If you have a cannabis use disorder, how much do you have to cut back on using it to feel and do better? Answer: A lot
For those interested in changing their cannabis use, abstinence may be the chosen course while others may prefer a goal of reduced use. In both cases, however, people are interested in doing better and feeling better. How much of a reduction in cannabis use is needed to see improvement in these functional outcomes is unknown. This study combined data from 7 clinical trials to explore what level of cannabis use reduction is associated with improvements in cannabis-related problems and functional outcomes.
As with any substance use disorder, there are many different pathways to recovery from cannabis use disorders. Broadly, these may include clinical, non-clinical, and self-management (i.e., natural recovery) pathways as well as abstinence and reduced use in terms of substance use goals. In addition to the varying pathways to recovery, there are a range of considerations for what “recovery” is (i.e., reduced use or abstinence). While improvements in functioning may be linked with reduced use, such as found with opioid and alcohol use, the relationship between moderated cannabis use and functional improvements is less clear. How much of a reduction in cannabis use is needed to see sustained reductions in cannabis-related problems and improvements in functioning is unknown. The researchers in this study pooled data from 7 cannabis use disorder clinical trials to investigate if they could find recommended cutoffs for reductions in cannabis use amount and frequency that are needed to see meaningful improvements.
HOW WAS THIS STUDY CONDUCTED?
The authors conducted a secondary data analysis of 7 clinical datasets from cannabis use disorder treatment studies, 2 with samples 21 years old and younger and 5 with samples 18+ years old. Although each study is a little different, they all are randomized control trials. The researchers of this study were also researchers in each of the 7 individual studies. Each study included individuals with cannabis use disorder. Cannabis use was measured in frequency and amount. Frequency of use was measured in days of use in the past 30 days. Amount of cannabis use was measured in grams per day and sessions/episodes (cannabis use separated by at least 2 hours of no use) per day. All cannabis use measures were self-reported. Five functional measures were included for their clinical relevance and use across studies: cannabis-related problems, clinical impression of severity, clinical impression of improvement, health-related quality of life, and sleep quality.
The primary outcome, cannabis-related problems, was measured with the Marijuana Problems Scale, which includes 19 items scored on a 3-point scale indicating the severity of different cannabis-related problems such as motivation, relationships, health, employment, productivity, self-esteem, finances, memory, and legal issues. It was used in all 7 studies. Clinical impressions of severity and improvement were measured by the Clinical Global Impressions severity and improvement scales. Each scale is clinician-administered and captures severity and improvement in symptoms on a 7-point scale. They were in 4 studies. Health-related quality of life was measured by the scale of the same name, the Health-Related Quality of Life Scale, which asks respondents to rate their general health on a 5-point scale and then asks how many days in the last 30 they experienced poor physical and mental health as well as the number of interrupted days due to poor mental or physical health. It was used in only 2 studies. Sleep quality was measured with the Pittsburgh Sleep Quality Index, which features 9 items capturing the quality of sleep in the past 30 days (for baseline assessment) or past 7 days (for follow-ups). It was in three of the original studies.
The principal objective of this study was to identify the needed reduction in cannabis use to see improvements in functional outcomes. Thus, the level of improvement in the outcomes needed to be considered meaningful was determined before the study took place based on existing benchmarks. Cannabis-related problem improvements were originally defined as total remission of problems. However, that was very rare. So, improvements in cannabis-related problems were then defined as either no items rated as severe (2 on the 3-point scale) or a 50% reduction in total score from baseline. Decrease in clinician-rated severity was considered clinically significant if participants improved at least one level from the baseline severity rating. Clinician-rated improvement was deemed achieved if they were rated very much or much improved (score of 1 or 2 out of 7). Improvement in health-related quality of life was defined as a one-unit positive change or a 50% reduction in interrupted days from poor mental or physical health. Sleep quality was deemed improved if there was a 50% reduction or greater in the total score.
The aggregated sample size was 920 for analyses. Individual sample sizes ranged from 72 to 302. This included adult (age 18 and older; five studies) and youth (ages 13-21; two studies) treatment trials, though average age was a maximum of 30 in adult trials suggesting samples tended to be younger than for alcohol and opioid use disorder trials. Treatments in constituent studies included contingency management, the medication N-acetyl cysteine (NAC) available as an over-the-counter supplement, buspirone, vilazodone, and varenicline. The percentage of females was 23–48%, and 58–78% identified as White. The average years of regular cannabis use across studies ranged from 3 to 15 years, and the percentage of cannabis use days in the last 30 days was 77–93%. Among the full sample, participants reported using cannabis on 84% of the 30 days prior and had used cannabis for an average of 9.7 years.
WHAT DID THIS STUDY FIND?
Decreasing both cannabis use amount and frequency associated with benchmark 50% reduction in cannabis-related problem scores
For every unit decrease in amount of cannabis used, there was a 19% increase in the odds of eliminating severe cannabis-related problems. For each 1 day of less frequent cannabis use, there was a 24% increase in the odds of achieving a 50% reduction in cannabis-related problem scores.
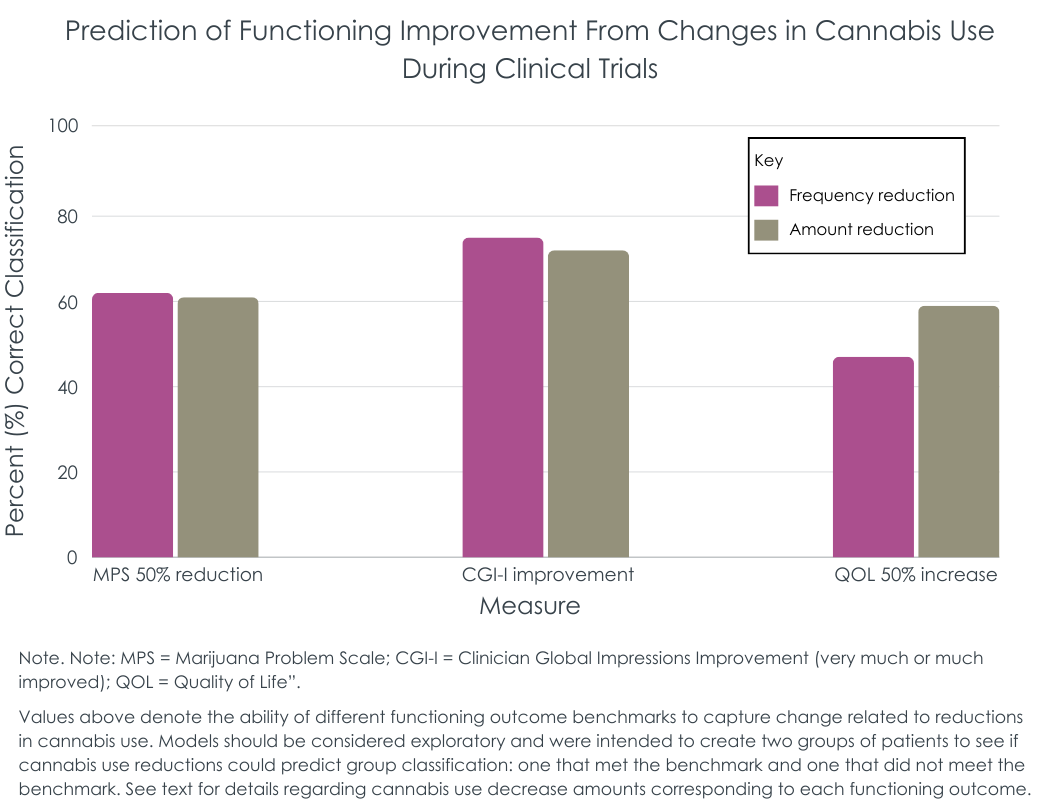
There was not a clear cut point in the frequency or amount of cannabis use reductions to estimate the elimination of severe cannabis-related problems. However, reducing the amount of cannabis used by 78% and the days of use by 51% were reliably better than chance at predicting that a participant would reach the benchmark of a 50% problem reduction. See figure below for benchmark functioning improvement categories and the extent to which reduced frequency and reduced amount of cannabis use was able to predict reaching those benchmarks.
Reducing cannabis use linked with higher odds of clinician-rated improvement
Reducing the amount of cannabis used by at least 50% corresponded with a 188% increase in odds of a clinician noting improvements (i.e., “very much” or “much improved” on a 1 to 7 scale capturing change over time). Similarly, reducing the number of cannabis use days by at least 50% corresponded with a 153% increase in odds of a clinician recording improvements.
In order to see a one-point improvement in clinician-rated illness severity, a participant needed to reduce their cannabis use amount by 74%. In contrast, 47% fewer cannabis use days was needed for clinician-rated improvement. As shown in the figure above, clinician-rated improvement was the most useful benchmark of functional improvement related to reduced cannabis use.
Health-related quality of life and sleep quality were minimally impacted by cannabis use reductions
Neither health-related quality of life nor interrupted days due to poor health were markers of reduced cannabis use amount or frequency. Of note, while sleep quality was related to decreased cannabis use, with a 69% increase in odds of improved sleep quality for a one unit decrease in amount used and a 63% increase in odds for each day less of cannabis use. However, there was not a clear cut point of cannabis use to predict reaching the 50% improved benchmark for sleep quality, in part because, a small sub-set of participants reached this benchmark across the 7 trials.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Many types of treatments, recovery support services, and harm reduction strategies have been shown, on average, to improve functioning and well-being in addition to reductions in substance use and related risk factors, especially for alcohol, opioid, and stimulant use disorders. However, much less has been done surrounding shifts in well-being beyond substance use for cannabis use disorder. The current landscape in the US for cannabis, including increasing legalization and commercialization, make cannabis important to study. Like other substances, individuals who develop cannabis-related problems may choose to resolve their problems in many ways (i.e., recovery pathways). These may include abstaining or reducing use. The authors in this study used an exploratory approach to identify how much a person with cannabis use disorder would need to reduce their use to meet previously-established benchmarks for functional improvements, with the answer being: a lot.
The researchers found that reductions in cannabis use amount and frequency were connected to functional improvements in cannabis-related problems, clinician-related improvements, and sleep. However, cutoffs were only better than chance at predicting a 50% reduction in cannabis-related problem scores and clinician-rated improvements. Cannabis use amount needed to decrease by ~75%, on average, to see the desired functional improvements. Cannabis use days needed to be reduced by ~50% on average to see those same improvements. These findings are exploratory and not intended as definitive cutoffs – more research is needed. However, individuals considering reducing their cannabis use may find these benchmarks helpful as general targets if they wish to improve functioning while still using cannabis to some degree. For instance, a person using cannabis 6 days a week might experience meaningful improvements by reducing their use to 3 days a week and others might improve their functioning and well-being by substantial reductions in the amount consumed.
Cannabis consumption methods vary widely, including pipes, bongs, blunts, dabbing, vaporizers, vape pens, edibles, and liquids, and the quantity used can differ significantly across these routes of administration. Thus, the ideal reduction in cannabis amount likely depends on an individual’s chosen method and the % THC (potency) in the cannabis they are using. One study found that a single blunt typically contains about one gram of cannabis. So, someone smoking one blunt per session could potentially see functional improvements by reducing their consumption to a quarter of a blunt per session. The research conducted here was exploratory, and future work needs to expand on how purposeful cannabis use reductions based on these guidelines are related to functional improvements.
The 7 trials included in this research study were not designed for the pooling procedure used here. The inclusion and exclusion criteria as well as the specific measures collected differed across studies. This limits the ability of these findings to generalize to the population of individuals with cannabis use disorder.
Although the total sample size was fairly large (n=920), the sample sizes used in each analysis was much smaller. For example, the sample size for the primary outcome (marijuana problem scale score) was only 208. This reduces the statistical power to find significant results, specifically with small effect sizes.
The analyses did not account for multiple comparisons, which increases the probability of finding statistically significant results purely by chance.
The benchmarks for what was deemed a functional improvement was somewhat subjective — slight changes in these cutoffs may have produced different results. Though these are commonly used benchmarks of functional improvement used in other studies.
Although both frequency and amount of cannabis were included, the potency of cannabis was not considered, which may be a key covariate when considering functional improvements.
BOTTOM LINE
Supporting the common subjective experience of individuals who use alcohol and/or other drugs regularly or intensively – that cutting back improves functioning – this study found the same thing – individuals with cannabis use disorder who reduce their cannabis use are likely to improve their health and functioning. Although this may seem obvious, there are not clear cutoffs for the degree to which one needs to reduce their use to experience improvements in functioning. The researchers in this study combined participants and findings from 7 different clinical trials to explore possible cutoffs in the amount and frequency of cannabis use needed. They found that individuals with cannabis use disorder needed to reduce the amount of cannabis used by ~75% and the frequency by ~50% to see meaningful and observable reductions in cannabis-related problems and clinician-rated improvements. A question remains of course is for how long someone would want, or be able, to remain at these lower levels of use. Future research is needed to confirm whether these cutoffs may inform clinical recommendations, and recovery supports designed to help individuals successfully sustain long-term reductions in their use rather than quit altogether.
For individuals and families seeking recovery: The researchers in this study found that reducing the amount of cannabis by ~75% and the frequency by ~50% related to meaningful functional improvements. If you or a loved one are looking to reduce cannabis use, these cutoffs may be a guide to maintaining some use but lowering the functional impact. However, seeking professional guidance from a clinician is recommended to help navigate changes in use and related obstacles that may arise.
For treatment professionals and treatment systems: Individuals with cannabis use disorder may choose cannabis use reduction as a goal, while unsure by how much they need to reduce their use to expect improvements. The findings from this study suggest that reducing the amount of cannabis used by about 75% and frequency by 50% would likely lead to meaningful functional improvements. However, more research is needed to determine if these cutoffs should be recommended by clinicians and recovery support services. It is unclear how stably someone may be able to sustain such lowered levels of use and still remain subjectively satisfied with the potentially much less rewarding or relieving pharmacologic effects that they once obtained at much higher levels of use.
For scientists: The researchers in this study pooled data from 7 randomized clinical cannabis treatment trials. They found that reducing cannabis use amounts by ~75% and frequency by ~50% was related to meaningful functional improvements. The analyses were exploratory, and future investigation is needed to replicate these findings. Furthermore, what is deemed meaningful functional improvement could be operationalized in additional ways. For example, expanding functional improvements to include employment and social relationships may reveal unique insights.
For policy makers: Reducing cannabis use may be an appealing goal for individuals with cannabis use disorder and related problems. Findings from this study suggest that large reductions in the amount and frequency of cannabis are needed to have meaningful functional improvements. Additional support and funding to explore how the cutoffs found in this study can inform harm reduction and recovery services would help counteract some of the unintended consequences of the changing cannabis landscape.
As with any substance use disorder, there are many different pathways to recovery from cannabis use disorders. Broadly, these may include clinical, non-clinical, and self-management (i.e., natural recovery) pathways as well as abstinence and reduced use in terms of substance use goals. In addition to the varying pathways to recovery, there are a range of considerations for what “recovery” is (i.e., reduced use or abstinence). While improvements in functioning may be linked with reduced use, such as found with opioid and alcohol use, the relationship between moderated cannabis use and functional improvements is less clear. How much of a reduction in cannabis use is needed to see sustained reductions in cannabis-related problems and improvements in functioning is unknown. The researchers in this study pooled data from 7 cannabis use disorder clinical trials to investigate if they could find recommended cutoffs for reductions in cannabis use amount and frequency that are needed to see meaningful improvements.
HOW WAS THIS STUDY CONDUCTED?
The authors conducted a secondary data analysis of 7 clinical datasets from cannabis use disorder treatment studies, 2 with samples 21 years old and younger and 5 with samples 18+ years old. Although each study is a little different, they all are randomized control trials. The researchers of this study were also researchers in each of the 7 individual studies. Each study included individuals with cannabis use disorder. Cannabis use was measured in frequency and amount. Frequency of use was measured in days of use in the past 30 days. Amount of cannabis use was measured in grams per day and sessions/episodes (cannabis use separated by at least 2 hours of no use) per day. All cannabis use measures were self-reported. Five functional measures were included for their clinical relevance and use across studies: cannabis-related problems, clinical impression of severity, clinical impression of improvement, health-related quality of life, and sleep quality.
The primary outcome, cannabis-related problems, was measured with the Marijuana Problems Scale, which includes 19 items scored on a 3-point scale indicating the severity of different cannabis-related problems such as motivation, relationships, health, employment, productivity, self-esteem, finances, memory, and legal issues. It was used in all 7 studies. Clinical impressions of severity and improvement were measured by the Clinical Global Impressions severity and improvement scales. Each scale is clinician-administered and captures severity and improvement in symptoms on a 7-point scale. They were in 4 studies. Health-related quality of life was measured by the scale of the same name, the Health-Related Quality of Life Scale, which asks respondents to rate their general health on a 5-point scale and then asks how many days in the last 30 they experienced poor physical and mental health as well as the number of interrupted days due to poor mental or physical health. It was used in only 2 studies. Sleep quality was measured with the Pittsburgh Sleep Quality Index, which features 9 items capturing the quality of sleep in the past 30 days (for baseline assessment) or past 7 days (for follow-ups). It was in three of the original studies.
The principal objective of this study was to identify the needed reduction in cannabis use to see improvements in functional outcomes. Thus, the level of improvement in the outcomes needed to be considered meaningful was determined before the study took place based on existing benchmarks. Cannabis-related problem improvements were originally defined as total remission of problems. However, that was very rare. So, improvements in cannabis-related problems were then defined as either no items rated as severe (2 on the 3-point scale) or a 50% reduction in total score from baseline. Decrease in clinician-rated severity was considered clinically significant if participants improved at least one level from the baseline severity rating. Clinician-rated improvement was deemed achieved if they were rated very much or much improved (score of 1 or 2 out of 7). Improvement in health-related quality of life was defined as a one-unit positive change or a 50% reduction in interrupted days from poor mental or physical health. Sleep quality was deemed improved if there was a 50% reduction or greater in the total score.
The aggregated sample size was 920 for analyses. Individual sample sizes ranged from 72 to 302. This included adult (age 18 and older; five studies) and youth (ages 13-21; two studies) treatment trials, though average age was a maximum of 30 in adult trials suggesting samples tended to be younger than for alcohol and opioid use disorder trials. Treatments in constituent studies included contingency management, the medication N-acetyl cysteine (NAC) available as an over-the-counter supplement, buspirone, vilazodone, and varenicline. The percentage of females was 23–48%, and 58–78% identified as White. The average years of regular cannabis use across studies ranged from 3 to 15 years, and the percentage of cannabis use days in the last 30 days was 77–93%. Among the full sample, participants reported using cannabis on 84% of the 30 days prior and had used cannabis for an average of 9.7 years.
WHAT DID THIS STUDY FIND?
Decreasing both cannabis use amount and frequency associated with benchmark 50% reduction in cannabis-related problem scores
For every unit decrease in amount of cannabis used, there was a 19% increase in the odds of eliminating severe cannabis-related problems. For each 1 day of less frequent cannabis use, there was a 24% increase in the odds of achieving a 50% reduction in cannabis-related problem scores.
There was not a clear cut point in the frequency or amount of cannabis use reductions to estimate the elimination of severe cannabis-related problems. However, reducing the amount of cannabis used by 78% and the days of use by 51% were reliably better than chance at predicting that a participant would reach the benchmark of a 50% problem reduction. See figure below for benchmark functioning improvement categories and the extent to which reduced frequency and reduced amount of cannabis use was able to predict reaching those benchmarks.
Reducing cannabis use linked with higher odds of clinician-rated improvement
Reducing the amount of cannabis used by at least 50% corresponded with a 188% increase in odds of a clinician noting improvements (i.e., “very much” or “much improved” on a 1 to 7 scale capturing change over time). Similarly, reducing the number of cannabis use days by at least 50% corresponded with a 153% increase in odds of a clinician recording improvements.
In order to see a one-point improvement in clinician-rated illness severity, a participant needed to reduce their cannabis use amount by 74%. In contrast, 47% fewer cannabis use days was needed for clinician-rated improvement. As shown in the figure above, clinician-rated improvement was the most useful benchmark of functional improvement related to reduced cannabis use.
Health-related quality of life and sleep quality were minimally impacted by cannabis use reductions
Neither health-related quality of life nor interrupted days due to poor health were markers of reduced cannabis use amount or frequency. Of note, while sleep quality was related to decreased cannabis use, with a 69% increase in odds of improved sleep quality for a one unit decrease in amount used and a 63% increase in odds for each day less of cannabis use. However, there was not a clear cut point of cannabis use to predict reaching the 50% improved benchmark for sleep quality, in part because, a small sub-set of participants reached this benchmark across the 7 trials.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Many types of treatments, recovery support services, and harm reduction strategies have been shown, on average, to improve functioning and well-being in addition to reductions in substance use and related risk factors, especially for alcohol, opioid, and stimulant use disorders. However, much less has been done surrounding shifts in well-being beyond substance use for cannabis use disorder. The current landscape in the US for cannabis, including increasing legalization and commercialization, make cannabis important to study. Like other substances, individuals who develop cannabis-related problems may choose to resolve their problems in many ways (i.e., recovery pathways). These may include abstaining or reducing use. The authors in this study used an exploratory approach to identify how much a person with cannabis use disorder would need to reduce their use to meet previously-established benchmarks for functional improvements, with the answer being: a lot.
The researchers found that reductions in cannabis use amount and frequency were connected to functional improvements in cannabis-related problems, clinician-related improvements, and sleep. However, cutoffs were only better than chance at predicting a 50% reduction in cannabis-related problem scores and clinician-rated improvements. Cannabis use amount needed to decrease by ~75%, on average, to see the desired functional improvements. Cannabis use days needed to be reduced by ~50% on average to see those same improvements. These findings are exploratory and not intended as definitive cutoffs – more research is needed. However, individuals considering reducing their cannabis use may find these benchmarks helpful as general targets if they wish to improve functioning while still using cannabis to some degree. For instance, a person using cannabis 6 days a week might experience meaningful improvements by reducing their use to 3 days a week and others might improve their functioning and well-being by substantial reductions in the amount consumed.
Cannabis consumption methods vary widely, including pipes, bongs, blunts, dabbing, vaporizers, vape pens, edibles, and liquids, and the quantity used can differ significantly across these routes of administration. Thus, the ideal reduction in cannabis amount likely depends on an individual’s chosen method and the % THC (potency) in the cannabis they are using. One study found that a single blunt typically contains about one gram of cannabis. So, someone smoking one blunt per session could potentially see functional improvements by reducing their consumption to a quarter of a blunt per session. The research conducted here was exploratory, and future work needs to expand on how purposeful cannabis use reductions based on these guidelines are related to functional improvements.
The 7 trials included in this research study were not designed for the pooling procedure used here. The inclusion and exclusion criteria as well as the specific measures collected differed across studies. This limits the ability of these findings to generalize to the population of individuals with cannabis use disorder.
Although the total sample size was fairly large (n=920), the sample sizes used in each analysis was much smaller. For example, the sample size for the primary outcome (marijuana problem scale score) was only 208. This reduces the statistical power to find significant results, specifically with small effect sizes.
The analyses did not account for multiple comparisons, which increases the probability of finding statistically significant results purely by chance.
The benchmarks for what was deemed a functional improvement was somewhat subjective — slight changes in these cutoffs may have produced different results. Though these are commonly used benchmarks of functional improvement used in other studies.
Although both frequency and amount of cannabis were included, the potency of cannabis was not considered, which may be a key covariate when considering functional improvements.
BOTTOM LINE
Supporting the common subjective experience of individuals who use alcohol and/or other drugs regularly or intensively – that cutting back improves functioning – this study found the same thing – individuals with cannabis use disorder who reduce their cannabis use are likely to improve their health and functioning. Although this may seem obvious, there are not clear cutoffs for the degree to which one needs to reduce their use to experience improvements in functioning. The researchers in this study combined participants and findings from 7 different clinical trials to explore possible cutoffs in the amount and frequency of cannabis use needed. They found that individuals with cannabis use disorder needed to reduce the amount of cannabis used by ~75% and the frequency by ~50% to see meaningful and observable reductions in cannabis-related problems and clinician-rated improvements. A question remains of course is for how long someone would want, or be able, to remain at these lower levels of use. Future research is needed to confirm whether these cutoffs may inform clinical recommendations, and recovery supports designed to help individuals successfully sustain long-term reductions in their use rather than quit altogether.
For individuals and families seeking recovery: The researchers in this study found that reducing the amount of cannabis by ~75% and the frequency by ~50% related to meaningful functional improvements. If you or a loved one are looking to reduce cannabis use, these cutoffs may be a guide to maintaining some use but lowering the functional impact. However, seeking professional guidance from a clinician is recommended to help navigate changes in use and related obstacles that may arise.
For treatment professionals and treatment systems: Individuals with cannabis use disorder may choose cannabis use reduction as a goal, while unsure by how much they need to reduce their use to expect improvements. The findings from this study suggest that reducing the amount of cannabis used by about 75% and frequency by 50% would likely lead to meaningful functional improvements. However, more research is needed to determine if these cutoffs should be recommended by clinicians and recovery support services. It is unclear how stably someone may be able to sustain such lowered levels of use and still remain subjectively satisfied with the potentially much less rewarding or relieving pharmacologic effects that they once obtained at much higher levels of use.
For scientists: The researchers in this study pooled data from 7 randomized clinical cannabis treatment trials. They found that reducing cannabis use amounts by ~75% and frequency by ~50% was related to meaningful functional improvements. The analyses were exploratory, and future investigation is needed to replicate these findings. Furthermore, what is deemed meaningful functional improvement could be operationalized in additional ways. For example, expanding functional improvements to include employment and social relationships may reveal unique insights.
For policy makers: Reducing cannabis use may be an appealing goal for individuals with cannabis use disorder and related problems. Findings from this study suggest that large reductions in the amount and frequency of cannabis are needed to have meaningful functional improvements. Additional support and funding to explore how the cutoffs found in this study can inform harm reduction and recovery services would help counteract some of the unintended consequences of the changing cannabis landscape.
As with any substance use disorder, there are many different pathways to recovery from cannabis use disorders. Broadly, these may include clinical, non-clinical, and self-management (i.e., natural recovery) pathways as well as abstinence and reduced use in terms of substance use goals. In addition to the varying pathways to recovery, there are a range of considerations for what “recovery” is (i.e., reduced use or abstinence). While improvements in functioning may be linked with reduced use, such as found with opioid and alcohol use, the relationship between moderated cannabis use and functional improvements is less clear. How much of a reduction in cannabis use is needed to see sustained reductions in cannabis-related problems and improvements in functioning is unknown. The researchers in this study pooled data from 7 cannabis use disorder clinical trials to investigate if they could find recommended cutoffs for reductions in cannabis use amount and frequency that are needed to see meaningful improvements.
HOW WAS THIS STUDY CONDUCTED?
The authors conducted a secondary data analysis of 7 clinical datasets from cannabis use disorder treatment studies, 2 with samples 21 years old and younger and 5 with samples 18+ years old. Although each study is a little different, they all are randomized control trials. The researchers of this study were also researchers in each of the 7 individual studies. Each study included individuals with cannabis use disorder. Cannabis use was measured in frequency and amount. Frequency of use was measured in days of use in the past 30 days. Amount of cannabis use was measured in grams per day and sessions/episodes (cannabis use separated by at least 2 hours of no use) per day. All cannabis use measures were self-reported. Five functional measures were included for their clinical relevance and use across studies: cannabis-related problems, clinical impression of severity, clinical impression of improvement, health-related quality of life, and sleep quality.
The primary outcome, cannabis-related problems, was measured with the Marijuana Problems Scale, which includes 19 items scored on a 3-point scale indicating the severity of different cannabis-related problems such as motivation, relationships, health, employment, productivity, self-esteem, finances, memory, and legal issues. It was used in all 7 studies. Clinical impressions of severity and improvement were measured by the Clinical Global Impressions severity and improvement scales. Each scale is clinician-administered and captures severity and improvement in symptoms on a 7-point scale. They were in 4 studies. Health-related quality of life was measured by the scale of the same name, the Health-Related Quality of Life Scale, which asks respondents to rate their general health on a 5-point scale and then asks how many days in the last 30 they experienced poor physical and mental health as well as the number of interrupted days due to poor mental or physical health. It was used in only 2 studies. Sleep quality was measured with the Pittsburgh Sleep Quality Index, which features 9 items capturing the quality of sleep in the past 30 days (for baseline assessment) or past 7 days (for follow-ups). It was in three of the original studies.
The principal objective of this study was to identify the needed reduction in cannabis use to see improvements in functional outcomes. Thus, the level of improvement in the outcomes needed to be considered meaningful was determined before the study took place based on existing benchmarks. Cannabis-related problem improvements were originally defined as total remission of problems. However, that was very rare. So, improvements in cannabis-related problems were then defined as either no items rated as severe (2 on the 3-point scale) or a 50% reduction in total score from baseline. Decrease in clinician-rated severity was considered clinically significant if participants improved at least one level from the baseline severity rating. Clinician-rated improvement was deemed achieved if they were rated very much or much improved (score of 1 or 2 out of 7). Improvement in health-related quality of life was defined as a one-unit positive change or a 50% reduction in interrupted days from poor mental or physical health. Sleep quality was deemed improved if there was a 50% reduction or greater in the total score.
The aggregated sample size was 920 for analyses. Individual sample sizes ranged from 72 to 302. This included adult (age 18 and older; five studies) and youth (ages 13-21; two studies) treatment trials, though average age was a maximum of 30 in adult trials suggesting samples tended to be younger than for alcohol and opioid use disorder trials. Treatments in constituent studies included contingency management, the medication N-acetyl cysteine (NAC) available as an over-the-counter supplement, buspirone, vilazodone, and varenicline. The percentage of females was 23–48%, and 58–78% identified as White. The average years of regular cannabis use across studies ranged from 3 to 15 years, and the percentage of cannabis use days in the last 30 days was 77–93%. Among the full sample, participants reported using cannabis on 84% of the 30 days prior and had used cannabis for an average of 9.7 years.
WHAT DID THIS STUDY FIND?
Decreasing both cannabis use amount and frequency associated with benchmark 50% reduction in cannabis-related problem scores
For every unit decrease in amount of cannabis used, there was a 19% increase in the odds of eliminating severe cannabis-related problems. For each 1 day of less frequent cannabis use, there was a 24% increase in the odds of achieving a 50% reduction in cannabis-related problem scores.
There was not a clear cut point in the frequency or amount of cannabis use reductions to estimate the elimination of severe cannabis-related problems. However, reducing the amount of cannabis used by 78% and the days of use by 51% were reliably better than chance at predicting that a participant would reach the benchmark of a 50% problem reduction. See figure below for benchmark functioning improvement categories and the extent to which reduced frequency and reduced amount of cannabis use was able to predict reaching those benchmarks.
Reducing cannabis use linked with higher odds of clinician-rated improvement
Reducing the amount of cannabis used by at least 50% corresponded with a 188% increase in odds of a clinician noting improvements (i.e., “very much” or “much improved” on a 1 to 7 scale capturing change over time). Similarly, reducing the number of cannabis use days by at least 50% corresponded with a 153% increase in odds of a clinician recording improvements.
In order to see a one-point improvement in clinician-rated illness severity, a participant needed to reduce their cannabis use amount by 74%. In contrast, 47% fewer cannabis use days was needed for clinician-rated improvement. As shown in the figure above, clinician-rated improvement was the most useful benchmark of functional improvement related to reduced cannabis use.
Health-related quality of life and sleep quality were minimally impacted by cannabis use reductions
Neither health-related quality of life nor interrupted days due to poor health were markers of reduced cannabis use amount or frequency. Of note, while sleep quality was related to decreased cannabis use, with a 69% increase in odds of improved sleep quality for a one unit decrease in amount used and a 63% increase in odds for each day less of cannabis use. However, there was not a clear cut point of cannabis use to predict reaching the 50% improved benchmark for sleep quality, in part because, a small sub-set of participants reached this benchmark across the 7 trials.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Many types of treatments, recovery support services, and harm reduction strategies have been shown, on average, to improve functioning and well-being in addition to reductions in substance use and related risk factors, especially for alcohol, opioid, and stimulant use disorders. However, much less has been done surrounding shifts in well-being beyond substance use for cannabis use disorder. The current landscape in the US for cannabis, including increasing legalization and commercialization, make cannabis important to study. Like other substances, individuals who develop cannabis-related problems may choose to resolve their problems in many ways (i.e., recovery pathways). These may include abstaining or reducing use. The authors in this study used an exploratory approach to identify how much a person with cannabis use disorder would need to reduce their use to meet previously-established benchmarks for functional improvements, with the answer being: a lot.
The researchers found that reductions in cannabis use amount and frequency were connected to functional improvements in cannabis-related problems, clinician-related improvements, and sleep. However, cutoffs were only better than chance at predicting a 50% reduction in cannabis-related problem scores and clinician-rated improvements. Cannabis use amount needed to decrease by ~75%, on average, to see the desired functional improvements. Cannabis use days needed to be reduced by ~50% on average to see those same improvements. These findings are exploratory and not intended as definitive cutoffs – more research is needed. However, individuals considering reducing their cannabis use may find these benchmarks helpful as general targets if they wish to improve functioning while still using cannabis to some degree. For instance, a person using cannabis 6 days a week might experience meaningful improvements by reducing their use to 3 days a week and others might improve their functioning and well-being by substantial reductions in the amount consumed.
Cannabis consumption methods vary widely, including pipes, bongs, blunts, dabbing, vaporizers, vape pens, edibles, and liquids, and the quantity used can differ significantly across these routes of administration. Thus, the ideal reduction in cannabis amount likely depends on an individual’s chosen method and the % THC (potency) in the cannabis they are using. One study found that a single blunt typically contains about one gram of cannabis. So, someone smoking one blunt per session could potentially see functional improvements by reducing their consumption to a quarter of a blunt per session. The research conducted here was exploratory, and future work needs to expand on how purposeful cannabis use reductions based on these guidelines are related to functional improvements.
The 7 trials included in this research study were not designed for the pooling procedure used here. The inclusion and exclusion criteria as well as the specific measures collected differed across studies. This limits the ability of these findings to generalize to the population of individuals with cannabis use disorder.
Although the total sample size was fairly large (n=920), the sample sizes used in each analysis was much smaller. For example, the sample size for the primary outcome (marijuana problem scale score) was only 208. This reduces the statistical power to find significant results, specifically with small effect sizes.
The analyses did not account for multiple comparisons, which increases the probability of finding statistically significant results purely by chance.
The benchmarks for what was deemed a functional improvement was somewhat subjective — slight changes in these cutoffs may have produced different results. Though these are commonly used benchmarks of functional improvement used in other studies.
Although both frequency and amount of cannabis were included, the potency of cannabis was not considered, which may be a key covariate when considering functional improvements.
BOTTOM LINE
Supporting the common subjective experience of individuals who use alcohol and/or other drugs regularly or intensively – that cutting back improves functioning – this study found the same thing – individuals with cannabis use disorder who reduce their cannabis use are likely to improve their health and functioning. Although this may seem obvious, there are not clear cutoffs for the degree to which one needs to reduce their use to experience improvements in functioning. The researchers in this study combined participants and findings from 7 different clinical trials to explore possible cutoffs in the amount and frequency of cannabis use needed. They found that individuals with cannabis use disorder needed to reduce the amount of cannabis used by ~75% and the frequency by ~50% to see meaningful and observable reductions in cannabis-related problems and clinician-rated improvements. A question remains of course is for how long someone would want, or be able, to remain at these lower levels of use. Future research is needed to confirm whether these cutoffs may inform clinical recommendations, and recovery supports designed to help individuals successfully sustain long-term reductions in their use rather than quit altogether.
For individuals and families seeking recovery: The researchers in this study found that reducing the amount of cannabis by ~75% and the frequency by ~50% related to meaningful functional improvements. If you or a loved one are looking to reduce cannabis use, these cutoffs may be a guide to maintaining some use but lowering the functional impact. However, seeking professional guidance from a clinician is recommended to help navigate changes in use and related obstacles that may arise.
For treatment professionals and treatment systems: Individuals with cannabis use disorder may choose cannabis use reduction as a goal, while unsure by how much they need to reduce their use to expect improvements. The findings from this study suggest that reducing the amount of cannabis used by about 75% and frequency by 50% would likely lead to meaningful functional improvements. However, more research is needed to determine if these cutoffs should be recommended by clinicians and recovery support services. It is unclear how stably someone may be able to sustain such lowered levels of use and still remain subjectively satisfied with the potentially much less rewarding or relieving pharmacologic effects that they once obtained at much higher levels of use.
For scientists: The researchers in this study pooled data from 7 randomized clinical cannabis treatment trials. They found that reducing cannabis use amounts by ~75% and frequency by ~50% was related to meaningful functional improvements. The analyses were exploratory, and future investigation is needed to replicate these findings. Furthermore, what is deemed meaningful functional improvement could be operationalized in additional ways. For example, expanding functional improvements to include employment and social relationships may reveal unique insights.
For policy makers: Reducing cannabis use may be an appealing goal for individuals with cannabis use disorder and related problems. Findings from this study suggest that large reductions in the amount and frequency of cannabis are needed to have meaningful functional improvements. Additional support and funding to explore how the cutoffs found in this study can inform harm reduction and recovery services would help counteract some of the unintended consequences of the changing cannabis landscape.