Can human support enhance the effectiveness of a digital alcohol use intervention?
Digital alcohol interventions demonstrate promise as accessible, cost-effective tools for reducing alcohol use, yet their implementation in real world settings remain limited. This study tested whether adding peer support specialists or health coaches to a digital alcohol intervention reduced heavy drinking days and improved quality of life compared to a self-managed digital alcohol app intervention for individuals with mild-to-moderate alcohol use disorder.
Alcohol misuse, including binge and heavy drinking, poses significant public health risks. More than 1 in 5 Americans – 61.2 million people – report binge drinking, defined as drinking 5 or more drinks on an occasion for men and 4 or more for women in the past month. For those who binge drink but do not meet criteria for an alcohol use disorder, this pattern of drinking over time can increase the risk for developing alcohol use disorder later in life, while representing a significant risk factor for accidents and injuries as well as disease and disability, irrespective of whether it is part of a pattern meeting clinical thresholds for alcohol use disorder. At the same time, early intervention strategies designed to reduce binge and heavy drinking (irrespective of clinical thresholds) can also help prevent the escalation from milder to more severe forms of alcohol use disorder, thereby reducing long-term harms.
Digital technology offers a promising cost-effective solution that might help extend the reach of evidence-based treatments for those who wish to quit or cut down on their alcohol use. Many digital interventions – e.g., delivered by smartphone application – while shown to be helpful ways of enhancing or maintaining alcohol abstinence, have targeted individuals with more severe alcohol use disorder receiving (or who had received) services in specialty substance use disorder treatment. In non-clinical samples, digital alcohol interventions have consistently shown modest but robust effects on reducing alcohol use up to 6 months, which given their low-cost and potential reach could make a significant public health impact. However, the real-world implementation of digital alcohol interventions is limited, and questions remain about whether adding human support – such as guidance from peer support specialists (e.g., recovery coaches) or health coaches – can improve them. Given the added costs of providing human support, a question remains as to whether it is worth the investment. This study aimed to fill this gap by testing the effectiveness of a digital alcohol app intervention for reducing heavy drinking and enhancing quality of life among individuals with risky alcohol use and/or mild-to-moderate alcohol use disorder – the primary goal was to test whether outcomes were different with and without human support (either peer support specialists or health coaches).
HOW WAS THIS STUDY CONDUCTED?
This study used a 12-month randomized controlled trial to evaluate both the effects of the digital, remotely-delivered intervention on alcohol use outcomes and quality of life. There was a 3-month intervention period with incentives and a 9-month follow-up period including 3-, 6-, and 12-month follow-up assessments.
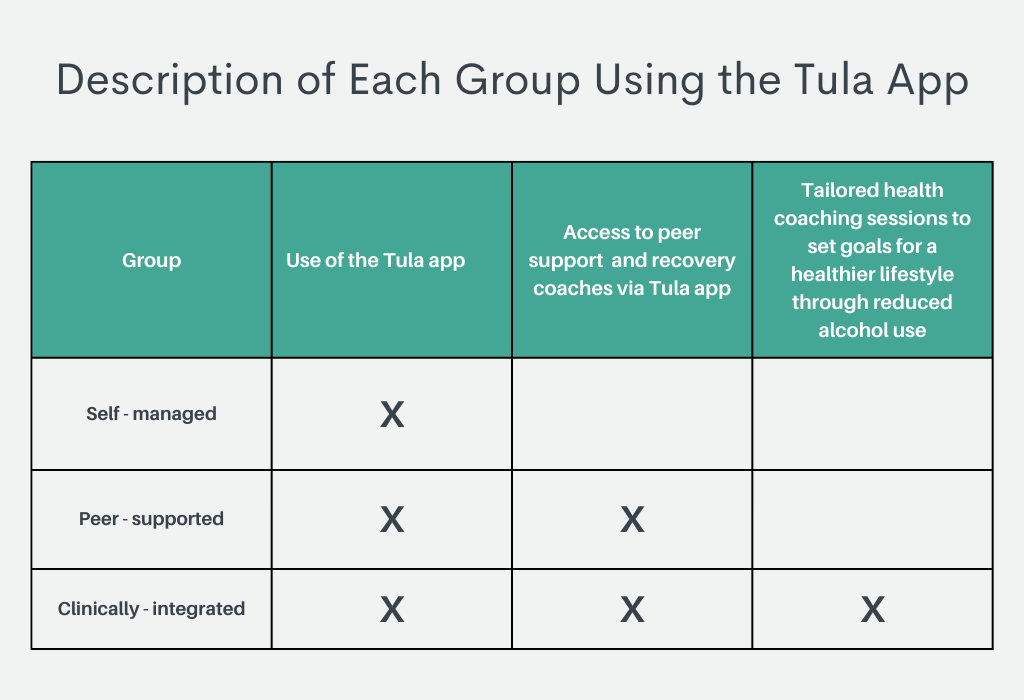
Between March 2020 and September 2023, participants were recruited across Wisconsin and the Upper Midwest through clinical sites, community organizations, and public media. Interested individuals remotely completed a web-based screening survey and eligibility criteria included: age 21 or older, a desire to reduce drinking, and a current drinking pattern associated with either risky/hazardous alcohol use and/or mild-to-moderate alcohol use disorder. This was operationally defined as meeting any of the following 3 criteria: 1) scoring at least an 8 or higher on the Alcohol Use Disorders Identification Test; 2) meeting at least 2 out of 11 DSM-5 symptoms; or 3) reporting moderate- to high-risk drinking patterns (e.g., 4+ drinks on a single occasion and >7 drinks per week for women; 5+ drinks on any single day and >14 drinks per week for men). Those with more severe drinking patterns (6 or more DSM-5 symptoms) were excluded from the study. To enroll in the study, eligible participants had to download the digital alcohol intervention app (called “Tula”), complete the baseline survey, and schedule a phone call with a study team member within 72 hours of completing the screener. Enrolled participants were then randomized to one of three groups, each with access to the basic content in the Tula app but varying levels of human support provided remotely, online: 1) self-managed group (no human support; n = 185), 2) peer-supported group (moderate human support; n = 186), or 3) clinically integrated group (high human support; n = 187). Participants were mostly white (91%), female (66%), and highly educated (72% had at least a bachelor’s degree) with an average age of about 43 years.
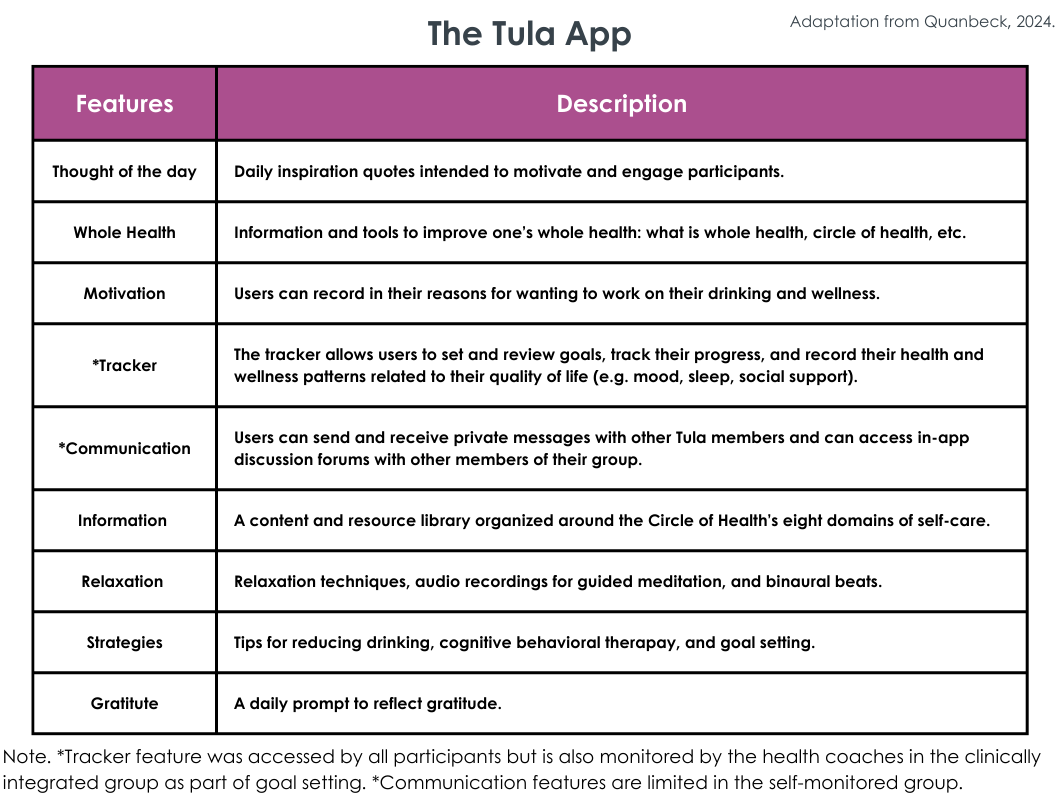
The digital alcohol intervention tested in this study, Tula, was adapted from the Addiction-Comprehensive Health Enhancement Support System (A-CHESS), a digital alcohol app previously shown to be helpful in reducing heavy drinking. Tula stripped components of A-CHESS that were focused on abstinence as a part of recovery from severe alcohol use disorder and instead adapted the focus to reducing alcohol consumption for individuals with mild-to-moderate alcohol use disorder. Intervention components (e.g., motivational content, progress tracking, relaxation exercises) included in the digital app are detailed in the figure below.
Participants in the self-managed group independently used the app with no external support, similar to a commercially available app. Those in the peer-supported group, in addition to the basic content features of the Tula app, also had access to social support from others in the study via an online discussion forum built into the app and could engage (either through the discussion forum or private messaging) with certified peer specialists (substance use disorder recovery coaches with lived experience with substance use disorder). Recovery coaches were not assigned to individual participants. Those in the clinically integrated group, in addition to the Tula app and discussion forum with other participants assigned to their study arm, also private messaged one-on-one with health coaches to set goals for a healthier lifestyle through reduced alcohol use and were offered up to three health coaching sessions over the phone.
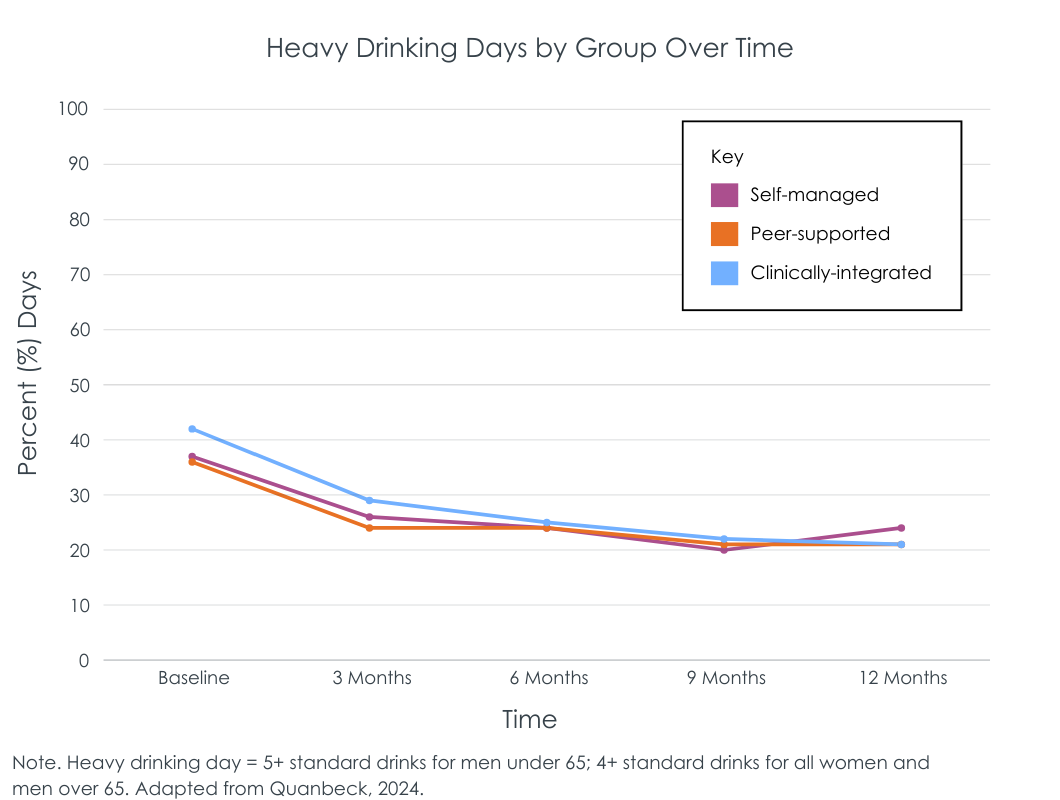
Participants completed weekly check-ins via the Tula App and quarterly follow-up assessments at 3, 6, 9, and 12 months. Primary outcomes were the number of heavy drinking days in the last 7 days (defined as number of days consuming 5+ standard drinks for men under 65, or 4+ standard drinks for women and men over 65 on any day based on the 7-day timeline follow-back survey) and quality of life (measured using the Patient-Reported Outcome Measurement Information System). To calculate the percentage of heavy drinking days for each participant, the researchers divided the number of weekly heavy drinking days by 7. The researchers used longitudinal mixed effects models to analyze changes in outcomes between study arms at 3-, 6-, 9-, and 12-month follow-ups, employing an intent-to-treat approach such that individuals were analyzed in the group to which they were assigned irrespective of how much or little treatment was received. They hypothesized that participants in both the clinically integrated group and peer-supported group would experience greater reductions in heavy drinking days and improvements in quality of life compared to the self-managed group, with the clinically integrated digital intervention expected to be more effective than the peer-supported digital intervention.
Participants were 43 years old, on average. Two-thirds identified as female. Most (91%) identified as White, while 5% identified as Black and smaller percentages identified as Latino and Asian. The sample had high levels of education, overall, with 70% having earned a Bachelor’s degree or higher. Their average AUDIT score was 12 (SD = 6), consistent with hazardous/harmful drinking, but not severe alcohol use disorder. Indeed, two-thirds met criteria for mild alcohol use disorder (2-3 symptoms) and then others for moderate (4-5 symptoms).
WHAT DID THIS STUDY FIND?
Participants were willing to engage with the app, though usage declined over time
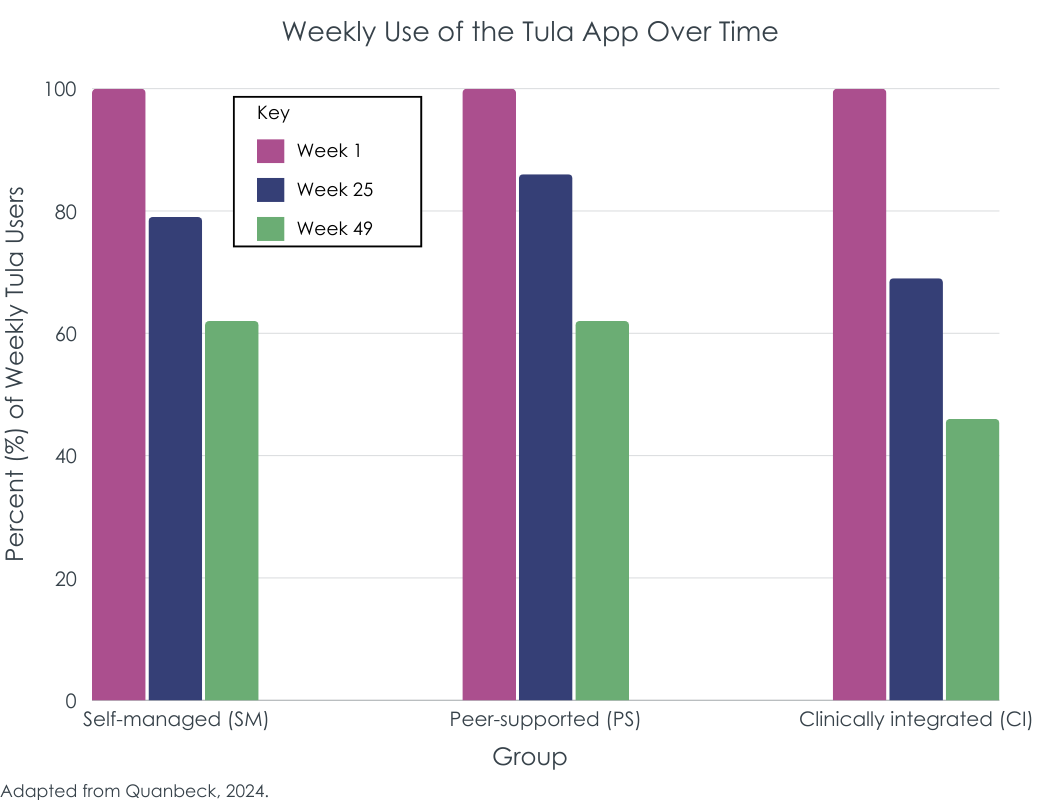
Throughout the 12-month study period, participants completed 70% (28 out of 40) of the weekly check-in surveys via the Tula app. Those in the peer-supported group and clinically integrated groups also had access to the Tula group discussion boards. Among participants in the peer-supported group, most (96%) read discussion forum messages, and slightly more than half (52%) posted at least one message. In the clinically integrated group, 97% of participants read posts to the discussion board, but only about 1 in 4 (28%) contributed at least one message. Additionally, 67% of participants in the clinically integrated group used the available health coaching phone calls, with an average number of 1.7 calls per participant. While more than 9 out of 10 participants in each of the three study arms used the Tula app in the first week, weekly usage steadily declined across all groups over time. By the end of the study, between 60-70% of those in the self-managed and peer-supported groups were using the app on a weekly basis, while weekly usage in the clinically integrated group dipped below 50%.
Heavy drinking decreased across all groups from baseline to 12 months, with no significant differences between groups
Across all three groups, the percentage of heavy drinking days decreased from 38.4% at baseline to 22.5% at 12-month follow up. There was no difference on the reduction in heavy drinking days across the groups during the 12-month study window, overall; however, there were additional significant reductions in heavy drinking days just between months 3 and 9 for the clinically integrated group that were not observed in the peer-supported and self-managed groups. That said, there were high study non-completion rates in the clinically integrated group compared to the other two intervention groups, which may distort or potentially inflate the benefits here assuming those who did not complete the study and dropped out had worse outcomes.
Quality of life remained largely unchanged, with minimal differences between study conditions
Physical health scores were stable from baseline to 12 months across all groups. Mental health scores improved slightly from baseline to 12 months for all three groups, with the clinically integrated (5.9%) and peer-supported groups (4.8%) experiencing slightly greater increases than the self-managed group (2.6%). Participants in the clinically integrated group reported significantly higher mental health scores compared to the self-managed group, particularly at 9 and 12 months. However, extremely high non-completion in the clinically integrated group may have accounted for this (only 55% of this group completed the assessment at the 12-month follow-up point)– such that those dropping out had worse mental health, potentially inflating the clinically integrated group’s positive effect on mental health.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study compared the effectiveness of a digital alcohol intervention app with varying levels of human support (no support, peer support, or clinical integration with health coaching) for reducing heavy drinking in individuals with mild-to-moderate alcohol use disorder. Somewhat surprisingly, despite different levels and types of available human support across the groups to which study participants were assigned there was no meaningful differences detected across the different groups in any of the outcomes of focus. Across all groups, the percentage of heavy drinking days decreased from an average of 38.4% at baseline to 22.5% at 12 months, representing a 41% relative reduction from baseline. While the clinical and societal significance of this reduction warrants further exploration, reducing heavy drinking lowers risks of alcohol-related injury and mortality. Achieving similar heavy drinking reductions at scale could result in significant public health impacts.
This study adds to existing evidence supporting digital alcohol interventions for effectively reducing alcohol consumption. All three intervention models – self-managed, peer-supported, and clinically integrated – reduced heavy drinking days. The digital alcohol app used in this study, Tula, was adapted from an existing empirically-supported app (A-CHESS) and incorporated features such as drink tracking and goal setting that are commonly used in empirically supported digital alcohol interventions. Such features may serve as foundational elements to build off of in future digital intervention development efforts. Results from this study also suggest that self-managed use of the digital alcohol app was just as helpful alone for reducing heavy drinking in individuals with mild-to-moderate alcohol use disorder as the versions with added human support from a peer-support specialist or health coach. This aligns with prior studies that have shown that adding human support to digital alcohol interventions did not result in improved outcomes, on average. However, meta-analyses have produced mixed results on the topic. While a meta-analysis of digital alcohol interventions indicated that human-supported interventions resulted in greater reductions in heavy drinking than fully automated interventions, others have found no additional benefit. One possible explanation for the lack of added benefit in this study’s peer-supported group is that participants were not each individually assigned a peer-support specialist but rather simply had the option to reach out via private message or discussion board. Future studies could investigate whether having more direct interaction – such as outreach phone calls or scheduled virtual meetings with a peer-support specialist – results in improved outcomes beyond those of the self-managed group.
Notably, there were higher attrition rates in the clinically integrated group, which required participants to engage in 1-on-1 messaging with a health coach to discuss goals for reducing alcohol use and provided access to up to 3 phone calls with the health coach. Although about 2 out of 3 participants opted for at least one phone call with a health coach, those who dropped out may have preferred a more autonomous approach, finding the direct interaction with a health coach too intensive for their needs.
Findings underscore the importance of better understanding which individuals in particular may prefer or benefit from human support added to digital alcohol interventions and to what extent and which may prefer a more autonomous, self-directed approach. Giving individuals choices as to the type of digital alcohol intervention they feel they need and prefer may be helpful.
Findings also indicate that the self-managed intervention produced similar effects on quality of life, including physical and mental health, as the peer-supported and clinically integrated versions. Although participants in the clinically integrated group experienced significantly greater improvements in mental health scores compared to the self-managed group, high attrition in the clinically integrated group (only 55% completed the 12 month follow up) complicates interpretation. Sensitivity analysis suggested the improvements in mental health observed in the clinically integrated group may be because those who dropped out of the study had worse baseline mental health. Thus, the better mental health in the clinically integrated group in the follow up assessments may be explained by those that were successfully followed up in the study having generally better mental health to begin with.
High attrition rates in the clinically integrated group limit the interpretation of findings for that group. Although the researchers used an intent-to-treat approach, participants who dropped out of the study may differ systematically from those who remained (e.g., may be less motivated), potentially affecting the results.
The study’s population consisted of primarily white, middle-aged, highly educated individuals, and may limit generalizability to broader populations of individuals engaged in patterns of drinking associated with mild-to-moderate alcohol use disorder.
BOTTOM LINE
This study compared the effectiveness of a digital alcohol intervention app with and without varying levels of human support (peer support specialists or health coaches) for reducing heavy drinking and improving quality of life in individuals with mild-to-moderate alcohol use disorder. Adding human support to the digital format did not improve outcomes. Results showed that all groups reduced their percentage of heavy drinking days from baseline (38.4%) to 12 months (22.5%) and experienced slight improvements in mental health. These findings indicate that a self-managed digital alcohol app could be a cost-effective option for health systems seeking to support individuals aiming to reduce or quit drinking. However, further research is needed to determine whether certain individuals may prefer – and benefit more from – digital alcohol interventions with and without varying levels of human support.
For individuals and families seeking recovery: For those with mild-to-moderate alcohol use disorder and a goal to reduce alcohol consumption, digital alcohol reduction interventions can be an accessible and effective tool to support self-managed efforts to reduce heavy drinking, especially for those who lack access to or prefer not to engage in more formal or in-person options. This study found that adding human support (from a peer-support specialist or health coach) did not improve effectiveness for reducing heavy drinking. However, some individuals, particularly those with more severe alcohol use disorder (not included in this study), may benefit from pairing digital alcohol interventions with formal treatment services or additional human support.
For treatment professionals and treatment systems: Digital alcohol interventions, including the app tested in this study, have been shown to be helpful in reducing alcohol use and problems among individuals with mild-to-moderate alcohol use disorder. Connecting patients who screen positive for mild-to-moderate alcohol use disorder in healthcare settings – and who express a desire to reduce their drinking through self-directed efforts – with digital alcohol interventions may be a beneficial approach. That said, real world engagement without the structure and support of being in a clinical study may result in different results and potentially more disengagement over time than what was observed here. Treatment providers could expand offerings to include a range of digital and hybrid options to assist individuals in their efforts to quit or cut down on their alcohol use, providing flexible support that can accommodate the diverse preferences and needs of broader population of at-risk drinkers.
For scientists: While digital alcohol interventions show promise for reducing alcohol use among heavy drinkers, there is limited understanding on how best to implement them in real-world settings without the structure of a clinical program to help with engagement over time. Evidence on the benefits of adding human support to self-directed digital alcohol interventions is mixed, with this study finding that adding human support did not improve outcomes. Better understanding how to enhance the effectiveness of digital alcohol interventions with human support – and identifying who is most likely to prefer or benefit from such support compared to a self-guided approach – could improve engagement and outcomes. Future research could explore whether specific groups (based on demographics, drinking goals, or personality) benefit more from human-supported digital alcohol interventions, and which may prefer or benefit more from an autonomous, self-directed approach. These studies could also investigate whether having more direct interaction – such as outreach phone calls or scheduled virtual meetings with a peer-support specialist – results in improved outcomes beyond those of the self-managed group.
For policy makers: Implementing scalable, cost-effective digital alcohol interventions like Tula can help reduce barriers to treatment and allow health systems to expand access without straining resources to a variety of supports for individuals with alcohol use disorder who wish to reduce or quit their drinking. This study showed that the more resource-friendly, self-managed access to the app produced similar outcomes to the app with additional available support from a recovery or health coach. Increased funding is needed, however, to identify how best to implement digital alcohol interventions – with and without varying levels of human support – to maximize their impact across the broad population of individuals engaged in heavy drinking. Funding this research would help to ensure that resources are allocated efficiently to most effectively support the broadest spectrum of people who use alcohol in harmful or hazardous ways.
Alcohol misuse, including binge and heavy drinking, poses significant public health risks. More than 1 in 5 Americans – 61.2 million people – report binge drinking, defined as drinking 5 or more drinks on an occasion for men and 4 or more for women in the past month. For those who binge drink but do not meet criteria for an alcohol use disorder, this pattern of drinking over time can increase the risk for developing alcohol use disorder later in life, while representing a significant risk factor for accidents and injuries as well as disease and disability, irrespective of whether it is part of a pattern meeting clinical thresholds for alcohol use disorder. At the same time, early intervention strategies designed to reduce binge and heavy drinking (irrespective of clinical thresholds) can also help prevent the escalation from milder to more severe forms of alcohol use disorder, thereby reducing long-term harms.
Digital technology offers a promising cost-effective solution that might help extend the reach of evidence-based treatments for those who wish to quit or cut down on their alcohol use. Many digital interventions – e.g., delivered by smartphone application – while shown to be helpful ways of enhancing or maintaining alcohol abstinence, have targeted individuals with more severe alcohol use disorder receiving (or who had received) services in specialty substance use disorder treatment. In non-clinical samples, digital alcohol interventions have consistently shown modest but robust effects on reducing alcohol use up to 6 months, which given their low-cost and potential reach could make a significant public health impact. However, the real-world implementation of digital alcohol interventions is limited, and questions remain about whether adding human support – such as guidance from peer support specialists (e.g., recovery coaches) or health coaches – can improve them. Given the added costs of providing human support, a question remains as to whether it is worth the investment. This study aimed to fill this gap by testing the effectiveness of a digital alcohol app intervention for reducing heavy drinking and enhancing quality of life among individuals with risky alcohol use and/or mild-to-moderate alcohol use disorder – the primary goal was to test whether outcomes were different with and without human support (either peer support specialists or health coaches).
HOW WAS THIS STUDY CONDUCTED?
This study used a 12-month randomized controlled trial to evaluate both the effects of the digital, remotely-delivered intervention on alcohol use outcomes and quality of life. There was a 3-month intervention period with incentives and a 9-month follow-up period including 3-, 6-, and 12-month follow-up assessments.
Between March 2020 and September 2023, participants were recruited across Wisconsin and the Upper Midwest through clinical sites, community organizations, and public media. Interested individuals remotely completed a web-based screening survey and eligibility criteria included: age 21 or older, a desire to reduce drinking, and a current drinking pattern associated with either risky/hazardous alcohol use and/or mild-to-moderate alcohol use disorder. This was operationally defined as meeting any of the following 3 criteria: 1) scoring at least an 8 or higher on the Alcohol Use Disorders Identification Test; 2) meeting at least 2 out of 11 DSM-5 symptoms; or 3) reporting moderate- to high-risk drinking patterns (e.g., 4+ drinks on a single occasion and >7 drinks per week for women; 5+ drinks on any single day and >14 drinks per week for men). Those with more severe drinking patterns (6 or more DSM-5 symptoms) were excluded from the study. To enroll in the study, eligible participants had to download the digital alcohol intervention app (called “Tula”), complete the baseline survey, and schedule a phone call with a study team member within 72 hours of completing the screener. Enrolled participants were then randomized to one of three groups, each with access to the basic content in the Tula app but varying levels of human support provided remotely, online: 1) self-managed group (no human support; n = 185), 2) peer-supported group (moderate human support; n = 186), or 3) clinically integrated group (high human support; n = 187). Participants were mostly white (91%), female (66%), and highly educated (72% had at least a bachelor’s degree) with an average age of about 43 years.
The digital alcohol intervention tested in this study, Tula, was adapted from the Addiction-Comprehensive Health Enhancement Support System (A-CHESS), a digital alcohol app previously shown to be helpful in reducing heavy drinking. Tula stripped components of A-CHESS that were focused on abstinence as a part of recovery from severe alcohol use disorder and instead adapted the focus to reducing alcohol consumption for individuals with mild-to-moderate alcohol use disorder. Intervention components (e.g., motivational content, progress tracking, relaxation exercises) included in the digital app are detailed in the figure below.
Participants in the self-managed group independently used the app with no external support, similar to a commercially available app. Those in the peer-supported group, in addition to the basic content features of the Tula app, also had access to social support from others in the study via an online discussion forum built into the app and could engage (either through the discussion forum or private messaging) with certified peer specialists (substance use disorder recovery coaches with lived experience with substance use disorder). Recovery coaches were not assigned to individual participants. Those in the clinically integrated group, in addition to the Tula app and discussion forum with other participants assigned to their study arm, also private messaged one-on-one with health coaches to set goals for a healthier lifestyle through reduced alcohol use and were offered up to three health coaching sessions over the phone.
Participants completed weekly check-ins via the Tula App and quarterly follow-up assessments at 3, 6, 9, and 12 months. Primary outcomes were the number of heavy drinking days in the last 7 days (defined as number of days consuming 5+ standard drinks for men under 65, or 4+ standard drinks for women and men over 65 on any day based on the 7-day timeline follow-back survey) and quality of life (measured using the Patient-Reported Outcome Measurement Information System). To calculate the percentage of heavy drinking days for each participant, the researchers divided the number of weekly heavy drinking days by 7. The researchers used longitudinal mixed effects models to analyze changes in outcomes between study arms at 3-, 6-, 9-, and 12-month follow-ups, employing an intent-to-treat approach such that individuals were analyzed in the group to which they were assigned irrespective of how much or little treatment was received. They hypothesized that participants in both the clinically integrated group and peer-supported group would experience greater reductions in heavy drinking days and improvements in quality of life compared to the self-managed group, with the clinically integrated digital intervention expected to be more effective than the peer-supported digital intervention.
Participants were 43 years old, on average. Two-thirds identified as female. Most (91%) identified as White, while 5% identified as Black and smaller percentages identified as Latino and Asian. The sample had high levels of education, overall, with 70% having earned a Bachelor’s degree or higher. Their average AUDIT score was 12 (SD = 6), consistent with hazardous/harmful drinking, but not severe alcohol use disorder. Indeed, two-thirds met criteria for mild alcohol use disorder (2-3 symptoms) and then others for moderate (4-5 symptoms).
WHAT DID THIS STUDY FIND?
Participants were willing to engage with the app, though usage declined over time
Throughout the 12-month study period, participants completed 70% (28 out of 40) of the weekly check-in surveys via the Tula app. Those in the peer-supported group and clinically integrated groups also had access to the Tula group discussion boards. Among participants in the peer-supported group, most (96%) read discussion forum messages, and slightly more than half (52%) posted at least one message. In the clinically integrated group, 97% of participants read posts to the discussion board, but only about 1 in 4 (28%) contributed at least one message. Additionally, 67% of participants in the clinically integrated group used the available health coaching phone calls, with an average number of 1.7 calls per participant. While more than 9 out of 10 participants in each of the three study arms used the Tula app in the first week, weekly usage steadily declined across all groups over time. By the end of the study, between 60-70% of those in the self-managed and peer-supported groups were using the app on a weekly basis, while weekly usage in the clinically integrated group dipped below 50%.
Heavy drinking decreased across all groups from baseline to 12 months, with no significant differences between groups
Across all three groups, the percentage of heavy drinking days decreased from 38.4% at baseline to 22.5% at 12-month follow up. There was no difference on the reduction in heavy drinking days across the groups during the 12-month study window, overall; however, there were additional significant reductions in heavy drinking days just between months 3 and 9 for the clinically integrated group that were not observed in the peer-supported and self-managed groups. That said, there were high study non-completion rates in the clinically integrated group compared to the other two intervention groups, which may distort or potentially inflate the benefits here assuming those who did not complete the study and dropped out had worse outcomes.
Quality of life remained largely unchanged, with minimal differences between study conditions
Physical health scores were stable from baseline to 12 months across all groups. Mental health scores improved slightly from baseline to 12 months for all three groups, with the clinically integrated (5.9%) and peer-supported groups (4.8%) experiencing slightly greater increases than the self-managed group (2.6%). Participants in the clinically integrated group reported significantly higher mental health scores compared to the self-managed group, particularly at 9 and 12 months. However, extremely high non-completion in the clinically integrated group may have accounted for this (only 55% of this group completed the assessment at the 12-month follow-up point)– such that those dropping out had worse mental health, potentially inflating the clinically integrated group’s positive effect on mental health.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study compared the effectiveness of a digital alcohol intervention app with varying levels of human support (no support, peer support, or clinical integration with health coaching) for reducing heavy drinking in individuals with mild-to-moderate alcohol use disorder. Somewhat surprisingly, despite different levels and types of available human support across the groups to which study participants were assigned there was no meaningful differences detected across the different groups in any of the outcomes of focus. Across all groups, the percentage of heavy drinking days decreased from an average of 38.4% at baseline to 22.5% at 12 months, representing a 41% relative reduction from baseline. While the clinical and societal significance of this reduction warrants further exploration, reducing heavy drinking lowers risks of alcohol-related injury and mortality. Achieving similar heavy drinking reductions at scale could result in significant public health impacts.
This study adds to existing evidence supporting digital alcohol interventions for effectively reducing alcohol consumption. All three intervention models – self-managed, peer-supported, and clinically integrated – reduced heavy drinking days. The digital alcohol app used in this study, Tula, was adapted from an existing empirically-supported app (A-CHESS) and incorporated features such as drink tracking and goal setting that are commonly used in empirically supported digital alcohol interventions. Such features may serve as foundational elements to build off of in future digital intervention development efforts. Results from this study also suggest that self-managed use of the digital alcohol app was just as helpful alone for reducing heavy drinking in individuals with mild-to-moderate alcohol use disorder as the versions with added human support from a peer-support specialist or health coach. This aligns with prior studies that have shown that adding human support to digital alcohol interventions did not result in improved outcomes, on average. However, meta-analyses have produced mixed results on the topic. While a meta-analysis of digital alcohol interventions indicated that human-supported interventions resulted in greater reductions in heavy drinking than fully automated interventions, others have found no additional benefit. One possible explanation for the lack of added benefit in this study’s peer-supported group is that participants were not each individually assigned a peer-support specialist but rather simply had the option to reach out via private message or discussion board. Future studies could investigate whether having more direct interaction – such as outreach phone calls or scheduled virtual meetings with a peer-support specialist – results in improved outcomes beyond those of the self-managed group.
Notably, there were higher attrition rates in the clinically integrated group, which required participants to engage in 1-on-1 messaging with a health coach to discuss goals for reducing alcohol use and provided access to up to 3 phone calls with the health coach. Although about 2 out of 3 participants opted for at least one phone call with a health coach, those who dropped out may have preferred a more autonomous approach, finding the direct interaction with a health coach too intensive for their needs.
Findings underscore the importance of better understanding which individuals in particular may prefer or benefit from human support added to digital alcohol interventions and to what extent and which may prefer a more autonomous, self-directed approach. Giving individuals choices as to the type of digital alcohol intervention they feel they need and prefer may be helpful.
Findings also indicate that the self-managed intervention produced similar effects on quality of life, including physical and mental health, as the peer-supported and clinically integrated versions. Although participants in the clinically integrated group experienced significantly greater improvements in mental health scores compared to the self-managed group, high attrition in the clinically integrated group (only 55% completed the 12 month follow up) complicates interpretation. Sensitivity analysis suggested the improvements in mental health observed in the clinically integrated group may be because those who dropped out of the study had worse baseline mental health. Thus, the better mental health in the clinically integrated group in the follow up assessments may be explained by those that were successfully followed up in the study having generally better mental health to begin with.
High attrition rates in the clinically integrated group limit the interpretation of findings for that group. Although the researchers used an intent-to-treat approach, participants who dropped out of the study may differ systematically from those who remained (e.g., may be less motivated), potentially affecting the results.
The study’s population consisted of primarily white, middle-aged, highly educated individuals, and may limit generalizability to broader populations of individuals engaged in patterns of drinking associated with mild-to-moderate alcohol use disorder.
BOTTOM LINE
This study compared the effectiveness of a digital alcohol intervention app with and without varying levels of human support (peer support specialists or health coaches) for reducing heavy drinking and improving quality of life in individuals with mild-to-moderate alcohol use disorder. Adding human support to the digital format did not improve outcomes. Results showed that all groups reduced their percentage of heavy drinking days from baseline (38.4%) to 12 months (22.5%) and experienced slight improvements in mental health. These findings indicate that a self-managed digital alcohol app could be a cost-effective option for health systems seeking to support individuals aiming to reduce or quit drinking. However, further research is needed to determine whether certain individuals may prefer – and benefit more from – digital alcohol interventions with and without varying levels of human support.
For individuals and families seeking recovery: For those with mild-to-moderate alcohol use disorder and a goal to reduce alcohol consumption, digital alcohol reduction interventions can be an accessible and effective tool to support self-managed efforts to reduce heavy drinking, especially for those who lack access to or prefer not to engage in more formal or in-person options. This study found that adding human support (from a peer-support specialist or health coach) did not improve effectiveness for reducing heavy drinking. However, some individuals, particularly those with more severe alcohol use disorder (not included in this study), may benefit from pairing digital alcohol interventions with formal treatment services or additional human support.
For treatment professionals and treatment systems: Digital alcohol interventions, including the app tested in this study, have been shown to be helpful in reducing alcohol use and problems among individuals with mild-to-moderate alcohol use disorder. Connecting patients who screen positive for mild-to-moderate alcohol use disorder in healthcare settings – and who express a desire to reduce their drinking through self-directed efforts – with digital alcohol interventions may be a beneficial approach. That said, real world engagement without the structure and support of being in a clinical study may result in different results and potentially more disengagement over time than what was observed here. Treatment providers could expand offerings to include a range of digital and hybrid options to assist individuals in their efforts to quit or cut down on their alcohol use, providing flexible support that can accommodate the diverse preferences and needs of broader population of at-risk drinkers.
For scientists: While digital alcohol interventions show promise for reducing alcohol use among heavy drinkers, there is limited understanding on how best to implement them in real-world settings without the structure of a clinical program to help with engagement over time. Evidence on the benefits of adding human support to self-directed digital alcohol interventions is mixed, with this study finding that adding human support did not improve outcomes. Better understanding how to enhance the effectiveness of digital alcohol interventions with human support – and identifying who is most likely to prefer or benefit from such support compared to a self-guided approach – could improve engagement and outcomes. Future research could explore whether specific groups (based on demographics, drinking goals, or personality) benefit more from human-supported digital alcohol interventions, and which may prefer or benefit more from an autonomous, self-directed approach. These studies could also investigate whether having more direct interaction – such as outreach phone calls or scheduled virtual meetings with a peer-support specialist – results in improved outcomes beyond those of the self-managed group.
For policy makers: Implementing scalable, cost-effective digital alcohol interventions like Tula can help reduce barriers to treatment and allow health systems to expand access without straining resources to a variety of supports for individuals with alcohol use disorder who wish to reduce or quit their drinking. This study showed that the more resource-friendly, self-managed access to the app produced similar outcomes to the app with additional available support from a recovery or health coach. Increased funding is needed, however, to identify how best to implement digital alcohol interventions – with and without varying levels of human support – to maximize their impact across the broad population of individuals engaged in heavy drinking. Funding this research would help to ensure that resources are allocated efficiently to most effectively support the broadest spectrum of people who use alcohol in harmful or hazardous ways.
Alcohol misuse, including binge and heavy drinking, poses significant public health risks. More than 1 in 5 Americans – 61.2 million people – report binge drinking, defined as drinking 5 or more drinks on an occasion for men and 4 or more for women in the past month. For those who binge drink but do not meet criteria for an alcohol use disorder, this pattern of drinking over time can increase the risk for developing alcohol use disorder later in life, while representing a significant risk factor for accidents and injuries as well as disease and disability, irrespective of whether it is part of a pattern meeting clinical thresholds for alcohol use disorder. At the same time, early intervention strategies designed to reduce binge and heavy drinking (irrespective of clinical thresholds) can also help prevent the escalation from milder to more severe forms of alcohol use disorder, thereby reducing long-term harms.
Digital technology offers a promising cost-effective solution that might help extend the reach of evidence-based treatments for those who wish to quit or cut down on their alcohol use. Many digital interventions – e.g., delivered by smartphone application – while shown to be helpful ways of enhancing or maintaining alcohol abstinence, have targeted individuals with more severe alcohol use disorder receiving (or who had received) services in specialty substance use disorder treatment. In non-clinical samples, digital alcohol interventions have consistently shown modest but robust effects on reducing alcohol use up to 6 months, which given their low-cost and potential reach could make a significant public health impact. However, the real-world implementation of digital alcohol interventions is limited, and questions remain about whether adding human support – such as guidance from peer support specialists (e.g., recovery coaches) or health coaches – can improve them. Given the added costs of providing human support, a question remains as to whether it is worth the investment. This study aimed to fill this gap by testing the effectiveness of a digital alcohol app intervention for reducing heavy drinking and enhancing quality of life among individuals with risky alcohol use and/or mild-to-moderate alcohol use disorder – the primary goal was to test whether outcomes were different with and without human support (either peer support specialists or health coaches).
HOW WAS THIS STUDY CONDUCTED?
This study used a 12-month randomized controlled trial to evaluate both the effects of the digital, remotely-delivered intervention on alcohol use outcomes and quality of life. There was a 3-month intervention period with incentives and a 9-month follow-up period including 3-, 6-, and 12-month follow-up assessments.
Between March 2020 and September 2023, participants were recruited across Wisconsin and the Upper Midwest through clinical sites, community organizations, and public media. Interested individuals remotely completed a web-based screening survey and eligibility criteria included: age 21 or older, a desire to reduce drinking, and a current drinking pattern associated with either risky/hazardous alcohol use and/or mild-to-moderate alcohol use disorder. This was operationally defined as meeting any of the following 3 criteria: 1) scoring at least an 8 or higher on the Alcohol Use Disorders Identification Test; 2) meeting at least 2 out of 11 DSM-5 symptoms; or 3) reporting moderate- to high-risk drinking patterns (e.g., 4+ drinks on a single occasion and >7 drinks per week for women; 5+ drinks on any single day and >14 drinks per week for men). Those with more severe drinking patterns (6 or more DSM-5 symptoms) were excluded from the study. To enroll in the study, eligible participants had to download the digital alcohol intervention app (called “Tula”), complete the baseline survey, and schedule a phone call with a study team member within 72 hours of completing the screener. Enrolled participants were then randomized to one of three groups, each with access to the basic content in the Tula app but varying levels of human support provided remotely, online: 1) self-managed group (no human support; n = 185), 2) peer-supported group (moderate human support; n = 186), or 3) clinically integrated group (high human support; n = 187). Participants were mostly white (91%), female (66%), and highly educated (72% had at least a bachelor’s degree) with an average age of about 43 years.
The digital alcohol intervention tested in this study, Tula, was adapted from the Addiction-Comprehensive Health Enhancement Support System (A-CHESS), a digital alcohol app previously shown to be helpful in reducing heavy drinking. Tula stripped components of A-CHESS that were focused on abstinence as a part of recovery from severe alcohol use disorder and instead adapted the focus to reducing alcohol consumption for individuals with mild-to-moderate alcohol use disorder. Intervention components (e.g., motivational content, progress tracking, relaxation exercises) included in the digital app are detailed in the figure below.
Participants in the self-managed group independently used the app with no external support, similar to a commercially available app. Those in the peer-supported group, in addition to the basic content features of the Tula app, also had access to social support from others in the study via an online discussion forum built into the app and could engage (either through the discussion forum or private messaging) with certified peer specialists (substance use disorder recovery coaches with lived experience with substance use disorder). Recovery coaches were not assigned to individual participants. Those in the clinically integrated group, in addition to the Tula app and discussion forum with other participants assigned to their study arm, also private messaged one-on-one with health coaches to set goals for a healthier lifestyle through reduced alcohol use and were offered up to three health coaching sessions over the phone.
Participants completed weekly check-ins via the Tula App and quarterly follow-up assessments at 3, 6, 9, and 12 months. Primary outcomes were the number of heavy drinking days in the last 7 days (defined as number of days consuming 5+ standard drinks for men under 65, or 4+ standard drinks for women and men over 65 on any day based on the 7-day timeline follow-back survey) and quality of life (measured using the Patient-Reported Outcome Measurement Information System). To calculate the percentage of heavy drinking days for each participant, the researchers divided the number of weekly heavy drinking days by 7. The researchers used longitudinal mixed effects models to analyze changes in outcomes between study arms at 3-, 6-, 9-, and 12-month follow-ups, employing an intent-to-treat approach such that individuals were analyzed in the group to which they were assigned irrespective of how much or little treatment was received. They hypothesized that participants in both the clinically integrated group and peer-supported group would experience greater reductions in heavy drinking days and improvements in quality of life compared to the self-managed group, with the clinically integrated digital intervention expected to be more effective than the peer-supported digital intervention.
Participants were 43 years old, on average. Two-thirds identified as female. Most (91%) identified as White, while 5% identified as Black and smaller percentages identified as Latino and Asian. The sample had high levels of education, overall, with 70% having earned a Bachelor’s degree or higher. Their average AUDIT score was 12 (SD = 6), consistent with hazardous/harmful drinking, but not severe alcohol use disorder. Indeed, two-thirds met criteria for mild alcohol use disorder (2-3 symptoms) and then others for moderate (4-5 symptoms).
WHAT DID THIS STUDY FIND?
Participants were willing to engage with the app, though usage declined over time
Throughout the 12-month study period, participants completed 70% (28 out of 40) of the weekly check-in surveys via the Tula app. Those in the peer-supported group and clinically integrated groups also had access to the Tula group discussion boards. Among participants in the peer-supported group, most (96%) read discussion forum messages, and slightly more than half (52%) posted at least one message. In the clinically integrated group, 97% of participants read posts to the discussion board, but only about 1 in 4 (28%) contributed at least one message. Additionally, 67% of participants in the clinically integrated group used the available health coaching phone calls, with an average number of 1.7 calls per participant. While more than 9 out of 10 participants in each of the three study arms used the Tula app in the first week, weekly usage steadily declined across all groups over time. By the end of the study, between 60-70% of those in the self-managed and peer-supported groups were using the app on a weekly basis, while weekly usage in the clinically integrated group dipped below 50%.
Heavy drinking decreased across all groups from baseline to 12 months, with no significant differences between groups
Across all three groups, the percentage of heavy drinking days decreased from 38.4% at baseline to 22.5% at 12-month follow up. There was no difference on the reduction in heavy drinking days across the groups during the 12-month study window, overall; however, there were additional significant reductions in heavy drinking days just between months 3 and 9 for the clinically integrated group that were not observed in the peer-supported and self-managed groups. That said, there were high study non-completion rates in the clinically integrated group compared to the other two intervention groups, which may distort or potentially inflate the benefits here assuming those who did not complete the study and dropped out had worse outcomes.
Quality of life remained largely unchanged, with minimal differences between study conditions
Physical health scores were stable from baseline to 12 months across all groups. Mental health scores improved slightly from baseline to 12 months for all three groups, with the clinically integrated (5.9%) and peer-supported groups (4.8%) experiencing slightly greater increases than the self-managed group (2.6%). Participants in the clinically integrated group reported significantly higher mental health scores compared to the self-managed group, particularly at 9 and 12 months. However, extremely high non-completion in the clinically integrated group may have accounted for this (only 55% of this group completed the assessment at the 12-month follow-up point)– such that those dropping out had worse mental health, potentially inflating the clinically integrated group’s positive effect on mental health.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study compared the effectiveness of a digital alcohol intervention app with varying levels of human support (no support, peer support, or clinical integration with health coaching) for reducing heavy drinking in individuals with mild-to-moderate alcohol use disorder. Somewhat surprisingly, despite different levels and types of available human support across the groups to which study participants were assigned there was no meaningful differences detected across the different groups in any of the outcomes of focus. Across all groups, the percentage of heavy drinking days decreased from an average of 38.4% at baseline to 22.5% at 12 months, representing a 41% relative reduction from baseline. While the clinical and societal significance of this reduction warrants further exploration, reducing heavy drinking lowers risks of alcohol-related injury and mortality. Achieving similar heavy drinking reductions at scale could result in significant public health impacts.
This study adds to existing evidence supporting digital alcohol interventions for effectively reducing alcohol consumption. All three intervention models – self-managed, peer-supported, and clinically integrated – reduced heavy drinking days. The digital alcohol app used in this study, Tula, was adapted from an existing empirically-supported app (A-CHESS) and incorporated features such as drink tracking and goal setting that are commonly used in empirically supported digital alcohol interventions. Such features may serve as foundational elements to build off of in future digital intervention development efforts. Results from this study also suggest that self-managed use of the digital alcohol app was just as helpful alone for reducing heavy drinking in individuals with mild-to-moderate alcohol use disorder as the versions with added human support from a peer-support specialist or health coach. This aligns with prior studies that have shown that adding human support to digital alcohol interventions did not result in improved outcomes, on average. However, meta-analyses have produced mixed results on the topic. While a meta-analysis of digital alcohol interventions indicated that human-supported interventions resulted in greater reductions in heavy drinking than fully automated interventions, others have found no additional benefit. One possible explanation for the lack of added benefit in this study’s peer-supported group is that participants were not each individually assigned a peer-support specialist but rather simply had the option to reach out via private message or discussion board. Future studies could investigate whether having more direct interaction – such as outreach phone calls or scheduled virtual meetings with a peer-support specialist – results in improved outcomes beyond those of the self-managed group.
Notably, there were higher attrition rates in the clinically integrated group, which required participants to engage in 1-on-1 messaging with a health coach to discuss goals for reducing alcohol use and provided access to up to 3 phone calls with the health coach. Although about 2 out of 3 participants opted for at least one phone call with a health coach, those who dropped out may have preferred a more autonomous approach, finding the direct interaction with a health coach too intensive for their needs.
Findings underscore the importance of better understanding which individuals in particular may prefer or benefit from human support added to digital alcohol interventions and to what extent and which may prefer a more autonomous, self-directed approach. Giving individuals choices as to the type of digital alcohol intervention they feel they need and prefer may be helpful.
Findings also indicate that the self-managed intervention produced similar effects on quality of life, including physical and mental health, as the peer-supported and clinically integrated versions. Although participants in the clinically integrated group experienced significantly greater improvements in mental health scores compared to the self-managed group, high attrition in the clinically integrated group (only 55% completed the 12 month follow up) complicates interpretation. Sensitivity analysis suggested the improvements in mental health observed in the clinically integrated group may be because those who dropped out of the study had worse baseline mental health. Thus, the better mental health in the clinically integrated group in the follow up assessments may be explained by those that were successfully followed up in the study having generally better mental health to begin with.
High attrition rates in the clinically integrated group limit the interpretation of findings for that group. Although the researchers used an intent-to-treat approach, participants who dropped out of the study may differ systematically from those who remained (e.g., may be less motivated), potentially affecting the results.
The study’s population consisted of primarily white, middle-aged, highly educated individuals, and may limit generalizability to broader populations of individuals engaged in patterns of drinking associated with mild-to-moderate alcohol use disorder.
BOTTOM LINE
This study compared the effectiveness of a digital alcohol intervention app with and without varying levels of human support (peer support specialists or health coaches) for reducing heavy drinking and improving quality of life in individuals with mild-to-moderate alcohol use disorder. Adding human support to the digital format did not improve outcomes. Results showed that all groups reduced their percentage of heavy drinking days from baseline (38.4%) to 12 months (22.5%) and experienced slight improvements in mental health. These findings indicate that a self-managed digital alcohol app could be a cost-effective option for health systems seeking to support individuals aiming to reduce or quit drinking. However, further research is needed to determine whether certain individuals may prefer – and benefit more from – digital alcohol interventions with and without varying levels of human support.
For individuals and families seeking recovery: For those with mild-to-moderate alcohol use disorder and a goal to reduce alcohol consumption, digital alcohol reduction interventions can be an accessible and effective tool to support self-managed efforts to reduce heavy drinking, especially for those who lack access to or prefer not to engage in more formal or in-person options. This study found that adding human support (from a peer-support specialist or health coach) did not improve effectiveness for reducing heavy drinking. However, some individuals, particularly those with more severe alcohol use disorder (not included in this study), may benefit from pairing digital alcohol interventions with formal treatment services or additional human support.
For treatment professionals and treatment systems: Digital alcohol interventions, including the app tested in this study, have been shown to be helpful in reducing alcohol use and problems among individuals with mild-to-moderate alcohol use disorder. Connecting patients who screen positive for mild-to-moderate alcohol use disorder in healthcare settings – and who express a desire to reduce their drinking through self-directed efforts – with digital alcohol interventions may be a beneficial approach. That said, real world engagement without the structure and support of being in a clinical study may result in different results and potentially more disengagement over time than what was observed here. Treatment providers could expand offerings to include a range of digital and hybrid options to assist individuals in their efforts to quit or cut down on their alcohol use, providing flexible support that can accommodate the diverse preferences and needs of broader population of at-risk drinkers.
For scientists: While digital alcohol interventions show promise for reducing alcohol use among heavy drinkers, there is limited understanding on how best to implement them in real-world settings without the structure of a clinical program to help with engagement over time. Evidence on the benefits of adding human support to self-directed digital alcohol interventions is mixed, with this study finding that adding human support did not improve outcomes. Better understanding how to enhance the effectiveness of digital alcohol interventions with human support – and identifying who is most likely to prefer or benefit from such support compared to a self-guided approach – could improve engagement and outcomes. Future research could explore whether specific groups (based on demographics, drinking goals, or personality) benefit more from human-supported digital alcohol interventions, and which may prefer or benefit more from an autonomous, self-directed approach. These studies could also investigate whether having more direct interaction – such as outreach phone calls or scheduled virtual meetings with a peer-support specialist – results in improved outcomes beyond those of the self-managed group.
For policy makers: Implementing scalable, cost-effective digital alcohol interventions like Tula can help reduce barriers to treatment and allow health systems to expand access without straining resources to a variety of supports for individuals with alcohol use disorder who wish to reduce or quit their drinking. This study showed that the more resource-friendly, self-managed access to the app produced similar outcomes to the app with additional available support from a recovery or health coach. Increased funding is needed, however, to identify how best to implement digital alcohol interventions – with and without varying levels of human support – to maximize their impact across the broad population of individuals engaged in heavy drinking. Funding this research would help to ensure that resources are allocated efficiently to most effectively support the broadest spectrum of people who use alcohol in harmful or hazardous ways.