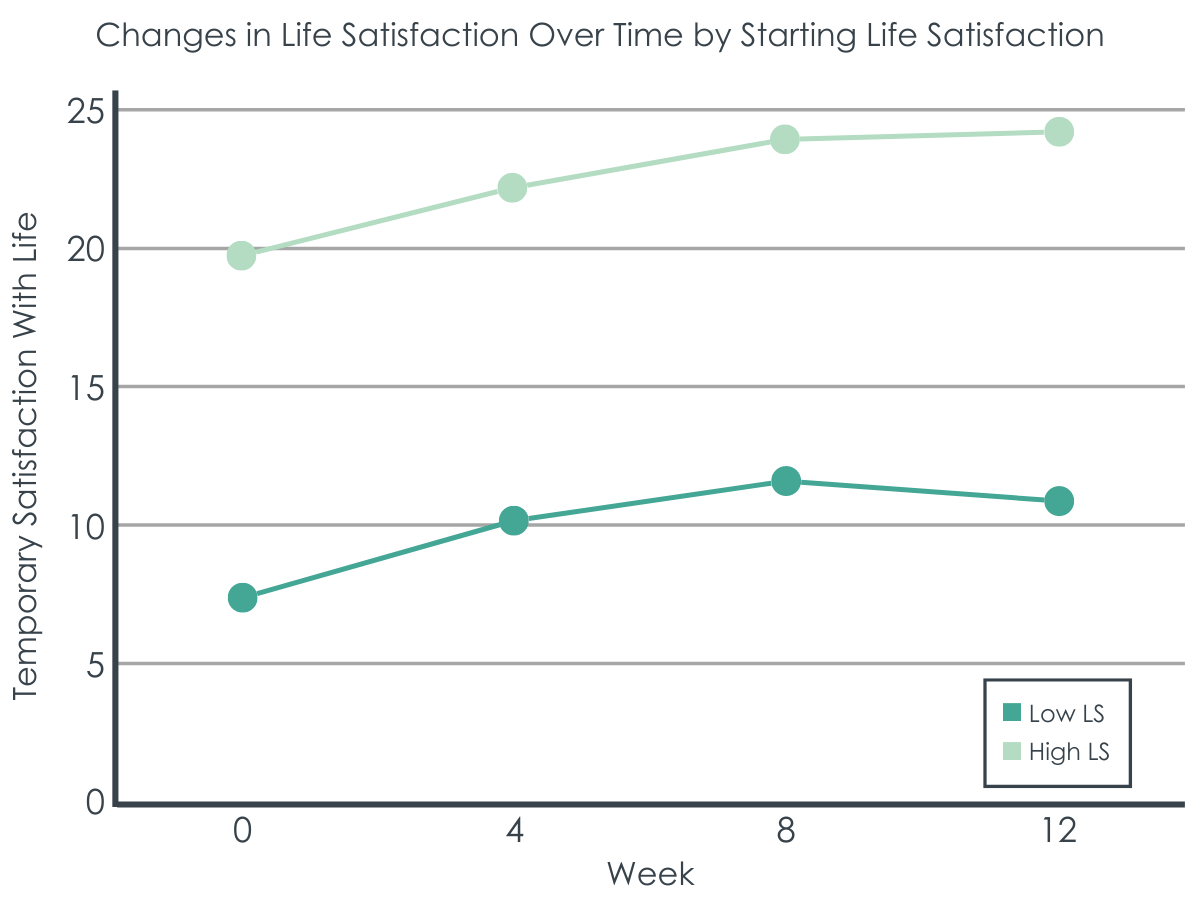
During the initial 12-week treatment phase, across all participants irrespective of which medication they received, the low life satisfaction group increased slightly at first then levelled off. The high life satisfaction group started out higher but changed very little during treatment. More opioid use was related to being in the lower satisfaction group, while those who were “indifferent” to their satisfaction with leisure time were more likely to be in the high satisfaction group compared to those who were “not satisfied” with their leisure time.
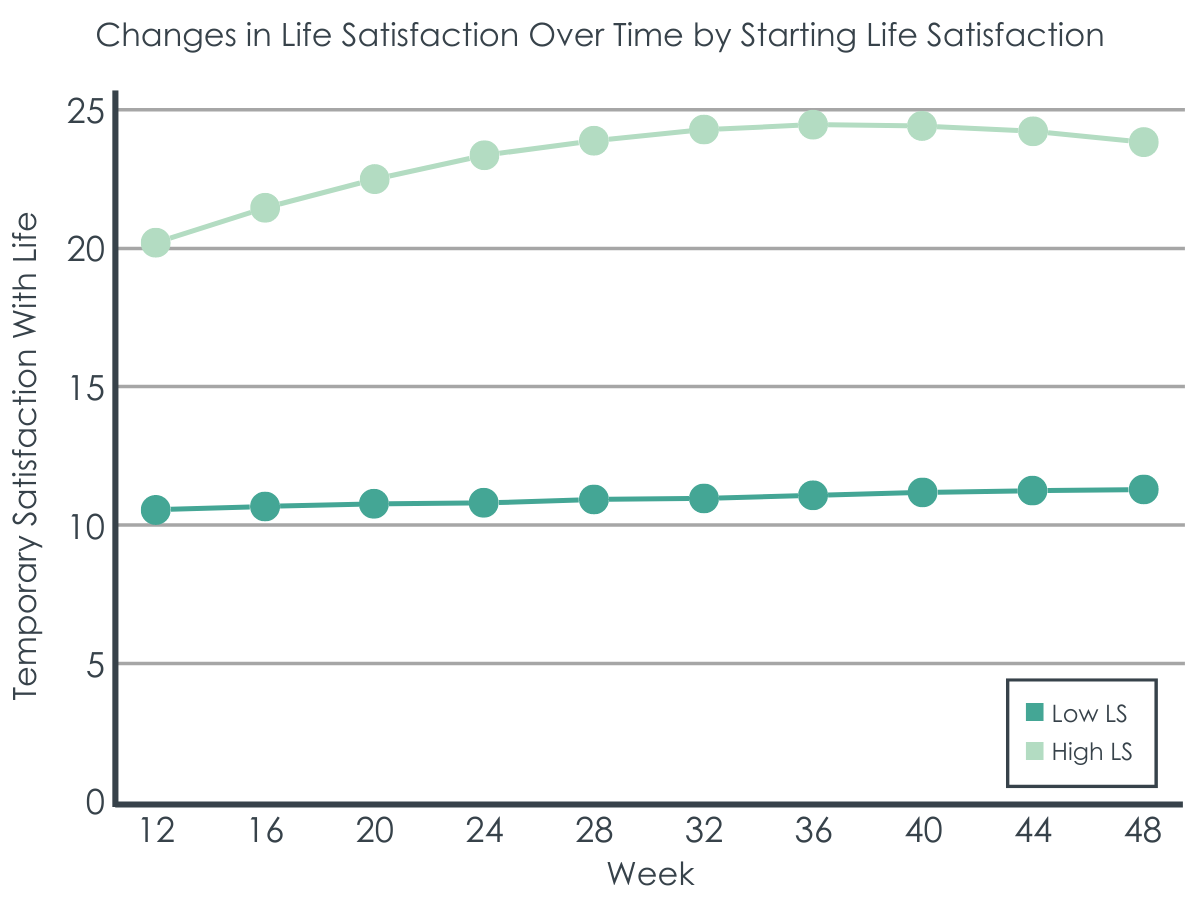
During the 32-week follow-up, again across all participants, those starting out higher on life satisfaction at the beginning of this follow-up period improved slightly over time. The group lower in life satisfaction did not improve at all during the follow-up period, however. Satisfaction with leisure time was the only factor that differed between the two groups, as above, such that those “indifferent” to their satisfaction with leisure time were more likely to be in the high satisfaction group compared to those “not satisfied.”
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This secondary analysis of a randomized controlled trial showed that participants receiving XR naltrexone generally had higher life satisfaction than those receiving buprenorphine. In a non-randomized follow-up where individuals could choose to switch medications if they wished, switching from buprenorphine to XR naltrexone helped these individuals catch up somewhat on life satisfaction, though being assigned to XR naltrexone and continuing on the medication still produced the highest levels of life satisfaction.
The study design may have accounted for the life satisfaction advantage for XR naltrexone, rather than the medication itself. Buprenorphine is widely available in Norway (the location of the study) and most participants in the trial appear to have signed up for the study as they were motivated to receive XR-naltrexone. It is possible that the lower improved life satisfaction of the buprenorphine group may have reflected that they received a treatment that they preferred less and/or the group that received XR naltrexone was more motivated and/or happier because they received their preferred treatment. Additionally, for buprenorphine participants, lower life satisfaction was associated with ranking satisfaction with leisure time as “low.” Given that participation in the buprenorphine-naltrexone arm required a daily clinic visit (whereas XR naltrexone does not), this requirement may have interfered with leisure activities, influencing this result. Future studies should compare identical modalities (i.e. XR naltrexone to XR Buprenorphine) and adopt a study design that guards against the possibility that outcomes such as lower life satisfaction reflect the patient’s randomization to a less-preferred medication.
Another important feature of the study design that may have contributed to this outcome was that participants currently taking opioids were required to undergo a medically supervised detox before they began treatment. Extended-release injectable naltrexone can be difficult to initiate because it requires a period of complete abstinence before treatment can start (to prevent inducing opioid withdrawal once naltrexone is started). In a prior study, only about 72% of patients randomly assigned to extended-release naltrexone successfully started it (vs. ~94% assigned to buprenorphine), presumably because of this difficulty of maintaining abstinence from opioids prior to beginning it. Consistently, about 37% of participants assigned to the naltrexone group in the current study failed to initiate this medication. This fact suggests that the XR naltrexone group may have been unusual in that they were highly motivated with abstinence as their desired goal. The greater increase in life satisfaction for the XR naltrexone group, therefore, may not generalize to less highly motivated groups or to groups with opioid use goals other than abstinence.
Previous research has established that buprenorphine has advantages compared to XR naltrexone for some crucial outcomes. When patients discontinue extended-release injectable naltrexone they have a reduced tolerance to opioids, and this puts them at greater risk of overdose should they return to opioid use at high enough doses, such as those used prior to treatment. Discontinuation of medication treatment also can occur more frequently with extended-release injectable naltrexone than buprenorphine. Buprenorphine is a partial opioid agonist and, as an agonist, it allows a patient to maintain a certain degree of opioid tolerance. Thus, a return to opioid use upon discontinuing buprenorphine treatment offers significantly greater protection from fatal overdose.
In terms of life satisfaction, the study population was divided into two trajectories (a higher and lower life satisfaction group), although the overall life satisfaction of both groups was quite modest. Most participants fell into the low life satisfaction group and, although this group showed some improvement in the first (randomized) phase of the study, this group remained stable with low life satisfaction during the second part of the study. In both phases, the high life satisfaction group saw a small amount of improvement, however this improvement levelled off toward the end of phase 2. The strongest predicators of belonging to the low life satisfaction group were higher frequency of opioid use and lower satisfaction with leisure time.
At the same time, it is important to note that this study saw high dropout rates for participants (only 58 of 159 participants completed the study), which impedes generalization of study findings. Further research is needed to explore whether these associations hold across different populations and, if so, the direction of influence (for example, whether lower life satisfaction leads to more opioid use, or more opioid use leads to lower life satisfaction, or some kind of bidirectional relationship exists between the two).
The fact that life satisfaction remained low for the majority of participants is concerning. However, it also raises the question of whether the life satisfaction measure is in fact capturing the relevant dynamics of change in the first year of recovery and whether 1 year is a sufficient time frame to capture increases in life satisfaction. Other measures, for example recovery capital, may well provide better indicators of a successful recovery trajectory. One study, based on a nationally representative sample of U.S. adults in recovery, suggests that quality of life, happiness, and self-esteem decrease during the initial months of recovery after initial stabilization before beginning to increase between 6 to 12 months after problem resolution. This dynamic is followed by steep increases in well-being over 6 years, followed by a more gradual increase afterwards. Notably, people with opioid use disorders are among the groups (along with women, certain racial/ethnic minorities, and people who use stimulants) that begin their recovery journey with less resources than other groups and experience more persistent problems with psychological distress in the first 3 years of recovery. Before the 1-year mark, life satisfaction measures may reflect an expected decrease in quality of life, happiness, and self-esteem as people begin to take stock of the challenges that lie ahead in recovery before these indices begin to improve towards or after the 1-year mark. Researchers may need to evaluate psychosocial outcomes on scales longer than 1 year in order to determine which measures accurately capture the longitudinal bigger picture improvements in well-being characteristic of long-term recovery.
Buprenorphine is widely available in Norway (the location of the study) and most participants in the trial appear to have been motivated to receive XR-naltrexone. It is possible that the lower improved life satisfaction of the buprenorphine group may have reflected the fact that they received a less preferred treatment.
Among this study population, lower life satisfaction was associated with ranking satisfaction with leisure time as “low.” Given that participation in the buprenorphine arm required a daily clinic visit (whereas injectable naltrexone does not), this requirement may have interfered with leisure activities, influencing the lower life satisfaction score.
There was substantial drop out over the course of the study (only 58 of 159 participants completed the study). Given the small sample size, these results cannot be generalized to other populations without further research.
BOTTOM LINE
This two-phase study found that XR (injectable) naltrexone was equal, and at some points superior, to daily, oral buprenorphine-naltrexone in terms of improvements in participant life satisfaction over one year. However, the life satisfaction of the majority of participants, even those with higher life satisfaction at the start and who showed the most improvement, remained low throughout the study period. Future research should continue to explore what patient reported outcomes best capture improvements across different phases of recovery while recognizing that the first year of recovery is likely variable and may not be indicative of later trends in recovery progress regarding life satisfaction.
For individuals and families seeking recovery: njectable, extended release (XR) naltrexone is 1 of 3 FDA approved medications for OUD (the other two being buprenorphine and methadone). This study compares XR naltrexone with daily, oral buprenorphine. It found that XR naltrexone is as effective as buprenorphine, and at some points it was more effective, in improving the life satisfaction of people with opioid use disorder. The same researchers previously published two articles that showed XR naltrexone was as effective as buprenorphine in terms of days abstinent from opioids, retention on the medication, and preventing relapse. These and other studies indicate that XR naltrexone is an effective treatment option for OUD. At the same time, the results should be balanced against studies that establish buprenorphine is superior in important measures, including reducing overdose risk and mortality. It is also important to note that extended-release injectable naltrexone can be difficult to initiate because it requires a period of complete abstinence before treatment can start (to prevent inducing opioid withdrawal once naltrexone is started). People in recovery from OUD and their families should talk through the benefits and drawbacks of all three medications with a qualified prescriber.
For treatment professionals and treatment systems: Injectable, extended release (XR) naltrexone is 1 of 3 FDA approved medications for OUD (the other two being buprenorphine and methadone). This study compares XR naltrexone with daily, oral buprenorphine. It found that XR naltrexone is as effective as buprenorphine, and at some points it was more effective, in improving the life satisfaction of people with opioid use disorder. The same researchers previously published two articles that showed XR naltrexone was as effective as buprenorphine in terms of days abstinent from opioids, retention on the medication, and preventing relapse. These and other studies indicate that XR naltrexone is an effective treatment option for OUD. At the same, the results should be balanced against studies that establish buprenorphine is superior in important measures, including reducing overdose risk and mortality. It is also important to note that extended-release injectable naltrexone can be difficult to initiate because it requires a period of complete abstinence before treatment can start (to prevent inducing opioid withdrawal once naltrexone is started). Treatment professionals should familiarize themselves with the current evidence regarding buprenorphine, methadone, and XR naltrexone and qualified prescribers should advise individuals in recovery and their families about the benefits and potential drawbacks of each medication.
For scientists:This two-phase study found that XR (injectable) naltrexone was not inferior, and at some points superior, to daily, oral buprenorphine-naltrexone in terms of improvements in participant life satisfaction over 48 months. However, the experience of these researchers suggests some lessons for future study design. Buprenorphine is widely available in Norway (the location of the study) and most participants in the trial may have been more motivated to receive XR-naltrexone compared to patients in general treatment settings. It is possible that members of the buprenorphine-naltrexone group may have received a treatment they preferred less. Additionally, among this population, lower life satisfaction was associated with ranking satisfaction with leisure time as “low.” Given that participation in the buprenorphine arm required a daily clinic visit (whereas injectable naltrexone did not), this requirement may have interfered with leisure activities, possibly influencing the result. Future studies should compare identical modalities (i.e., XR naltrexone to XR buprenorphine) and adopt a design that guards against the possibility that outcomes such as lower life satisfaction reflects a patient’s randomization to a less-preferred medication. Researchers may need to evaluate psychosocial outcomes on scales longer than 1 year in order to determine which measures in particular accurately capture the longitudinal improvements in well-being characteristic of long-term recovery.
For policy makers: Injectable, extended release (XR) naltrexone is 1 of 3 FDA approved medications for OUD (the other two being buprenorphine and methadone). This study compares XR naltrexone with daily, oral buprenorphine. It found that XR naltrexone is as effective as buprenorphine, and at some points it was more effective, in improving the life satisfaction of people with opioid use disorder. The same researchers previously published a 12-week study that showed XR naltrexone was also as effective as buprenorphine in terms of days abstinent from opioids and retention on medication. These and other studies indicate that XR naltrexone is an effective treatment option for OUD. At the same, the results should be balanced against studies that establish buprenorphine is superior in important measures, including reducing overdose risk and mortality. It is also important to note that extended-release injectable naltrexone can be difficult to initiate because it requires a period of complete abstinence before treatment can start (to prevent inducing opioid withdrawal once naltrexone is started). Policy makers should continue to support expanded access to all three FDA-approved medications for opioid use disorder.
There is substantial research showing that opioid use disorder medications reduce opioid use, overdose risk, and overdose mortality. While opioid use is associated with other functional outcomes, studies that specifically include outcomes beyond substance use–quality of life, reduction of psychological symptoms, or social determinants of health, for example–can help inform treatment and public health messaging and recommendations. At the same time, researchers have not yet reached agreement on what measures other than reduced substance use best capture recovery progress and on what time scale, although a growing consensus favors some combination of standardized measures and patient centered outcomes.
Life satisfaction provides one potential way to measure a general sense of well-being in recovery. Life satisfaction has been defined as the degree to which people evaluate the overall quality of life based on the factors that matter most to them. Although not specific to a particular time or domain of life, life satisfaction is associated with positive health outcomes such as longer life expectancy, better disease tolerance, and fewer mental disorders. Low self-reported life satisfaction is associated with higher risk of suicide, among other negative health outcomes.
Individuals with opioid use disorder seeking treatment have a low life satisfaction compared to the general population. There is relatively little research on opioid use disorder medications, such as naltrexone, methadone, and buprenorphine, and life satisfaction. One study suggests that higher life satisfaction is associated with increased likelihood of prolonged abstinence among individuals with substance dependence. Another short-term 3-month trial showed an increase in life satisfaction among individuals treated with buprenorphine compared to the control group. However, participants emphasized that their lives were still not good, only somewhat better than before. This study conducted in Norway employs a measure of life satisfaction in comparing extended-release (injectable) naltrexone (also known by the brand name Vivitrol) to daily, oral buprenorphine (also known by the brand name Suboxone) in treating opioid use disorder.
HOW WAS THIS STUDY CONDUCTED?
This paper presents secondary outcomes from a trial conducted in Norway from November 2012 to July 2016 that compared monthly, injectable (XR) naltrexone to daily sublingual buprenorphine-naltrexone for the treatment of opioid use disorder. An earlier paper by the researchers reported that the trial found XR-naltrexone was equally effective as buprenorphine-naltrexone in terms of retention and abstinence from illicit opioids during a 12-week trial. An earlier secondary analysis of the same data found that XR naltrexone was more effective than buprenorphine-naltrexone in preventing relapses -defined as 4 consecutive weeks when any opioid (other than buprenorphine) was used or 7 consecutive days when any opioid (other than buprenorphine).
The first stage of this study was a 12-week, randomized control “open label” trial (“open label” means that participants knew which medication they were taking). Upon qualifying for the study, patients completed medically supervised withdrawal (i.e., detoxification) if necessary and were randomized to one of two treatment conditions. After 12 weeks, participants were given the choice of whether to continue on the medication that they were randomized to or switch to the other medication. By this point in the study, all but five participants in the buprenorphine group either dropped out or decided to switch to XR naltrexone. No participants switched from XR naltrexone to buprenorphine. As a result, the study researchers adapted their design for the second phase of the trial and compared the group that switched to naltrexone (“switchers”) to the group that continued naltrexone (“continuers”) for the remaining 26 weeks of the trial.
The researchers measured life satisfaction using the section from the Temporary Satisfaction with Life Scale that evaluates life satisfaction in the present. They administered the survey at the start of the study (“baseline”) and every four weeks through both the 12-week randomized, control trial and the 36-week comparison study. The researchers used the European Addiction Severity Index to assess the number of days that participants used illicit opioids, satisfaction with civil status, satisfaction with living arrangements, and satisfaction with leisure time.
The researchers created statistical models to estimate the strength of the association between 1) life satisfaction and opioid use (adjusted for age and gender); 2) between life satisfaction and satisfaction with living arrangements, civil status, and leisure time; and 3) life satisfaction and years of opioid use. They used another type of statistical model to evaluate whether there were well-defined sub-groups within the study population that followed distinct life satisfaction trajectories.
The study was open to men and women 18 to 60 years of age who met DSM IV criteria of opioid dependence. People were excluded from participation if they met the criteria for DSM IV alcohol dependence, were pregnant or breast-feeding, or met the criteria for a serious mental or somatic illness that could interfere with study participation. Men represented 73 percent of the study participants and the average age was 36.1 years old. On average, participants had been using illicit opioids for 7.6 years.
WHAT DID THIS STUDY FIND?
Receiving XR naltrexone associated with more life satisfaction.
At baseline, both groups had similar life satisfaction scores. At weeks 4 and 8, the life satisfaction score of the XR naltrexone group increased more than the buprenorphine group. The two groups were similar by the end of the 12-week treatment period.
During the 32-week follow-up, the group that switched from buprenorphine to XR naltrexone had a greater increase in life satisfaction than those who continued on XR naltrexone. Throughout this follow-up period, though, those continuing on XR naltrexone had either better or similar life satisfaction compared to those who switched onto XR naltrexone. This suggests those randomly assigned to buprenorphine during the initial treatment phase were not doing as well on life satisfaction but were able to somewhat catch up to those assigned to XR naltrexone and continued on that medication during follow-up.
More opioid use was associated with lower life satisfaction.
During the 12-week trial, frequent use of opioids (more than 20 days a month) was associated with lower life satisfaction scores across all participants, whether they received buprenorphine or XR naltrexone. However, at week 12, life satisfaction was similar for all participants, regardless of the number of times they used each month. In other words, people who were not using opioids or only used opioids a few days a month showed a small increase in life satisfaction from baseline to week 12, while people who used frequently had lower life satisfaction scores most weeks during the trial, but similar life satisfaction scores to other participants at week 12.
Participants starting out low on life satisfaction increased slightly at first, but changed little thereafter.
During the initial 12-week treatment phase, across all participants irrespective of which medication they received, the low life satisfaction group increased slightly at first then levelled off. The high life satisfaction group started out higher but changed very little during treatment. More opioid use was related to being in the lower satisfaction group, while those who were “indifferent” to their satisfaction with leisure time were more likely to be in the high satisfaction group compared to those who were “not satisfied” with their leisure time.
During the 32-week follow-up, again across all participants, those starting out higher on life satisfaction at the beginning of this follow-up period improved slightly over time. The group lower in life satisfaction did not improve at all during the follow-up period, however. Satisfaction with leisure time was the only factor that differed between the two groups, as above, such that those “indifferent” to their satisfaction with leisure time were more likely to be in the high satisfaction group compared to those “not satisfied.”
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This secondary analysis of a randomized controlled trial showed that participants receiving XR naltrexone generally had higher life satisfaction than those receiving buprenorphine. In a non-randomized follow-up where individuals could choose to switch medications if they wished, switching from buprenorphine to XR naltrexone helped these individuals catch up somewhat on life satisfaction, though being assigned to XR naltrexone and continuing on the medication still produced the highest levels of life satisfaction.
The study design may have accounted for the life satisfaction advantage for XR naltrexone, rather than the medication itself. Buprenorphine is widely available in Norway (the location of the study) and most participants in the trial appear to have signed up for the study as they were motivated to receive XR-naltrexone. It is possible that the lower improved life satisfaction of the buprenorphine group may have reflected that they received a treatment that they preferred less and/or the group that received XR naltrexone was more motivated and/or happier because they received their preferred treatment. Additionally, for buprenorphine participants, lower life satisfaction was associated with ranking satisfaction with leisure time as “low.” Given that participation in the buprenorphine-naltrexone arm required a daily clinic visit (whereas XR naltrexone does not), this requirement may have interfered with leisure activities, influencing this result. Future studies should compare identical modalities (i.e. XR naltrexone to XR Buprenorphine) and adopt a study design that guards against the possibility that outcomes such as lower life satisfaction reflect the patient’s randomization to a less-preferred medication.
Another important feature of the study design that may have contributed to this outcome was that participants currently taking opioids were required to undergo a medically supervised detox before they began treatment. Extended-release injectable naltrexone can be difficult to initiate because it requires a period of complete abstinence before treatment can start (to prevent inducing opioid withdrawal once naltrexone is started). In a prior study, only about 72% of patients randomly assigned to extended-release naltrexone successfully started it (vs. ~94% assigned to buprenorphine), presumably because of this difficulty of maintaining abstinence from opioids prior to beginning it. Consistently, about 37% of participants assigned to the naltrexone group in the current study failed to initiate this medication. This fact suggests that the XR naltrexone group may have been unusual in that they were highly motivated with abstinence as their desired goal. The greater increase in life satisfaction for the XR naltrexone group, therefore, may not generalize to less highly motivated groups or to groups with opioid use goals other than abstinence.
Previous research has established that buprenorphine has advantages compared to XR naltrexone for some crucial outcomes. When patients discontinue extended-release injectable naltrexone they have a reduced tolerance to opioids, and this puts them at greater risk of overdose should they return to opioid use at high enough doses, such as those used prior to treatment. Discontinuation of medication treatment also can occur more frequently with extended-release injectable naltrexone than buprenorphine. Buprenorphine is a partial opioid agonist and, as an agonist, it allows a patient to maintain a certain degree of opioid tolerance. Thus, a return to opioid use upon discontinuing buprenorphine treatment offers significantly greater protection from fatal overdose.
In terms of life satisfaction, the study population was divided into two trajectories (a higher and lower life satisfaction group), although the overall life satisfaction of both groups was quite modest. Most participants fell into the low life satisfaction group and, although this group showed some improvement in the first (randomized) phase of the study, this group remained stable with low life satisfaction during the second part of the study. In both phases, the high life satisfaction group saw a small amount of improvement, however this improvement levelled off toward the end of phase 2. The strongest predicators of belonging to the low life satisfaction group were higher frequency of opioid use and lower satisfaction with leisure time.
At the same time, it is important to note that this study saw high dropout rates for participants (only 58 of 159 participants completed the study), which impedes generalization of study findings. Further research is needed to explore whether these associations hold across different populations and, if so, the direction of influence (for example, whether lower life satisfaction leads to more opioid use, or more opioid use leads to lower life satisfaction, or some kind of bidirectional relationship exists between the two).
The fact that life satisfaction remained low for the majority of participants is concerning. However, it also raises the question of whether the life satisfaction measure is in fact capturing the relevant dynamics of change in the first year of recovery and whether 1 year is a sufficient time frame to capture increases in life satisfaction. Other measures, for example recovery capital, may well provide better indicators of a successful recovery trajectory. One study, based on a nationally representative sample of U.S. adults in recovery, suggests that quality of life, happiness, and self-esteem decrease during the initial months of recovery after initial stabilization before beginning to increase between 6 to 12 months after problem resolution. This dynamic is followed by steep increases in well-being over 6 years, followed by a more gradual increase afterwards. Notably, people with opioid use disorders are among the groups (along with women, certain racial/ethnic minorities, and people who use stimulants) that begin their recovery journey with less resources than other groups and experience more persistent problems with psychological distress in the first 3 years of recovery. Before the 1-year mark, life satisfaction measures may reflect an expected decrease in quality of life, happiness, and self-esteem as people begin to take stock of the challenges that lie ahead in recovery before these indices begin to improve towards or after the 1-year mark. Researchers may need to evaluate psychosocial outcomes on scales longer than 1 year in order to determine which measures accurately capture the longitudinal bigger picture improvements in well-being characteristic of long-term recovery.
Buprenorphine is widely available in Norway (the location of the study) and most participants in the trial appear to have been motivated to receive XR-naltrexone. It is possible that the lower improved life satisfaction of the buprenorphine group may have reflected the fact that they received a less preferred treatment.
Among this study population, lower life satisfaction was associated with ranking satisfaction with leisure time as “low.” Given that participation in the buprenorphine arm required a daily clinic visit (whereas injectable naltrexone does not), this requirement may have interfered with leisure activities, influencing the lower life satisfaction score.
There was substantial drop out over the course of the study (only 58 of 159 participants completed the study). Given the small sample size, these results cannot be generalized to other populations without further research.
BOTTOM LINE
This two-phase study found that XR (injectable) naltrexone was equal, and at some points superior, to daily, oral buprenorphine-naltrexone in terms of improvements in participant life satisfaction over one year. However, the life satisfaction of the majority of participants, even those with higher life satisfaction at the start and who showed the most improvement, remained low throughout the study period. Future research should continue to explore what patient reported outcomes best capture improvements across different phases of recovery while recognizing that the first year of recovery is likely variable and may not be indicative of later trends in recovery progress regarding life satisfaction.
For individuals and families seeking recovery: njectable, extended release (XR) naltrexone is 1 of 3 FDA approved medications for OUD (the other two being buprenorphine and methadone). This study compares XR naltrexone with daily, oral buprenorphine. It found that XR naltrexone is as effective as buprenorphine, and at some points it was more effective, in improving the life satisfaction of people with opioid use disorder. The same researchers previously published two articles that showed XR naltrexone was as effective as buprenorphine in terms of days abstinent from opioids, retention on the medication, and preventing relapse. These and other studies indicate that XR naltrexone is an effective treatment option for OUD. At the same time, the results should be balanced against studies that establish buprenorphine is superior in important measures, including reducing overdose risk and mortality. It is also important to note that extended-release injectable naltrexone can be difficult to initiate because it requires a period of complete abstinence before treatment can start (to prevent inducing opioid withdrawal once naltrexone is started). People in recovery from OUD and their families should talk through the benefits and drawbacks of all three medications with a qualified prescriber.
For treatment professionals and treatment systems: Injectable, extended release (XR) naltrexone is 1 of 3 FDA approved medications for OUD (the other two being buprenorphine and methadone). This study compares XR naltrexone with daily, oral buprenorphine. It found that XR naltrexone is as effective as buprenorphine, and at some points it was more effective, in improving the life satisfaction of people with opioid use disorder. The same researchers previously published two articles that showed XR naltrexone was as effective as buprenorphine in terms of days abstinent from opioids, retention on the medication, and preventing relapse. These and other studies indicate that XR naltrexone is an effective treatment option for OUD. At the same, the results should be balanced against studies that establish buprenorphine is superior in important measures, including reducing overdose risk and mortality. It is also important to note that extended-release injectable naltrexone can be difficult to initiate because it requires a period of complete abstinence before treatment can start (to prevent inducing opioid withdrawal once naltrexone is started). Treatment professionals should familiarize themselves with the current evidence regarding buprenorphine, methadone, and XR naltrexone and qualified prescribers should advise individuals in recovery and their families about the benefits and potential drawbacks of each medication.
For scientists:This two-phase study found that XR (injectable) naltrexone was not inferior, and at some points superior, to daily, oral buprenorphine-naltrexone in terms of improvements in participant life satisfaction over 48 months. However, the experience of these researchers suggests some lessons for future study design. Buprenorphine is widely available in Norway (the location of the study) and most participants in the trial may have been more motivated to receive XR-naltrexone compared to patients in general treatment settings. It is possible that members of the buprenorphine-naltrexone group may have received a treatment they preferred less. Additionally, among this population, lower life satisfaction was associated with ranking satisfaction with leisure time as “low.” Given that participation in the buprenorphine arm required a daily clinic visit (whereas injectable naltrexone did not), this requirement may have interfered with leisure activities, possibly influencing the result. Future studies should compare identical modalities (i.e., XR naltrexone to XR buprenorphine) and adopt a design that guards against the possibility that outcomes such as lower life satisfaction reflects a patient’s randomization to a less-preferred medication. Researchers may need to evaluate psychosocial outcomes on scales longer than 1 year in order to determine which measures in particular accurately capture the longitudinal improvements in well-being characteristic of long-term recovery.
For policy makers: Injectable, extended release (XR) naltrexone is 1 of 3 FDA approved medications for OUD (the other two being buprenorphine and methadone). This study compares XR naltrexone with daily, oral buprenorphine. It found that XR naltrexone is as effective as buprenorphine, and at some points it was more effective, in improving the life satisfaction of people with opioid use disorder. The same researchers previously published a 12-week study that showed XR naltrexone was also as effective as buprenorphine in terms of days abstinent from opioids and retention on medication. These and other studies indicate that XR naltrexone is an effective treatment option for OUD. At the same, the results should be balanced against studies that establish buprenorphine is superior in important measures, including reducing overdose risk and mortality. It is also important to note that extended-release injectable naltrexone can be difficult to initiate because it requires a period of complete abstinence before treatment can start (to prevent inducing opioid withdrawal once naltrexone is started). Policy makers should continue to support expanded access to all three FDA-approved medications for opioid use disorder.
There is substantial research showing that opioid use disorder medications reduce opioid use, overdose risk, and overdose mortality. While opioid use is associated with other functional outcomes, studies that specifically include outcomes beyond substance use–quality of life, reduction of psychological symptoms, or social determinants of health, for example–can help inform treatment and public health messaging and recommendations. At the same time, researchers have not yet reached agreement on what measures other than reduced substance use best capture recovery progress and on what time scale, although a growing consensus favors some combination of standardized measures and patient centered outcomes.
Life satisfaction provides one potential way to measure a general sense of well-being in recovery. Life satisfaction has been defined as the degree to which people evaluate the overall quality of life based on the factors that matter most to them. Although not specific to a particular time or domain of life, life satisfaction is associated with positive health outcomes such as longer life expectancy, better disease tolerance, and fewer mental disorders. Low self-reported life satisfaction is associated with higher risk of suicide, among other negative health outcomes.
Individuals with opioid use disorder seeking treatment have a low life satisfaction compared to the general population. There is relatively little research on opioid use disorder medications, such as naltrexone, methadone, and buprenorphine, and life satisfaction. One study suggests that higher life satisfaction is associated with increased likelihood of prolonged abstinence among individuals with substance dependence. Another short-term 3-month trial showed an increase in life satisfaction among individuals treated with buprenorphine compared to the control group. However, participants emphasized that their lives were still not good, only somewhat better than before. This study conducted in Norway employs a measure of life satisfaction in comparing extended-release (injectable) naltrexone (also known by the brand name Vivitrol) to daily, oral buprenorphine (also known by the brand name Suboxone) in treating opioid use disorder.
HOW WAS THIS STUDY CONDUCTED?
This paper presents secondary outcomes from a trial conducted in Norway from November 2012 to July 2016 that compared monthly, injectable (XR) naltrexone to daily sublingual buprenorphine-naltrexone for the treatment of opioid use disorder. An earlier paper by the researchers reported that the trial found XR-naltrexone was equally effective as buprenorphine-naltrexone in terms of retention and abstinence from illicit opioids during a 12-week trial. An earlier secondary analysis of the same data found that XR naltrexone was more effective than buprenorphine-naltrexone in preventing relapses -defined as 4 consecutive weeks when any opioid (other than buprenorphine) was used or 7 consecutive days when any opioid (other than buprenorphine).
The first stage of this study was a 12-week, randomized control “open label” trial (“open label” means that participants knew which medication they were taking). Upon qualifying for the study, patients completed medically supervised withdrawal (i.e., detoxification) if necessary and were randomized to one of two treatment conditions. After 12 weeks, participants were given the choice of whether to continue on the medication that they were randomized to or switch to the other medication. By this point in the study, all but five participants in the buprenorphine group either dropped out or decided to switch to XR naltrexone. No participants switched from XR naltrexone to buprenorphine. As a result, the study researchers adapted their design for the second phase of the trial and compared the group that switched to naltrexone (“switchers”) to the group that continued naltrexone (“continuers”) for the remaining 26 weeks of the trial.
The researchers measured life satisfaction using the section from the Temporary Satisfaction with Life Scale that evaluates life satisfaction in the present. They administered the survey at the start of the study (“baseline”) and every four weeks through both the 12-week randomized, control trial and the 36-week comparison study. The researchers used the European Addiction Severity Index to assess the number of days that participants used illicit opioids, satisfaction with civil status, satisfaction with living arrangements, and satisfaction with leisure time.
The researchers created statistical models to estimate the strength of the association between 1) life satisfaction and opioid use (adjusted for age and gender); 2) between life satisfaction and satisfaction with living arrangements, civil status, and leisure time; and 3) life satisfaction and years of opioid use. They used another type of statistical model to evaluate whether there were well-defined sub-groups within the study population that followed distinct life satisfaction trajectories.
The study was open to men and women 18 to 60 years of age who met DSM IV criteria of opioid dependence. People were excluded from participation if they met the criteria for DSM IV alcohol dependence, were pregnant or breast-feeding, or met the criteria for a serious mental or somatic illness that could interfere with study participation. Men represented 73 percent of the study participants and the average age was 36.1 years old. On average, participants had been using illicit opioids for 7.6 years.
WHAT DID THIS STUDY FIND?
Receiving XR naltrexone associated with more life satisfaction.
At baseline, both groups had similar life satisfaction scores. At weeks 4 and 8, the life satisfaction score of the XR naltrexone group increased more than the buprenorphine group. The two groups were similar by the end of the 12-week treatment period.
During the 32-week follow-up, the group that switched from buprenorphine to XR naltrexone had a greater increase in life satisfaction than those who continued on XR naltrexone. Throughout this follow-up period, though, those continuing on XR naltrexone had either better or similar life satisfaction compared to those who switched onto XR naltrexone. This suggests those randomly assigned to buprenorphine during the initial treatment phase were not doing as well on life satisfaction but were able to somewhat catch up to those assigned to XR naltrexone and continued on that medication during follow-up.
More opioid use was associated with lower life satisfaction.
During the 12-week trial, frequent use of opioids (more than 20 days a month) was associated with lower life satisfaction scores across all participants, whether they received buprenorphine or XR naltrexone. However, at week 12, life satisfaction was similar for all participants, regardless of the number of times they used each month. In other words, people who were not using opioids or only used opioids a few days a month showed a small increase in life satisfaction from baseline to week 12, while people who used frequently had lower life satisfaction scores most weeks during the trial, but similar life satisfaction scores to other participants at week 12.
Participants starting out low on life satisfaction increased slightly at first, but changed little thereafter.
During the initial 12-week treatment phase, across all participants irrespective of which medication they received, the low life satisfaction group increased slightly at first then levelled off. The high life satisfaction group started out higher but changed very little during treatment. More opioid use was related to being in the lower satisfaction group, while those who were “indifferent” to their satisfaction with leisure time were more likely to be in the high satisfaction group compared to those who were “not satisfied” with their leisure time.
During the 32-week follow-up, again across all participants, those starting out higher on life satisfaction at the beginning of this follow-up period improved slightly over time. The group lower in life satisfaction did not improve at all during the follow-up period, however. Satisfaction with leisure time was the only factor that differed between the two groups, as above, such that those “indifferent” to their satisfaction with leisure time were more likely to be in the high satisfaction group compared to those “not satisfied.”
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This secondary analysis of a randomized controlled trial showed that participants receiving XR naltrexone generally had higher life satisfaction than those receiving buprenorphine. In a non-randomized follow-up where individuals could choose to switch medications if they wished, switching from buprenorphine to XR naltrexone helped these individuals catch up somewhat on life satisfaction, though being assigned to XR naltrexone and continuing on the medication still produced the highest levels of life satisfaction.
The study design may have accounted for the life satisfaction advantage for XR naltrexone, rather than the medication itself. Buprenorphine is widely available in Norway (the location of the study) and most participants in the trial appear to have signed up for the study as they were motivated to receive XR-naltrexone. It is possible that the lower improved life satisfaction of the buprenorphine group may have reflected that they received a treatment that they preferred less and/or the group that received XR naltrexone was more motivated and/or happier because they received their preferred treatment. Additionally, for buprenorphine participants, lower life satisfaction was associated with ranking satisfaction with leisure time as “low.” Given that participation in the buprenorphine-naltrexone arm required a daily clinic visit (whereas XR naltrexone does not), this requirement may have interfered with leisure activities, influencing this result. Future studies should compare identical modalities (i.e. XR naltrexone to XR Buprenorphine) and adopt a study design that guards against the possibility that outcomes such as lower life satisfaction reflect the patient’s randomization to a less-preferred medication.
Another important feature of the study design that may have contributed to this outcome was that participants currently taking opioids were required to undergo a medically supervised detox before they began treatment. Extended-release injectable naltrexone can be difficult to initiate because it requires a period of complete abstinence before treatment can start (to prevent inducing opioid withdrawal once naltrexone is started). In a prior study, only about 72% of patients randomly assigned to extended-release naltrexone successfully started it (vs. ~94% assigned to buprenorphine), presumably because of this difficulty of maintaining abstinence from opioids prior to beginning it. Consistently, about 37% of participants assigned to the naltrexone group in the current study failed to initiate this medication. This fact suggests that the XR naltrexone group may have been unusual in that they were highly motivated with abstinence as their desired goal. The greater increase in life satisfaction for the XR naltrexone group, therefore, may not generalize to less highly motivated groups or to groups with opioid use goals other than abstinence.
Previous research has established that buprenorphine has advantages compared to XR naltrexone for some crucial outcomes. When patients discontinue extended-release injectable naltrexone they have a reduced tolerance to opioids, and this puts them at greater risk of overdose should they return to opioid use at high enough doses, such as those used prior to treatment. Discontinuation of medication treatment also can occur more frequently with extended-release injectable naltrexone than buprenorphine. Buprenorphine is a partial opioid agonist and, as an agonist, it allows a patient to maintain a certain degree of opioid tolerance. Thus, a return to opioid use upon discontinuing buprenorphine treatment offers significantly greater protection from fatal overdose.
In terms of life satisfaction, the study population was divided into two trajectories (a higher and lower life satisfaction group), although the overall life satisfaction of both groups was quite modest. Most participants fell into the low life satisfaction group and, although this group showed some improvement in the first (randomized) phase of the study, this group remained stable with low life satisfaction during the second part of the study. In both phases, the high life satisfaction group saw a small amount of improvement, however this improvement levelled off toward the end of phase 2. The strongest predicators of belonging to the low life satisfaction group were higher frequency of opioid use and lower satisfaction with leisure time.
At the same time, it is important to note that this study saw high dropout rates for participants (only 58 of 159 participants completed the study), which impedes generalization of study findings. Further research is needed to explore whether these associations hold across different populations and, if so, the direction of influence (for example, whether lower life satisfaction leads to more opioid use, or more opioid use leads to lower life satisfaction, or some kind of bidirectional relationship exists between the two).
The fact that life satisfaction remained low for the majority of participants is concerning. However, it also raises the question of whether the life satisfaction measure is in fact capturing the relevant dynamics of change in the first year of recovery and whether 1 year is a sufficient time frame to capture increases in life satisfaction. Other measures, for example recovery capital, may well provide better indicators of a successful recovery trajectory. One study, based on a nationally representative sample of U.S. adults in recovery, suggests that quality of life, happiness, and self-esteem decrease during the initial months of recovery after initial stabilization before beginning to increase between 6 to 12 months after problem resolution. This dynamic is followed by steep increases in well-being over 6 years, followed by a more gradual increase afterwards. Notably, people with opioid use disorders are among the groups (along with women, certain racial/ethnic minorities, and people who use stimulants) that begin their recovery journey with less resources than other groups and experience more persistent problems with psychological distress in the first 3 years of recovery. Before the 1-year mark, life satisfaction measures may reflect an expected decrease in quality of life, happiness, and self-esteem as people begin to take stock of the challenges that lie ahead in recovery before these indices begin to improve towards or after the 1-year mark. Researchers may need to evaluate psychosocial outcomes on scales longer than 1 year in order to determine which measures accurately capture the longitudinal bigger picture improvements in well-being characteristic of long-term recovery.
Buprenorphine is widely available in Norway (the location of the study) and most participants in the trial appear to have been motivated to receive XR-naltrexone. It is possible that the lower improved life satisfaction of the buprenorphine group may have reflected the fact that they received a less preferred treatment.
Among this study population, lower life satisfaction was associated with ranking satisfaction with leisure time as “low.” Given that participation in the buprenorphine arm required a daily clinic visit (whereas injectable naltrexone does not), this requirement may have interfered with leisure activities, influencing the lower life satisfaction score.
There was substantial drop out over the course of the study (only 58 of 159 participants completed the study). Given the small sample size, these results cannot be generalized to other populations without further research.
BOTTOM LINE
This two-phase study found that XR (injectable) naltrexone was equal, and at some points superior, to daily, oral buprenorphine-naltrexone in terms of improvements in participant life satisfaction over one year. However, the life satisfaction of the majority of participants, even those with higher life satisfaction at the start and who showed the most improvement, remained low throughout the study period. Future research should continue to explore what patient reported outcomes best capture improvements across different phases of recovery while recognizing that the first year of recovery is likely variable and may not be indicative of later trends in recovery progress regarding life satisfaction.
For individuals and families seeking recovery: njectable, extended release (XR) naltrexone is 1 of 3 FDA approved medications for OUD (the other two being buprenorphine and methadone). This study compares XR naltrexone with daily, oral buprenorphine. It found that XR naltrexone is as effective as buprenorphine, and at some points it was more effective, in improving the life satisfaction of people with opioid use disorder. The same researchers previously published two articles that showed XR naltrexone was as effective as buprenorphine in terms of days abstinent from opioids, retention on the medication, and preventing relapse. These and other studies indicate that XR naltrexone is an effective treatment option for OUD. At the same time, the results should be balanced against studies that establish buprenorphine is superior in important measures, including reducing overdose risk and mortality. It is also important to note that extended-release injectable naltrexone can be difficult to initiate because it requires a period of complete abstinence before treatment can start (to prevent inducing opioid withdrawal once naltrexone is started). People in recovery from OUD and their families should talk through the benefits and drawbacks of all three medications with a qualified prescriber.
For treatment professionals and treatment systems: Injectable, extended release (XR) naltrexone is 1 of 3 FDA approved medications for OUD (the other two being buprenorphine and methadone). This study compares XR naltrexone with daily, oral buprenorphine. It found that XR naltrexone is as effective as buprenorphine, and at some points it was more effective, in improving the life satisfaction of people with opioid use disorder. The same researchers previously published two articles that showed XR naltrexone was as effective as buprenorphine in terms of days abstinent from opioids, retention on the medication, and preventing relapse. These and other studies indicate that XR naltrexone is an effective treatment option for OUD. At the same, the results should be balanced against studies that establish buprenorphine is superior in important measures, including reducing overdose risk and mortality. It is also important to note that extended-release injectable naltrexone can be difficult to initiate because it requires a period of complete abstinence before treatment can start (to prevent inducing opioid withdrawal once naltrexone is started). Treatment professionals should familiarize themselves with the current evidence regarding buprenorphine, methadone, and XR naltrexone and qualified prescribers should advise individuals in recovery and their families about the benefits and potential drawbacks of each medication.
For scientists:This two-phase study found that XR (injectable) naltrexone was not inferior, and at some points superior, to daily, oral buprenorphine-naltrexone in terms of improvements in participant life satisfaction over 48 months. However, the experience of these researchers suggests some lessons for future study design. Buprenorphine is widely available in Norway (the location of the study) and most participants in the trial may have been more motivated to receive XR-naltrexone compared to patients in general treatment settings. It is possible that members of the buprenorphine-naltrexone group may have received a treatment they preferred less. Additionally, among this population, lower life satisfaction was associated with ranking satisfaction with leisure time as “low.” Given that participation in the buprenorphine arm required a daily clinic visit (whereas injectable naltrexone did not), this requirement may have interfered with leisure activities, possibly influencing the result. Future studies should compare identical modalities (i.e., XR naltrexone to XR buprenorphine) and adopt a design that guards against the possibility that outcomes such as lower life satisfaction reflects a patient’s randomization to a less-preferred medication. Researchers may need to evaluate psychosocial outcomes on scales longer than 1 year in order to determine which measures in particular accurately capture the longitudinal improvements in well-being characteristic of long-term recovery.
For policy makers: Injectable, extended release (XR) naltrexone is 1 of 3 FDA approved medications for OUD (the other two being buprenorphine and methadone). This study compares XR naltrexone with daily, oral buprenorphine. It found that XR naltrexone is as effective as buprenorphine, and at some points it was more effective, in improving the life satisfaction of people with opioid use disorder. The same researchers previously published a 12-week study that showed XR naltrexone was also as effective as buprenorphine in terms of days abstinent from opioids and retention on medication. These and other studies indicate that XR naltrexone is an effective treatment option for OUD. At the same, the results should be balanced against studies that establish buprenorphine is superior in important measures, including reducing overdose risk and mortality. It is also important to note that extended-release injectable naltrexone can be difficult to initiate because it requires a period of complete abstinence before treatment can start (to prevent inducing opioid withdrawal once naltrexone is started). Policy makers should continue to support expanded access to all three FDA-approved medications for opioid use disorder.