Recovery support and harm reduction strategies both critical to addressing the opioid crisis, new research shows
More than 1 million Americans have died of a drug overdose since 1999, with these deaths at an all-time high despite significant investments to address this public health emergency. In this study, researchers used a simulation model to test the potential impact of 11 strategies across the continuum of care – prevention, harm reduction, treatment, and recovery – on opioid use disorder and opioid-related overdose death.
In 2021, drug overdose deaths set another record with more than 108,000 Americans losing their lives to this preventable condition, a 50% increase from just 2 years ago. Overall, more than 1 million Americans have died of a drug overdose since 1999. These deaths have been driven by opioids, with the latest and worst wave of deaths involving illicitly manufactured fentanyl.
There has been a large investment in implementing policies and interventions to address this opioid overdose crisis, primarily aimed at reducing opioid prescribing, expanding access to medication treatment for opioid use disorder, and increasing the amount of naloxone (“Narcan”) in communities. Despite these efforts, the crisis continues to worsen.
Models that simulate future scenarios can be useful in helping policymakers identify the best strategies to pursue in the face of limited resources. Previously, a team of researchers developed SOURCE (Simulation of Opioid Use, Response, Consequences, and Effects), a model of the evolution of the opioid crisis in the United States that provides a basis for projecting and analyzing potential policy impacts and solutions. In this study, researchers used the SOURCE model to project the impact of 11 strategies, and combinations thereof, on the prevalence of opioid use disorder and fatal opioid overdoses from 2022 to 2032. These strategies represented interventions across the continuum of care – prevention, harm reduction, treatment, and recovery. Results from this simulated model could provide insight into which types of strategies are critical in turning the tide of the opioid crisis.
HOW WAS THIS STUDY CONDUCTED?
This study leverages the previously developed SOURCE model to project the impact of 11 strategies across the continuum of care – prevention, harm reduction, treatment, and recovery – on the prevalence of opioid use disorder and fatal opioid overdose from 2022 to 2032.
The SOURCE model draws on multiple data sources to replicate how risks of opioid misuse initiation and overdose have evolved over time in the United States and suggests how those risks may evolve in the future under specific conditions. The model is considered high-level and data-driven, and uses a systems dynamics approach of individuals transitioning through states of opioid use and opioid use disorder as well as treatment, remission, and stable remission. The model incorporates feedback loops that may influence these transition states. These feedback loops include social influence, perceived risk, treatment availability, and prescription opioid availability on the street. As an example of a feedback loop, an increase in the perceived risk of prescription opioids would be expected to decrease the number of people who begin misusing opioids. In addition to deriving some assumptions from epidemiological data, assumptions are also informed by interviews and close collaboration with subject matter experts. More detail on how the SOURCE model was developed, including assumptions built into the model, can be found here.
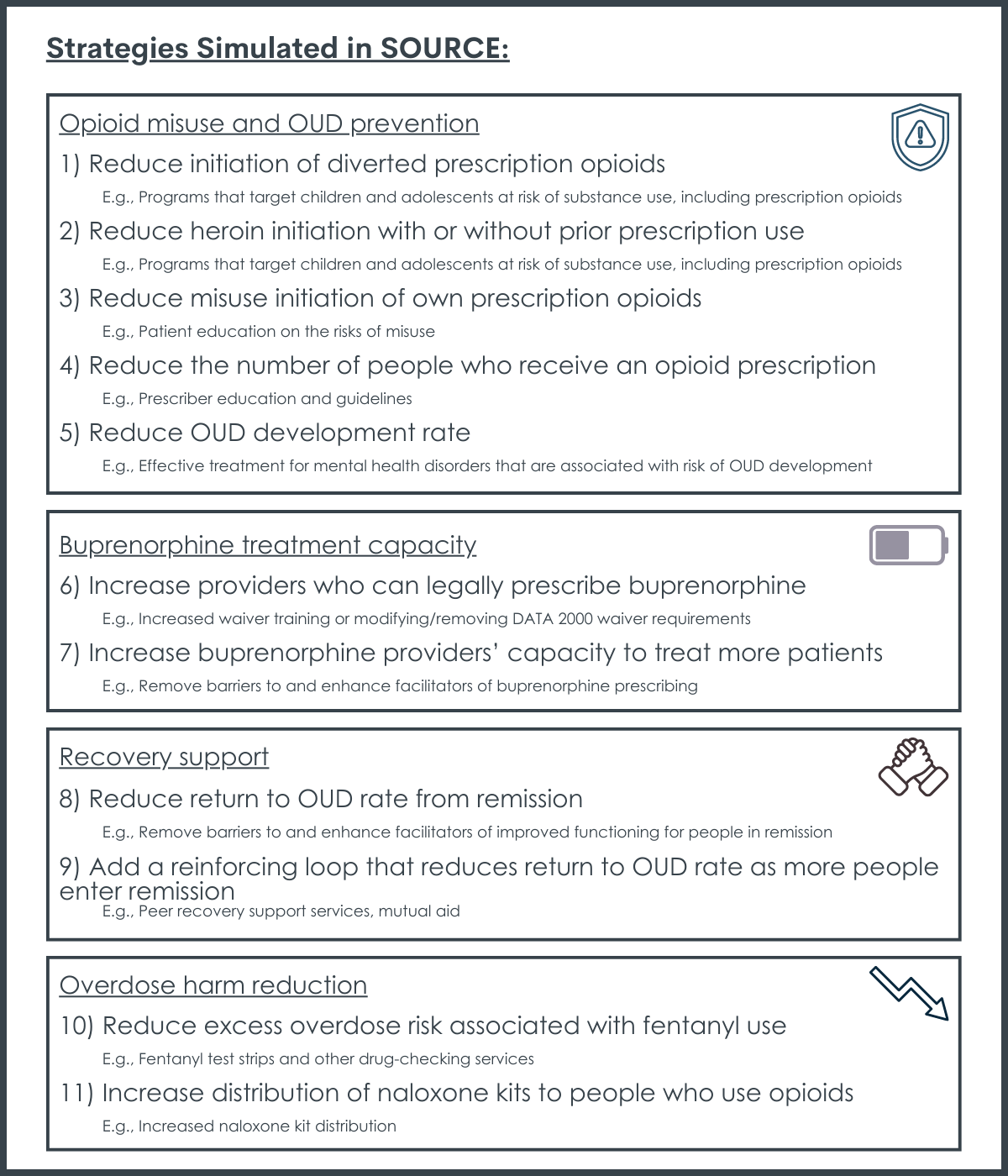
The 11 strategies applied to the SOURCE model and an example of each strategy include:
The model measured the impact of each strategy on both prevalence of opioid use disorder and fatal opioid overdose from 2022 to 2032. The model assumes that it will take 3 years for full implementation of each strategy and that the strategies are then fully sustained throughout the study period.
Because of the lack of documented effect sizes and the varying level of evidence across the 11 strategies, the model assumed an across-the-board 20% effect size for each strategy. However, given the evidence on the efficiency of naloxone (“Narcan”) distribution, a 20% effect size was assumed to translate into a real-world 10% increase in the probability of naloxone administration in the event of an overdose. Researchers also combined strategies to see which set of strategies might have the largest impact. More detail on the assumptions and parameters on the model can be found here.
It is important to note that these strategies as tested in the model are broad and evidence is still emerging on what are the most helpful ways (i.e., specific interventions) to accomplish these broader approaches to addressing the overdose crisis. For example, one strategy is to reduce the excess overdose risk associated with fentanyl. However, evidence is still lacking on how to best reduce this risk. Therefore, the model oftentimes will highlight the importance of a broad strategy, but much work still needs to be done to figure out the best way to realize this strategy in the real world. In other words, the model is not identifying specific types of interventions needed to address the opioid crisis. Rather, the model tests approaches where allocating resources into research and practice could be most helpful in identifying specific types of interventions that would have the maximal impact on reducing the prevalence of opioid use disorder and fatal opioid overdoses.
WHAT DID THIS STUDY FIND?
Recovery support most impactful on prevalence of opioid use disorder.
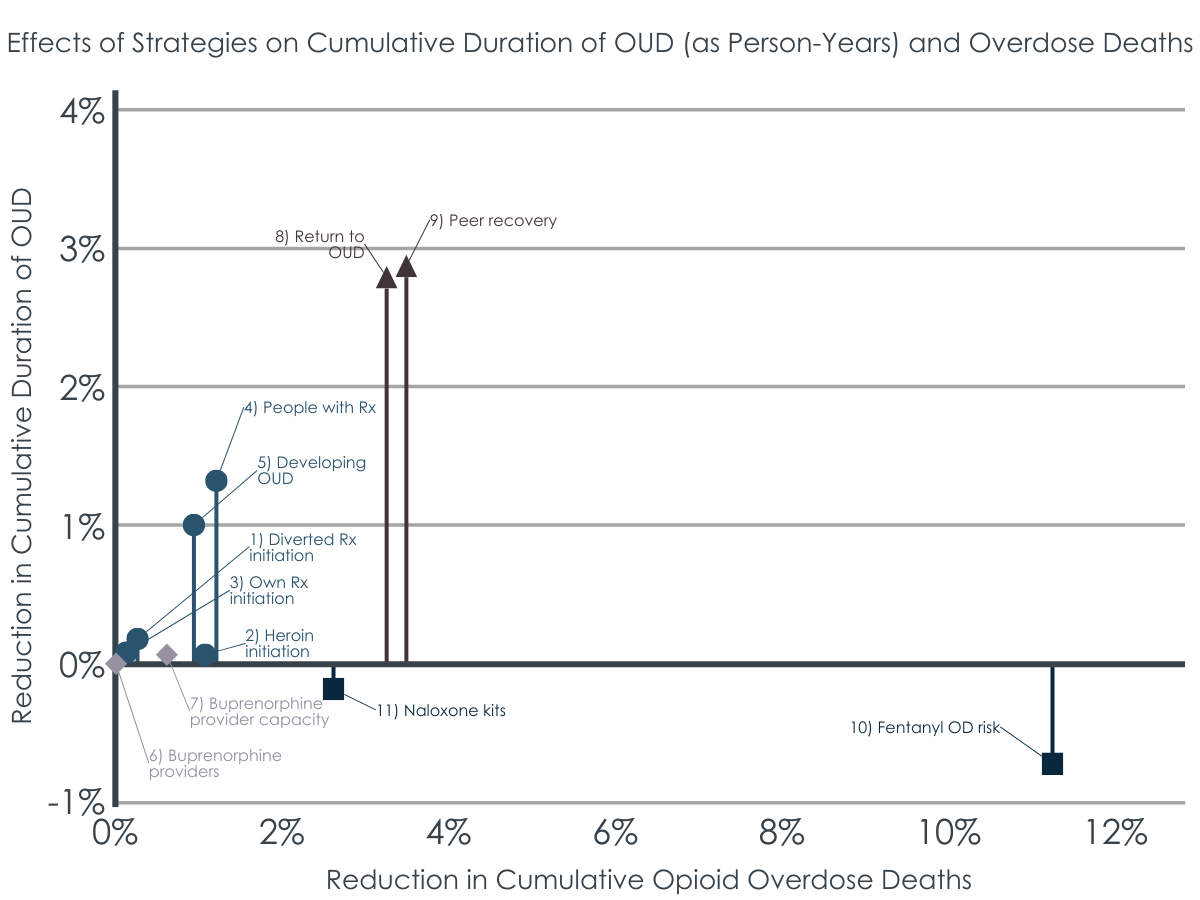
By 2032, the model projected a 5.2% and 5.4% decrease in the prevalence of opioid use disorder for the strategies of reducing the return to opioid use disorder and peer support, respectively, and this impact was gradual over the time period modelled. The model predicted that people returning to problematic opioid use after a year of remission would be a larger source for opioid use disorder prevalence than new cases, contributing to the large impact seen. The recovery support strategies also had a large impact on fatal opioid overdoses, with reduction of 5.7% and 6.1% by 2032 for the strategies of reducing the return to opioid use disorder and peer support, respectively.
Harm reduction strategies most impactful on number of fatal opioid overdoses.
By 2032, the models projected a 14.2% and 3.4% decrease in the prevalence of fatal opioid overdose for the fentanyl harm reduction strategy and increasing naloxone distribution to people who use opioids, respectively, and this impact was immediate after full implementation of these strategies (after 3 years or by 2025). The model predicted that the overdose harm reduction strategies led to a small increase in the prevalence of opioid use disorder because of the lives saved by these strategies.
Expanding buprenorphine treatment capacity only had impact in the short term.
Somewhat surprisingly, expanding buprenorphine treatment capacity had only a modest impact on the prevalence of opioid use disorder and fatal opioid overdose. Increasing the number of buprenorphine providers had no impact and increasing buprenorphine provider capacity had very little impact on the prevalence of opioid use disorder and a modest impact on fatal opioid overdoses, but only in the short term (i.e., first 3 years). These modest impacts are seen largely because the model predicted a decrease in opioid use disorder over time, and thus a decrease in the demand for treatment. In addition, the model accounts for a realistic number of patients that each buprenorphine prescriber can treat, and it is built into the model that most providers qualified to prescribe buprenorphine do not treat any patients.
The impact of prevention strategies took many years to materialize.
Some of the prevention strategies had an impact on the prevalence of opioid use disorder and fatal opioid overdose, but this impact was not seen until full implementation of the intervention (i.e., 3 years or 2025) and the impact increased gradually over time. Decreasing heroin initiation mainly had a gradual impact on fatal opioid overdoses, whereas reducing the number of people who receive an opioid prescription and reducing the development of opioid use disorder had a gradual impact on both the prevalence of opioid use disorder and fatal opioid overdoses.
A combination of strategies produced the largest impact on the prevalence of opioid use disorder and fatal opioid overdoses.
The largest impacts were realized when strategies were combined, although the effects of the strategies were found to be additive rather than synergistic (i.e., there were no multiplicative effects where the full impact is greater than the sum of each strategy’s impact). The most impactful set of strategies was combining the recovery support strategies, overdose harm reduction strategies, and the prevention strategies of reducing heroin initiation, the number of people who receive an opioid prescription, and the development of opioid use disorder. This set of strategies achieved a 29.9% reduction in fatal opioid overdoses and a 15.1% reduction in the prevalence of opioid use disorder by 2032.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This modelling study found that recovery support strategies had the largest impact on reducing the prevalence of opioid use disorder and overdose harm reduction strategies had the largest impact on decreasing fatal opioid overdoses, while, somewhat surprisingly, expanding buprenorphine treatment capacity had only a modest impact on decreasing fatal opioid overdoses and this impact was only present in the short term. The largest impact was seen when recovery support, overdose harm reduction, and prevention strategies were combined.
This is not the first modelling study to forecast the impact of policies and interventions to address the opioid crisis, which have consistently found that expanding access to treatment and increasing naloxone distribution are critical strategies. However, this is the first modelling study to include recovery support in the model.
Findings from this study show that recovery support strategies are essential in addressing the opioid crisis, especially in reducing the prevalence of opioid use disorder over time, by helping individuals stay in remission (i.e., preventing relapse).
Both the recovery support strategies that reduce return to active opioid use disorder and increase peer support were found to be equally effective in reducing the prevalence of opioid use disorder and fatal opioid overdose over the study period. Within these broad strategies, reducing return to active opioid use disorder might include policies and interventions that remove barriers to and enhance facilitators of improved functioning for people in remission, such as employment supports, housing stability assistance, and improved social role functioning. Peer support strategies might include mutual-help groups, recovery residences, and peer-based recovery community centers, and the model assumed a positive feedback loop serving as a proxy for the strengthening of the recovery community as more people with opioid use disorder move into remission. These findings suggest that the recovery community and recovery support services, an often-overlooked component of the treatment continuum for opioid use disorder, are critical in the national response to the opioid crisis and should be adequately funded as such. In addition, recovery capital, which captures improvements in many of these domains, might be an important measurement to incorporate in research studies on opioid use disorder treatment and recovery.
The model found that harm reduction strategies were critical in lowering fatal opioid overdoses, especially interventions that would reduce the excess overdose risk associated with fentanyl. Naloxone distribution is a known evidence-based strategy to reduce fatal opioid overdoses, although substantial expansion is needed to realize its potential. Evidence for types of fentanyl harm reduction strategies is emerging, with drug checking being one promising intervention in this domain, although it is unclear if these types of services could achieve the hypothetical 20% effect size used in the model. Rather, the impact of the broad strategy of fentanyl overdose harm reduction should be interpreted as the number of lives that could be saved if people who use, or may be exposed to, fentanyl could reduce their risk of overdose reliably. Therefore, more research into practices that could increase this reliability are warranted.
Findings from this modelling study are unique in that the impact of treatment expansion was modest and only impactful in the short term.
Reasons given for this modest impact include: most providers qualified to prescribe buprenorphine do not treat any patients with opioid use disorder, there will be capacity limitations for current buprenorphine prescribers especially if retention is increased, and there was a declining trend in the prevalence of opioid use disorder at the beginning of the study period that would translate into a decreasing demand for treatment. However, there is rigorous evidence that buprenorphine treatment saves lives and is a critical tool in addressing the opioid crisis. Therefore, findings from this modelling study do not necessarily discount the value of expanding treatment access but encourage us to think about innovative ways to expand treatment capacity (e.g., increase fee reimbursements, decrease administrative burden on providers) while also emphasizing potentially higher-impact strategies like harm reduction and recovery support. Notably, the strategy of reducing return to active opioid use disorder is considered a recovery support strategy, although strategies to improve long-term maintenance of medications, which are oftentimes delivered in treatment settings, are also likely to reduce return to active opioid use disorder.
The model suggests that certain prevention strategies are important, but their effects are likely to be gradual and over a longer horizon. Decreasing heroin initiation (with or without initial use of prescription opioids), which might include programs aimed at children and adolescents at risk of substance use, mainly had a gradual impact on fatal opioid overdoses. Reducing the number of people who receive an opioid prescription, such as policies and interventions that reduce the number of people initiating opioid use as well as using alternatives to opioids for conditions where opioids might be appropriate, had a gradual impact on both the prevalence of opioid use disorder and fatal opioid overdoses. Reducing the development of opioid use disorder among people misusing opioids had a gradual impact on both the prevalence of opioid use disorder and fatal opioid overdoses, and this broad strategy might include addressing factors that increase the risk of this transition, such as economic deprivation and mental health conditions. Overall, prevention strategies are necessary to prevent new cases of opioid misuse and opioid use disorder that put people at risk for opioid overdose.
Previous findings of modelling studies highlight the importance of a portfolio of policies and interventions to address the opioid crisis, and findings from this study corroborate this. Somewhat surprisingly, this model finds that including strategies to expand treatment is not as important, and that combining recovery support strategies, overdose harm reduction strategies, and the prevention strategies of reducing heroin initiation, the number of people who receive an opioid prescription, and the development of opioid use disorder led to the largest impact on the prevalence of opioid use disorder and fatal opioid overdose.
The SOURCE model itself, as well as this study that tests the impact of 11 strategies using the SOURCE model, make many assumptions due to gaps in the literature and rely on epidemiological data with significant limitations. Although the researchers incorporated expert interviews to improve their assumptions and made adjustments to address some of the limitations of the epidemiological data sources used, forecasting the future with these types of models is extremely difficult. In light of these limitations, the model, although not perfect, is still useful to inform policies and responses to the U.S. opioid crisis.
This is a US-specific national modelling study. Therefore, generalizing the model’s findings to states or regions in the U.S., as well as other countries, should be done with caution.
Only buprenorphine was used to measure expanding treatment capacity, although methadone and extended-release naltrexone are other medication options for opioid use disorder. Excluding these treatment options may have diminished the impact of treatment expansion in the model.
The model assumes that people who are prescribed opioids but do not misuse them are not at risk of developing opioid use disorder. Other studies have shown that chronic pain patients, who are often prescribed high doses of opioids over long durations, can develop opioid use disorder when taking the medication exactly as prescribed.
The opioid crisis has increasingly become a polysubstance and fentanyl crisis, where people with opioid use disorder more often than not are using several other substances and many overdose deaths are occurring in individuals without an opioid use disorder who are experimenting with counterfeit pills containing fentanyl. The model would likely have difficulty forecasting the impact of strategies given these recent developments.
Other factors that have driven the opioid crisis were not included in the SOURCE model, such as socioeconomic status, involvement in the criminal justice system, co-occurring mental health conditions, and trauma.
BOTTOM LINE
This study leverages the previously developed SOURCE model to project the impact of 11 strategies across the continuum of care – prevention, harm reduction, treatment, and recovery – on the prevalence of opioid use disorder and fatal opioid overdose from 2022 to 2032. Recovery support strategies had the largest impact on reducing the prevalence of opioid use disorder, and overdose harm reduction strategies had the largest impact on decreasing fatal opioid overdoses, while, somewhat surprisingly, expanding buprenorphine treatment capacity had an impact only on decreasing fatal opioid overdoses and this impact was only present in the short term. The largest impact was seen when recovery support, overdose harm reduction, and prevention strategies were combined.
For individuals and families seeking recovery: Although treatment with medications is emphasized as vital in helping individuals with opioid use disorder, this study shows that other strategies are just as important. For individuals who are actively using opioids, harm reduction strategies are critical for reducing overdose risk. For individuals who are in remission from opioid use disorder (e.g., finished a treatment program and/or stable on a medication), engagement in recovery support services and the recovery community in general could help them sustain remission and improve their quality of life.
For treatment professionals and treatment systems: Although treatment with medications is emphasized as vital in helping individuals with opioid use disorder, this study shows that other strategies are just as important. A treatment continuum that provides education on and access to harm reduction services is likely to reduce overdose risk for people who return to problematic substance use. Aftercare following treatment completion with a long horizon (i.e., 5 years after treatment initiation), which includes engagement in recovery support services and the recovery community in general, is likely to help clients sustain remission and improve their quality of life.
For scientists:In light of the limitations discussed above, this study that tests 11 different strategies using the SOURCE model, although not without limitations, is still useful to inform responses to the U.S. opioid crisis. The model uses a hypothetical effect size (20%) and broad strategies to identify areas where additional research might be fruitful. For example, harm reduction strategies to reduce fentanyl overdose risk is one area where additional research is warranted, as different types of drug checking are recently emerging as promising interventions to address an illicit drug supply contaminated with fentanyl. In addition, according to the model, recovery support services, such as those addressing housing, employment, and education, and peer support strategies, such as mutual aid, recovery community centers, and increasing the recovery community in general, will be critical in sustaining remission of opioid use disorder. Research into better understanding which types of interventions remove barriers to or enhance facilitators of improved functioning for people in remission are warranted.
For policy makers: The results of this study highlight the importance of a comprehensive response to the opioid crisis. Although treatment with medications is vital in helping individuals with opioid use disorder, other strategies may be just as important or even more important in pursuing. Supporting research for and implementation of harm reduction programs, especially those aimed at reducing the risk of fentanyl overdose, are critical in reducing opioid overdose deaths. Supporting research for and implementation of recovery support services, along with enhancing the overall impact of peer support delivered by the recovery community, are critical to helping people stay in remission from opioid use disorder and improve their quality of life. The best response to the opioid crisis will be a comprehensive set of strategies that involves the best policies and interventions to prevent new cases of opioid use disorder, reduce overdose risk, and get people with opioid use disorder into remission and sustain their remission over time.
In 2021, drug overdose deaths set another record with more than 108,000 Americans losing their lives to this preventable condition, a 50% increase from just 2 years ago. Overall, more than 1 million Americans have died of a drug overdose since 1999. These deaths have been driven by opioids, with the latest and worst wave of deaths involving illicitly manufactured fentanyl.
There has been a large investment in implementing policies and interventions to address this opioid overdose crisis, primarily aimed at reducing opioid prescribing, expanding access to medication treatment for opioid use disorder, and increasing the amount of naloxone (“Narcan”) in communities. Despite these efforts, the crisis continues to worsen.
Models that simulate future scenarios can be useful in helping policymakers identify the best strategies to pursue in the face of limited resources. Previously, a team of researchers developed SOURCE (Simulation of Opioid Use, Response, Consequences, and Effects), a model of the evolution of the opioid crisis in the United States that provides a basis for projecting and analyzing potential policy impacts and solutions. In this study, researchers used the SOURCE model to project the impact of 11 strategies, and combinations thereof, on the prevalence of opioid use disorder and fatal opioid overdoses from 2022 to 2032. These strategies represented interventions across the continuum of care – prevention, harm reduction, treatment, and recovery. Results from this simulated model could provide insight into which types of strategies are critical in turning the tide of the opioid crisis.
HOW WAS THIS STUDY CONDUCTED?
This study leverages the previously developed SOURCE model to project the impact of 11 strategies across the continuum of care – prevention, harm reduction, treatment, and recovery – on the prevalence of opioid use disorder and fatal opioid overdose from 2022 to 2032.
The SOURCE model draws on multiple data sources to replicate how risks of opioid misuse initiation and overdose have evolved over time in the United States and suggests how those risks may evolve in the future under specific conditions. The model is considered high-level and data-driven, and uses a systems dynamics approach of individuals transitioning through states of opioid use and opioid use disorder as well as treatment, remission, and stable remission. The model incorporates feedback loops that may influence these transition states. These feedback loops include social influence, perceived risk, treatment availability, and prescription opioid availability on the street. As an example of a feedback loop, an increase in the perceived risk of prescription opioids would be expected to decrease the number of people who begin misusing opioids. In addition to deriving some assumptions from epidemiological data, assumptions are also informed by interviews and close collaboration with subject matter experts. More detail on how the SOURCE model was developed, including assumptions built into the model, can be found here.
The 11 strategies applied to the SOURCE model and an example of each strategy include:
The model measured the impact of each strategy on both prevalence of opioid use disorder and fatal opioid overdose from 2022 to 2032. The model assumes that it will take 3 years for full implementation of each strategy and that the strategies are then fully sustained throughout the study period.
Because of the lack of documented effect sizes and the varying level of evidence across the 11 strategies, the model assumed an across-the-board 20% effect size for each strategy. However, given the evidence on the efficiency of naloxone (“Narcan”) distribution, a 20% effect size was assumed to translate into a real-world 10% increase in the probability of naloxone administration in the event of an overdose. Researchers also combined strategies to see which set of strategies might have the largest impact. More detail on the assumptions and parameters on the model can be found here.
It is important to note that these strategies as tested in the model are broad and evidence is still emerging on what are the most helpful ways (i.e., specific interventions) to accomplish these broader approaches to addressing the overdose crisis. For example, one strategy is to reduce the excess overdose risk associated with fentanyl. However, evidence is still lacking on how to best reduce this risk. Therefore, the model oftentimes will highlight the importance of a broad strategy, but much work still needs to be done to figure out the best way to realize this strategy in the real world. In other words, the model is not identifying specific types of interventions needed to address the opioid crisis. Rather, the model tests approaches where allocating resources into research and practice could be most helpful in identifying specific types of interventions that would have the maximal impact on reducing the prevalence of opioid use disorder and fatal opioid overdoses.
WHAT DID THIS STUDY FIND?
Recovery support most impactful on prevalence of opioid use disorder.
By 2032, the model projected a 5.2% and 5.4% decrease in the prevalence of opioid use disorder for the strategies of reducing the return to opioid use disorder and peer support, respectively, and this impact was gradual over the time period modelled. The model predicted that people returning to problematic opioid use after a year of remission would be a larger source for opioid use disorder prevalence than new cases, contributing to the large impact seen. The recovery support strategies also had a large impact on fatal opioid overdoses, with reduction of 5.7% and 6.1% by 2032 for the strategies of reducing the return to opioid use disorder and peer support, respectively.
Harm reduction strategies most impactful on number of fatal opioid overdoses.
By 2032, the models projected a 14.2% and 3.4% decrease in the prevalence of fatal opioid overdose for the fentanyl harm reduction strategy and increasing naloxone distribution to people who use opioids, respectively, and this impact was immediate after full implementation of these strategies (after 3 years or by 2025). The model predicted that the overdose harm reduction strategies led to a small increase in the prevalence of opioid use disorder because of the lives saved by these strategies.
Expanding buprenorphine treatment capacity only had impact in the short term.
Somewhat surprisingly, expanding buprenorphine treatment capacity had only a modest impact on the prevalence of opioid use disorder and fatal opioid overdose. Increasing the number of buprenorphine providers had no impact and increasing buprenorphine provider capacity had very little impact on the prevalence of opioid use disorder and a modest impact on fatal opioid overdoses, but only in the short term (i.e., first 3 years). These modest impacts are seen largely because the model predicted a decrease in opioid use disorder over time, and thus a decrease in the demand for treatment. In addition, the model accounts for a realistic number of patients that each buprenorphine prescriber can treat, and it is built into the model that most providers qualified to prescribe buprenorphine do not treat any patients.
The impact of prevention strategies took many years to materialize.
Some of the prevention strategies had an impact on the prevalence of opioid use disorder and fatal opioid overdose, but this impact was not seen until full implementation of the intervention (i.e., 3 years or 2025) and the impact increased gradually over time. Decreasing heroin initiation mainly had a gradual impact on fatal opioid overdoses, whereas reducing the number of people who receive an opioid prescription and reducing the development of opioid use disorder had a gradual impact on both the prevalence of opioid use disorder and fatal opioid overdoses.
A combination of strategies produced the largest impact on the prevalence of opioid use disorder and fatal opioid overdoses.
The largest impacts were realized when strategies were combined, although the effects of the strategies were found to be additive rather than synergistic (i.e., there were no multiplicative effects where the full impact is greater than the sum of each strategy’s impact). The most impactful set of strategies was combining the recovery support strategies, overdose harm reduction strategies, and the prevention strategies of reducing heroin initiation, the number of people who receive an opioid prescription, and the development of opioid use disorder. This set of strategies achieved a 29.9% reduction in fatal opioid overdoses and a 15.1% reduction in the prevalence of opioid use disorder by 2032.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This modelling study found that recovery support strategies had the largest impact on reducing the prevalence of opioid use disorder and overdose harm reduction strategies had the largest impact on decreasing fatal opioid overdoses, while, somewhat surprisingly, expanding buprenorphine treatment capacity had only a modest impact on decreasing fatal opioid overdoses and this impact was only present in the short term. The largest impact was seen when recovery support, overdose harm reduction, and prevention strategies were combined.
This is not the first modelling study to forecast the impact of policies and interventions to address the opioid crisis, which have consistently found that expanding access to treatment and increasing naloxone distribution are critical strategies. However, this is the first modelling study to include recovery support in the model.
Findings from this study show that recovery support strategies are essential in addressing the opioid crisis, especially in reducing the prevalence of opioid use disorder over time, by helping individuals stay in remission (i.e., preventing relapse).
Both the recovery support strategies that reduce return to active opioid use disorder and increase peer support were found to be equally effective in reducing the prevalence of opioid use disorder and fatal opioid overdose over the study period. Within these broad strategies, reducing return to active opioid use disorder might include policies and interventions that remove barriers to and enhance facilitators of improved functioning for people in remission, such as employment supports, housing stability assistance, and improved social role functioning. Peer support strategies might include mutual-help groups, recovery residences, and peer-based recovery community centers, and the model assumed a positive feedback loop serving as a proxy for the strengthening of the recovery community as more people with opioid use disorder move into remission. These findings suggest that the recovery community and recovery support services, an often-overlooked component of the treatment continuum for opioid use disorder, are critical in the national response to the opioid crisis and should be adequately funded as such. In addition, recovery capital, which captures improvements in many of these domains, might be an important measurement to incorporate in research studies on opioid use disorder treatment and recovery.
The model found that harm reduction strategies were critical in lowering fatal opioid overdoses, especially interventions that would reduce the excess overdose risk associated with fentanyl. Naloxone distribution is a known evidence-based strategy to reduce fatal opioid overdoses, although substantial expansion is needed to realize its potential. Evidence for types of fentanyl harm reduction strategies is emerging, with drug checking being one promising intervention in this domain, although it is unclear if these types of services could achieve the hypothetical 20% effect size used in the model. Rather, the impact of the broad strategy of fentanyl overdose harm reduction should be interpreted as the number of lives that could be saved if people who use, or may be exposed to, fentanyl could reduce their risk of overdose reliably. Therefore, more research into practices that could increase this reliability are warranted.
Findings from this modelling study are unique in that the impact of treatment expansion was modest and only impactful in the short term.
Reasons given for this modest impact include: most providers qualified to prescribe buprenorphine do not treat any patients with opioid use disorder, there will be capacity limitations for current buprenorphine prescribers especially if retention is increased, and there was a declining trend in the prevalence of opioid use disorder at the beginning of the study period that would translate into a decreasing demand for treatment. However, there is rigorous evidence that buprenorphine treatment saves lives and is a critical tool in addressing the opioid crisis. Therefore, findings from this modelling study do not necessarily discount the value of expanding treatment access but encourage us to think about innovative ways to expand treatment capacity (e.g., increase fee reimbursements, decrease administrative burden on providers) while also emphasizing potentially higher-impact strategies like harm reduction and recovery support. Notably, the strategy of reducing return to active opioid use disorder is considered a recovery support strategy, although strategies to improve long-term maintenance of medications, which are oftentimes delivered in treatment settings, are also likely to reduce return to active opioid use disorder.
The model suggests that certain prevention strategies are important, but their effects are likely to be gradual and over a longer horizon. Decreasing heroin initiation (with or without initial use of prescription opioids), which might include programs aimed at children and adolescents at risk of substance use, mainly had a gradual impact on fatal opioid overdoses. Reducing the number of people who receive an opioid prescription, such as policies and interventions that reduce the number of people initiating opioid use as well as using alternatives to opioids for conditions where opioids might be appropriate, had a gradual impact on both the prevalence of opioid use disorder and fatal opioid overdoses. Reducing the development of opioid use disorder among people misusing opioids had a gradual impact on both the prevalence of opioid use disorder and fatal opioid overdoses, and this broad strategy might include addressing factors that increase the risk of this transition, such as economic deprivation and mental health conditions. Overall, prevention strategies are necessary to prevent new cases of opioid misuse and opioid use disorder that put people at risk for opioid overdose.
Previous findings of modelling studies highlight the importance of a portfolio of policies and interventions to address the opioid crisis, and findings from this study corroborate this. Somewhat surprisingly, this model finds that including strategies to expand treatment is not as important, and that combining recovery support strategies, overdose harm reduction strategies, and the prevention strategies of reducing heroin initiation, the number of people who receive an opioid prescription, and the development of opioid use disorder led to the largest impact on the prevalence of opioid use disorder and fatal opioid overdose.
The SOURCE model itself, as well as this study that tests the impact of 11 strategies using the SOURCE model, make many assumptions due to gaps in the literature and rely on epidemiological data with significant limitations. Although the researchers incorporated expert interviews to improve their assumptions and made adjustments to address some of the limitations of the epidemiological data sources used, forecasting the future with these types of models is extremely difficult. In light of these limitations, the model, although not perfect, is still useful to inform policies and responses to the U.S. opioid crisis.
This is a US-specific national modelling study. Therefore, generalizing the model’s findings to states or regions in the U.S., as well as other countries, should be done with caution.
Only buprenorphine was used to measure expanding treatment capacity, although methadone and extended-release naltrexone are other medication options for opioid use disorder. Excluding these treatment options may have diminished the impact of treatment expansion in the model.
The model assumes that people who are prescribed opioids but do not misuse them are not at risk of developing opioid use disorder. Other studies have shown that chronic pain patients, who are often prescribed high doses of opioids over long durations, can develop opioid use disorder when taking the medication exactly as prescribed.
The opioid crisis has increasingly become a polysubstance and fentanyl crisis, where people with opioid use disorder more often than not are using several other substances and many overdose deaths are occurring in individuals without an opioid use disorder who are experimenting with counterfeit pills containing fentanyl. The model would likely have difficulty forecasting the impact of strategies given these recent developments.
Other factors that have driven the opioid crisis were not included in the SOURCE model, such as socioeconomic status, involvement in the criminal justice system, co-occurring mental health conditions, and trauma.
BOTTOM LINE
This study leverages the previously developed SOURCE model to project the impact of 11 strategies across the continuum of care – prevention, harm reduction, treatment, and recovery – on the prevalence of opioid use disorder and fatal opioid overdose from 2022 to 2032. Recovery support strategies had the largest impact on reducing the prevalence of opioid use disorder, and overdose harm reduction strategies had the largest impact on decreasing fatal opioid overdoses, while, somewhat surprisingly, expanding buprenorphine treatment capacity had an impact only on decreasing fatal opioid overdoses and this impact was only present in the short term. The largest impact was seen when recovery support, overdose harm reduction, and prevention strategies were combined.
For individuals and families seeking recovery: Although treatment with medications is emphasized as vital in helping individuals with opioid use disorder, this study shows that other strategies are just as important. For individuals who are actively using opioids, harm reduction strategies are critical for reducing overdose risk. For individuals who are in remission from opioid use disorder (e.g., finished a treatment program and/or stable on a medication), engagement in recovery support services and the recovery community in general could help them sustain remission and improve their quality of life.
For treatment professionals and treatment systems: Although treatment with medications is emphasized as vital in helping individuals with opioid use disorder, this study shows that other strategies are just as important. A treatment continuum that provides education on and access to harm reduction services is likely to reduce overdose risk for people who return to problematic substance use. Aftercare following treatment completion with a long horizon (i.e., 5 years after treatment initiation), which includes engagement in recovery support services and the recovery community in general, is likely to help clients sustain remission and improve their quality of life.
For scientists:In light of the limitations discussed above, this study that tests 11 different strategies using the SOURCE model, although not without limitations, is still useful to inform responses to the U.S. opioid crisis. The model uses a hypothetical effect size (20%) and broad strategies to identify areas where additional research might be fruitful. For example, harm reduction strategies to reduce fentanyl overdose risk is one area where additional research is warranted, as different types of drug checking are recently emerging as promising interventions to address an illicit drug supply contaminated with fentanyl. In addition, according to the model, recovery support services, such as those addressing housing, employment, and education, and peer support strategies, such as mutual aid, recovery community centers, and increasing the recovery community in general, will be critical in sustaining remission of opioid use disorder. Research into better understanding which types of interventions remove barriers to or enhance facilitators of improved functioning for people in remission are warranted.
For policy makers: The results of this study highlight the importance of a comprehensive response to the opioid crisis. Although treatment with medications is vital in helping individuals with opioid use disorder, other strategies may be just as important or even more important in pursuing. Supporting research for and implementation of harm reduction programs, especially those aimed at reducing the risk of fentanyl overdose, are critical in reducing opioid overdose deaths. Supporting research for and implementation of recovery support services, along with enhancing the overall impact of peer support delivered by the recovery community, are critical to helping people stay in remission from opioid use disorder and improve their quality of life. The best response to the opioid crisis will be a comprehensive set of strategies that involves the best policies and interventions to prevent new cases of opioid use disorder, reduce overdose risk, and get people with opioid use disorder into remission and sustain their remission over time.
In 2021, drug overdose deaths set another record with more than 108,000 Americans losing their lives to this preventable condition, a 50% increase from just 2 years ago. Overall, more than 1 million Americans have died of a drug overdose since 1999. These deaths have been driven by opioids, with the latest and worst wave of deaths involving illicitly manufactured fentanyl.
There has been a large investment in implementing policies and interventions to address this opioid overdose crisis, primarily aimed at reducing opioid prescribing, expanding access to medication treatment for opioid use disorder, and increasing the amount of naloxone (“Narcan”) in communities. Despite these efforts, the crisis continues to worsen.
Models that simulate future scenarios can be useful in helping policymakers identify the best strategies to pursue in the face of limited resources. Previously, a team of researchers developed SOURCE (Simulation of Opioid Use, Response, Consequences, and Effects), a model of the evolution of the opioid crisis in the United States that provides a basis for projecting and analyzing potential policy impacts and solutions. In this study, researchers used the SOURCE model to project the impact of 11 strategies, and combinations thereof, on the prevalence of opioid use disorder and fatal opioid overdoses from 2022 to 2032. These strategies represented interventions across the continuum of care – prevention, harm reduction, treatment, and recovery. Results from this simulated model could provide insight into which types of strategies are critical in turning the tide of the opioid crisis.
HOW WAS THIS STUDY CONDUCTED?
This study leverages the previously developed SOURCE model to project the impact of 11 strategies across the continuum of care – prevention, harm reduction, treatment, and recovery – on the prevalence of opioid use disorder and fatal opioid overdose from 2022 to 2032.
The SOURCE model draws on multiple data sources to replicate how risks of opioid misuse initiation and overdose have evolved over time in the United States and suggests how those risks may evolve in the future under specific conditions. The model is considered high-level and data-driven, and uses a systems dynamics approach of individuals transitioning through states of opioid use and opioid use disorder as well as treatment, remission, and stable remission. The model incorporates feedback loops that may influence these transition states. These feedback loops include social influence, perceived risk, treatment availability, and prescription opioid availability on the street. As an example of a feedback loop, an increase in the perceived risk of prescription opioids would be expected to decrease the number of people who begin misusing opioids. In addition to deriving some assumptions from epidemiological data, assumptions are also informed by interviews and close collaboration with subject matter experts. More detail on how the SOURCE model was developed, including assumptions built into the model, can be found here.
The 11 strategies applied to the SOURCE model and an example of each strategy include:
The model measured the impact of each strategy on both prevalence of opioid use disorder and fatal opioid overdose from 2022 to 2032. The model assumes that it will take 3 years for full implementation of each strategy and that the strategies are then fully sustained throughout the study period.
Because of the lack of documented effect sizes and the varying level of evidence across the 11 strategies, the model assumed an across-the-board 20% effect size for each strategy. However, given the evidence on the efficiency of naloxone (“Narcan”) distribution, a 20% effect size was assumed to translate into a real-world 10% increase in the probability of naloxone administration in the event of an overdose. Researchers also combined strategies to see which set of strategies might have the largest impact. More detail on the assumptions and parameters on the model can be found here.
It is important to note that these strategies as tested in the model are broad and evidence is still emerging on what are the most helpful ways (i.e., specific interventions) to accomplish these broader approaches to addressing the overdose crisis. For example, one strategy is to reduce the excess overdose risk associated with fentanyl. However, evidence is still lacking on how to best reduce this risk. Therefore, the model oftentimes will highlight the importance of a broad strategy, but much work still needs to be done to figure out the best way to realize this strategy in the real world. In other words, the model is not identifying specific types of interventions needed to address the opioid crisis. Rather, the model tests approaches where allocating resources into research and practice could be most helpful in identifying specific types of interventions that would have the maximal impact on reducing the prevalence of opioid use disorder and fatal opioid overdoses.
WHAT DID THIS STUDY FIND?
Recovery support most impactful on prevalence of opioid use disorder.
By 2032, the model projected a 5.2% and 5.4% decrease in the prevalence of opioid use disorder for the strategies of reducing the return to opioid use disorder and peer support, respectively, and this impact was gradual over the time period modelled. The model predicted that people returning to problematic opioid use after a year of remission would be a larger source for opioid use disorder prevalence than new cases, contributing to the large impact seen. The recovery support strategies also had a large impact on fatal opioid overdoses, with reduction of 5.7% and 6.1% by 2032 for the strategies of reducing the return to opioid use disorder and peer support, respectively.
Harm reduction strategies most impactful on number of fatal opioid overdoses.
By 2032, the models projected a 14.2% and 3.4% decrease in the prevalence of fatal opioid overdose for the fentanyl harm reduction strategy and increasing naloxone distribution to people who use opioids, respectively, and this impact was immediate after full implementation of these strategies (after 3 years or by 2025). The model predicted that the overdose harm reduction strategies led to a small increase in the prevalence of opioid use disorder because of the lives saved by these strategies.
Expanding buprenorphine treatment capacity only had impact in the short term.
Somewhat surprisingly, expanding buprenorphine treatment capacity had only a modest impact on the prevalence of opioid use disorder and fatal opioid overdose. Increasing the number of buprenorphine providers had no impact and increasing buprenorphine provider capacity had very little impact on the prevalence of opioid use disorder and a modest impact on fatal opioid overdoses, but only in the short term (i.e., first 3 years). These modest impacts are seen largely because the model predicted a decrease in opioid use disorder over time, and thus a decrease in the demand for treatment. In addition, the model accounts for a realistic number of patients that each buprenorphine prescriber can treat, and it is built into the model that most providers qualified to prescribe buprenorphine do not treat any patients.
The impact of prevention strategies took many years to materialize.
Some of the prevention strategies had an impact on the prevalence of opioid use disorder and fatal opioid overdose, but this impact was not seen until full implementation of the intervention (i.e., 3 years or 2025) and the impact increased gradually over time. Decreasing heroin initiation mainly had a gradual impact on fatal opioid overdoses, whereas reducing the number of people who receive an opioid prescription and reducing the development of opioid use disorder had a gradual impact on both the prevalence of opioid use disorder and fatal opioid overdoses.
A combination of strategies produced the largest impact on the prevalence of opioid use disorder and fatal opioid overdoses.
The largest impacts were realized when strategies were combined, although the effects of the strategies were found to be additive rather than synergistic (i.e., there were no multiplicative effects where the full impact is greater than the sum of each strategy’s impact). The most impactful set of strategies was combining the recovery support strategies, overdose harm reduction strategies, and the prevention strategies of reducing heroin initiation, the number of people who receive an opioid prescription, and the development of opioid use disorder. This set of strategies achieved a 29.9% reduction in fatal opioid overdoses and a 15.1% reduction in the prevalence of opioid use disorder by 2032.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This modelling study found that recovery support strategies had the largest impact on reducing the prevalence of opioid use disorder and overdose harm reduction strategies had the largest impact on decreasing fatal opioid overdoses, while, somewhat surprisingly, expanding buprenorphine treatment capacity had only a modest impact on decreasing fatal opioid overdoses and this impact was only present in the short term. The largest impact was seen when recovery support, overdose harm reduction, and prevention strategies were combined.
This is not the first modelling study to forecast the impact of policies and interventions to address the opioid crisis, which have consistently found that expanding access to treatment and increasing naloxone distribution are critical strategies. However, this is the first modelling study to include recovery support in the model.
Findings from this study show that recovery support strategies are essential in addressing the opioid crisis, especially in reducing the prevalence of opioid use disorder over time, by helping individuals stay in remission (i.e., preventing relapse).
Both the recovery support strategies that reduce return to active opioid use disorder and increase peer support were found to be equally effective in reducing the prevalence of opioid use disorder and fatal opioid overdose over the study period. Within these broad strategies, reducing return to active opioid use disorder might include policies and interventions that remove barriers to and enhance facilitators of improved functioning for people in remission, such as employment supports, housing stability assistance, and improved social role functioning. Peer support strategies might include mutual-help groups, recovery residences, and peer-based recovery community centers, and the model assumed a positive feedback loop serving as a proxy for the strengthening of the recovery community as more people with opioid use disorder move into remission. These findings suggest that the recovery community and recovery support services, an often-overlooked component of the treatment continuum for opioid use disorder, are critical in the national response to the opioid crisis and should be adequately funded as such. In addition, recovery capital, which captures improvements in many of these domains, might be an important measurement to incorporate in research studies on opioid use disorder treatment and recovery.
The model found that harm reduction strategies were critical in lowering fatal opioid overdoses, especially interventions that would reduce the excess overdose risk associated with fentanyl. Naloxone distribution is a known evidence-based strategy to reduce fatal opioid overdoses, although substantial expansion is needed to realize its potential. Evidence for types of fentanyl harm reduction strategies is emerging, with drug checking being one promising intervention in this domain, although it is unclear if these types of services could achieve the hypothetical 20% effect size used in the model. Rather, the impact of the broad strategy of fentanyl overdose harm reduction should be interpreted as the number of lives that could be saved if people who use, or may be exposed to, fentanyl could reduce their risk of overdose reliably. Therefore, more research into practices that could increase this reliability are warranted.
Findings from this modelling study are unique in that the impact of treatment expansion was modest and only impactful in the short term.
Reasons given for this modest impact include: most providers qualified to prescribe buprenorphine do not treat any patients with opioid use disorder, there will be capacity limitations for current buprenorphine prescribers especially if retention is increased, and there was a declining trend in the prevalence of opioid use disorder at the beginning of the study period that would translate into a decreasing demand for treatment. However, there is rigorous evidence that buprenorphine treatment saves lives and is a critical tool in addressing the opioid crisis. Therefore, findings from this modelling study do not necessarily discount the value of expanding treatment access but encourage us to think about innovative ways to expand treatment capacity (e.g., increase fee reimbursements, decrease administrative burden on providers) while also emphasizing potentially higher-impact strategies like harm reduction and recovery support. Notably, the strategy of reducing return to active opioid use disorder is considered a recovery support strategy, although strategies to improve long-term maintenance of medications, which are oftentimes delivered in treatment settings, are also likely to reduce return to active opioid use disorder.
The model suggests that certain prevention strategies are important, but their effects are likely to be gradual and over a longer horizon. Decreasing heroin initiation (with or without initial use of prescription opioids), which might include programs aimed at children and adolescents at risk of substance use, mainly had a gradual impact on fatal opioid overdoses. Reducing the number of people who receive an opioid prescription, such as policies and interventions that reduce the number of people initiating opioid use as well as using alternatives to opioids for conditions where opioids might be appropriate, had a gradual impact on both the prevalence of opioid use disorder and fatal opioid overdoses. Reducing the development of opioid use disorder among people misusing opioids had a gradual impact on both the prevalence of opioid use disorder and fatal opioid overdoses, and this broad strategy might include addressing factors that increase the risk of this transition, such as economic deprivation and mental health conditions. Overall, prevention strategies are necessary to prevent new cases of opioid misuse and opioid use disorder that put people at risk for opioid overdose.
Previous findings of modelling studies highlight the importance of a portfolio of policies and interventions to address the opioid crisis, and findings from this study corroborate this. Somewhat surprisingly, this model finds that including strategies to expand treatment is not as important, and that combining recovery support strategies, overdose harm reduction strategies, and the prevention strategies of reducing heroin initiation, the number of people who receive an opioid prescription, and the development of opioid use disorder led to the largest impact on the prevalence of opioid use disorder and fatal opioid overdose.
The SOURCE model itself, as well as this study that tests the impact of 11 strategies using the SOURCE model, make many assumptions due to gaps in the literature and rely on epidemiological data with significant limitations. Although the researchers incorporated expert interviews to improve their assumptions and made adjustments to address some of the limitations of the epidemiological data sources used, forecasting the future with these types of models is extremely difficult. In light of these limitations, the model, although not perfect, is still useful to inform policies and responses to the U.S. opioid crisis.
This is a US-specific national modelling study. Therefore, generalizing the model’s findings to states or regions in the U.S., as well as other countries, should be done with caution.
Only buprenorphine was used to measure expanding treatment capacity, although methadone and extended-release naltrexone are other medication options for opioid use disorder. Excluding these treatment options may have diminished the impact of treatment expansion in the model.
The model assumes that people who are prescribed opioids but do not misuse them are not at risk of developing opioid use disorder. Other studies have shown that chronic pain patients, who are often prescribed high doses of opioids over long durations, can develop opioid use disorder when taking the medication exactly as prescribed.
The opioid crisis has increasingly become a polysubstance and fentanyl crisis, where people with opioid use disorder more often than not are using several other substances and many overdose deaths are occurring in individuals without an opioid use disorder who are experimenting with counterfeit pills containing fentanyl. The model would likely have difficulty forecasting the impact of strategies given these recent developments.
Other factors that have driven the opioid crisis were not included in the SOURCE model, such as socioeconomic status, involvement in the criminal justice system, co-occurring mental health conditions, and trauma.
BOTTOM LINE
This study leverages the previously developed SOURCE model to project the impact of 11 strategies across the continuum of care – prevention, harm reduction, treatment, and recovery – on the prevalence of opioid use disorder and fatal opioid overdose from 2022 to 2032. Recovery support strategies had the largest impact on reducing the prevalence of opioid use disorder, and overdose harm reduction strategies had the largest impact on decreasing fatal opioid overdoses, while, somewhat surprisingly, expanding buprenorphine treatment capacity had an impact only on decreasing fatal opioid overdoses and this impact was only present in the short term. The largest impact was seen when recovery support, overdose harm reduction, and prevention strategies were combined.
For individuals and families seeking recovery: Although treatment with medications is emphasized as vital in helping individuals with opioid use disorder, this study shows that other strategies are just as important. For individuals who are actively using opioids, harm reduction strategies are critical for reducing overdose risk. For individuals who are in remission from opioid use disorder (e.g., finished a treatment program and/or stable on a medication), engagement in recovery support services and the recovery community in general could help them sustain remission and improve their quality of life.
For treatment professionals and treatment systems: Although treatment with medications is emphasized as vital in helping individuals with opioid use disorder, this study shows that other strategies are just as important. A treatment continuum that provides education on and access to harm reduction services is likely to reduce overdose risk for people who return to problematic substance use. Aftercare following treatment completion with a long horizon (i.e., 5 years after treatment initiation), which includes engagement in recovery support services and the recovery community in general, is likely to help clients sustain remission and improve their quality of life.
For scientists:In light of the limitations discussed above, this study that tests 11 different strategies using the SOURCE model, although not without limitations, is still useful to inform responses to the U.S. opioid crisis. The model uses a hypothetical effect size (20%) and broad strategies to identify areas where additional research might be fruitful. For example, harm reduction strategies to reduce fentanyl overdose risk is one area where additional research is warranted, as different types of drug checking are recently emerging as promising interventions to address an illicit drug supply contaminated with fentanyl. In addition, according to the model, recovery support services, such as those addressing housing, employment, and education, and peer support strategies, such as mutual aid, recovery community centers, and increasing the recovery community in general, will be critical in sustaining remission of opioid use disorder. Research into better understanding which types of interventions remove barriers to or enhance facilitators of improved functioning for people in remission are warranted.
For policy makers: The results of this study highlight the importance of a comprehensive response to the opioid crisis. Although treatment with medications is vital in helping individuals with opioid use disorder, other strategies may be just as important or even more important in pursuing. Supporting research for and implementation of harm reduction programs, especially those aimed at reducing the risk of fentanyl overdose, are critical in reducing opioid overdose deaths. Supporting research for and implementation of recovery support services, along with enhancing the overall impact of peer support delivered by the recovery community, are critical to helping people stay in remission from opioid use disorder and improve their quality of life. The best response to the opioid crisis will be a comprehensive set of strategies that involves the best policies and interventions to prevent new cases of opioid use disorder, reduce overdose risk, and get people with opioid use disorder into remission and sustain their remission over time.