Does recovery coaching after an opioid-related emergency department visit help prevent overdose?
Peer recovery support service providers like recovery coaches are increasingly employed in hospital emergency departments (ED) to support people presenting with substance-related medical and psychiatric problems. This randomized trial compared recovery coaching during and after an ED visit with standard clinical support provided only during the ED stay for individuals experiencing opioid overdose.
Peer recovery support services like recovery coaches are increasingly being employed in hospital emergency departments to support people presenting with medical and psychiatric problems related to substance use disorder. Results from previous studies suggests recovery coaches can be instrumental in helping patients engage with substance use disorder care after emergency department discharge, while reducing emergency department readmissions and supporting better substance use related outcomes.
Some studies have also shown that engagement with recovery coaches is associated with reduced rates of subsequent opioid-involved overdose (see examples here & here), however, other studies have not shown a major benefit. Questions remain about the capacity for recovery coaches working in ED to effect more long-term outcomes like subsequent opioid poisoning events. Also, it is not yet known if outcomes for recovery coaching differ from more typical services provided during an ED visit – for example clinical social workers who help refer patients to outpatient care. To begin to address these questions, this randomized trial tested whether recovery coaching started in the ED with plans for ongoing support post-discharge was better at reducing overdose risk compared with social work services provided only during the ED visit.
HOW WAS THIS STUDY CONDUCTED?
This was a parallel, two-arm, randomized trial with 648 participants presenting to an ED with opioid overdose or other opioid use harms who received intervention by either a certified recovery coach or licensed clinical social worker. The primary study outcome was non-fatal opioid-involved overdose over 18-month follow-up.
Individuals presenting to a Rhode Island, USA hospital emergency department for opioid-involved overdose or opioid use disorder-related complications between November 2018 and May 2021 were invited to participate in this study and were randomized to receive either recovery coaching, or care from a licensed clinical social worker.
Recovery coaches used standard evidence-based interviewing and intervention techniques, shared their own lived experience with substance use and recovery, evaluated patients for readiness to seek treatment, offered referrals to treatment, helped patients navigate barriers to treatment, and provided drug overdose prevention education.
After the ED visit, recovery coaches then reached out to the patient daily for up to 10 days to initiate follow-up support using a community-based follow-up contact plan. In the first few days following discharge, recovery coaches helped patients navigate barriers to treatment, while providing continuing peer support and drug poisoning prevention education. Coaches then provided ongoing support for 90 days to those patients who engaged with coaching. Of note, the study did not report whether and to what degree participants engaged in recovery coaching after ED discharge because authors noted “this was a pragmatic trial”. That said, this does not necessarily mean it cannot be analyzed. In fact, this is a bit puzzling as to why they did not examine this as it would be very helpful to know how much recovery coaching each patient received and how that related to outcomes.
Also notably, the researchers did initially include a “no support” control group of patients who declined any behavioral intervention in their study design, however, recruitment for this arm was stopped after 6 months because eligible patients (those who did not want to meet with either a recovery coach or social worker) were also declining participation in the study.
Clinical social workers were similarly trained in a variety of evidence-based interviewing and intervention techniques, with their practice based on clinical experience rather than personal lived addiction recovery experience. They provided standard behavioral care using evidence-based interviewing and intervention techniques and referrals to treatment. Per standard practice, clinical social workers did not provide services to patients following ED discharge.
The primary study outcome was non-fatal opioid poisoning over 18-month follow-up, measured with statewide data from emergency medical services. Possible non-fatal opioid poisonings that occurred outside of the state of Rhode Island were not measured. Secondary outcomes included median time to first non-fatal overdose among those who overdosed, and death due to opioid overdose in the 18 months following the index ED visit.
The average age of study participants was 37 years, 68% were male, and 69% were White, 10% were mixed, biracial or multi-racial, 6% were Black, and 3% were Native American/Hawaiian. Two-thirds had a prior history of opioid overdose and 45% were being treated for an opioid overdose event when they entered the study. Many participants reported current or past substance use disorder treatment, with 28% currently in treatment, and 49% previously in treatment.
WHAT DID THIS STUDY FIND?
Non-fatal opioid overdose outcomes were similar between groups
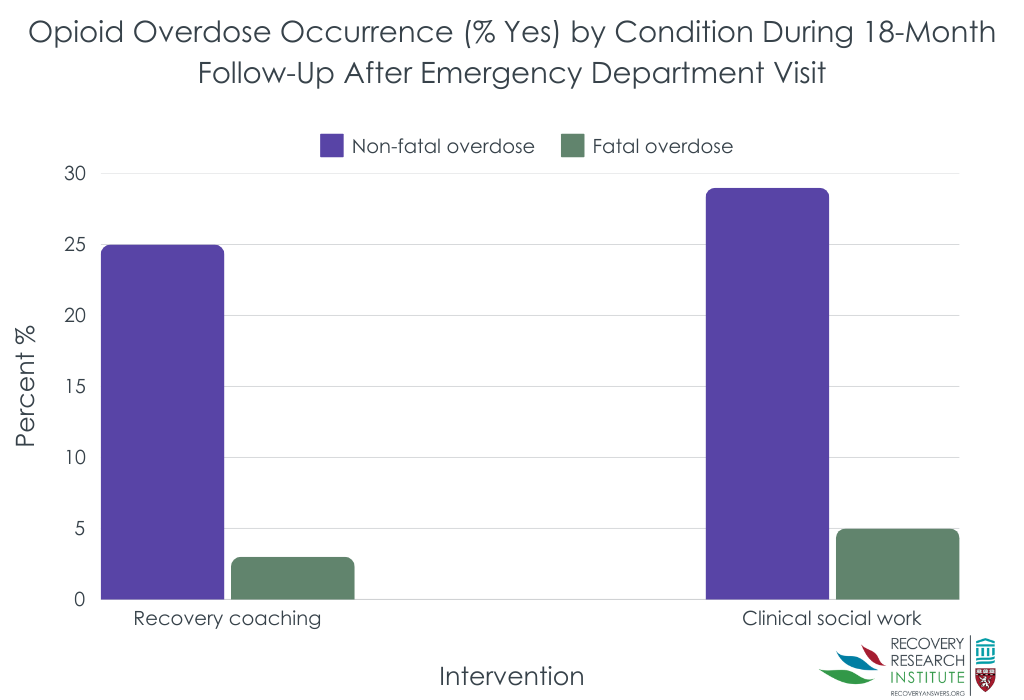
In the recovery coaching group, 25% experienced an opioid-involved non-fatal overdose, statistically similar to the 29% of those in the social work group (see figure below). Across the entire sample including both groups, 27% of participants experienced an overdose during follow-up, with 18% experiencing one, 5% with two, 3% with three, and 2% with 4 or more. Among those with at least 1 non-fatal overdose, median time to overdose was 146 days after ED discharge for the recovery coaching group and 119 days for social work group – again, though, while seemingly quite a large difference there was a lot of variability within these groups, this difference did not reach statistical significance.
Fatal opioid overdose outcomes were also similar, though the median time to overdose slightly favored the social work condition
Regarding fatal overdose, 3% of the recovery coaching group and 5% of the social work group experienced fatal overdose. Among those with fatal overdose, median time to death was 124 days in the recovery coaching group and 202 for the social work group. This latter advantage for the social work group on time to overdose death just missed statistical significance.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study did not find a notable difference in opioid overdose events during the 18 months following an ED visit between patients randomized to recovery coaching with ongoing support during the 90 days after discharge versus clinical social work where services to aid follow-up care were only provided during the ED visit.
It’s possible that both these interventions help mitigate subsequent opioid poisoning, however, the absence of a ‘no support’ control group means this can’t be known from these results. It is also unclear why the recovery coaching group did not have more favorable outcomes both given potential benefits of peer support and the possibility of ongoing coaching for 90 days.
It may be helpful to highlight that whether and to what degree patients actually engaged with the recovery coaches was not reported in the current study so it is unclear whether the coaching truly did not add any benefit or not. Given that coaches outreached to patients up to 10 consecutive days after discharge to make contact, it seems more likely that recovery coaching and clinical social work produced similar effects than patients simply not connecting with their recovery coaches.
Studies to date support the potential of recovery coaches as well as licensed clinicians to help people with substance use disorder reduce or stop substance use across a range of settings. Recovery coaches appear to be especially capable of increasing treatment engagement, overall, which could reduce rates of subsequent opioid poisoning events. The capacity for recovery coaches to support changes in substance use and treatment engagement among patients presenting to EDs is more mixed. Another set of findings from this same overall study showed recovery coaching and social work led to similar treatment engagement as well. This may be due to the very challenging circumstances patients tend to be experiencing that lead to the ED visit. Also, some patients seeking care in EDs are in earlier stages of readiness to change their substance use (e.g., “pre-contemplative”) so they may be less inclined to follow up with treatment recommendations – or in this case with recovery coaches. Notably half of the sample overall had not attended prior treatment. So, future analyses might examine who in particular responded best to which particular treatment and continuing care approach. Approaches that allow for ongoing, but periodic low-intensity contact, like recovery management checkups, may be needed to best help patients with both high severity and much ambivalence about change. Linkages to harm reduction resources may also be good fits clinically with emergency department approaches to engaging such patients.
Regardless, EDs offer critical points of contact between recovery allies like recovery coaches and clinicians and people with active substance use disorder who may be minimally, or not at all engaged in care. Interventions like those investigated in this study are likely to confer benefits other than the outcomes measured.
This study did not include a ‘no support’ control group; thus, it can’t be known from this study if recovery coaching or care from a clinical social worker are superior to no intervention at all.
As mentioned above, whether and to what degree patients randomized to recovery coaching actually engaged with the recovery coaches was not reported in this study. Future work can help clarify whether patients did not benefit from recovery coaching after actually engaging with coaches, or whether it was challenging to get people to engage with the recovery coach at all.
The researchers utilized emergency medical services data from the state of Rhode Island to determine opioid poisoning events over the 18-minth follow-up period. It’s likely some participants experienced opioid poisoning events in states other than Rhode Island.
BOTTOM LINE
In this study, contrary to expectations, no meaningful difference was observed in rate of opioid overdose events following emergency department (ED) care provided by either recovery coaches or clinical social workers. It is unclear whether there were differences in other types of outcomes such as the proportion of patients achieving remission, employment, legal system involvement, psychosocial functioning, or other recovery outcomes as these were not reported.
For individuals and families seeking recovery: Emergency departments are increasingly offering support to people with substance use disorder that extends beyond care for their acute presenting problem, such as linkages to treatment and other recovery support services, including life-saving medications for opioid use disorder like buprenorphine (known by common brand names like Suboxone and Subutex).
For treatment professionals and treatment systems: Emergency departments offer a critical point of contact for individuals with substance use disorder who may be minimally or not at all engaged in care. The results of this study suggest recovery coaches are roughly equivalent to clinical social workers for impacting post emergency department opioid overdose events. It remains unclear whether there are observable differences in other types of outcomes such as the proportion of patients achieving remission, employment, legal system involvement, psychosocial functioning, or other recovery outcomes between these two approaches as these were not reported.
For scientists: It can’t be known from these findings if recovery coaches and clinical social workers intervening in the emergency department have impact on the problem of subsequent opioid overdose events above no intervention at all. Future studies should test for this. Future studies might also examine whether and to what degree individuals assigned to recovery coaching actually received these services, thereby informing other work and recovery support recommendations. To test further also are any differences in other types of outcomes such as the proportion of patients achieving remission, employment, legal system involvement, psychosocial functioning, or other recovery outcomes between these two approaches. These were not reported in this study.
For policy makers: Emergency departments offer a critical point of contact with individuals with substance use disorder who may be minimally or not at all engaged in care. Ongoing funding to support development and evaluation of strategies to engage ED patients in care is likely to reduce the health care and financial burdens of opioid use and other substance use disorders.
Peer recovery support services like recovery coaches are increasingly being employed in hospital emergency departments to support people presenting with medical and psychiatric problems related to substance use disorder. Results from previous studies suggests recovery coaches can be instrumental in helping patients engage with substance use disorder care after emergency department discharge, while reducing emergency department readmissions and supporting better substance use related outcomes.
Some studies have also shown that engagement with recovery coaches is associated with reduced rates of subsequent opioid-involved overdose (see examples here & here), however, other studies have not shown a major benefit. Questions remain about the capacity for recovery coaches working in ED to effect more long-term outcomes like subsequent opioid poisoning events. Also, it is not yet known if outcomes for recovery coaching differ from more typical services provided during an ED visit – for example clinical social workers who help refer patients to outpatient care. To begin to address these questions, this randomized trial tested whether recovery coaching started in the ED with plans for ongoing support post-discharge was better at reducing overdose risk compared with social work services provided only during the ED visit.
HOW WAS THIS STUDY CONDUCTED?
This was a parallel, two-arm, randomized trial with 648 participants presenting to an ED with opioid overdose or other opioid use harms who received intervention by either a certified recovery coach or licensed clinical social worker. The primary study outcome was non-fatal opioid-involved overdose over 18-month follow-up.
Individuals presenting to a Rhode Island, USA hospital emergency department for opioid-involved overdose or opioid use disorder-related complications between November 2018 and May 2021 were invited to participate in this study and were randomized to receive either recovery coaching, or care from a licensed clinical social worker.
Recovery coaches used standard evidence-based interviewing and intervention techniques, shared their own lived experience with substance use and recovery, evaluated patients for readiness to seek treatment, offered referrals to treatment, helped patients navigate barriers to treatment, and provided drug overdose prevention education.
After the ED visit, recovery coaches then reached out to the patient daily for up to 10 days to initiate follow-up support using a community-based follow-up contact plan. In the first few days following discharge, recovery coaches helped patients navigate barriers to treatment, while providing continuing peer support and drug poisoning prevention education. Coaches then provided ongoing support for 90 days to those patients who engaged with coaching. Of note, the study did not report whether and to what degree participants engaged in recovery coaching after ED discharge because authors noted “this was a pragmatic trial”. That said, this does not necessarily mean it cannot be analyzed. In fact, this is a bit puzzling as to why they did not examine this as it would be very helpful to know how much recovery coaching each patient received and how that related to outcomes.
Also notably, the researchers did initially include a “no support” control group of patients who declined any behavioral intervention in their study design, however, recruitment for this arm was stopped after 6 months because eligible patients (those who did not want to meet with either a recovery coach or social worker) were also declining participation in the study.
Clinical social workers were similarly trained in a variety of evidence-based interviewing and intervention techniques, with their practice based on clinical experience rather than personal lived addiction recovery experience. They provided standard behavioral care using evidence-based interviewing and intervention techniques and referrals to treatment. Per standard practice, clinical social workers did not provide services to patients following ED discharge.
The primary study outcome was non-fatal opioid poisoning over 18-month follow-up, measured with statewide data from emergency medical services. Possible non-fatal opioid poisonings that occurred outside of the state of Rhode Island were not measured. Secondary outcomes included median time to first non-fatal overdose among those who overdosed, and death due to opioid overdose in the 18 months following the index ED visit.
The average age of study participants was 37 years, 68% were male, and 69% were White, 10% were mixed, biracial or multi-racial, 6% were Black, and 3% were Native American/Hawaiian. Two-thirds had a prior history of opioid overdose and 45% were being treated for an opioid overdose event when they entered the study. Many participants reported current or past substance use disorder treatment, with 28% currently in treatment, and 49% previously in treatment.
WHAT DID THIS STUDY FIND?
Non-fatal opioid overdose outcomes were similar between groups
In the recovery coaching group, 25% experienced an opioid-involved non-fatal overdose, statistically similar to the 29% of those in the social work group (see figure below). Across the entire sample including both groups, 27% of participants experienced an overdose during follow-up, with 18% experiencing one, 5% with two, 3% with three, and 2% with 4 or more. Among those with at least 1 non-fatal overdose, median time to overdose was 146 days after ED discharge for the recovery coaching group and 119 days for social work group – again, though, while seemingly quite a large difference there was a lot of variability within these groups, this difference did not reach statistical significance.
Fatal opioid overdose outcomes were also similar, though the median time to overdose slightly favored the social work condition
Regarding fatal overdose, 3% of the recovery coaching group and 5% of the social work group experienced fatal overdose. Among those with fatal overdose, median time to death was 124 days in the recovery coaching group and 202 for the social work group. This latter advantage for the social work group on time to overdose death just missed statistical significance.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study did not find a notable difference in opioid overdose events during the 18 months following an ED visit between patients randomized to recovery coaching with ongoing support during the 90 days after discharge versus clinical social work where services to aid follow-up care were only provided during the ED visit.
It’s possible that both these interventions help mitigate subsequent opioid poisoning, however, the absence of a ‘no support’ control group means this can’t be known from these results. It is also unclear why the recovery coaching group did not have more favorable outcomes both given potential benefits of peer support and the possibility of ongoing coaching for 90 days.
It may be helpful to highlight that whether and to what degree patients actually engaged with the recovery coaches was not reported in the current study so it is unclear whether the coaching truly did not add any benefit or not. Given that coaches outreached to patients up to 10 consecutive days after discharge to make contact, it seems more likely that recovery coaching and clinical social work produced similar effects than patients simply not connecting with their recovery coaches.
Studies to date support the potential of recovery coaches as well as licensed clinicians to help people with substance use disorder reduce or stop substance use across a range of settings. Recovery coaches appear to be especially capable of increasing treatment engagement, overall, which could reduce rates of subsequent opioid poisoning events. The capacity for recovery coaches to support changes in substance use and treatment engagement among patients presenting to EDs is more mixed. Another set of findings from this same overall study showed recovery coaching and social work led to similar treatment engagement as well. This may be due to the very challenging circumstances patients tend to be experiencing that lead to the ED visit. Also, some patients seeking care in EDs are in earlier stages of readiness to change their substance use (e.g., “pre-contemplative”) so they may be less inclined to follow up with treatment recommendations – or in this case with recovery coaches. Notably half of the sample overall had not attended prior treatment. So, future analyses might examine who in particular responded best to which particular treatment and continuing care approach. Approaches that allow for ongoing, but periodic low-intensity contact, like recovery management checkups, may be needed to best help patients with both high severity and much ambivalence about change. Linkages to harm reduction resources may also be good fits clinically with emergency department approaches to engaging such patients.
Regardless, EDs offer critical points of contact between recovery allies like recovery coaches and clinicians and people with active substance use disorder who may be minimally, or not at all engaged in care. Interventions like those investigated in this study are likely to confer benefits other than the outcomes measured.
This study did not include a ‘no support’ control group; thus, it can’t be known from this study if recovery coaching or care from a clinical social worker are superior to no intervention at all.
As mentioned above, whether and to what degree patients randomized to recovery coaching actually engaged with the recovery coaches was not reported in this study. Future work can help clarify whether patients did not benefit from recovery coaching after actually engaging with coaches, or whether it was challenging to get people to engage with the recovery coach at all.
The researchers utilized emergency medical services data from the state of Rhode Island to determine opioid poisoning events over the 18-minth follow-up period. It’s likely some participants experienced opioid poisoning events in states other than Rhode Island.
BOTTOM LINE
In this study, contrary to expectations, no meaningful difference was observed in rate of opioid overdose events following emergency department (ED) care provided by either recovery coaches or clinical social workers. It is unclear whether there were differences in other types of outcomes such as the proportion of patients achieving remission, employment, legal system involvement, psychosocial functioning, or other recovery outcomes as these were not reported.
For individuals and families seeking recovery: Emergency departments are increasingly offering support to people with substance use disorder that extends beyond care for their acute presenting problem, such as linkages to treatment and other recovery support services, including life-saving medications for opioid use disorder like buprenorphine (known by common brand names like Suboxone and Subutex).
For treatment professionals and treatment systems: Emergency departments offer a critical point of contact for individuals with substance use disorder who may be minimally or not at all engaged in care. The results of this study suggest recovery coaches are roughly equivalent to clinical social workers for impacting post emergency department opioid overdose events. It remains unclear whether there are observable differences in other types of outcomes such as the proportion of patients achieving remission, employment, legal system involvement, psychosocial functioning, or other recovery outcomes between these two approaches as these were not reported.
For scientists: It can’t be known from these findings if recovery coaches and clinical social workers intervening in the emergency department have impact on the problem of subsequent opioid overdose events above no intervention at all. Future studies should test for this. Future studies might also examine whether and to what degree individuals assigned to recovery coaching actually received these services, thereby informing other work and recovery support recommendations. To test further also are any differences in other types of outcomes such as the proportion of patients achieving remission, employment, legal system involvement, psychosocial functioning, or other recovery outcomes between these two approaches. These were not reported in this study.
For policy makers: Emergency departments offer a critical point of contact with individuals with substance use disorder who may be minimally or not at all engaged in care. Ongoing funding to support development and evaluation of strategies to engage ED patients in care is likely to reduce the health care and financial burdens of opioid use and other substance use disorders.
Peer recovery support services like recovery coaches are increasingly being employed in hospital emergency departments to support people presenting with medical and psychiatric problems related to substance use disorder. Results from previous studies suggests recovery coaches can be instrumental in helping patients engage with substance use disorder care after emergency department discharge, while reducing emergency department readmissions and supporting better substance use related outcomes.
Some studies have also shown that engagement with recovery coaches is associated with reduced rates of subsequent opioid-involved overdose (see examples here & here), however, other studies have not shown a major benefit. Questions remain about the capacity for recovery coaches working in ED to effect more long-term outcomes like subsequent opioid poisoning events. Also, it is not yet known if outcomes for recovery coaching differ from more typical services provided during an ED visit – for example clinical social workers who help refer patients to outpatient care. To begin to address these questions, this randomized trial tested whether recovery coaching started in the ED with plans for ongoing support post-discharge was better at reducing overdose risk compared with social work services provided only during the ED visit.
HOW WAS THIS STUDY CONDUCTED?
This was a parallel, two-arm, randomized trial with 648 participants presenting to an ED with opioid overdose or other opioid use harms who received intervention by either a certified recovery coach or licensed clinical social worker. The primary study outcome was non-fatal opioid-involved overdose over 18-month follow-up.
Individuals presenting to a Rhode Island, USA hospital emergency department for opioid-involved overdose or opioid use disorder-related complications between November 2018 and May 2021 were invited to participate in this study and were randomized to receive either recovery coaching, or care from a licensed clinical social worker.
Recovery coaches used standard evidence-based interviewing and intervention techniques, shared their own lived experience with substance use and recovery, evaluated patients for readiness to seek treatment, offered referrals to treatment, helped patients navigate barriers to treatment, and provided drug overdose prevention education.
After the ED visit, recovery coaches then reached out to the patient daily for up to 10 days to initiate follow-up support using a community-based follow-up contact plan. In the first few days following discharge, recovery coaches helped patients navigate barriers to treatment, while providing continuing peer support and drug poisoning prevention education. Coaches then provided ongoing support for 90 days to those patients who engaged with coaching. Of note, the study did not report whether and to what degree participants engaged in recovery coaching after ED discharge because authors noted “this was a pragmatic trial”. That said, this does not necessarily mean it cannot be analyzed. In fact, this is a bit puzzling as to why they did not examine this as it would be very helpful to know how much recovery coaching each patient received and how that related to outcomes.
Also notably, the researchers did initially include a “no support” control group of patients who declined any behavioral intervention in their study design, however, recruitment for this arm was stopped after 6 months because eligible patients (those who did not want to meet with either a recovery coach or social worker) were also declining participation in the study.
Clinical social workers were similarly trained in a variety of evidence-based interviewing and intervention techniques, with their practice based on clinical experience rather than personal lived addiction recovery experience. They provided standard behavioral care using evidence-based interviewing and intervention techniques and referrals to treatment. Per standard practice, clinical social workers did not provide services to patients following ED discharge.
The primary study outcome was non-fatal opioid poisoning over 18-month follow-up, measured with statewide data from emergency medical services. Possible non-fatal opioid poisonings that occurred outside of the state of Rhode Island were not measured. Secondary outcomes included median time to first non-fatal overdose among those who overdosed, and death due to opioid overdose in the 18 months following the index ED visit.
The average age of study participants was 37 years, 68% were male, and 69% were White, 10% were mixed, biracial or multi-racial, 6% were Black, and 3% were Native American/Hawaiian. Two-thirds had a prior history of opioid overdose and 45% were being treated for an opioid overdose event when they entered the study. Many participants reported current or past substance use disorder treatment, with 28% currently in treatment, and 49% previously in treatment.
WHAT DID THIS STUDY FIND?
Non-fatal opioid overdose outcomes were similar between groups
In the recovery coaching group, 25% experienced an opioid-involved non-fatal overdose, statistically similar to the 29% of those in the social work group (see figure below). Across the entire sample including both groups, 27% of participants experienced an overdose during follow-up, with 18% experiencing one, 5% with two, 3% with three, and 2% with 4 or more. Among those with at least 1 non-fatal overdose, median time to overdose was 146 days after ED discharge for the recovery coaching group and 119 days for social work group – again, though, while seemingly quite a large difference there was a lot of variability within these groups, this difference did not reach statistical significance.
Fatal opioid overdose outcomes were also similar, though the median time to overdose slightly favored the social work condition
Regarding fatal overdose, 3% of the recovery coaching group and 5% of the social work group experienced fatal overdose. Among those with fatal overdose, median time to death was 124 days in the recovery coaching group and 202 for the social work group. This latter advantage for the social work group on time to overdose death just missed statistical significance.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study did not find a notable difference in opioid overdose events during the 18 months following an ED visit between patients randomized to recovery coaching with ongoing support during the 90 days after discharge versus clinical social work where services to aid follow-up care were only provided during the ED visit.
It’s possible that both these interventions help mitigate subsequent opioid poisoning, however, the absence of a ‘no support’ control group means this can’t be known from these results. It is also unclear why the recovery coaching group did not have more favorable outcomes both given potential benefits of peer support and the possibility of ongoing coaching for 90 days.
It may be helpful to highlight that whether and to what degree patients actually engaged with the recovery coaches was not reported in the current study so it is unclear whether the coaching truly did not add any benefit or not. Given that coaches outreached to patients up to 10 consecutive days after discharge to make contact, it seems more likely that recovery coaching and clinical social work produced similar effects than patients simply not connecting with their recovery coaches.
Studies to date support the potential of recovery coaches as well as licensed clinicians to help people with substance use disorder reduce or stop substance use across a range of settings. Recovery coaches appear to be especially capable of increasing treatment engagement, overall, which could reduce rates of subsequent opioid poisoning events. The capacity for recovery coaches to support changes in substance use and treatment engagement among patients presenting to EDs is more mixed. Another set of findings from this same overall study showed recovery coaching and social work led to similar treatment engagement as well. This may be due to the very challenging circumstances patients tend to be experiencing that lead to the ED visit. Also, some patients seeking care in EDs are in earlier stages of readiness to change their substance use (e.g., “pre-contemplative”) so they may be less inclined to follow up with treatment recommendations – or in this case with recovery coaches. Notably half of the sample overall had not attended prior treatment. So, future analyses might examine who in particular responded best to which particular treatment and continuing care approach. Approaches that allow for ongoing, but periodic low-intensity contact, like recovery management checkups, may be needed to best help patients with both high severity and much ambivalence about change. Linkages to harm reduction resources may also be good fits clinically with emergency department approaches to engaging such patients.
Regardless, EDs offer critical points of contact between recovery allies like recovery coaches and clinicians and people with active substance use disorder who may be minimally, or not at all engaged in care. Interventions like those investigated in this study are likely to confer benefits other than the outcomes measured.
This study did not include a ‘no support’ control group; thus, it can’t be known from this study if recovery coaching or care from a clinical social worker are superior to no intervention at all.
As mentioned above, whether and to what degree patients randomized to recovery coaching actually engaged with the recovery coaches was not reported in this study. Future work can help clarify whether patients did not benefit from recovery coaching after actually engaging with coaches, or whether it was challenging to get people to engage with the recovery coach at all.
The researchers utilized emergency medical services data from the state of Rhode Island to determine opioid poisoning events over the 18-minth follow-up period. It’s likely some participants experienced opioid poisoning events in states other than Rhode Island.
BOTTOM LINE
In this study, contrary to expectations, no meaningful difference was observed in rate of opioid overdose events following emergency department (ED) care provided by either recovery coaches or clinical social workers. It is unclear whether there were differences in other types of outcomes such as the proportion of patients achieving remission, employment, legal system involvement, psychosocial functioning, or other recovery outcomes as these were not reported.
For individuals and families seeking recovery: Emergency departments are increasingly offering support to people with substance use disorder that extends beyond care for their acute presenting problem, such as linkages to treatment and other recovery support services, including life-saving medications for opioid use disorder like buprenorphine (known by common brand names like Suboxone and Subutex).
For treatment professionals and treatment systems: Emergency departments offer a critical point of contact for individuals with substance use disorder who may be minimally or not at all engaged in care. The results of this study suggest recovery coaches are roughly equivalent to clinical social workers for impacting post emergency department opioid overdose events. It remains unclear whether there are observable differences in other types of outcomes such as the proportion of patients achieving remission, employment, legal system involvement, psychosocial functioning, or other recovery outcomes between these two approaches as these were not reported.
For scientists: It can’t be known from these findings if recovery coaches and clinical social workers intervening in the emergency department have impact on the problem of subsequent opioid overdose events above no intervention at all. Future studies should test for this. Future studies might also examine whether and to what degree individuals assigned to recovery coaching actually received these services, thereby informing other work and recovery support recommendations. To test further also are any differences in other types of outcomes such as the proportion of patients achieving remission, employment, legal system involvement, psychosocial functioning, or other recovery outcomes between these two approaches. These were not reported in this study.
For policy makers: Emergency departments offer a critical point of contact with individuals with substance use disorder who may be minimally or not at all engaged in care. Ongoing funding to support development and evaluation of strategies to engage ED patients in care is likely to reduce the health care and financial burdens of opioid use and other substance use disorders.