Does proactive outreach and family involvement improve extended-release naltrexone outcomes?
Medication treatments for alcohol and opioid use disorders can help individuals achieve and maintain recovery, but many have difficulty staying on these medications. This study tested whether adding assertive patient outreach and family involvement to standard extended-release naltrexone treatment improved medication adherence.
Extended-release naltrexone (i.e. also known by the brand name Vivitrol) is a once-monthly injection that is commonly used to treat both opioid use disorder and alcohol use disorder. Studies have demonstrated benefits, relative to placebo and psychosocial treatment alone, including its ability to reduce opioid/alcohol craving and use.
Though once-monthly injections — versus daily pills — help to increase patient adherence to naltrexone, there is room for improvement when it comes to helping people continue receiving the medication. Among individuals with opioid use disorder who receive an initial injection of extended-release naltrexone, only 25% make it to 4 months of injections. Similar outcomes are seen for people with alcohol use disorder, with only about 25% making it to 6 months. This is important because discontinuing medication treatment too early obviously prevents its ongoing positive benefits.
Recent research has begun to test new ways to improve adherence to extended-release naltrexone, including methods of assertive outreach (i.e. proactive and persistent patient outreach to engage and retain them in treatment) and significant other (i.e. family) involvement, which have the potential to help overcome barriers to initiating and continuing medication treatment. For example, the Youth Opioid Recovery Support intervention, which combines assertive outreach, significant other involvement, contingency management, and home-based delivery of medication, has shown to significantly improve extended-release naltrexone adherence among young adults with opioid use disorder. Additional interventions for adults have incorporated significant others to engage their loved ones in treatment (e.g., Community Reinforcement and Family Training; CRAFT) and to monitor their loved ones’ medication adherence, with encouraging results. However, research assessing these interventions lacks a comparison group (without significant other involvement), limiting our ability to determine whether family-based interventions improve adherence compared to standard treatment.
Additional medication research is needed to determine the best way to improve adherence. This randomized controlled trial examined the effects of a new intervention on extended-release naltrexone adherence, in which patients with alcohol and opioid use disorder received assertive outreach and significant other involvement in their medication treatment.
HOW WAS THIS STUDY CONDUCTED?
This study was a 16-week pilot randomized controlled trial of a new intervention for adults receiving extended-release naltrexone for alcohol or opioid use disorder, which consisted of assertive outreach and involvement of a significant other in treatment, with the goal of improving patient adherence to extended-release naltrexone.
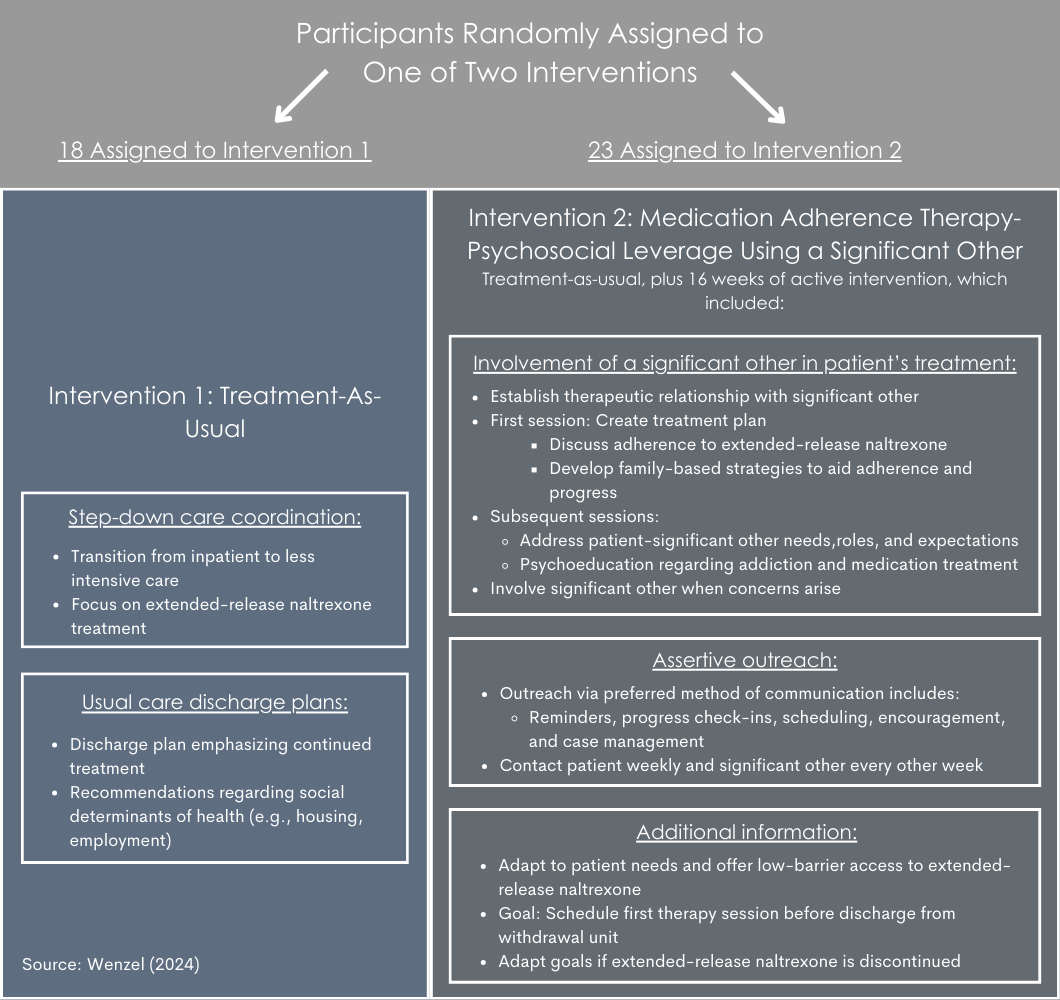
Forty-one individuals with alcohol use disorder and/or opioid use disorder were recruited from an inpatient medically-managed withdrawal unit, within a treatment facility in Baltimore, Maryland. At the time of study enrollment, all patients were planning to receive or had recently received their first dose of extended-release naltrexone, and planned to continue outpatient treatment at the same treatment facility. Consistent with standard procedures at the facility, all patients received their first injection of extended-release naltrexone before being discharged from the inpatient withdrawal unit. Patients typically transitioned to outpatient treatment within 1 week of discharge. Patients were randomized to 1 of 2 conditions, treatment-as-usual or treatment-as-usual plus medication adherence therapy (see figure below).
Twenty-three patients were assigned to treatment as usual and 18 were assigned to the active intervention. For each patient in the active intervention, 1 or more adult significant others were identified and enrolled in the study (n=19).
Patients completed study assessments before being discharged from the withdrawal unit (i.e. baseline) and 16 weeks later (follow-up), with substance use measures assessed at 2-week intervals in between. Primary outcomes of interest included:
1) Number of prescribed extended-release naltrexone doses received over the 16-week follow-up.
a. Measured by self-report questionnaire with supplemental information from patients’ electronic health records.
2) Relapse, or a return to regular substance use
a. Defined as ≥10 days of opioid use (for patients with opioid use disorder) or heavy alcohol use (i.e. ≥5 drinks for men; ≥4 for women; for patients with alcohol use disorder), within any 4-week period. Measured via self-report (Timeline Follow-Back) and urine drug screen.
Other outcomes assessed: (1) percentage of patients receiving all prescribed extended-release naltrexone doses; (2) number of days of heavy opioid/alcohol use (i.e. any opioid use; ≥5 standard drinks for men and ≥4 for women); (3) intervention satisfaction at the end of the study, as assessed with a study-specific survey of patients and significant others in the active intervention condition.
When medication dosing data was missing for a given timepoint, it was assumed that the patient did not receive that respective dose. Missing and positive drug screens for alcohol/opioids were treated as use of these substances for 5 consecutive days over a given 2-week period. The data were analyzed for differences between patients assigned to the active intervention and treatment-as-usual. The researchers also examined outcomes controlling for patients’ substance use disorder diagnoses (i.e. alcohol and/or opioid use disorder).
The majority of patient participants were non-White (68%) men (78%) with public insurance (93%) and an average age of 36 years. Twenty-nine percent of patients had a current diagnosis of both alcohol and opioid use disorders, 37% had opioid use disorder only, 34% had alcohol use disorder only. One-quarter of patients had a prior history of extended-release naltrexone treatment, and one-third had a history of buprenorphine or methadone treatment. All participants reported opioid/alcohol use in the 30 days before study enrollment and were willing to involve a significant other in their treatment. Among individuals with alcohol use disorder, those assigned to treatment-as-usual reported an older age at the time of their first alcoholic drink relative to those in the active intervention group. For the active intervention, patient and significant-other pairs completed an average of 3 group therapy sessions (range: 1 to 6 sessions). Significant others included patients’ mothers (37%), fathers (21%), siblings (16%), romantic partners (11%), daughters (5%), cousins (5%), and others (5%).
WHAT DID THIS STUDY FIND?
Assertive outreach and family-involved treatment resulted in better medication adherence
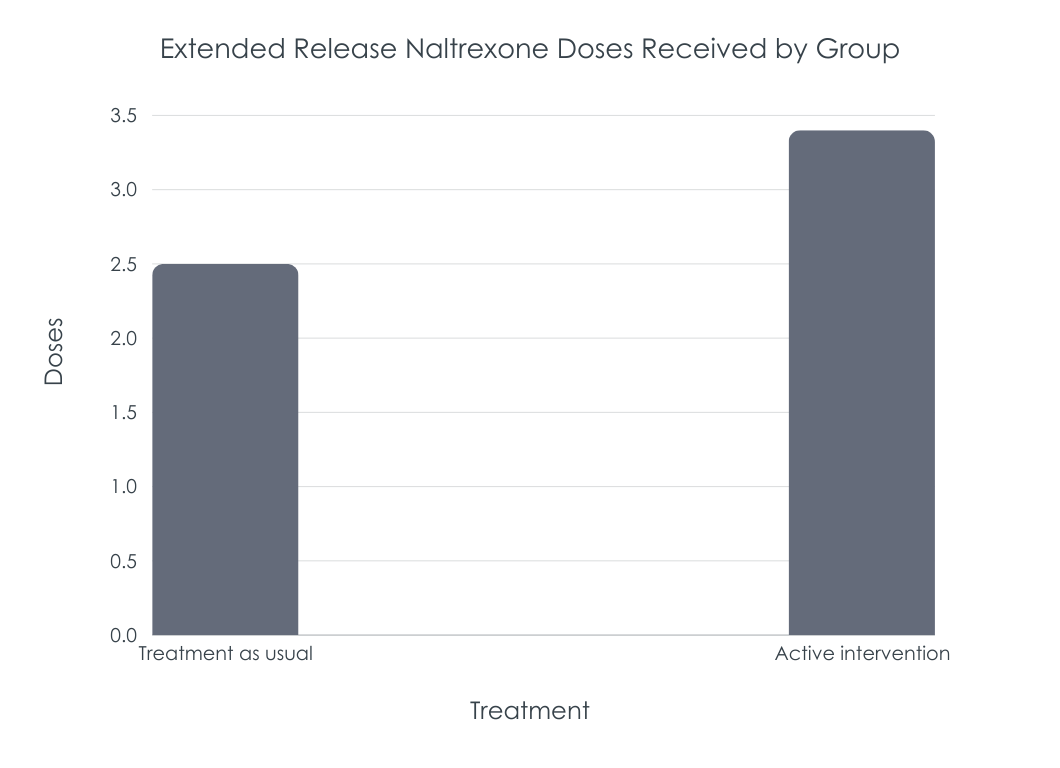
On average and over the 4-month study, patients assigned to the active intervention received about 1 more extended-release naltrexone dose than patients assigned to treatment-as-usual. This difference was statistically significant when analyses controlled for current substance use disorder diagnoses.
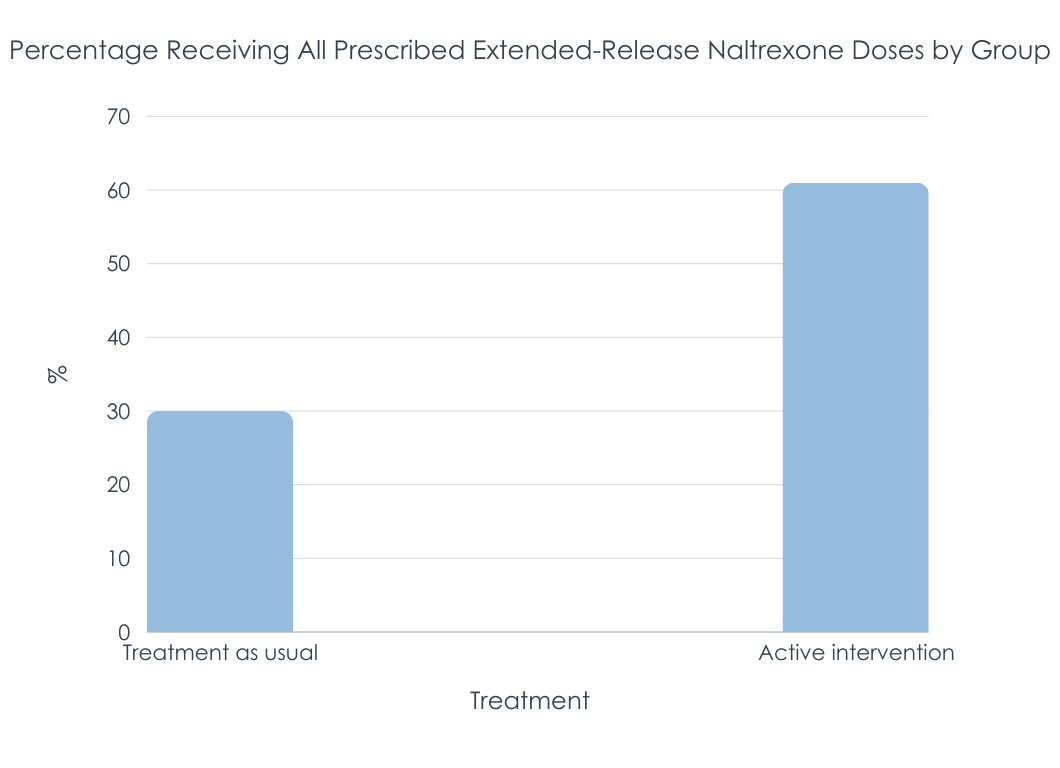
Compared to treatment-as-usual, twice as many patients in the active intervention group received all of their prescribed extended-release naltrexone doses over the 4-month period. Controlling for substance use disorder diagnoses, active intervention patients were about 5 times more likely than usual care patients to receive all prescribed doses.
Assertive outreach and family-involved treatment did not affect relapse above and beyond treatment-as-usual
Relapse rates for the active intervention and treatment-as-usual groups were identical (61% returned to regular opioid/alcohol use) irrespective of substance use disorder diagnoses.
The number of opioid/heavy alcohol use days during the trial did not differ between patients assigned to treatment-as-usual (18.3 days) and the active intervention (19.5 days).
Patients were satisfied with the assertive outreach and family-involved treatment they received
Active-intervention satisfaction questionnaires were completed by 67% of patients and significant others who received it. On average, patients were highly satisfied with the level of significant other involvement in their treatment (scored: 9/10). Patient and significant-other feedback noted family involvement, calls/checkups/reminders, and structured treatment plans as helpful aspects of the intervention.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this can help identify new interventions that help address ongoing difficulty with patient adherence to medication treatments for alcohol and opioid use disorder. Adherence to extended-release naltrexone is important because its beneficial effects on substance use wane once discontinued, and outcomes are better among patients with longer treatment durations. This study investigated a new intervention combining assertive outreach and family involvement in treatment with the goal of improving patient adherence to extended-release naltrexone over a 4-month period. Results suggest that adding assertive outreach and family involvement to standard outpatient medication treatment improves medication adherence (i.e. number of doses received & percentage of patients who received all doses during the study), relative to treatment-as-usual, but this advantage did not translate into better substance use outcomes. Though intervention satisfaction ratings were only obtained from a small subset of participants, they suggested patients were also highly satisfied with the intervention and the level of family involvement in their treatment. Findings highlight the benefits of family support and assertive outreach for improving medication treatment adherence. They also support the feasibility and acceptability of delivering an intervention like this in standard outpatient care.
Outcomes are consistent with prior research of family-involved interventions for young adults, showing that assertive outreach and family-involved treatment, emphasizing medication adherence, results in extended-release naltrexone adherence rates that are 44% higher than standard medication treatment. Slightly lower adherence rates in the current study (31% higher adherence with active intervention) may be because parents – half of the current sample – have a more active support role for their children as young adults versus middle aged adults – note that the average sample age here was 36 years old. Also, prior work, but not the current study, included payment incentives for doses and medication home delivery. In addition, more than half of the significant others in this study were parents of patients, whereas studies of other evidence-based approaches for adults (e.g., CRAFT) have primarily consisted of romantic partners or spouses in their significant-other samples. Despite these differences, adherence outcomes suggest the utility of assertive outreach to help maintain patients on treatment, and family involvement in treatment to support treatment maintenance and progress.
Despite receiving a greater number of medication doses, the active intervention group did not have better relapse rates than the treatment-as-usual group. Relapse rates in this study are similar to relapse (defined as 7 consecutive days or 4 consecutive weeks of opioid use) when taking extended-release naltrexone in another rigorous trial. All participants in this study had exposure to extended-release naltrexone for at least some period of time. The intervention group was also more clinically severe (e.g., higher rates of lifetime injection opioid use — 50% vs. 37% — and recent hospital visits 50 vs. 39%); small sample sizes in the two groups made it difficult to detect significant differences that may have real-world meaning. More medication doses may not have translated to better outcomes because this group was contending with more challenges. Additional research will help clarify the role of assertive outreach and family-involved treatment in relapse prevention, and will help determine whether combining it with interventions targeting relapse prevention can further enhance patient outcomes.
It’s important to note that, of the 128 people screened in this study, 63% were ineligible to participate – though the majority were ineligible because they planned care transition to an outside facility (38%), over one-quarter were ineligible because they refused treatment with extended-release naltrexone (28%), and some refused to identify a significant other to involve in their treatment (7%). This highlights the need to better understand patients’ reasons for refusing medication treatment and for not wanting to involve other people in their treatment and recovery journeys. Doing so can ultimately inform new methods for encouraging patient willingness to engage in treatment, and can help identify the best treatment models for patients with different treatment and recovery goals.
Participant characteristics (e.g., age, gender, clinical severity) were not considered when randomly assigned to groups which has the potential to influence outcomes as with small sample sizes (such as in this study) differences between groups on these can still occur even after randomization because the small sample size is insufficiently large to eradicate differences and equate groups on these variables. Though significant differences didn’t emerge, clinical severity was somewhat greater in the active intervention group than the treatment-as-usual group. See implications for more detail.
All patients who enrolled in the study planned to start or had recently started extended-release naltrexone, and were willing to involve a significant other in their treatment. Thus, this study cohort represents a group of individuals who were already motivated to engage in medication treatment and do so with the help of a loved one. In addition, people were excluded for medical, legal, and living situations that would have made study participation unsafe or difficult. Thus, further evaluation of this intervention is needed in patients with more complex life circumstances.
This study had a very small sample size and short duration of follow-up. Thus, the study may not have had a large enough sample (i.e., was underpowered) to detect interactions between intervention assignment and substance use disorder diagnoses, preventing thorough analysis of the different effects of the intervention on individuals with opioid use disorder, alcohol use disorder, or both alcohol and opioid use disorder.
Intervention satisfaction was also only rated by a small subset of participants (n=12) who completed the study and may therefore represent those with more positive intervention experiences.
BOTTOM LINE
This study suggests that assertive patient outreach and involvement of a trusted family member in a patient’s care can increase adherence to extended-release naltrexone for the treatment of alcohol and opioid use disorders, relative to standard medication treatment. Assertive outreach, family involvement did not reduce relapse (i.e., return to regular use) over and above standard treatment, however. Though, the pilot nature of the study, including the small sample size, warrants caution when interpreting results and needs additional research before formal conclusions are made.
For individuals and families seeking recovery: Many individuals struggle to adhere to opioid and alcohol use disorder medications. Monthly injections of extended-release naltrexone help promote adherence compared to daily dosing, but rates of treatment discontinuation are still high. Though assertive patient outreach and involvement of supportive family members in patient treatment are not typically a part of standard care, this study suggests that their addition to usual treatment may help improve adherence to medication. Individuals and families seeking treatment might consider finding a program that supports family involvement and education on addiction treatment. They may also benefit from programs that proactively engage patients with more frequent or intensive follow-up (e.g., repeat phone calls to reschedule missed appointments) to help keep patients engaged in treatment.
For treatment professionals and treatment systems: Assertive outreach and family-involved treatment may be an ideal method for increasing patient adherence to medication treatment. Some practices have already begun to implement assertive outreach or intensive patient follow-up to help promote patient retention and engagement in care. Incorporating practice policies that help retain patients in treatment (e.g., not dropping patients for ongoing substance use, missed appointments, etc.) and working with involved family members to help educate them about their loved one’s treatment may help address ongoing difficulty with patient adherence to medication treatment.
For scientists: Additional research is needed to parse out the effects of family involvement and assertive outreach on treatment adherence and outcomes. Intent-to-treat and per-protocol studies with larger samples, conducted over a longer period of time, that evaluate adherence to additional medication treatments are needed. Investigation of the interaction between intervention assignment and substance use disorder diagnoses will help develop a better understanding of the intervention’s effects on patient sub-populations. Additional assessment of the intervention and its effect on patient progress from the significant-other’s perspective will also aid ongoing refinement of family-based interventions for addiction treatment.
For policy makers: Although medication treatments for opioid and alcohol use disorder are shown to be effective, a large proportion of patients discontinue treatment early, placing them at risk of relapse and/or overdose. Studies like this help identify new ways to support patients that help address early discontinuation and low adherence to medication treatment. Given the limited number of studies examining the effect of assertive outreach and family involvement on medication treatment adherence, funds for additional research will help determine the effect of interventions like this on sub-populations with different clinical histories and on adherence to medications other than extended-release naltrexone. Funding for longer-term and larger-scale studies will also help determine intervention effects beyond the first few months of treatment, as well as the feasibility of broadly incorporating such interventions into standard treatment practices.
Extended-release naltrexone (i.e. also known by the brand name Vivitrol) is a once-monthly injection that is commonly used to treat both opioid use disorder and alcohol use disorder. Studies have demonstrated benefits, relative to placebo and psychosocial treatment alone, including its ability to reduce opioid/alcohol craving and use.
Though once-monthly injections — versus daily pills — help to increase patient adherence to naltrexone, there is room for improvement when it comes to helping people continue receiving the medication. Among individuals with opioid use disorder who receive an initial injection of extended-release naltrexone, only 25% make it to 4 months of injections. Similar outcomes are seen for people with alcohol use disorder, with only about 25% making it to 6 months. This is important because discontinuing medication treatment too early obviously prevents its ongoing positive benefits.
Recent research has begun to test new ways to improve adherence to extended-release naltrexone, including methods of assertive outreach (i.e. proactive and persistent patient outreach to engage and retain them in treatment) and significant other (i.e. family) involvement, which have the potential to help overcome barriers to initiating and continuing medication treatment. For example, the Youth Opioid Recovery Support intervention, which combines assertive outreach, significant other involvement, contingency management, and home-based delivery of medication, has shown to significantly improve extended-release naltrexone adherence among young adults with opioid use disorder. Additional interventions for adults have incorporated significant others to engage their loved ones in treatment (e.g., Community Reinforcement and Family Training; CRAFT) and to monitor their loved ones’ medication adherence, with encouraging results. However, research assessing these interventions lacks a comparison group (without significant other involvement), limiting our ability to determine whether family-based interventions improve adherence compared to standard treatment.
Additional medication research is needed to determine the best way to improve adherence. This randomized controlled trial examined the effects of a new intervention on extended-release naltrexone adherence, in which patients with alcohol and opioid use disorder received assertive outreach and significant other involvement in their medication treatment.
HOW WAS THIS STUDY CONDUCTED?
This study was a 16-week pilot randomized controlled trial of a new intervention for adults receiving extended-release naltrexone for alcohol or opioid use disorder, which consisted of assertive outreach and involvement of a significant other in treatment, with the goal of improving patient adherence to extended-release naltrexone.
Forty-one individuals with alcohol use disorder and/or opioid use disorder were recruited from an inpatient medically-managed withdrawal unit, within a treatment facility in Baltimore, Maryland. At the time of study enrollment, all patients were planning to receive or had recently received their first dose of extended-release naltrexone, and planned to continue outpatient treatment at the same treatment facility. Consistent with standard procedures at the facility, all patients received their first injection of extended-release naltrexone before being discharged from the inpatient withdrawal unit. Patients typically transitioned to outpatient treatment within 1 week of discharge. Patients were randomized to 1 of 2 conditions, treatment-as-usual or treatment-as-usual plus medication adherence therapy (see figure below).
Twenty-three patients were assigned to treatment as usual and 18 were assigned to the active intervention. For each patient in the active intervention, 1 or more adult significant others were identified and enrolled in the study (n=19).
Patients completed study assessments before being discharged from the withdrawal unit (i.e. baseline) and 16 weeks later (follow-up), with substance use measures assessed at 2-week intervals in between. Primary outcomes of interest included:
1) Number of prescribed extended-release naltrexone doses received over the 16-week follow-up.
a. Measured by self-report questionnaire with supplemental information from patients’ electronic health records.
2) Relapse, or a return to regular substance use
a. Defined as ≥10 days of opioid use (for patients with opioid use disorder) or heavy alcohol use (i.e. ≥5 drinks for men; ≥4 for women; for patients with alcohol use disorder), within any 4-week period. Measured via self-report (Timeline Follow-Back) and urine drug screen.
Other outcomes assessed: (1) percentage of patients receiving all prescribed extended-release naltrexone doses; (2) number of days of heavy opioid/alcohol use (i.e. any opioid use; ≥5 standard drinks for men and ≥4 for women); (3) intervention satisfaction at the end of the study, as assessed with a study-specific survey of patients and significant others in the active intervention condition.
When medication dosing data was missing for a given timepoint, it was assumed that the patient did not receive that respective dose. Missing and positive drug screens for alcohol/opioids were treated as use of these substances for 5 consecutive days over a given 2-week period. The data were analyzed for differences between patients assigned to the active intervention and treatment-as-usual. The researchers also examined outcomes controlling for patients’ substance use disorder diagnoses (i.e. alcohol and/or opioid use disorder).
The majority of patient participants were non-White (68%) men (78%) with public insurance (93%) and an average age of 36 years. Twenty-nine percent of patients had a current diagnosis of both alcohol and opioid use disorders, 37% had opioid use disorder only, 34% had alcohol use disorder only. One-quarter of patients had a prior history of extended-release naltrexone treatment, and one-third had a history of buprenorphine or methadone treatment. All participants reported opioid/alcohol use in the 30 days before study enrollment and were willing to involve a significant other in their treatment. Among individuals with alcohol use disorder, those assigned to treatment-as-usual reported an older age at the time of their first alcoholic drink relative to those in the active intervention group. For the active intervention, patient and significant-other pairs completed an average of 3 group therapy sessions (range: 1 to 6 sessions). Significant others included patients’ mothers (37%), fathers (21%), siblings (16%), romantic partners (11%), daughters (5%), cousins (5%), and others (5%).
WHAT DID THIS STUDY FIND?
Assertive outreach and family-involved treatment resulted in better medication adherence
On average and over the 4-month study, patients assigned to the active intervention received about 1 more extended-release naltrexone dose than patients assigned to treatment-as-usual. This difference was statistically significant when analyses controlled for current substance use disorder diagnoses.
Compared to treatment-as-usual, twice as many patients in the active intervention group received all of their prescribed extended-release naltrexone doses over the 4-month period. Controlling for substance use disorder diagnoses, active intervention patients were about 5 times more likely than usual care patients to receive all prescribed doses.
Assertive outreach and family-involved treatment did not affect relapse above and beyond treatment-as-usual
Relapse rates for the active intervention and treatment-as-usual groups were identical (61% returned to regular opioid/alcohol use) irrespective of substance use disorder diagnoses.
The number of opioid/heavy alcohol use days during the trial did not differ between patients assigned to treatment-as-usual (18.3 days) and the active intervention (19.5 days).
Patients were satisfied with the assertive outreach and family-involved treatment they received
Active-intervention satisfaction questionnaires were completed by 67% of patients and significant others who received it. On average, patients were highly satisfied with the level of significant other involvement in their treatment (scored: 9/10). Patient and significant-other feedback noted family involvement, calls/checkups/reminders, and structured treatment plans as helpful aspects of the intervention.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this can help identify new interventions that help address ongoing difficulty with patient adherence to medication treatments for alcohol and opioid use disorder. Adherence to extended-release naltrexone is important because its beneficial effects on substance use wane once discontinued, and outcomes are better among patients with longer treatment durations. This study investigated a new intervention combining assertive outreach and family involvement in treatment with the goal of improving patient adherence to extended-release naltrexone over a 4-month period. Results suggest that adding assertive outreach and family involvement to standard outpatient medication treatment improves medication adherence (i.e. number of doses received & percentage of patients who received all doses during the study), relative to treatment-as-usual, but this advantage did not translate into better substance use outcomes. Though intervention satisfaction ratings were only obtained from a small subset of participants, they suggested patients were also highly satisfied with the intervention and the level of family involvement in their treatment. Findings highlight the benefits of family support and assertive outreach for improving medication treatment adherence. They also support the feasibility and acceptability of delivering an intervention like this in standard outpatient care.
Outcomes are consistent with prior research of family-involved interventions for young adults, showing that assertive outreach and family-involved treatment, emphasizing medication adherence, results in extended-release naltrexone adherence rates that are 44% higher than standard medication treatment. Slightly lower adherence rates in the current study (31% higher adherence with active intervention) may be because parents – half of the current sample – have a more active support role for their children as young adults versus middle aged adults – note that the average sample age here was 36 years old. Also, prior work, but not the current study, included payment incentives for doses and medication home delivery. In addition, more than half of the significant others in this study were parents of patients, whereas studies of other evidence-based approaches for adults (e.g., CRAFT) have primarily consisted of romantic partners or spouses in their significant-other samples. Despite these differences, adherence outcomes suggest the utility of assertive outreach to help maintain patients on treatment, and family involvement in treatment to support treatment maintenance and progress.
Despite receiving a greater number of medication doses, the active intervention group did not have better relapse rates than the treatment-as-usual group. Relapse rates in this study are similar to relapse (defined as 7 consecutive days or 4 consecutive weeks of opioid use) when taking extended-release naltrexone in another rigorous trial. All participants in this study had exposure to extended-release naltrexone for at least some period of time. The intervention group was also more clinically severe (e.g., higher rates of lifetime injection opioid use — 50% vs. 37% — and recent hospital visits 50 vs. 39%); small sample sizes in the two groups made it difficult to detect significant differences that may have real-world meaning. More medication doses may not have translated to better outcomes because this group was contending with more challenges. Additional research will help clarify the role of assertive outreach and family-involved treatment in relapse prevention, and will help determine whether combining it with interventions targeting relapse prevention can further enhance patient outcomes.
It’s important to note that, of the 128 people screened in this study, 63% were ineligible to participate – though the majority were ineligible because they planned care transition to an outside facility (38%), over one-quarter were ineligible because they refused treatment with extended-release naltrexone (28%), and some refused to identify a significant other to involve in their treatment (7%). This highlights the need to better understand patients’ reasons for refusing medication treatment and for not wanting to involve other people in their treatment and recovery journeys. Doing so can ultimately inform new methods for encouraging patient willingness to engage in treatment, and can help identify the best treatment models for patients with different treatment and recovery goals.
Participant characteristics (e.g., age, gender, clinical severity) were not considered when randomly assigned to groups which has the potential to influence outcomes as with small sample sizes (such as in this study) differences between groups on these can still occur even after randomization because the small sample size is insufficiently large to eradicate differences and equate groups on these variables. Though significant differences didn’t emerge, clinical severity was somewhat greater in the active intervention group than the treatment-as-usual group. See implications for more detail.
All patients who enrolled in the study planned to start or had recently started extended-release naltrexone, and were willing to involve a significant other in their treatment. Thus, this study cohort represents a group of individuals who were already motivated to engage in medication treatment and do so with the help of a loved one. In addition, people were excluded for medical, legal, and living situations that would have made study participation unsafe or difficult. Thus, further evaluation of this intervention is needed in patients with more complex life circumstances.
This study had a very small sample size and short duration of follow-up. Thus, the study may not have had a large enough sample (i.e., was underpowered) to detect interactions between intervention assignment and substance use disorder diagnoses, preventing thorough analysis of the different effects of the intervention on individuals with opioid use disorder, alcohol use disorder, or both alcohol and opioid use disorder.
Intervention satisfaction was also only rated by a small subset of participants (n=12) who completed the study and may therefore represent those with more positive intervention experiences.
BOTTOM LINE
This study suggests that assertive patient outreach and involvement of a trusted family member in a patient’s care can increase adherence to extended-release naltrexone for the treatment of alcohol and opioid use disorders, relative to standard medication treatment. Assertive outreach, family involvement did not reduce relapse (i.e., return to regular use) over and above standard treatment, however. Though, the pilot nature of the study, including the small sample size, warrants caution when interpreting results and needs additional research before formal conclusions are made.
For individuals and families seeking recovery: Many individuals struggle to adhere to opioid and alcohol use disorder medications. Monthly injections of extended-release naltrexone help promote adherence compared to daily dosing, but rates of treatment discontinuation are still high. Though assertive patient outreach and involvement of supportive family members in patient treatment are not typically a part of standard care, this study suggests that their addition to usual treatment may help improve adherence to medication. Individuals and families seeking treatment might consider finding a program that supports family involvement and education on addiction treatment. They may also benefit from programs that proactively engage patients with more frequent or intensive follow-up (e.g., repeat phone calls to reschedule missed appointments) to help keep patients engaged in treatment.
For treatment professionals and treatment systems: Assertive outreach and family-involved treatment may be an ideal method for increasing patient adherence to medication treatment. Some practices have already begun to implement assertive outreach or intensive patient follow-up to help promote patient retention and engagement in care. Incorporating practice policies that help retain patients in treatment (e.g., not dropping patients for ongoing substance use, missed appointments, etc.) and working with involved family members to help educate them about their loved one’s treatment may help address ongoing difficulty with patient adherence to medication treatment.
For scientists: Additional research is needed to parse out the effects of family involvement and assertive outreach on treatment adherence and outcomes. Intent-to-treat and per-protocol studies with larger samples, conducted over a longer period of time, that evaluate adherence to additional medication treatments are needed. Investigation of the interaction between intervention assignment and substance use disorder diagnoses will help develop a better understanding of the intervention’s effects on patient sub-populations. Additional assessment of the intervention and its effect on patient progress from the significant-other’s perspective will also aid ongoing refinement of family-based interventions for addiction treatment.
For policy makers: Although medication treatments for opioid and alcohol use disorder are shown to be effective, a large proportion of patients discontinue treatment early, placing them at risk of relapse and/or overdose. Studies like this help identify new ways to support patients that help address early discontinuation and low adherence to medication treatment. Given the limited number of studies examining the effect of assertive outreach and family involvement on medication treatment adherence, funds for additional research will help determine the effect of interventions like this on sub-populations with different clinical histories and on adherence to medications other than extended-release naltrexone. Funding for longer-term and larger-scale studies will also help determine intervention effects beyond the first few months of treatment, as well as the feasibility of broadly incorporating such interventions into standard treatment practices.
Extended-release naltrexone (i.e. also known by the brand name Vivitrol) is a once-monthly injection that is commonly used to treat both opioid use disorder and alcohol use disorder. Studies have demonstrated benefits, relative to placebo and psychosocial treatment alone, including its ability to reduce opioid/alcohol craving and use.
Though once-monthly injections — versus daily pills — help to increase patient adherence to naltrexone, there is room for improvement when it comes to helping people continue receiving the medication. Among individuals with opioid use disorder who receive an initial injection of extended-release naltrexone, only 25% make it to 4 months of injections. Similar outcomes are seen for people with alcohol use disorder, with only about 25% making it to 6 months. This is important because discontinuing medication treatment too early obviously prevents its ongoing positive benefits.
Recent research has begun to test new ways to improve adherence to extended-release naltrexone, including methods of assertive outreach (i.e. proactive and persistent patient outreach to engage and retain them in treatment) and significant other (i.e. family) involvement, which have the potential to help overcome barriers to initiating and continuing medication treatment. For example, the Youth Opioid Recovery Support intervention, which combines assertive outreach, significant other involvement, contingency management, and home-based delivery of medication, has shown to significantly improve extended-release naltrexone adherence among young adults with opioid use disorder. Additional interventions for adults have incorporated significant others to engage their loved ones in treatment (e.g., Community Reinforcement and Family Training; CRAFT) and to monitor their loved ones’ medication adherence, with encouraging results. However, research assessing these interventions lacks a comparison group (without significant other involvement), limiting our ability to determine whether family-based interventions improve adherence compared to standard treatment.
Additional medication research is needed to determine the best way to improve adherence. This randomized controlled trial examined the effects of a new intervention on extended-release naltrexone adherence, in which patients with alcohol and opioid use disorder received assertive outreach and significant other involvement in their medication treatment.
HOW WAS THIS STUDY CONDUCTED?
This study was a 16-week pilot randomized controlled trial of a new intervention for adults receiving extended-release naltrexone for alcohol or opioid use disorder, which consisted of assertive outreach and involvement of a significant other in treatment, with the goal of improving patient adherence to extended-release naltrexone.
Forty-one individuals with alcohol use disorder and/or opioid use disorder were recruited from an inpatient medically-managed withdrawal unit, within a treatment facility in Baltimore, Maryland. At the time of study enrollment, all patients were planning to receive or had recently received their first dose of extended-release naltrexone, and planned to continue outpatient treatment at the same treatment facility. Consistent with standard procedures at the facility, all patients received their first injection of extended-release naltrexone before being discharged from the inpatient withdrawal unit. Patients typically transitioned to outpatient treatment within 1 week of discharge. Patients were randomized to 1 of 2 conditions, treatment-as-usual or treatment-as-usual plus medication adherence therapy (see figure below).
Twenty-three patients were assigned to treatment as usual and 18 were assigned to the active intervention. For each patient in the active intervention, 1 or more adult significant others were identified and enrolled in the study (n=19).
Patients completed study assessments before being discharged from the withdrawal unit (i.e. baseline) and 16 weeks later (follow-up), with substance use measures assessed at 2-week intervals in between. Primary outcomes of interest included:
1) Number of prescribed extended-release naltrexone doses received over the 16-week follow-up.
a. Measured by self-report questionnaire with supplemental information from patients’ electronic health records.
2) Relapse, or a return to regular substance use
a. Defined as ≥10 days of opioid use (for patients with opioid use disorder) or heavy alcohol use (i.e. ≥5 drinks for men; ≥4 for women; for patients with alcohol use disorder), within any 4-week period. Measured via self-report (Timeline Follow-Back) and urine drug screen.
Other outcomes assessed: (1) percentage of patients receiving all prescribed extended-release naltrexone doses; (2) number of days of heavy opioid/alcohol use (i.e. any opioid use; ≥5 standard drinks for men and ≥4 for women); (3) intervention satisfaction at the end of the study, as assessed with a study-specific survey of patients and significant others in the active intervention condition.
When medication dosing data was missing for a given timepoint, it was assumed that the patient did not receive that respective dose. Missing and positive drug screens for alcohol/opioids were treated as use of these substances for 5 consecutive days over a given 2-week period. The data were analyzed for differences between patients assigned to the active intervention and treatment-as-usual. The researchers also examined outcomes controlling for patients’ substance use disorder diagnoses (i.e. alcohol and/or opioid use disorder).
The majority of patient participants were non-White (68%) men (78%) with public insurance (93%) and an average age of 36 years. Twenty-nine percent of patients had a current diagnosis of both alcohol and opioid use disorders, 37% had opioid use disorder only, 34% had alcohol use disorder only. One-quarter of patients had a prior history of extended-release naltrexone treatment, and one-third had a history of buprenorphine or methadone treatment. All participants reported opioid/alcohol use in the 30 days before study enrollment and were willing to involve a significant other in their treatment. Among individuals with alcohol use disorder, those assigned to treatment-as-usual reported an older age at the time of their first alcoholic drink relative to those in the active intervention group. For the active intervention, patient and significant-other pairs completed an average of 3 group therapy sessions (range: 1 to 6 sessions). Significant others included patients’ mothers (37%), fathers (21%), siblings (16%), romantic partners (11%), daughters (5%), cousins (5%), and others (5%).
WHAT DID THIS STUDY FIND?
Assertive outreach and family-involved treatment resulted in better medication adherence
On average and over the 4-month study, patients assigned to the active intervention received about 1 more extended-release naltrexone dose than patients assigned to treatment-as-usual. This difference was statistically significant when analyses controlled for current substance use disorder diagnoses.
Compared to treatment-as-usual, twice as many patients in the active intervention group received all of their prescribed extended-release naltrexone doses over the 4-month period. Controlling for substance use disorder diagnoses, active intervention patients were about 5 times more likely than usual care patients to receive all prescribed doses.
Assertive outreach and family-involved treatment did not affect relapse above and beyond treatment-as-usual
Relapse rates for the active intervention and treatment-as-usual groups were identical (61% returned to regular opioid/alcohol use) irrespective of substance use disorder diagnoses.
The number of opioid/heavy alcohol use days during the trial did not differ between patients assigned to treatment-as-usual (18.3 days) and the active intervention (19.5 days).
Patients were satisfied with the assertive outreach and family-involved treatment they received
Active-intervention satisfaction questionnaires were completed by 67% of patients and significant others who received it. On average, patients were highly satisfied with the level of significant other involvement in their treatment (scored: 9/10). Patient and significant-other feedback noted family involvement, calls/checkups/reminders, and structured treatment plans as helpful aspects of the intervention.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this can help identify new interventions that help address ongoing difficulty with patient adherence to medication treatments for alcohol and opioid use disorder. Adherence to extended-release naltrexone is important because its beneficial effects on substance use wane once discontinued, and outcomes are better among patients with longer treatment durations. This study investigated a new intervention combining assertive outreach and family involvement in treatment with the goal of improving patient adherence to extended-release naltrexone over a 4-month period. Results suggest that adding assertive outreach and family involvement to standard outpatient medication treatment improves medication adherence (i.e. number of doses received & percentage of patients who received all doses during the study), relative to treatment-as-usual, but this advantage did not translate into better substance use outcomes. Though intervention satisfaction ratings were only obtained from a small subset of participants, they suggested patients were also highly satisfied with the intervention and the level of family involvement in their treatment. Findings highlight the benefits of family support and assertive outreach for improving medication treatment adherence. They also support the feasibility and acceptability of delivering an intervention like this in standard outpatient care.
Outcomes are consistent with prior research of family-involved interventions for young adults, showing that assertive outreach and family-involved treatment, emphasizing medication adherence, results in extended-release naltrexone adherence rates that are 44% higher than standard medication treatment. Slightly lower adherence rates in the current study (31% higher adherence with active intervention) may be because parents – half of the current sample – have a more active support role for their children as young adults versus middle aged adults – note that the average sample age here was 36 years old. Also, prior work, but not the current study, included payment incentives for doses and medication home delivery. In addition, more than half of the significant others in this study were parents of patients, whereas studies of other evidence-based approaches for adults (e.g., CRAFT) have primarily consisted of romantic partners or spouses in their significant-other samples. Despite these differences, adherence outcomes suggest the utility of assertive outreach to help maintain patients on treatment, and family involvement in treatment to support treatment maintenance and progress.
Despite receiving a greater number of medication doses, the active intervention group did not have better relapse rates than the treatment-as-usual group. Relapse rates in this study are similar to relapse (defined as 7 consecutive days or 4 consecutive weeks of opioid use) when taking extended-release naltrexone in another rigorous trial. All participants in this study had exposure to extended-release naltrexone for at least some period of time. The intervention group was also more clinically severe (e.g., higher rates of lifetime injection opioid use — 50% vs. 37% — and recent hospital visits 50 vs. 39%); small sample sizes in the two groups made it difficult to detect significant differences that may have real-world meaning. More medication doses may not have translated to better outcomes because this group was contending with more challenges. Additional research will help clarify the role of assertive outreach and family-involved treatment in relapse prevention, and will help determine whether combining it with interventions targeting relapse prevention can further enhance patient outcomes.
It’s important to note that, of the 128 people screened in this study, 63% were ineligible to participate – though the majority were ineligible because they planned care transition to an outside facility (38%), over one-quarter were ineligible because they refused treatment with extended-release naltrexone (28%), and some refused to identify a significant other to involve in their treatment (7%). This highlights the need to better understand patients’ reasons for refusing medication treatment and for not wanting to involve other people in their treatment and recovery journeys. Doing so can ultimately inform new methods for encouraging patient willingness to engage in treatment, and can help identify the best treatment models for patients with different treatment and recovery goals.
Participant characteristics (e.g., age, gender, clinical severity) were not considered when randomly assigned to groups which has the potential to influence outcomes as with small sample sizes (such as in this study) differences between groups on these can still occur even after randomization because the small sample size is insufficiently large to eradicate differences and equate groups on these variables. Though significant differences didn’t emerge, clinical severity was somewhat greater in the active intervention group than the treatment-as-usual group. See implications for more detail.
All patients who enrolled in the study planned to start or had recently started extended-release naltrexone, and were willing to involve a significant other in their treatment. Thus, this study cohort represents a group of individuals who were already motivated to engage in medication treatment and do so with the help of a loved one. In addition, people were excluded for medical, legal, and living situations that would have made study participation unsafe or difficult. Thus, further evaluation of this intervention is needed in patients with more complex life circumstances.
This study had a very small sample size and short duration of follow-up. Thus, the study may not have had a large enough sample (i.e., was underpowered) to detect interactions between intervention assignment and substance use disorder diagnoses, preventing thorough analysis of the different effects of the intervention on individuals with opioid use disorder, alcohol use disorder, or both alcohol and opioid use disorder.
Intervention satisfaction was also only rated by a small subset of participants (n=12) who completed the study and may therefore represent those with more positive intervention experiences.
BOTTOM LINE
This study suggests that assertive patient outreach and involvement of a trusted family member in a patient’s care can increase adherence to extended-release naltrexone for the treatment of alcohol and opioid use disorders, relative to standard medication treatment. Assertive outreach, family involvement did not reduce relapse (i.e., return to regular use) over and above standard treatment, however. Though, the pilot nature of the study, including the small sample size, warrants caution when interpreting results and needs additional research before formal conclusions are made.
For individuals and families seeking recovery: Many individuals struggle to adhere to opioid and alcohol use disorder medications. Monthly injections of extended-release naltrexone help promote adherence compared to daily dosing, but rates of treatment discontinuation are still high. Though assertive patient outreach and involvement of supportive family members in patient treatment are not typically a part of standard care, this study suggests that their addition to usual treatment may help improve adherence to medication. Individuals and families seeking treatment might consider finding a program that supports family involvement and education on addiction treatment. They may also benefit from programs that proactively engage patients with more frequent or intensive follow-up (e.g., repeat phone calls to reschedule missed appointments) to help keep patients engaged in treatment.
For treatment professionals and treatment systems: Assertive outreach and family-involved treatment may be an ideal method for increasing patient adherence to medication treatment. Some practices have already begun to implement assertive outreach or intensive patient follow-up to help promote patient retention and engagement in care. Incorporating practice policies that help retain patients in treatment (e.g., not dropping patients for ongoing substance use, missed appointments, etc.) and working with involved family members to help educate them about their loved one’s treatment may help address ongoing difficulty with patient adherence to medication treatment.
For scientists: Additional research is needed to parse out the effects of family involvement and assertive outreach on treatment adherence and outcomes. Intent-to-treat and per-protocol studies with larger samples, conducted over a longer period of time, that evaluate adherence to additional medication treatments are needed. Investigation of the interaction between intervention assignment and substance use disorder diagnoses will help develop a better understanding of the intervention’s effects on patient sub-populations. Additional assessment of the intervention and its effect on patient progress from the significant-other’s perspective will also aid ongoing refinement of family-based interventions for addiction treatment.
For policy makers: Although medication treatments for opioid and alcohol use disorder are shown to be effective, a large proportion of patients discontinue treatment early, placing them at risk of relapse and/or overdose. Studies like this help identify new ways to support patients that help address early discontinuation and low adherence to medication treatment. Given the limited number of studies examining the effect of assertive outreach and family involvement on medication treatment adherence, funds for additional research will help determine the effect of interventions like this on sub-populations with different clinical histories and on adherence to medications other than extended-release naltrexone. Funding for longer-term and larger-scale studies will also help determine intervention effects beyond the first few months of treatment, as well as the feasibility of broadly incorporating such interventions into standard treatment practices.