Professional and community-based continuing care following residential treatment
The 30 days following residential treatment are high risk for return to substance use. Because recovery activities and support on any given day could make the difference in one’s ability to marshal newly developed skills critical to abstinence, measuring daily service utilization and outcomes can inform recommendations during this risky period. This study examined engagement with outpatient treatment and other community-based continuing care (e.g., AA) during the first 30 days of community re-entry following residential care and looked at same-day associations between treatment attendance by type of service used and substance use.
Residential substance use disorder treatment provides 24-hour acute care for patients typically with higher levels of severity, chronicity, and complexity. Many also either offer or link to continuing care to help patients maintain gains once discharged from residential care upon re-entry to the community. Among those receiving treatment for a substance use disorder, outpatient treatment is the most common but residential care is also common: approximately 1.3 million Americans receive care in a residential treatment setting each year, representing 1/3 of those seeking treatment. Despite the intensive nature of residential treatment programs, return to substance use upon re-entry is high, and many return to their lives feeling inadequately prepared. Although continuing care – for example, providing or linking to step-down outpatient treatment – is a “best practice”, residential settings vary in their willingness to provide assistance in finding outpatient treatment following the residential stay. Many patients do not participate in any kind of continuing care and are at higher risk for relapse and recurrence. Individuals with opioid use disorder returning to substance use are at a heightened risk for overdose if they are not taking an opioid use disorder treatment medication due to reduced tolerance during the period of abstinence in residential treatment.
The goals of this study were to identify the types of outpatient services including both professional treatment and mutual-help, as well as the degree of engagement, during the first 30 days of community re-entry following residential treatment. The authors also examined associations between attendance at different types of services and substance use on the same day.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of a naturalistic longitudinal survey study. The authors recruited 128 patients discharging from two residential treatment centers in Rhode Island to participate, of whom 65 met with research staff at discharge and attended a follow-up assessment interview. Of the 63 recruited but not included, 44 did not meet with staff at discharge (e.g., participant left treatment earlier than anticipated) and 18 met with staff at discharge but did not attend the 30-day follow-up (1 participant is not accounted for in the study’s methods). To participate, patients needed to be 18 years of age or older, fluent in English, own a smartphone (due to the primary aims of the overall primary study not described in this summary), a history of traumatic experiences (also due to the primary aims of the primary study), discharge in the next 7 days, as well as no current mania, psychosis, or impairment in cognitive functioning. During the follow up assessment, participants reported (retrospectively) any substance use and treatment engagement for each day since residential treatment discharge. The researchers first wanted to characterize the types of outpatient services that patients participated in during the 30 days immediately following residential care. Types of services included community-based Alcoholics Anonymous (AA) or Narcotics Anonymous (NA) meetings, FDA-approved medications (e.g., methadone and buprenorphine for opioid use disorder and naltrexone for opioid or alcohol use disorder), outpatient therapy, inpatient treatment, emergency room visits, short-term residential, long-term residential, recovery coaching, peer support specialist services apart from recovery coaching. Anyone who did not receive one of these services were categorized as receiving no services. The authors characterized (1) how many participants were engaged in any treatment or services at all, and (2) how often they were engaged in each service during the 30-day period. Next, the authors examined whether engagement in each type of service was associated with substance use on that same day. Of note, due to the study’s sample of 65 participants, the reliability/stability of findings from sub-sets of participants may be quite low. As such, we focus the summary findings on results where 3 or more of those services in which at least 3 people reported engagement.
WHAT DID THIS STUDY FIND?
Service utilization was common in the first 30 days after residential treatment
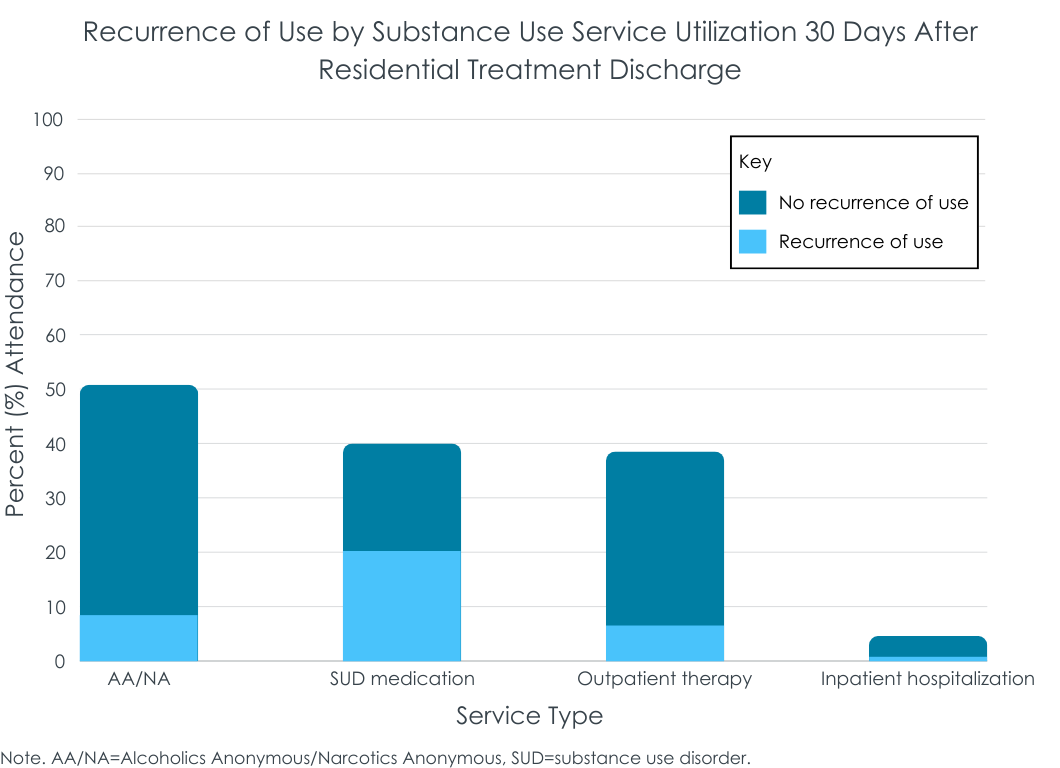
Most of the 65 participants (54, or 83.1%) engaged in at least 1 day of treatment during the 30 days following residential care, with 47.7% engaging in 2+ services during this period. Counting non-attendees as 0 days, participants averaged 17.9 days of service utilization. AA/NA was the most common service (50.8%), followed by taking an FDA-approved medication (40%), outpatient therapy (38.5%), and inpatient hospitalization (4.6%). Only 2 participants reported an emergency room visit, and only 1 participant reported engaging in each of the following: long-term residential treatment, short-term residential treatment, working with a peer support specialist, or working with a recovery coach.
Among those who attended at least 1 Alcoholics/Narcotics Anonymous meeting, participants attended 1+ meeting, on average, for 17.6 days. Those taking medications did so on average for 28 days, whereas those engaged in outpatient therapy or inpatient treatment were engaged for overall less days during the month (11.4 and 15.3, respectively). Most (71%) of those who utilized a service did so on the first day following discharge. On average, people started AA/NA 2 days, medication assisted treatment 2.23 days, outpatient therapy 5.6 days, and inpatient treatment 14.3 days, after discharge from residential care.
Outpatient therapy was associated with reduced risk of same-day substance use
Just over 1/3 (35.4%) of participants reported alcohol or drug use in the 30 days following residential substance use treatment discharge, on average 10 days following discharge. Descriptively, different services were associated with different rates of return to use. Among those taking a medication, 50% returned to use, followed by inpatient treatment (33%), outpatient therapy (16%), and Alcoholics/Narcotics anonymous (16%). See the figure below for return to use during the 30 days after residential discharge by service utilization. Similarly, the number of days until return to use occurred differed by service. Of those who attended Alcoholics/Narcotics Anonymous and returned to use did so, on average, 15.4 days after discharge. Of those who took medication and returned to use, they did so 9 days after discharge on average, and of those who attended outpatient treatment and returned to use, they did so 7 days after discharge on average.
On days that participants reported any (versus no) outpatient therapy, substance use was significantly less likely on that same day controlling for use of other service. On days that participants reported taking an FDA-approved medication for alcohol or opioid use disorder, they were more likely to report substance use on that same day. No other service utilization on a given day was significantly associated with substance use on that same day.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study of a small sample of adults followed after residential treatment found that 4 out of every 5 individuals made contact with some treatment or recovery support service in the month following discharge, and that of those who engaged with continuing care, most did so on the first day after discharge. This suggests that many in this study received the necessary care transition to help facilitate sustained recovery. The most common form of follow up service was attendance at a 12-step mutual-help NA or AA group – both of which are widely available in the community and online and free to access. The results suggested that these mutual-help groups are associated with low rates of return to use as well.
A very important and substantial limitation of the results reported in this study, however, is that the study included only participants that met with staff at discharge and attended the follow-up assessment – 51% of those eligible. These continuing care service utilization rates may be overestimates as they do not include the 49% who may have left residential treatment or otherwise had risk factors both to miss the follow-up and not utilize continuing care (e.g., relapse or otherwise having difficulty functioning). Even among those participants who were included, analyses did not account for important individual factors like clinical severity. That said, while the current study did not include rigorous tests of mutual-help participation effects on substance use outcomes, many high-quality studies, mostly focused on AA for alcohol use disorder, show that AA participation reduces alcohol and other drug use, while increasing rates of abstinence and remission.
One interesting finding was that substance use was less likely on days when outpatient services were received, whereas this was not the case for any other service, including AA/NA attendance which had an overall low rate of return to use across the 30 day follow-up. One possibility is that many 12-step community meetings occur in the evening whereas treatment is often delivered during the day. Especially for individuals in early recovery – as was the case here for participants – activities during the morning/day may help increase participants’ motivation, provide reminders on coping skills cultivated during residential, or plan for risky situations to be encountered later that day/evening, especially for those not employed or who have less structured daytime hours. Future research using multiple daily assessments, such as ecological momentary assessment, of different types of service engagement may help tease apart these same-day effects.
Beyond AA/NA and outpatient treatment, those engaging in other services still saw more favorable rates of continued sobriety across the entire 30-day period compared to those that did not engage in any services during this period. Half of those taking an FDA-approved medication, and 1 in 3 of those who used inpatient services, used alcohol or other drugs on at least 1 in 30 days. Regarding daily service utilization and substance use, it is unclear why taking a medication was associated with an increased risk of substance use on any given day. Those prescribed medications may have had more severe or more chronic patterns of substance use prior to residential treatment entry which can be a predictor of higher rates of return to use post-treatment. Important clinical variables such as clinical severity/chronicity and primary substance (e.g., alcohol, opioid, stimulants, etc.) were not included in these models. Alternatively, these participants may be more likely to use multiple substances, and the medications may be geared toward reducing use of one, but not all, substances (e.g., buprenorphine to address opioid use but not alcohol use). Regardless, rates of return to use were better among those who took a medication relative to those who did not engage in any kind of service following residential. Of the full sample, 17% of those stepping down from residential treatment did not engage in any care, and of those, 70% reported a return to use event in the first 30 days following residential. There are likely to be important differences between those who utilized services (e.g., more motivated, more of other kinds of recovery capital, better access to care, etc.) and those who did not, potentially providing an additional partial explanation for the better outcomes among those who utilized a continuing care service. At the same time, these largely descriptive data are consistent with other more rigorous studies that show various outpatient therapies, mutual-help groups, and FDA-approved medications improve short-term and long-term recovery outcomes. Of note, however, the study did not include recovery residences in their assessment of continuing care after residential, which has been shown to improve substance use outcomes after residential treatment. Nevertheless, these results highlight the importance of continuing care for sustaining progress made in recovery during residential into the first month after discharge.
Although the authors initially attempted to recruit 141 participants, 76 participants did not complete the follow-up survey for various reasons. Those who were still engaged in research after the first month may have different characteristics or patterns of recovery over the month following residential care compared to those who did not complete the follow up.
Analyses examined one service at a time (e.g., outpatient vs. no outpatient, AA/NA vs. no AA/NA, etc.). It is possible that use of multiple services (e.g., taking a medication and attending outpatient treatment) would provide additional protection but this was not tested empirically.
BOTTOM LINE
In combination with many other rigorous studies of continuing care after residential treatment, this study highlights the utility of empirically-supported services such as outpatient therapy, 12-step mutual-help attendance, and FDA-approved medications early in recovery after discharge from residential care.
For individuals and families seeking recovery: The period after residential treatment is a risky period for return to use. However, people who utilize empirically-supported services like outpatient therapy, mutual-help, and FDA-approved medications tend to have better outcomes. If you or a loved one is returning from residential care, engaging in outpatient therapy or AA/NA may buffer against the risk of return to use in the first month as these tend to bolster and boost relapse prevention coping skills and keep cognitive vigilance at a high level.
For treatment professionals and treatment systems: Residential programs that facilitate or provide assistance with helping patients find and connect with continuing care are likely to have better outcomes post-discharge compared to those that do not help with continuing care. If you are a treating provider for an individual who is returning from residential treatment, your patient may benefit from professional and community-based continuing care, including outpatient therapy, AA/NA attendance and FDA-approved medications.
For scientists: In addition to identifying risk factors for return to use in early recovery, it may also be useful to identify factors that are associated with utilizing continuing care (i.e., facilitators and barriers to continuing care attendance). Examining the mechanisms underlying benefits of continuing care may also provide guidance for incrementally improving existing systems of care.
For policy makers: Policies that improve access to care, or that help facilitate ease of transition in the continuity of care from residential to non-residential community-based approaches, will likely provide returns on investment through improved treatment outcomes during critically risky periods following residential care.
Residential substance use disorder treatment provides 24-hour acute care for patients typically with higher levels of severity, chronicity, and complexity. Many also either offer or link to continuing care to help patients maintain gains once discharged from residential care upon re-entry to the community. Among those receiving treatment for a substance use disorder, outpatient treatment is the most common but residential care is also common: approximately 1.3 million Americans receive care in a residential treatment setting each year, representing 1/3 of those seeking treatment. Despite the intensive nature of residential treatment programs, return to substance use upon re-entry is high, and many return to their lives feeling inadequately prepared. Although continuing care – for example, providing or linking to step-down outpatient treatment – is a “best practice”, residential settings vary in their willingness to provide assistance in finding outpatient treatment following the residential stay. Many patients do not participate in any kind of continuing care and are at higher risk for relapse and recurrence. Individuals with opioid use disorder returning to substance use are at a heightened risk for overdose if they are not taking an opioid use disorder treatment medication due to reduced tolerance during the period of abstinence in residential treatment.
The goals of this study were to identify the types of outpatient services including both professional treatment and mutual-help, as well as the degree of engagement, during the first 30 days of community re-entry following residential treatment. The authors also examined associations between attendance at different types of services and substance use on the same day.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of a naturalistic longitudinal survey study. The authors recruited 128 patients discharging from two residential treatment centers in Rhode Island to participate, of whom 65 met with research staff at discharge and attended a follow-up assessment interview. Of the 63 recruited but not included, 44 did not meet with staff at discharge (e.g., participant left treatment earlier than anticipated) and 18 met with staff at discharge but did not attend the 30-day follow-up (1 participant is not accounted for in the study’s methods). To participate, patients needed to be 18 years of age or older, fluent in English, own a smartphone (due to the primary aims of the overall primary study not described in this summary), a history of traumatic experiences (also due to the primary aims of the primary study), discharge in the next 7 days, as well as no current mania, psychosis, or impairment in cognitive functioning. During the follow up assessment, participants reported (retrospectively) any substance use and treatment engagement for each day since residential treatment discharge. The researchers first wanted to characterize the types of outpatient services that patients participated in during the 30 days immediately following residential care. Types of services included community-based Alcoholics Anonymous (AA) or Narcotics Anonymous (NA) meetings, FDA-approved medications (e.g., methadone and buprenorphine for opioid use disorder and naltrexone for opioid or alcohol use disorder), outpatient therapy, inpatient treatment, emergency room visits, short-term residential, long-term residential, recovery coaching, peer support specialist services apart from recovery coaching. Anyone who did not receive one of these services were categorized as receiving no services. The authors characterized (1) how many participants were engaged in any treatment or services at all, and (2) how often they were engaged in each service during the 30-day period. Next, the authors examined whether engagement in each type of service was associated with substance use on that same day. Of note, due to the study’s sample of 65 participants, the reliability/stability of findings from sub-sets of participants may be quite low. As such, we focus the summary findings on results where 3 or more of those services in which at least 3 people reported engagement.
WHAT DID THIS STUDY FIND?
Service utilization was common in the first 30 days after residential treatment
Most of the 65 participants (54, or 83.1%) engaged in at least 1 day of treatment during the 30 days following residential care, with 47.7% engaging in 2+ services during this period. Counting non-attendees as 0 days, participants averaged 17.9 days of service utilization. AA/NA was the most common service (50.8%), followed by taking an FDA-approved medication (40%), outpatient therapy (38.5%), and inpatient hospitalization (4.6%). Only 2 participants reported an emergency room visit, and only 1 participant reported engaging in each of the following: long-term residential treatment, short-term residential treatment, working with a peer support specialist, or working with a recovery coach.
Among those who attended at least 1 Alcoholics/Narcotics Anonymous meeting, participants attended 1+ meeting, on average, for 17.6 days. Those taking medications did so on average for 28 days, whereas those engaged in outpatient therapy or inpatient treatment were engaged for overall less days during the month (11.4 and 15.3, respectively). Most (71%) of those who utilized a service did so on the first day following discharge. On average, people started AA/NA 2 days, medication assisted treatment 2.23 days, outpatient therapy 5.6 days, and inpatient treatment 14.3 days, after discharge from residential care.
Outpatient therapy was associated with reduced risk of same-day substance use
Just over 1/3 (35.4%) of participants reported alcohol or drug use in the 30 days following residential substance use treatment discharge, on average 10 days following discharge. Descriptively, different services were associated with different rates of return to use. Among those taking a medication, 50% returned to use, followed by inpatient treatment (33%), outpatient therapy (16%), and Alcoholics/Narcotics anonymous (16%). See the figure below for return to use during the 30 days after residential discharge by service utilization. Similarly, the number of days until return to use occurred differed by service. Of those who attended Alcoholics/Narcotics Anonymous and returned to use did so, on average, 15.4 days after discharge. Of those who took medication and returned to use, they did so 9 days after discharge on average, and of those who attended outpatient treatment and returned to use, they did so 7 days after discharge on average.
On days that participants reported any (versus no) outpatient therapy, substance use was significantly less likely on that same day controlling for use of other service. On days that participants reported taking an FDA-approved medication for alcohol or opioid use disorder, they were more likely to report substance use on that same day. No other service utilization on a given day was significantly associated with substance use on that same day.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study of a small sample of adults followed after residential treatment found that 4 out of every 5 individuals made contact with some treatment or recovery support service in the month following discharge, and that of those who engaged with continuing care, most did so on the first day after discharge. This suggests that many in this study received the necessary care transition to help facilitate sustained recovery. The most common form of follow up service was attendance at a 12-step mutual-help NA or AA group – both of which are widely available in the community and online and free to access. The results suggested that these mutual-help groups are associated with low rates of return to use as well.
A very important and substantial limitation of the results reported in this study, however, is that the study included only participants that met with staff at discharge and attended the follow-up assessment – 51% of those eligible. These continuing care service utilization rates may be overestimates as they do not include the 49% who may have left residential treatment or otherwise had risk factors both to miss the follow-up and not utilize continuing care (e.g., relapse or otherwise having difficulty functioning). Even among those participants who were included, analyses did not account for important individual factors like clinical severity. That said, while the current study did not include rigorous tests of mutual-help participation effects on substance use outcomes, many high-quality studies, mostly focused on AA for alcohol use disorder, show that AA participation reduces alcohol and other drug use, while increasing rates of abstinence and remission.
One interesting finding was that substance use was less likely on days when outpatient services were received, whereas this was not the case for any other service, including AA/NA attendance which had an overall low rate of return to use across the 30 day follow-up. One possibility is that many 12-step community meetings occur in the evening whereas treatment is often delivered during the day. Especially for individuals in early recovery – as was the case here for participants – activities during the morning/day may help increase participants’ motivation, provide reminders on coping skills cultivated during residential, or plan for risky situations to be encountered later that day/evening, especially for those not employed or who have less structured daytime hours. Future research using multiple daily assessments, such as ecological momentary assessment, of different types of service engagement may help tease apart these same-day effects.
Beyond AA/NA and outpatient treatment, those engaging in other services still saw more favorable rates of continued sobriety across the entire 30-day period compared to those that did not engage in any services during this period. Half of those taking an FDA-approved medication, and 1 in 3 of those who used inpatient services, used alcohol or other drugs on at least 1 in 30 days. Regarding daily service utilization and substance use, it is unclear why taking a medication was associated with an increased risk of substance use on any given day. Those prescribed medications may have had more severe or more chronic patterns of substance use prior to residential treatment entry which can be a predictor of higher rates of return to use post-treatment. Important clinical variables such as clinical severity/chronicity and primary substance (e.g., alcohol, opioid, stimulants, etc.) were not included in these models. Alternatively, these participants may be more likely to use multiple substances, and the medications may be geared toward reducing use of one, but not all, substances (e.g., buprenorphine to address opioid use but not alcohol use). Regardless, rates of return to use were better among those who took a medication relative to those who did not engage in any kind of service following residential. Of the full sample, 17% of those stepping down from residential treatment did not engage in any care, and of those, 70% reported a return to use event in the first 30 days following residential. There are likely to be important differences between those who utilized services (e.g., more motivated, more of other kinds of recovery capital, better access to care, etc.) and those who did not, potentially providing an additional partial explanation for the better outcomes among those who utilized a continuing care service. At the same time, these largely descriptive data are consistent with other more rigorous studies that show various outpatient therapies, mutual-help groups, and FDA-approved medications improve short-term and long-term recovery outcomes. Of note, however, the study did not include recovery residences in their assessment of continuing care after residential, which has been shown to improve substance use outcomes after residential treatment. Nevertheless, these results highlight the importance of continuing care for sustaining progress made in recovery during residential into the first month after discharge.
Although the authors initially attempted to recruit 141 participants, 76 participants did not complete the follow-up survey for various reasons. Those who were still engaged in research after the first month may have different characteristics or patterns of recovery over the month following residential care compared to those who did not complete the follow up.
Analyses examined one service at a time (e.g., outpatient vs. no outpatient, AA/NA vs. no AA/NA, etc.). It is possible that use of multiple services (e.g., taking a medication and attending outpatient treatment) would provide additional protection but this was not tested empirically.
BOTTOM LINE
In combination with many other rigorous studies of continuing care after residential treatment, this study highlights the utility of empirically-supported services such as outpatient therapy, 12-step mutual-help attendance, and FDA-approved medications early in recovery after discharge from residential care.
For individuals and families seeking recovery: The period after residential treatment is a risky period for return to use. However, people who utilize empirically-supported services like outpatient therapy, mutual-help, and FDA-approved medications tend to have better outcomes. If you or a loved one is returning from residential care, engaging in outpatient therapy or AA/NA may buffer against the risk of return to use in the first month as these tend to bolster and boost relapse prevention coping skills and keep cognitive vigilance at a high level.
For treatment professionals and treatment systems: Residential programs that facilitate or provide assistance with helping patients find and connect with continuing care are likely to have better outcomes post-discharge compared to those that do not help with continuing care. If you are a treating provider for an individual who is returning from residential treatment, your patient may benefit from professional and community-based continuing care, including outpatient therapy, AA/NA attendance and FDA-approved medications.
For scientists: In addition to identifying risk factors for return to use in early recovery, it may also be useful to identify factors that are associated with utilizing continuing care (i.e., facilitators and barriers to continuing care attendance). Examining the mechanisms underlying benefits of continuing care may also provide guidance for incrementally improving existing systems of care.
For policy makers: Policies that improve access to care, or that help facilitate ease of transition in the continuity of care from residential to non-residential community-based approaches, will likely provide returns on investment through improved treatment outcomes during critically risky periods following residential care.
Residential substance use disorder treatment provides 24-hour acute care for patients typically with higher levels of severity, chronicity, and complexity. Many also either offer or link to continuing care to help patients maintain gains once discharged from residential care upon re-entry to the community. Among those receiving treatment for a substance use disorder, outpatient treatment is the most common but residential care is also common: approximately 1.3 million Americans receive care in a residential treatment setting each year, representing 1/3 of those seeking treatment. Despite the intensive nature of residential treatment programs, return to substance use upon re-entry is high, and many return to their lives feeling inadequately prepared. Although continuing care – for example, providing or linking to step-down outpatient treatment – is a “best practice”, residential settings vary in their willingness to provide assistance in finding outpatient treatment following the residential stay. Many patients do not participate in any kind of continuing care and are at higher risk for relapse and recurrence. Individuals with opioid use disorder returning to substance use are at a heightened risk for overdose if they are not taking an opioid use disorder treatment medication due to reduced tolerance during the period of abstinence in residential treatment.
The goals of this study were to identify the types of outpatient services including both professional treatment and mutual-help, as well as the degree of engagement, during the first 30 days of community re-entry following residential treatment. The authors also examined associations between attendance at different types of services and substance use on the same day.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of a naturalistic longitudinal survey study. The authors recruited 128 patients discharging from two residential treatment centers in Rhode Island to participate, of whom 65 met with research staff at discharge and attended a follow-up assessment interview. Of the 63 recruited but not included, 44 did not meet with staff at discharge (e.g., participant left treatment earlier than anticipated) and 18 met with staff at discharge but did not attend the 30-day follow-up (1 participant is not accounted for in the study’s methods). To participate, patients needed to be 18 years of age or older, fluent in English, own a smartphone (due to the primary aims of the overall primary study not described in this summary), a history of traumatic experiences (also due to the primary aims of the primary study), discharge in the next 7 days, as well as no current mania, psychosis, or impairment in cognitive functioning. During the follow up assessment, participants reported (retrospectively) any substance use and treatment engagement for each day since residential treatment discharge. The researchers first wanted to characterize the types of outpatient services that patients participated in during the 30 days immediately following residential care. Types of services included community-based Alcoholics Anonymous (AA) or Narcotics Anonymous (NA) meetings, FDA-approved medications (e.g., methadone and buprenorphine for opioid use disorder and naltrexone for opioid or alcohol use disorder), outpatient therapy, inpatient treatment, emergency room visits, short-term residential, long-term residential, recovery coaching, peer support specialist services apart from recovery coaching. Anyone who did not receive one of these services were categorized as receiving no services. The authors characterized (1) how many participants were engaged in any treatment or services at all, and (2) how often they were engaged in each service during the 30-day period. Next, the authors examined whether engagement in each type of service was associated with substance use on that same day. Of note, due to the study’s sample of 65 participants, the reliability/stability of findings from sub-sets of participants may be quite low. As such, we focus the summary findings on results where 3 or more of those services in which at least 3 people reported engagement.
WHAT DID THIS STUDY FIND?
Service utilization was common in the first 30 days after residential treatment
Most of the 65 participants (54, or 83.1%) engaged in at least 1 day of treatment during the 30 days following residential care, with 47.7% engaging in 2+ services during this period. Counting non-attendees as 0 days, participants averaged 17.9 days of service utilization. AA/NA was the most common service (50.8%), followed by taking an FDA-approved medication (40%), outpatient therapy (38.5%), and inpatient hospitalization (4.6%). Only 2 participants reported an emergency room visit, and only 1 participant reported engaging in each of the following: long-term residential treatment, short-term residential treatment, working with a peer support specialist, or working with a recovery coach.
Among those who attended at least 1 Alcoholics/Narcotics Anonymous meeting, participants attended 1+ meeting, on average, for 17.6 days. Those taking medications did so on average for 28 days, whereas those engaged in outpatient therapy or inpatient treatment were engaged for overall less days during the month (11.4 and 15.3, respectively). Most (71%) of those who utilized a service did so on the first day following discharge. On average, people started AA/NA 2 days, medication assisted treatment 2.23 days, outpatient therapy 5.6 days, and inpatient treatment 14.3 days, after discharge from residential care.
Outpatient therapy was associated with reduced risk of same-day substance use
Just over 1/3 (35.4%) of participants reported alcohol or drug use in the 30 days following residential substance use treatment discharge, on average 10 days following discharge. Descriptively, different services were associated with different rates of return to use. Among those taking a medication, 50% returned to use, followed by inpatient treatment (33%), outpatient therapy (16%), and Alcoholics/Narcotics anonymous (16%). See the figure below for return to use during the 30 days after residential discharge by service utilization. Similarly, the number of days until return to use occurred differed by service. Of those who attended Alcoholics/Narcotics Anonymous and returned to use did so, on average, 15.4 days after discharge. Of those who took medication and returned to use, they did so 9 days after discharge on average, and of those who attended outpatient treatment and returned to use, they did so 7 days after discharge on average.
On days that participants reported any (versus no) outpatient therapy, substance use was significantly less likely on that same day controlling for use of other service. On days that participants reported taking an FDA-approved medication for alcohol or opioid use disorder, they were more likely to report substance use on that same day. No other service utilization on a given day was significantly associated with substance use on that same day.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study of a small sample of adults followed after residential treatment found that 4 out of every 5 individuals made contact with some treatment or recovery support service in the month following discharge, and that of those who engaged with continuing care, most did so on the first day after discharge. This suggests that many in this study received the necessary care transition to help facilitate sustained recovery. The most common form of follow up service was attendance at a 12-step mutual-help NA or AA group – both of which are widely available in the community and online and free to access. The results suggested that these mutual-help groups are associated with low rates of return to use as well.
A very important and substantial limitation of the results reported in this study, however, is that the study included only participants that met with staff at discharge and attended the follow-up assessment – 51% of those eligible. These continuing care service utilization rates may be overestimates as they do not include the 49% who may have left residential treatment or otherwise had risk factors both to miss the follow-up and not utilize continuing care (e.g., relapse or otherwise having difficulty functioning). Even among those participants who were included, analyses did not account for important individual factors like clinical severity. That said, while the current study did not include rigorous tests of mutual-help participation effects on substance use outcomes, many high-quality studies, mostly focused on AA for alcohol use disorder, show that AA participation reduces alcohol and other drug use, while increasing rates of abstinence and remission.
One interesting finding was that substance use was less likely on days when outpatient services were received, whereas this was not the case for any other service, including AA/NA attendance which had an overall low rate of return to use across the 30 day follow-up. One possibility is that many 12-step community meetings occur in the evening whereas treatment is often delivered during the day. Especially for individuals in early recovery – as was the case here for participants – activities during the morning/day may help increase participants’ motivation, provide reminders on coping skills cultivated during residential, or plan for risky situations to be encountered later that day/evening, especially for those not employed or who have less structured daytime hours. Future research using multiple daily assessments, such as ecological momentary assessment, of different types of service engagement may help tease apart these same-day effects.
Beyond AA/NA and outpatient treatment, those engaging in other services still saw more favorable rates of continued sobriety across the entire 30-day period compared to those that did not engage in any services during this period. Half of those taking an FDA-approved medication, and 1 in 3 of those who used inpatient services, used alcohol or other drugs on at least 1 in 30 days. Regarding daily service utilization and substance use, it is unclear why taking a medication was associated with an increased risk of substance use on any given day. Those prescribed medications may have had more severe or more chronic patterns of substance use prior to residential treatment entry which can be a predictor of higher rates of return to use post-treatment. Important clinical variables such as clinical severity/chronicity and primary substance (e.g., alcohol, opioid, stimulants, etc.) were not included in these models. Alternatively, these participants may be more likely to use multiple substances, and the medications may be geared toward reducing use of one, but not all, substances (e.g., buprenorphine to address opioid use but not alcohol use). Regardless, rates of return to use were better among those who took a medication relative to those who did not engage in any kind of service following residential. Of the full sample, 17% of those stepping down from residential treatment did not engage in any care, and of those, 70% reported a return to use event in the first 30 days following residential. There are likely to be important differences between those who utilized services (e.g., more motivated, more of other kinds of recovery capital, better access to care, etc.) and those who did not, potentially providing an additional partial explanation for the better outcomes among those who utilized a continuing care service. At the same time, these largely descriptive data are consistent with other more rigorous studies that show various outpatient therapies, mutual-help groups, and FDA-approved medications improve short-term and long-term recovery outcomes. Of note, however, the study did not include recovery residences in their assessment of continuing care after residential, which has been shown to improve substance use outcomes after residential treatment. Nevertheless, these results highlight the importance of continuing care for sustaining progress made in recovery during residential into the first month after discharge.
Although the authors initially attempted to recruit 141 participants, 76 participants did not complete the follow-up survey for various reasons. Those who were still engaged in research after the first month may have different characteristics or patterns of recovery over the month following residential care compared to those who did not complete the follow up.
Analyses examined one service at a time (e.g., outpatient vs. no outpatient, AA/NA vs. no AA/NA, etc.). It is possible that use of multiple services (e.g., taking a medication and attending outpatient treatment) would provide additional protection but this was not tested empirically.
BOTTOM LINE
In combination with many other rigorous studies of continuing care after residential treatment, this study highlights the utility of empirically-supported services such as outpatient therapy, 12-step mutual-help attendance, and FDA-approved medications early in recovery after discharge from residential care.
For individuals and families seeking recovery: The period after residential treatment is a risky period for return to use. However, people who utilize empirically-supported services like outpatient therapy, mutual-help, and FDA-approved medications tend to have better outcomes. If you or a loved one is returning from residential care, engaging in outpatient therapy or AA/NA may buffer against the risk of return to use in the first month as these tend to bolster and boost relapse prevention coping skills and keep cognitive vigilance at a high level.
For treatment professionals and treatment systems: Residential programs that facilitate or provide assistance with helping patients find and connect with continuing care are likely to have better outcomes post-discharge compared to those that do not help with continuing care. If you are a treating provider for an individual who is returning from residential treatment, your patient may benefit from professional and community-based continuing care, including outpatient therapy, AA/NA attendance and FDA-approved medications.
For scientists: In addition to identifying risk factors for return to use in early recovery, it may also be useful to identify factors that are associated with utilizing continuing care (i.e., facilitators and barriers to continuing care attendance). Examining the mechanisms underlying benefits of continuing care may also provide guidance for incrementally improving existing systems of care.
For policy makers: Policies that improve access to care, or that help facilitate ease of transition in the continuity of care from residential to non-residential community-based approaches, will likely provide returns on investment through improved treatment outcomes during critically risky periods following residential care.