Re-wiring young minds online: Can web-based cognitive bias modification reduce social anxiety and alcohol use among young adults?
Social anxiety and alcohol use disorder are two pressing public health concerns for young adults. For some, these conditions are both present and exacerbate one another, driven by underlying cognitive biases. This pilot study evaluated the feasibility, acceptability, and effectiveness of cognitive bias modification to address co-occurring social anxiety and hazardous alcohol use in young adults.
One way of framing this set of challenges is that both social anxiety and alcohol use disorder are at least in part driven by underlying modifiable cognitive biases, specifically interpretation biases in social anxiety and alcohol approach biases in alcohol use disorder. Interpretation bias modification aims to alter negative interpretations of ambiguous situations or information, which can contribute to social anxiety, by training individuals to resolve these situations in a more positive or neutral manner. Alcohol approach bias modification is geared towards reducing alcohol-related cravings and desire by training participants to repeatedly avoid alcohol-related cues (e.g., by pushing away a computer mouse when an image of an alcoholic beverage is displayed). There is evidence suggesting cognitive bias modification training, including interpretation bias modification and approach bias modification, can be effective at reducing these biases and associated symptoms. Prior studies have also shown that these cognitive bias modification interventions, particularly when combined with standard treatment like CBT, can significantly reduce anxiety symptoms and increase rates of alcohol abstinence. However, studies have collectively produced mixed results and evidence supporting the effectiveness of cognitive bias modification interventions as a stand-alone treatment for nonclinical samples is limited.
With recent shifting preferences for digital technology, especially among younger audiences, there have been increased efforts to deliver interpretation bias modification and approach bias modification interventions via web-based and app-based formats, which may have the potential to offer scalable treatments at rather low cost. Initial findings indicate that these online delivery methods have resulted in good uptake and adherence to online training sessions, though study drop-out (i.e., attrition) remains a concern. Early studies examining their utility suggest there is potential for these digital cognitive bias modification interventions to reduce cognitive biases, and in turn, social anxiety symptoms and alcohol cravings and consumption. However, existing studies have primarily focused on anxiety interpretation bias modification and alcohol approach bias modification programs in isolation of one another. The potential for combining these two web-based cognitive bias modification interventions warrants further investigation, particularly for young adults with comorbid conditions. This pilot RCT evaluated the feasibility, acceptability, and preliminary efficacy of a web-based cognitive bias modification intervention combining interpretation bias modification and approach bias modification as an adjunctive treatment for young adults with co-morbid social anxiety and hazardous alcohol use.
HOW WAS THIS STUDY CONDUCTED?
This was a 3-arm pilot randomized control trial conducted in an online setting in Australia. Participants were recruited via a combination of methods (e.g., paid social media advertisements, flyers at educational institutions) from March 2021 to July 2022. Upon registering for the study on the study website, participants were asked to complete an online screener to determine eligibility status followed by a longer initial survey. In order to be eligible, participants had to: 1) be Australian, 2) be between 18-30 years old, 3) report current hazardous alcohol use, 4) report currently experiencing at least mild social anxiety symptoms, 5) have access to internet and mouse-operable PC or laptop, 6) be receiving psychological treatment for anxiety, alcohol use problems, or both, and 7) be willing to complete intervention components. A total of 100 eligible participants were randomized to either 1) integrated intervention plus treatment-as-usual (each session split in half to include both interpretation bias modification + approach bias modification; n = 35), 2) alternating intervention plus treatment-as-usual (each session focused on interpretation bias modification or approach bias modification in alternating pattern; n = 32), or 3) treatment-as-usual control group (i.e., receiving psychological treatment from a mental health professional for anxiety, alcohol use problems, or both; n = 33).
The Re-Train Your Brain intervention incorporating interpretation bias modification and alcohol approach bias modification was delivered alongside participants’ treatment as usual in both intervention groups. The Re-Train Your Brain intervention consisted of 10 online 20-minute sessions to be completed across five weeks (2 per week). Before beginning the training sessions, participants had to complete a web-based psychoeducational alcohol-anxiety module explaining the link between anxiety and alcohol use, cognitive biases, and the importance of changing these biases.
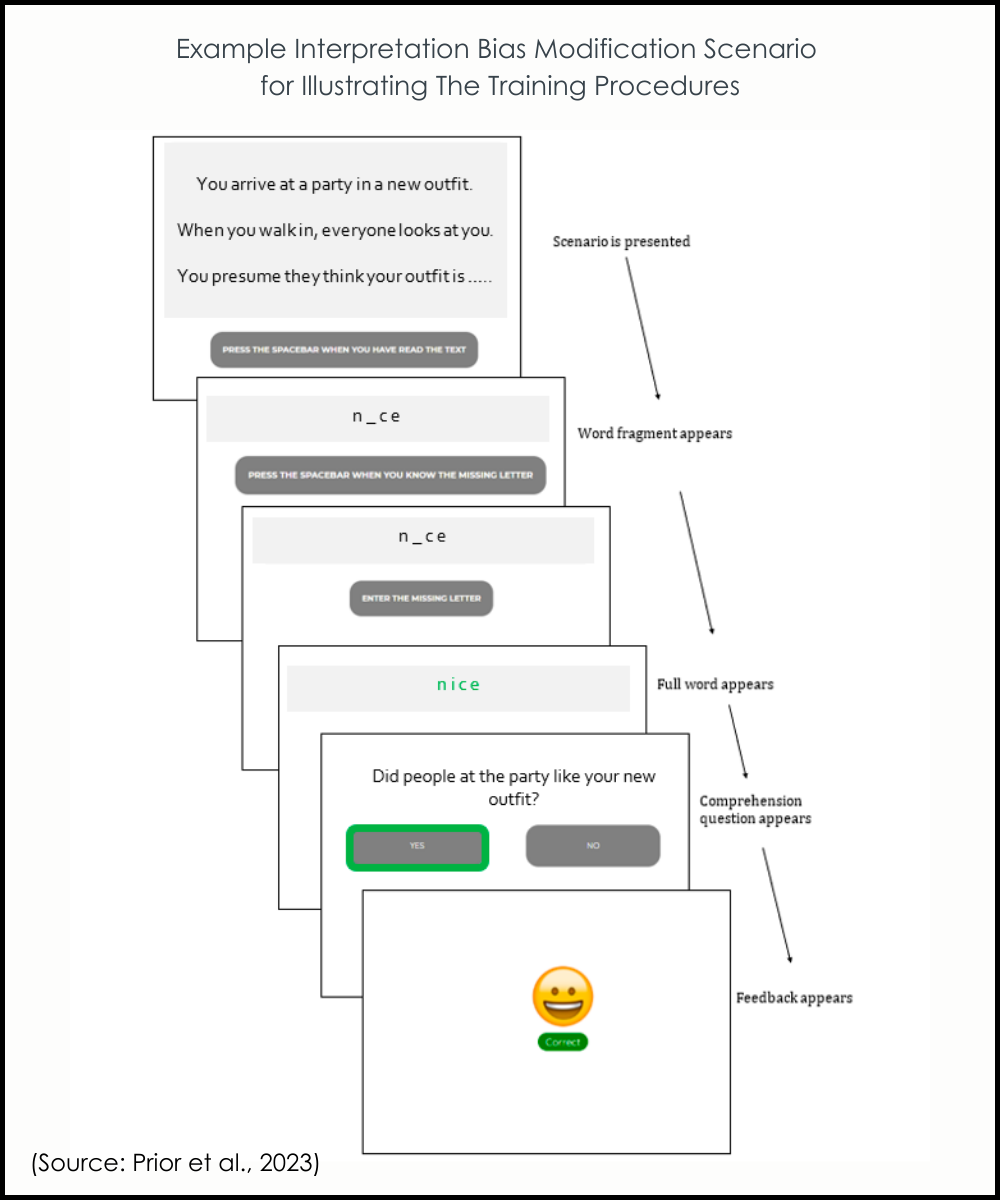
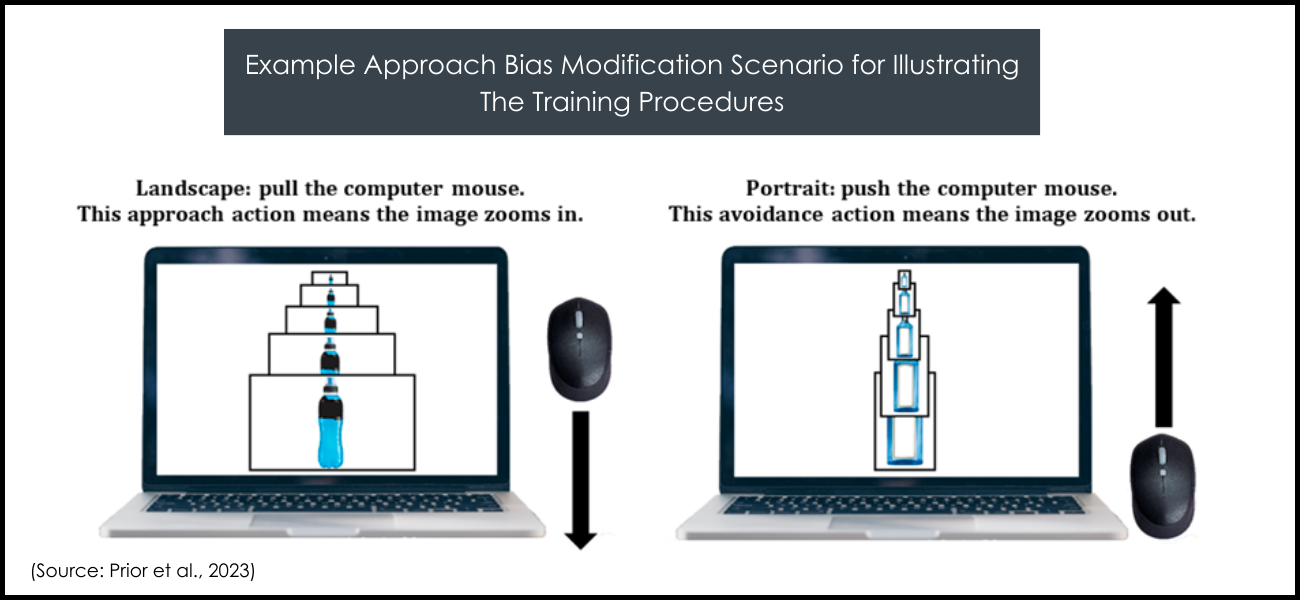
The interpretation bias component of the Re-Train Your Brain intervention involved presenting ambiguous social scenarios to participants and requesting for them to complete word fragments in a positive or neutral manner. Comprehension questions after each social scenario were answered and points were awarded for correct answers to enhance engagement. For alcohol approach bias modification designed to modify participants’ response to alcohol-related cues, participants were instructed to react to images of alcoholic and nonalcoholic drinks by pulling or pushing a computer mouse, causing the image size to increase or decrease accordingly. Positive feedback and points were awarded for correct responses. The Re-Train Your Brain intervention was delivered in two formats alongside treatment-as-usual: integrated and alternating. Both formats consisted of the same treatment dose. In the integrated treatment group, participants completed 10 online training sessions combining shortened versions of both types of training within each session. The alternating treatment group also consisted of 10 online training sessions but each session consisted of only one type of training in alternating order. The treatment-as-usual control group received their usual treatment from their clinical provider and were placed on a waitlist to access the intervention after the study period.
Primary outcomes, including feasibility of the research and intervention and acceptability of the intervention, were assessed at 6 weeks after baseline. Secondary outcomes were assessed at 6 and 12 weeks after baseline and included cognitive biases (social anxiety interpretation biases, alcohol approach biases, comorbid interpretation biases for social anxiety and alcohol use), social anxiety disorder symptoms, and alcohol-related outcomes (hazardous alcohol use, alcohol consumption, alcohol dependence, alcohol cravings). Comorbid interpretation biases for social anxiety and alcohol assess the extent to which individuals presented with an ambiguous situation that has several possible explanations choose the option that link alcohol use with social concerns. It was hypothesized that both formats of the intervention would be feasible to implement and deemed acceptable by young adults. Additionally, both intervention conditions in combination with their existing therapy were hypothesized to result in greater improvements cognitive biases, anxiety symptoms, and alcohol-related outcomes, compared with therapy only. Finally, the integrated intervention format was hypothesized to be more engaging and to produce larger improvements than the alternating intervention format.
Participants in the study were primarily female (76%), in their mid-20s (Mean age = 26.4), well-educated (54%), and employed (72%). The majority of participants (54%) reported generalized anxiety as their primary concern, while fewer (34%) reported social anxiety as their main concern. A large proportion of participants reported high levels of social anxiety (70%) and 61% had AUDIT scores consistent with “probable alcohol dependence” at baseline. All participants in the study were receiving treatment from for their anxiety, alcohol use, or both, considered “treatment as usual”. Participants most often reported seeing general practitioners (63%), psychologists (49%), clinical psychologists (22%), and counselors (21%).
WHAT DID THIS STUDY FIND?
Both formats of the intervention were feasible and acceptable.
At 6 weeks after baseline, 75% of participants completed the survey and 71% completed the cognitive assessment. Completion rates at 6 weeks after baseline were lower for the alternating intervention group compared to the control group. At 12 weeks after baseline, 67% of participants completed the survey, and 62% completed the cognitive assessment. Completion rate of at least one follow-up was significantly higher in the control group compared to the alternating intervention group. Only 4% of participants withdrew from the study.
In terms of intervention feasibility, 76% across both the integrated and alternating intervention groups completed the initial psychoeducational anxiety-alcohol module. A large proportion (81%) of these participants also completed at least 1 of 10 ten training sessions, almost half (49%) completed the optimum number of 6 training sessions, and more than one in three (37%) completed all 10 training sessions. There were no differences between the integrated and alternating intervention groups on number of training sessions completed.
Interventions were acceptable in some respects, but not others.
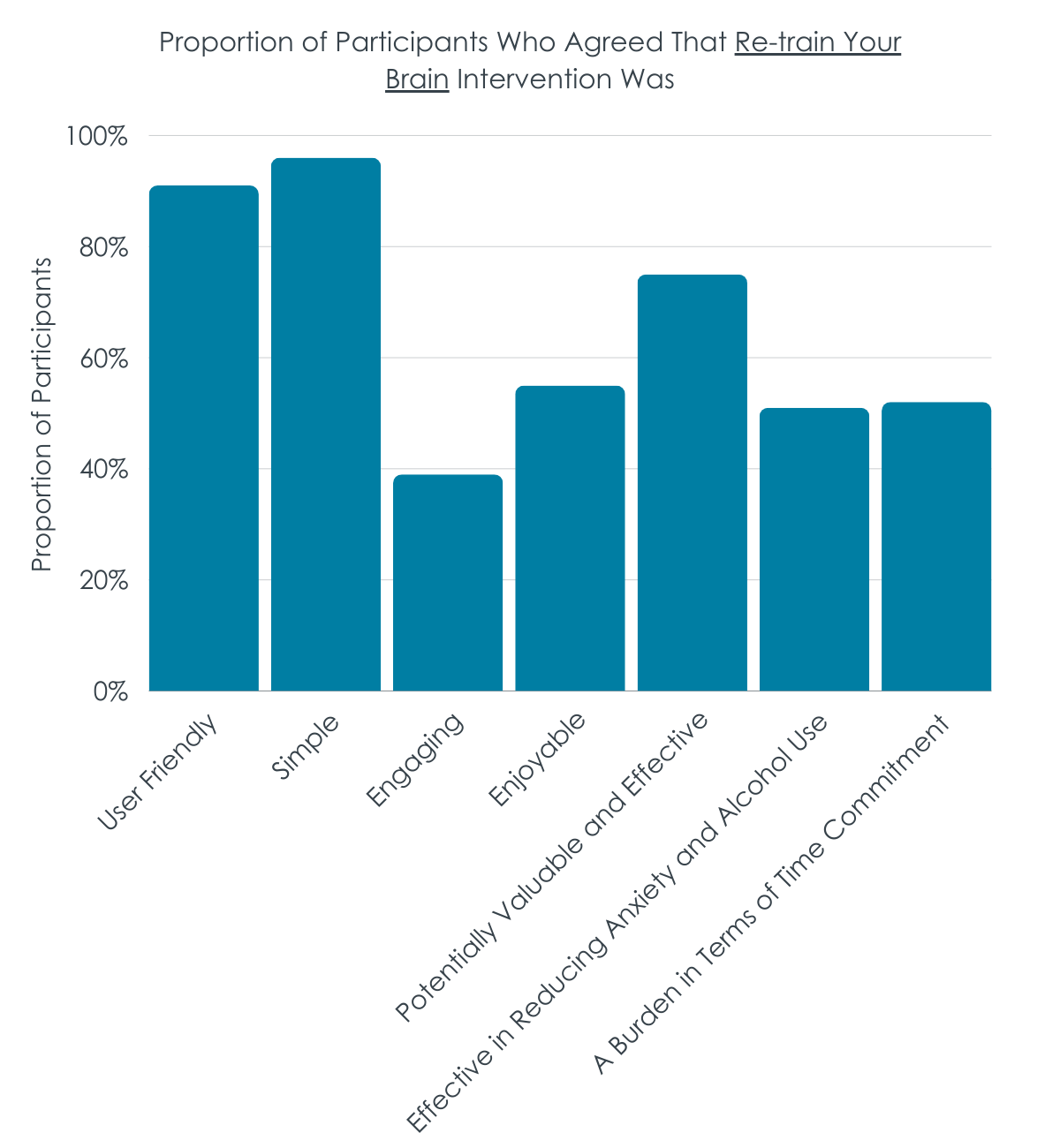
Across both intervention groups, most (88%) found the Re-Train Your Brain program to be acceptable, user friendly (91%), simple (96%), and easy to complete (91%). Most participants also agreed that they perceived the potential value and effectiveness of the intervention (75%). On the other hand, there were mixed views related to other acceptability measures; about half or less of participants found the intervention enjoyable (55%), motivating (43%), engaging (39%), and likely to be effective in reducing anxiety and alcohol use (52%). About half of participants (51%) also found the intervention to a burden in terms of the time commitment. The alternating intervention group was rated as simpler and more user-friendly when compared to the integrated group.
Intervention participants improved anxiety interpretation biases, but not alcohol approach biases.
Participants in both intervention groups showed large reductions in anxiety interpretation biases from baseline to 6 weeks, and moderate to large reductions from baseline to 12 weeks. The control group did not exhibit changes in interpretation biases over time. When compared to control, both intervention formats were associated with a greater reduction in interpretation biases from baseline to 6 weeks, but these differences in changes did not sustain until 12 weeks. There were no substantial differences between the integrated and alternating intervention groups on interpretation biases. Also, there were no changes over time or differences between groups on alcohol approach biases or non-alcohol approach biases. All groups experienced small to moderate reductions in comorbid interpretation biases at 6 weeks, and these reductions remained at 12 weeks for both intervention groups but were not sustained by the control group. Reductions in comorbid interpretation biases at 12 weeks for the intervention groups were greater than those in the control group. Reductions in comorbid interpretation biases over time, however, were comparable between the integrated and alternating intervention groups.
Intervention groups with greater reductions on social anxiety symptoms, hazardous drinking, and alcohol cravings.
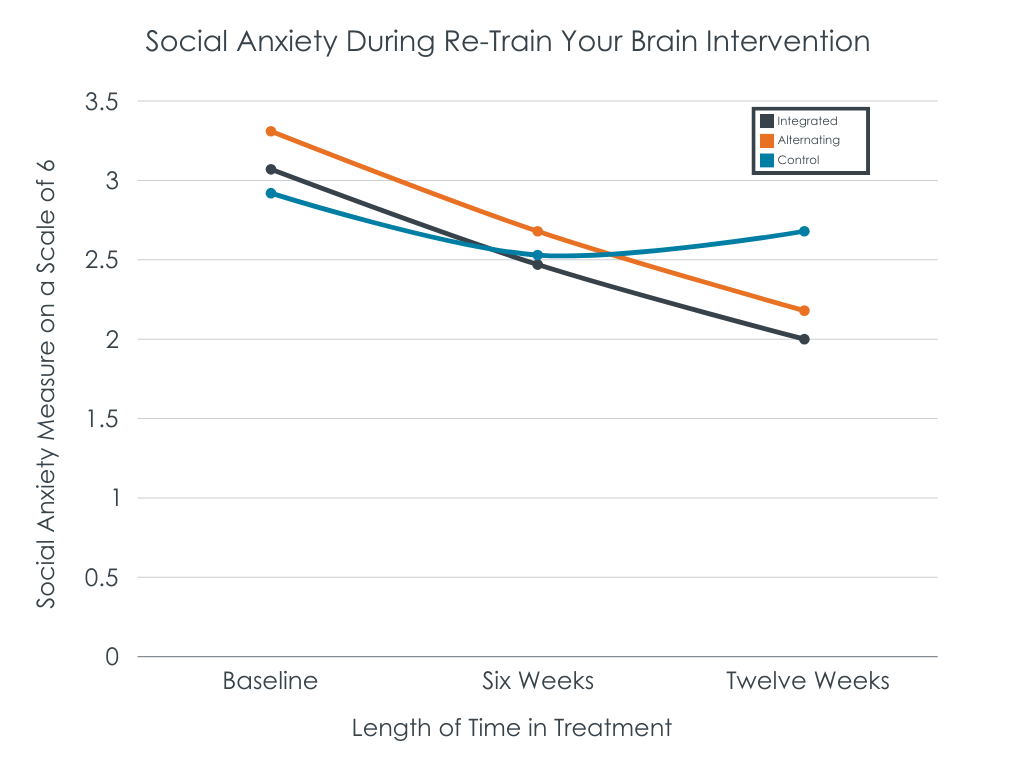
On social anxiety symptoms, only the alternating intervention group showed reductions between baseline and 12-week follow-up that were small to moderate in magnitude. Reductions on hazardous drinking were descriptively greater in the intervention groups relative to control, though the difference was not large enough in this small pilot study to reach statistical significance. Compared to the control group, the alternating intervention – but not the integrated intervention – had greater reduction in alcohol craving at the 6-week follow-up. All three groups had similar levels of alcohol craving, however, by the 12-week follow-up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Both formats of the Re-Train Your Brain intervention were feasible to implement and were acceptable by young adults with social anxiety and hazardous drinking, indicating suitability for this age group. This is in line with other research supporting the feasibility and acceptability of delivering cognitive bias modification interventions in digital formats, especially among younger age groups. Nevertheless, results from this study indicate a need for improvement with regard to enhancing participant retention and engagement and adherence to the Re-Train Your Brain intervention, an oft-cited issue in the digital mental health intervention literature. This area of investigation remains critical in order to maximize the effectiveness of digital cognitive bias modification interventions.
This pilot study’s findings that interpretation bias modification and approach bias modification may help to reduce cognitive biases, anxiety symptoms, and alcohol use outcomes aligns with prior research on the effectiveness of cognitive bias modification training to lead to improvements in psychological symptoms. More specifically, this web-based cognitive bias modification intervention incorporating both interpretation bias modification and alcohol approach bias modification, when combined with each participant’s therapy in the community, resulted in greater improvements in anxiety interpretation biases and comorbid interpretation biases when compared to therapy alone. Both formats – the integrated and the alternating session models – were shown to be equally helpful. Of note, however, participants found the alternating model simpler and more user-friendly. It may be that combining training approaches in one session adds complexity rather than its intended purpose of enhancing engagement.
Given the web-based and low-threshold nature of this digital intervention, the Re-Train Your Brain intervention could potentially represent a low-cost and scalable adjunctive treatment for co-occurring social anxiety and alcohol use disorder among young adults. However, given this was a pilot study using a small sample size, results are to be interpreted with caution. Larger randomized control trials testing the efficacy of this cognitive bias modification intervention among a diverse sample of young adults are needed. If the intervention is proven to be a helpful treatment option for young adults with comorbid social anxiety and alcohol use disorder in real-world settings, there is potential for societal benefit.
This was a pilot study and these findings should be considered preliminary, to be tested in larger randomized control trials to see if these findings are replicated.
Most participants reported “generalized anxiety” as their main clinical concern with few participants specifically reporting social anxiety as their primary concern. Although participants all met the threshold for hazardous drinking on the AUDIT, one-third of participants had not consumed any alcohol in the past month at baseline. Additionally, this intervention was delivered online and may not be as effective or accessible for individuals with limited access to technology or low digital literacy. Each of these factors might limit generalizability to all individuals with co-occurring social anxiety and hazardous drinking.
The researchers did not prespecify feasibility and acceptability benchmarks, limiting interpretation of the intervention’s successful implementation.
Participants had to be currently receiving treatment from mental health professionals for their anxiety, alcohol use, or both to be included in the study and this variable was used to indicate receipt of treatment-as-usual. However, the researchers did not standardize the type of therapy received by participants. Thus it is unclear to what the cognitive bias modification interventions are being compared.
BOTTOM LINE
Preliminary results from this small pilot study evaluating a web-based interpretation bias modification and alcohol approach bias modification cognitive retraining intervention show that the intervention is feasible and acceptable for young adults in Australia with comorbid social anxiety and hazardous alcohol use. The format where each session consisted of one type of retraining – rather than one where the trainings were integrated – may have been simpler and more user-friendly, however. The intervention showed promise for different types of anxiety interpretation biases, as well as reducing social anxiety symptoms and alcohol cravings. Larger clinical trials are needed to more rigorously test for the efficacy of the intervention in terms of reducing cognitive biases, social anxiety symptoms, and alcohol-related outcomes among young adults with co-occurring social anxiety disorder and hazardous drinking.
For individuals and families seeking recovery: For co-occurring social anxiety and hazardous drinking, the web-based Re-Train Your Brain cognitive bias modification intervention appears to be an acceptable format for young adults and may prove a beneficial supplement to standard treatment provided by a health professional. This web-based cognitive bias modification intervention shows potential for reducing anxiety and comorbid interpretation biases, which may play an underlying role in managing social anxiety and alcohol use disorder, though further research is needed to properly evaluate the large-scale efficacy of the intervention. Additionally, being a web-based intervention, Re-Train Your Brain could present a low- or no-cost option that can be accessed remotely and easily incorporated into one’s recovery process.
For treatment professionals and treatment systems: Substance use treatment professionals may consider incorporating digital tools, such as the Re-Train Your Brain program, to be used alongside traditional therapies for young adults with co-occurring social anxiety and hazardous alcohol use. Such tools may offer appeal to young adults, given their comfort with technology and receptivity to digital interventions. Online programs can also serve to cut through common barriers related to treatment accessibility (e.g., cost, geography, transportation), as these interventions can be administered remotely in contexts with limited mental health resources. This study also highlights the role of cognitive bias modification in treating comorbid anxiety and alcohol use among young adults. While treatment systems might benefit from incorporating interpretation bias modification and alcohol approach bias modification approaches as adjunctive treatments, more research is needed to examine the cost-effectiveness of these approaches.
For scientists: This study adds to evidence supporting the potential for cognitive bias modification interventions to be used as adjunctive treatments for anxiety and alcohol use alongside standard treatment and highlights the importance of continuing to address comorbidity in mental health research. The study also underscores the potential and need to further explore digital mental health solutions, especially among young adults who are particularly receptive to digital intervention formats. The preliminary nature of this study limits interpretation of results but provides a strong basis for the need to conduct a larger, more comprehensive randomized control trial to evaluate the long-term efficacy for the web-based Re-Train Your Brain intervention to reduce cognitive biases, social anxiety, and alcohol-related outcomes. User engagement and retention in digital interventions, including in this pilot study, remain an important area of investigation if the effectiveness of these programs is to be maximized.
For policy makers: The potential for digital cognitive bias modification interventions to help individuals suffering from comorbid social anxiety and alcohol use disorder warrants support for funding initiatives to support this line of research. More funding in this area would help to address the complexities of comorbid mental health conditions and support the development and implementation of online interventions that can serve to cut across commonly cited barriers to in-person treatment offerings. Similar to in-person treatment offerings, individuals may have difficulty navigating treatment resources and identifying evidence-based treatment services in their area. As the number of digital mental health offerings continues to grow, it will be vital to develop standards and regulations to ensure their efficacy and safety, and to provide resources to communicate about and increase public awareness of the availability and effectiveness of evidence-based digital mental health services.
One way of framing this set of challenges is that both social anxiety and alcohol use disorder are at least in part driven by underlying modifiable cognitive biases, specifically interpretation biases in social anxiety and alcohol approach biases in alcohol use disorder. Interpretation bias modification aims to alter negative interpretations of ambiguous situations or information, which can contribute to social anxiety, by training individuals to resolve these situations in a more positive or neutral manner. Alcohol approach bias modification is geared towards reducing alcohol-related cravings and desire by training participants to repeatedly avoid alcohol-related cues (e.g., by pushing away a computer mouse when an image of an alcoholic beverage is displayed). There is evidence suggesting cognitive bias modification training, including interpretation bias modification and approach bias modification, can be effective at reducing these biases and associated symptoms. Prior studies have also shown that these cognitive bias modification interventions, particularly when combined with standard treatment like CBT, can significantly reduce anxiety symptoms and increase rates of alcohol abstinence. However, studies have collectively produced mixed results and evidence supporting the effectiveness of cognitive bias modification interventions as a stand-alone treatment for nonclinical samples is limited.
With recent shifting preferences for digital technology, especially among younger audiences, there have been increased efforts to deliver interpretation bias modification and approach bias modification interventions via web-based and app-based formats, which may have the potential to offer scalable treatments at rather low cost. Initial findings indicate that these online delivery methods have resulted in good uptake and adherence to online training sessions, though study drop-out (i.e., attrition) remains a concern. Early studies examining their utility suggest there is potential for these digital cognitive bias modification interventions to reduce cognitive biases, and in turn, social anxiety symptoms and alcohol cravings and consumption. However, existing studies have primarily focused on anxiety interpretation bias modification and alcohol approach bias modification programs in isolation of one another. The potential for combining these two web-based cognitive bias modification interventions warrants further investigation, particularly for young adults with comorbid conditions. This pilot RCT evaluated the feasibility, acceptability, and preliminary efficacy of a web-based cognitive bias modification intervention combining interpretation bias modification and approach bias modification as an adjunctive treatment for young adults with co-morbid social anxiety and hazardous alcohol use.
HOW WAS THIS STUDY CONDUCTED?
This was a 3-arm pilot randomized control trial conducted in an online setting in Australia. Participants were recruited via a combination of methods (e.g., paid social media advertisements, flyers at educational institutions) from March 2021 to July 2022. Upon registering for the study on the study website, participants were asked to complete an online screener to determine eligibility status followed by a longer initial survey. In order to be eligible, participants had to: 1) be Australian, 2) be between 18-30 years old, 3) report current hazardous alcohol use, 4) report currently experiencing at least mild social anxiety symptoms, 5) have access to internet and mouse-operable PC or laptop, 6) be receiving psychological treatment for anxiety, alcohol use problems, or both, and 7) be willing to complete intervention components. A total of 100 eligible participants were randomized to either 1) integrated intervention plus treatment-as-usual (each session split in half to include both interpretation bias modification + approach bias modification; n = 35), 2) alternating intervention plus treatment-as-usual (each session focused on interpretation bias modification or approach bias modification in alternating pattern; n = 32), or 3) treatment-as-usual control group (i.e., receiving psychological treatment from a mental health professional for anxiety, alcohol use problems, or both; n = 33).
The Re-Train Your Brain intervention incorporating interpretation bias modification and alcohol approach bias modification was delivered alongside participants’ treatment as usual in both intervention groups. The Re-Train Your Brain intervention consisted of 10 online 20-minute sessions to be completed across five weeks (2 per week). Before beginning the training sessions, participants had to complete a web-based psychoeducational alcohol-anxiety module explaining the link between anxiety and alcohol use, cognitive biases, and the importance of changing these biases.
The interpretation bias component of the Re-Train Your Brain intervention involved presenting ambiguous social scenarios to participants and requesting for them to complete word fragments in a positive or neutral manner. Comprehension questions after each social scenario were answered and points were awarded for correct answers to enhance engagement. For alcohol approach bias modification designed to modify participants’ response to alcohol-related cues, participants were instructed to react to images of alcoholic and nonalcoholic drinks by pulling or pushing a computer mouse, causing the image size to increase or decrease accordingly. Positive feedback and points were awarded for correct responses. The Re-Train Your Brain intervention was delivered in two formats alongside treatment-as-usual: integrated and alternating. Both formats consisted of the same treatment dose. In the integrated treatment group, participants completed 10 online training sessions combining shortened versions of both types of training within each session. The alternating treatment group also consisted of 10 online training sessions but each session consisted of only one type of training in alternating order. The treatment-as-usual control group received their usual treatment from their clinical provider and were placed on a waitlist to access the intervention after the study period.
Primary outcomes, including feasibility of the research and intervention and acceptability of the intervention, were assessed at 6 weeks after baseline. Secondary outcomes were assessed at 6 and 12 weeks after baseline and included cognitive biases (social anxiety interpretation biases, alcohol approach biases, comorbid interpretation biases for social anxiety and alcohol use), social anxiety disorder symptoms, and alcohol-related outcomes (hazardous alcohol use, alcohol consumption, alcohol dependence, alcohol cravings). Comorbid interpretation biases for social anxiety and alcohol assess the extent to which individuals presented with an ambiguous situation that has several possible explanations choose the option that link alcohol use with social concerns. It was hypothesized that both formats of the intervention would be feasible to implement and deemed acceptable by young adults. Additionally, both intervention conditions in combination with their existing therapy were hypothesized to result in greater improvements cognitive biases, anxiety symptoms, and alcohol-related outcomes, compared with therapy only. Finally, the integrated intervention format was hypothesized to be more engaging and to produce larger improvements than the alternating intervention format.
Participants in the study were primarily female (76%), in their mid-20s (Mean age = 26.4), well-educated (54%), and employed (72%). The majority of participants (54%) reported generalized anxiety as their primary concern, while fewer (34%) reported social anxiety as their main concern. A large proportion of participants reported high levels of social anxiety (70%) and 61% had AUDIT scores consistent with “probable alcohol dependence” at baseline. All participants in the study were receiving treatment from for their anxiety, alcohol use, or both, considered “treatment as usual”. Participants most often reported seeing general practitioners (63%), psychologists (49%), clinical psychologists (22%), and counselors (21%).
WHAT DID THIS STUDY FIND?
Both formats of the intervention were feasible and acceptable.
At 6 weeks after baseline, 75% of participants completed the survey and 71% completed the cognitive assessment. Completion rates at 6 weeks after baseline were lower for the alternating intervention group compared to the control group. At 12 weeks after baseline, 67% of participants completed the survey, and 62% completed the cognitive assessment. Completion rate of at least one follow-up was significantly higher in the control group compared to the alternating intervention group. Only 4% of participants withdrew from the study.
In terms of intervention feasibility, 76% across both the integrated and alternating intervention groups completed the initial psychoeducational anxiety-alcohol module. A large proportion (81%) of these participants also completed at least 1 of 10 ten training sessions, almost half (49%) completed the optimum number of 6 training sessions, and more than one in three (37%) completed all 10 training sessions. There were no differences between the integrated and alternating intervention groups on number of training sessions completed.
Interventions were acceptable in some respects, but not others.
Across both intervention groups, most (88%) found the Re-Train Your Brain program to be acceptable, user friendly (91%), simple (96%), and easy to complete (91%). Most participants also agreed that they perceived the potential value and effectiveness of the intervention (75%). On the other hand, there were mixed views related to other acceptability measures; about half or less of participants found the intervention enjoyable (55%), motivating (43%), engaging (39%), and likely to be effective in reducing anxiety and alcohol use (52%). About half of participants (51%) also found the intervention to a burden in terms of the time commitment. The alternating intervention group was rated as simpler and more user-friendly when compared to the integrated group.
Intervention participants improved anxiety interpretation biases, but not alcohol approach biases.
Participants in both intervention groups showed large reductions in anxiety interpretation biases from baseline to 6 weeks, and moderate to large reductions from baseline to 12 weeks. The control group did not exhibit changes in interpretation biases over time. When compared to control, both intervention formats were associated with a greater reduction in interpretation biases from baseline to 6 weeks, but these differences in changes did not sustain until 12 weeks. There were no substantial differences between the integrated and alternating intervention groups on interpretation biases. Also, there were no changes over time or differences between groups on alcohol approach biases or non-alcohol approach biases. All groups experienced small to moderate reductions in comorbid interpretation biases at 6 weeks, and these reductions remained at 12 weeks for both intervention groups but were not sustained by the control group. Reductions in comorbid interpretation biases at 12 weeks for the intervention groups were greater than those in the control group. Reductions in comorbid interpretation biases over time, however, were comparable between the integrated and alternating intervention groups.
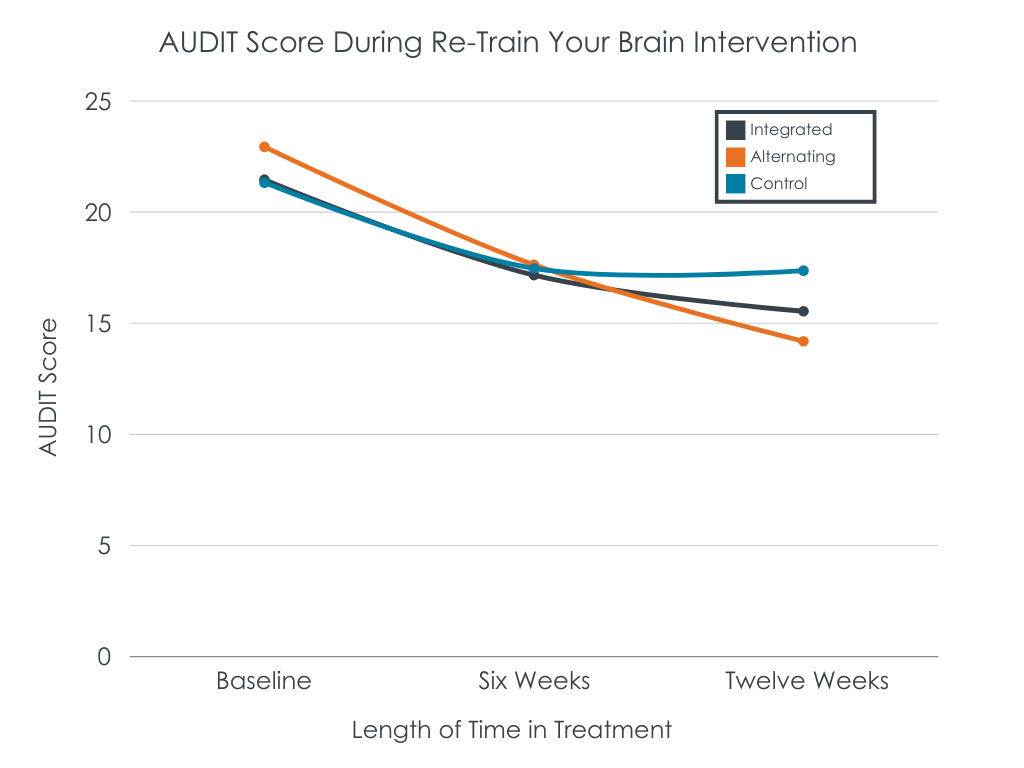
Intervention groups with greater reductions on social anxiety symptoms, hazardous drinking, and alcohol cravings.
On social anxiety symptoms, only the alternating intervention group showed reductions between baseline and 12-week follow-up that were small to moderate in magnitude. Reductions on hazardous drinking were descriptively greater in the intervention groups relative to control, though the difference was not large enough in this small pilot study to reach statistical significance. Compared to the control group, the alternating intervention – but not the integrated intervention – had greater reduction in alcohol craving at the 6-week follow-up. All three groups had similar levels of alcohol craving, however, by the 12-week follow-up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Both formats of the Re-Train Your Brain intervention were feasible to implement and were acceptable by young adults with social anxiety and hazardous drinking, indicating suitability for this age group. This is in line with other research supporting the feasibility and acceptability of delivering cognitive bias modification interventions in digital formats, especially among younger age groups. Nevertheless, results from this study indicate a need for improvement with regard to enhancing participant retention and engagement and adherence to the Re-Train Your Brain intervention, an oft-cited issue in the digital mental health intervention literature. This area of investigation remains critical in order to maximize the effectiveness of digital cognitive bias modification interventions.
This pilot study’s findings that interpretation bias modification and approach bias modification may help to reduce cognitive biases, anxiety symptoms, and alcohol use outcomes aligns with prior research on the effectiveness of cognitive bias modification training to lead to improvements in psychological symptoms. More specifically, this web-based cognitive bias modification intervention incorporating both interpretation bias modification and alcohol approach bias modification, when combined with each participant’s therapy in the community, resulted in greater improvements in anxiety interpretation biases and comorbid interpretation biases when compared to therapy alone. Both formats – the integrated and the alternating session models – were shown to be equally helpful. Of note, however, participants found the alternating model simpler and more user-friendly. It may be that combining training approaches in one session adds complexity rather than its intended purpose of enhancing engagement.
Given the web-based and low-threshold nature of this digital intervention, the Re-Train Your Brain intervention could potentially represent a low-cost and scalable adjunctive treatment for co-occurring social anxiety and alcohol use disorder among young adults. However, given this was a pilot study using a small sample size, results are to be interpreted with caution. Larger randomized control trials testing the efficacy of this cognitive bias modification intervention among a diverse sample of young adults are needed. If the intervention is proven to be a helpful treatment option for young adults with comorbid social anxiety and alcohol use disorder in real-world settings, there is potential for societal benefit.
This was a pilot study and these findings should be considered preliminary, to be tested in larger randomized control trials to see if these findings are replicated.
Most participants reported “generalized anxiety” as their main clinical concern with few participants specifically reporting social anxiety as their primary concern. Although participants all met the threshold for hazardous drinking on the AUDIT, one-third of participants had not consumed any alcohol in the past month at baseline. Additionally, this intervention was delivered online and may not be as effective or accessible for individuals with limited access to technology or low digital literacy. Each of these factors might limit generalizability to all individuals with co-occurring social anxiety and hazardous drinking.
The researchers did not prespecify feasibility and acceptability benchmarks, limiting interpretation of the intervention’s successful implementation.
Participants had to be currently receiving treatment from mental health professionals for their anxiety, alcohol use, or both to be included in the study and this variable was used to indicate receipt of treatment-as-usual. However, the researchers did not standardize the type of therapy received by participants. Thus it is unclear to what the cognitive bias modification interventions are being compared.
BOTTOM LINE
Preliminary results from this small pilot study evaluating a web-based interpretation bias modification and alcohol approach bias modification cognitive retraining intervention show that the intervention is feasible and acceptable for young adults in Australia with comorbid social anxiety and hazardous alcohol use. The format where each session consisted of one type of retraining – rather than one where the trainings were integrated – may have been simpler and more user-friendly, however. The intervention showed promise for different types of anxiety interpretation biases, as well as reducing social anxiety symptoms and alcohol cravings. Larger clinical trials are needed to more rigorously test for the efficacy of the intervention in terms of reducing cognitive biases, social anxiety symptoms, and alcohol-related outcomes among young adults with co-occurring social anxiety disorder and hazardous drinking.
For individuals and families seeking recovery: For co-occurring social anxiety and hazardous drinking, the web-based Re-Train Your Brain cognitive bias modification intervention appears to be an acceptable format for young adults and may prove a beneficial supplement to standard treatment provided by a health professional. This web-based cognitive bias modification intervention shows potential for reducing anxiety and comorbid interpretation biases, which may play an underlying role in managing social anxiety and alcohol use disorder, though further research is needed to properly evaluate the large-scale efficacy of the intervention. Additionally, being a web-based intervention, Re-Train Your Brain could present a low- or no-cost option that can be accessed remotely and easily incorporated into one’s recovery process.
For treatment professionals and treatment systems: Substance use treatment professionals may consider incorporating digital tools, such as the Re-Train Your Brain program, to be used alongside traditional therapies for young adults with co-occurring social anxiety and hazardous alcohol use. Such tools may offer appeal to young adults, given their comfort with technology and receptivity to digital interventions. Online programs can also serve to cut through common barriers related to treatment accessibility (e.g., cost, geography, transportation), as these interventions can be administered remotely in contexts with limited mental health resources. This study also highlights the role of cognitive bias modification in treating comorbid anxiety and alcohol use among young adults. While treatment systems might benefit from incorporating interpretation bias modification and alcohol approach bias modification approaches as adjunctive treatments, more research is needed to examine the cost-effectiveness of these approaches.
For scientists: This study adds to evidence supporting the potential for cognitive bias modification interventions to be used as adjunctive treatments for anxiety and alcohol use alongside standard treatment and highlights the importance of continuing to address comorbidity in mental health research. The study also underscores the potential and need to further explore digital mental health solutions, especially among young adults who are particularly receptive to digital intervention formats. The preliminary nature of this study limits interpretation of results but provides a strong basis for the need to conduct a larger, more comprehensive randomized control trial to evaluate the long-term efficacy for the web-based Re-Train Your Brain intervention to reduce cognitive biases, social anxiety, and alcohol-related outcomes. User engagement and retention in digital interventions, including in this pilot study, remain an important area of investigation if the effectiveness of these programs is to be maximized.
For policy makers: The potential for digital cognitive bias modification interventions to help individuals suffering from comorbid social anxiety and alcohol use disorder warrants support for funding initiatives to support this line of research. More funding in this area would help to address the complexities of comorbid mental health conditions and support the development and implementation of online interventions that can serve to cut across commonly cited barriers to in-person treatment offerings. Similar to in-person treatment offerings, individuals may have difficulty navigating treatment resources and identifying evidence-based treatment services in their area. As the number of digital mental health offerings continues to grow, it will be vital to develop standards and regulations to ensure their efficacy and safety, and to provide resources to communicate about and increase public awareness of the availability and effectiveness of evidence-based digital mental health services.
One way of framing this set of challenges is that both social anxiety and alcohol use disorder are at least in part driven by underlying modifiable cognitive biases, specifically interpretation biases in social anxiety and alcohol approach biases in alcohol use disorder. Interpretation bias modification aims to alter negative interpretations of ambiguous situations or information, which can contribute to social anxiety, by training individuals to resolve these situations in a more positive or neutral manner. Alcohol approach bias modification is geared towards reducing alcohol-related cravings and desire by training participants to repeatedly avoid alcohol-related cues (e.g., by pushing away a computer mouse when an image of an alcoholic beverage is displayed). There is evidence suggesting cognitive bias modification training, including interpretation bias modification and approach bias modification, can be effective at reducing these biases and associated symptoms. Prior studies have also shown that these cognitive bias modification interventions, particularly when combined with standard treatment like CBT, can significantly reduce anxiety symptoms and increase rates of alcohol abstinence. However, studies have collectively produced mixed results and evidence supporting the effectiveness of cognitive bias modification interventions as a stand-alone treatment for nonclinical samples is limited.
With recent shifting preferences for digital technology, especially among younger audiences, there have been increased efforts to deliver interpretation bias modification and approach bias modification interventions via web-based and app-based formats, which may have the potential to offer scalable treatments at rather low cost. Initial findings indicate that these online delivery methods have resulted in good uptake and adherence to online training sessions, though study drop-out (i.e., attrition) remains a concern. Early studies examining their utility suggest there is potential for these digital cognitive bias modification interventions to reduce cognitive biases, and in turn, social anxiety symptoms and alcohol cravings and consumption. However, existing studies have primarily focused on anxiety interpretation bias modification and alcohol approach bias modification programs in isolation of one another. The potential for combining these two web-based cognitive bias modification interventions warrants further investigation, particularly for young adults with comorbid conditions. This pilot RCT evaluated the feasibility, acceptability, and preliminary efficacy of a web-based cognitive bias modification intervention combining interpretation bias modification and approach bias modification as an adjunctive treatment for young adults with co-morbid social anxiety and hazardous alcohol use.
HOW WAS THIS STUDY CONDUCTED?
This was a 3-arm pilot randomized control trial conducted in an online setting in Australia. Participants were recruited via a combination of methods (e.g., paid social media advertisements, flyers at educational institutions) from March 2021 to July 2022. Upon registering for the study on the study website, participants were asked to complete an online screener to determine eligibility status followed by a longer initial survey. In order to be eligible, participants had to: 1) be Australian, 2) be between 18-30 years old, 3) report current hazardous alcohol use, 4) report currently experiencing at least mild social anxiety symptoms, 5) have access to internet and mouse-operable PC or laptop, 6) be receiving psychological treatment for anxiety, alcohol use problems, or both, and 7) be willing to complete intervention components. A total of 100 eligible participants were randomized to either 1) integrated intervention plus treatment-as-usual (each session split in half to include both interpretation bias modification + approach bias modification; n = 35), 2) alternating intervention plus treatment-as-usual (each session focused on interpretation bias modification or approach bias modification in alternating pattern; n = 32), or 3) treatment-as-usual control group (i.e., receiving psychological treatment from a mental health professional for anxiety, alcohol use problems, or both; n = 33).
The Re-Train Your Brain intervention incorporating interpretation bias modification and alcohol approach bias modification was delivered alongside participants’ treatment as usual in both intervention groups. The Re-Train Your Brain intervention consisted of 10 online 20-minute sessions to be completed across five weeks (2 per week). Before beginning the training sessions, participants had to complete a web-based psychoeducational alcohol-anxiety module explaining the link between anxiety and alcohol use, cognitive biases, and the importance of changing these biases.
The interpretation bias component of the Re-Train Your Brain intervention involved presenting ambiguous social scenarios to participants and requesting for them to complete word fragments in a positive or neutral manner. Comprehension questions after each social scenario were answered and points were awarded for correct answers to enhance engagement. For alcohol approach bias modification designed to modify participants’ response to alcohol-related cues, participants were instructed to react to images of alcoholic and nonalcoholic drinks by pulling or pushing a computer mouse, causing the image size to increase or decrease accordingly. Positive feedback and points were awarded for correct responses. The Re-Train Your Brain intervention was delivered in two formats alongside treatment-as-usual: integrated and alternating. Both formats consisted of the same treatment dose. In the integrated treatment group, participants completed 10 online training sessions combining shortened versions of both types of training within each session. The alternating treatment group also consisted of 10 online training sessions but each session consisted of only one type of training in alternating order. The treatment-as-usual control group received their usual treatment from their clinical provider and were placed on a waitlist to access the intervention after the study period.
Primary outcomes, including feasibility of the research and intervention and acceptability of the intervention, were assessed at 6 weeks after baseline. Secondary outcomes were assessed at 6 and 12 weeks after baseline and included cognitive biases (social anxiety interpretation biases, alcohol approach biases, comorbid interpretation biases for social anxiety and alcohol use), social anxiety disorder symptoms, and alcohol-related outcomes (hazardous alcohol use, alcohol consumption, alcohol dependence, alcohol cravings). Comorbid interpretation biases for social anxiety and alcohol assess the extent to which individuals presented with an ambiguous situation that has several possible explanations choose the option that link alcohol use with social concerns. It was hypothesized that both formats of the intervention would be feasible to implement and deemed acceptable by young adults. Additionally, both intervention conditions in combination with their existing therapy were hypothesized to result in greater improvements cognitive biases, anxiety symptoms, and alcohol-related outcomes, compared with therapy only. Finally, the integrated intervention format was hypothesized to be more engaging and to produce larger improvements than the alternating intervention format.
Participants in the study were primarily female (76%), in their mid-20s (Mean age = 26.4), well-educated (54%), and employed (72%). The majority of participants (54%) reported generalized anxiety as their primary concern, while fewer (34%) reported social anxiety as their main concern. A large proportion of participants reported high levels of social anxiety (70%) and 61% had AUDIT scores consistent with “probable alcohol dependence” at baseline. All participants in the study were receiving treatment from for their anxiety, alcohol use, or both, considered “treatment as usual”. Participants most often reported seeing general practitioners (63%), psychologists (49%), clinical psychologists (22%), and counselors (21%).
WHAT DID THIS STUDY FIND?
Both formats of the intervention were feasible and acceptable.
At 6 weeks after baseline, 75% of participants completed the survey and 71% completed the cognitive assessment. Completion rates at 6 weeks after baseline were lower for the alternating intervention group compared to the control group. At 12 weeks after baseline, 67% of participants completed the survey, and 62% completed the cognitive assessment. Completion rate of at least one follow-up was significantly higher in the control group compared to the alternating intervention group. Only 4% of participants withdrew from the study.
In terms of intervention feasibility, 76% across both the integrated and alternating intervention groups completed the initial psychoeducational anxiety-alcohol module. A large proportion (81%) of these participants also completed at least 1 of 10 ten training sessions, almost half (49%) completed the optimum number of 6 training sessions, and more than one in three (37%) completed all 10 training sessions. There were no differences between the integrated and alternating intervention groups on number of training sessions completed.
Interventions were acceptable in some respects, but not others.
Across both intervention groups, most (88%) found the Re-Train Your Brain program to be acceptable, user friendly (91%), simple (96%), and easy to complete (91%). Most participants also agreed that they perceived the potential value and effectiveness of the intervention (75%). On the other hand, there were mixed views related to other acceptability measures; about half or less of participants found the intervention enjoyable (55%), motivating (43%), engaging (39%), and likely to be effective in reducing anxiety and alcohol use (52%). About half of participants (51%) also found the intervention to a burden in terms of the time commitment. The alternating intervention group was rated as simpler and more user-friendly when compared to the integrated group.
Intervention participants improved anxiety interpretation biases, but not alcohol approach biases.
Participants in both intervention groups showed large reductions in anxiety interpretation biases from baseline to 6 weeks, and moderate to large reductions from baseline to 12 weeks. The control group did not exhibit changes in interpretation biases over time. When compared to control, both intervention formats were associated with a greater reduction in interpretation biases from baseline to 6 weeks, but these differences in changes did not sustain until 12 weeks. There were no substantial differences between the integrated and alternating intervention groups on interpretation biases. Also, there were no changes over time or differences between groups on alcohol approach biases or non-alcohol approach biases. All groups experienced small to moderate reductions in comorbid interpretation biases at 6 weeks, and these reductions remained at 12 weeks for both intervention groups but were not sustained by the control group. Reductions in comorbid interpretation biases at 12 weeks for the intervention groups were greater than those in the control group. Reductions in comorbid interpretation biases over time, however, were comparable between the integrated and alternating intervention groups.
Intervention groups with greater reductions on social anxiety symptoms, hazardous drinking, and alcohol cravings.
On social anxiety symptoms, only the alternating intervention group showed reductions between baseline and 12-week follow-up that were small to moderate in magnitude. Reductions on hazardous drinking were descriptively greater in the intervention groups relative to control, though the difference was not large enough in this small pilot study to reach statistical significance. Compared to the control group, the alternating intervention – but not the integrated intervention – had greater reduction in alcohol craving at the 6-week follow-up. All three groups had similar levels of alcohol craving, however, by the 12-week follow-up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Both formats of the Re-Train Your Brain intervention were feasible to implement and were acceptable by young adults with social anxiety and hazardous drinking, indicating suitability for this age group. This is in line with other research supporting the feasibility and acceptability of delivering cognitive bias modification interventions in digital formats, especially among younger age groups. Nevertheless, results from this study indicate a need for improvement with regard to enhancing participant retention and engagement and adherence to the Re-Train Your Brain intervention, an oft-cited issue in the digital mental health intervention literature. This area of investigation remains critical in order to maximize the effectiveness of digital cognitive bias modification interventions.
This pilot study’s findings that interpretation bias modification and approach bias modification may help to reduce cognitive biases, anxiety symptoms, and alcohol use outcomes aligns with prior research on the effectiveness of cognitive bias modification training to lead to improvements in psychological symptoms. More specifically, this web-based cognitive bias modification intervention incorporating both interpretation bias modification and alcohol approach bias modification, when combined with each participant’s therapy in the community, resulted in greater improvements in anxiety interpretation biases and comorbid interpretation biases when compared to therapy alone. Both formats – the integrated and the alternating session models – were shown to be equally helpful. Of note, however, participants found the alternating model simpler and more user-friendly. It may be that combining training approaches in one session adds complexity rather than its intended purpose of enhancing engagement.
Given the web-based and low-threshold nature of this digital intervention, the Re-Train Your Brain intervention could potentially represent a low-cost and scalable adjunctive treatment for co-occurring social anxiety and alcohol use disorder among young adults. However, given this was a pilot study using a small sample size, results are to be interpreted with caution. Larger randomized control trials testing the efficacy of this cognitive bias modification intervention among a diverse sample of young adults are needed. If the intervention is proven to be a helpful treatment option for young adults with comorbid social anxiety and alcohol use disorder in real-world settings, there is potential for societal benefit.
This was a pilot study and these findings should be considered preliminary, to be tested in larger randomized control trials to see if these findings are replicated.
Most participants reported “generalized anxiety” as their main clinical concern with few participants specifically reporting social anxiety as their primary concern. Although participants all met the threshold for hazardous drinking on the AUDIT, one-third of participants had not consumed any alcohol in the past month at baseline. Additionally, this intervention was delivered online and may not be as effective or accessible for individuals with limited access to technology or low digital literacy. Each of these factors might limit generalizability to all individuals with co-occurring social anxiety and hazardous drinking.
The researchers did not prespecify feasibility and acceptability benchmarks, limiting interpretation of the intervention’s successful implementation.
Participants had to be currently receiving treatment from mental health professionals for their anxiety, alcohol use, or both to be included in the study and this variable was used to indicate receipt of treatment-as-usual. However, the researchers did not standardize the type of therapy received by participants. Thus it is unclear to what the cognitive bias modification interventions are being compared.
BOTTOM LINE
Preliminary results from this small pilot study evaluating a web-based interpretation bias modification and alcohol approach bias modification cognitive retraining intervention show that the intervention is feasible and acceptable for young adults in Australia with comorbid social anxiety and hazardous alcohol use. The format where each session consisted of one type of retraining – rather than one where the trainings were integrated – may have been simpler and more user-friendly, however. The intervention showed promise for different types of anxiety interpretation biases, as well as reducing social anxiety symptoms and alcohol cravings. Larger clinical trials are needed to more rigorously test for the efficacy of the intervention in terms of reducing cognitive biases, social anxiety symptoms, and alcohol-related outcomes among young adults with co-occurring social anxiety disorder and hazardous drinking.
For individuals and families seeking recovery: For co-occurring social anxiety and hazardous drinking, the web-based Re-Train Your Brain cognitive bias modification intervention appears to be an acceptable format for young adults and may prove a beneficial supplement to standard treatment provided by a health professional. This web-based cognitive bias modification intervention shows potential for reducing anxiety and comorbid interpretation biases, which may play an underlying role in managing social anxiety and alcohol use disorder, though further research is needed to properly evaluate the large-scale efficacy of the intervention. Additionally, being a web-based intervention, Re-Train Your Brain could present a low- or no-cost option that can be accessed remotely and easily incorporated into one’s recovery process.
For treatment professionals and treatment systems: Substance use treatment professionals may consider incorporating digital tools, such as the Re-Train Your Brain program, to be used alongside traditional therapies for young adults with co-occurring social anxiety and hazardous alcohol use. Such tools may offer appeal to young adults, given their comfort with technology and receptivity to digital interventions. Online programs can also serve to cut through common barriers related to treatment accessibility (e.g., cost, geography, transportation), as these interventions can be administered remotely in contexts with limited mental health resources. This study also highlights the role of cognitive bias modification in treating comorbid anxiety and alcohol use among young adults. While treatment systems might benefit from incorporating interpretation bias modification and alcohol approach bias modification approaches as adjunctive treatments, more research is needed to examine the cost-effectiveness of these approaches.
For scientists: This study adds to evidence supporting the potential for cognitive bias modification interventions to be used as adjunctive treatments for anxiety and alcohol use alongside standard treatment and highlights the importance of continuing to address comorbidity in mental health research. The study also underscores the potential and need to further explore digital mental health solutions, especially among young adults who are particularly receptive to digital intervention formats. The preliminary nature of this study limits interpretation of results but provides a strong basis for the need to conduct a larger, more comprehensive randomized control trial to evaluate the long-term efficacy for the web-based Re-Train Your Brain intervention to reduce cognitive biases, social anxiety, and alcohol-related outcomes. User engagement and retention in digital interventions, including in this pilot study, remain an important area of investigation if the effectiveness of these programs is to be maximized.
For policy makers: The potential for digital cognitive bias modification interventions to help individuals suffering from comorbid social anxiety and alcohol use disorder warrants support for funding initiatives to support this line of research. More funding in this area would help to address the complexities of comorbid mental health conditions and support the development and implementation of online interventions that can serve to cut across commonly cited barriers to in-person treatment offerings. Similar to in-person treatment offerings, individuals may have difficulty navigating treatment resources and identifying evidence-based treatment services in their area. As the number of digital mental health offerings continues to grow, it will be vital to develop standards and regulations to ensure their efficacy and safety, and to provide resources to communicate about and increase public awareness of the availability and effectiveness of evidence-based digital mental health services.