Access to opioid use disorder treatment in US jails: Prevalence and related factors
The provision of opioid use disorder medications in criminal justice settings is an opportunity to reduce post-incarceration overdose and to lower treatment barriers for inmates. To better understand the availability of jail-based medication treatment in the US, this national study examined the prevalence of jails that provide opioid use disorder treatment, including FDA-approved medications, during incarceration, as well as the county-level factors associated with delivering these treatments.
Two-thirds of the US jail population has a current substance use disorder, and about one-quarter has an opioid use disorder. When individuals with opioid use disorder enter jail, lose access to illicit opioids, and begin a period of abstinence, their physiological tolerance to opioids decreases, which increases their risk of overdose if they return to illicit opioid use (e.g., upon release from jail).
Criminal justice settings offer an ideal opportunity to provide medication treatment for opioid use disorder, as a means to help reduce overdose risk and to help individuals initiate their path to wellness. Medications for opioid use disorder help prevent overdose and studies suggest that receiving medication treatment during and after incarceration is just as beneficial for incarcerated individuals as receiving community-based medication treatment is for non-incarcerated individuals.
Despite their benefits, studies have estimated that less than one-half of US jails offer medication treatment to all incarcerated individuals with an opioid use disorder, with many jails citing financial and regulatory factors as reasons for not providing it. There have been recent callsto action from federal institutions and other public health organizations, for increased access to opioid use disorder medication and other treatment services within jails and prisons, as well as coordinated treatment and services after release. This makes good sense from a societal perspective as well because assuming that at least a portion of this population’s crime is driven/related to their opioid use disorder, adequately treating it could go a long way to reducing or eradicating criminal recidivism on release.
As more jails and prisons answer this call to action, it is important to continue to evaluate the prevalence of providing medication treatment in jail as well as the factors that might influence their provision. Further understanding of jail-based treatment programs can help to better address potential barriers to their implementation, and ultimately expand access to medication treatment to help reduce post-incarceration overdose. This study examined the prevalence of US jails providing opioid use disorder medication treatment, and the county-level factors associated with it.
HOW WAS THIS STUDY CONDUCTED?
This study was a nationally representative cross-sectional survey study that examined prevalence and correlates of the provision of substance use disorder treatment services, including opioid use disorder medications, across 1,028 United States jails between 2022 and 2023.
A random sample of 2791 federally-listed jails, stratified by US Census region and selected to represent over 3,500 US jails, was invited to participate in the survey. Jails and detention facilities (not prisons) that hold individuals before and after sentencing were eligible. Survey data were linked to county-level data obtained from the Opioid Environment Policy Scan (OEPS) database, which offers a variety of opioid-related and county-level data. The researchers analyzed the prevalence of medication treatment provision and its relationship to county-level characteristics.
There was a modest survey response rate, with only 37% of jails responding (1028 out of 3500) and county-level data being available only for 927 jails. Like other nationally representative surveys, findings were weighted statistically to increase their fit with the overall distribution of jails in each Census region while also accounting for the reality that many individuals (jails in this case) will not respond to a survey despite being asked to do so. Ultimately, these weighted findings are the best, unbiased estimate of US jails.
Surveys were administered by mail, phone, and internet, and instructed recipients that the survey should be completed by jail staff who were knowledgeable about substance use disorder services available in their jails.
Surveys consisted of 23 multiple choice questions developed for this study that addressed jail characteristics and procedures for substance use disorder screening and treatment, including medication treatment for opioid use disorder. For the survey, medication treatment was defined as “the use of medications, often in combination with behavioral therapies, to provide a whole-patient approach to the treatment of opioid use disorder. Medications used include buprenorphine, methadone, and naltrexone.”
Primary outcomes included:
1. Any availability of addiction services, defined as jails currently having any kind of substance use treatment or recovery support for people during incarceration (available vs. not available).
2. Any availability of medication treatment, defined as jails that offered opioid use disorder medication treatment over the past year to at least some incarcerated people with opioid use disorder, meaning to specific groups like pregnant individuals, for example, but not to all inmates (available vs. not available).
3. Universal availability of medication treatment, defined as jails that offered opioid use disorder medication treatment over the past year to all incarcerated people with opioid use disorder (available vs. not available).
County-level characteristics of interest included:
1. Access to treatment: Jail’s driving distance to the nearest facility providing one or more medication treatments for opioid use disorder, according to SAMHSA’s treatment locator.
2. Jail-county’s social vulnerability: Measured with the CDC Social Vulnerability Index, which ranks counties based on 16 social factors (e.g., housing, transport, poverty). A lower percentile ranking reflects a less socially vulnerable county.
The majority of jails were located in non-metropolitan counties (56%) and had contracted healthcare-service delivery models (60%), wherein all health care services were provided by contracted vendors or clinicians. Twenty-one percent had hybrid models where healthcare was provided by a combination of contracted vendors, contracted clinicians, and jail employees. Fewer jails in the South completed the survey than did jails in other regions.
WHAT DID THIS STUDY FIND?
Fewer than half of the jails offered any opioid use disorder medication treatment
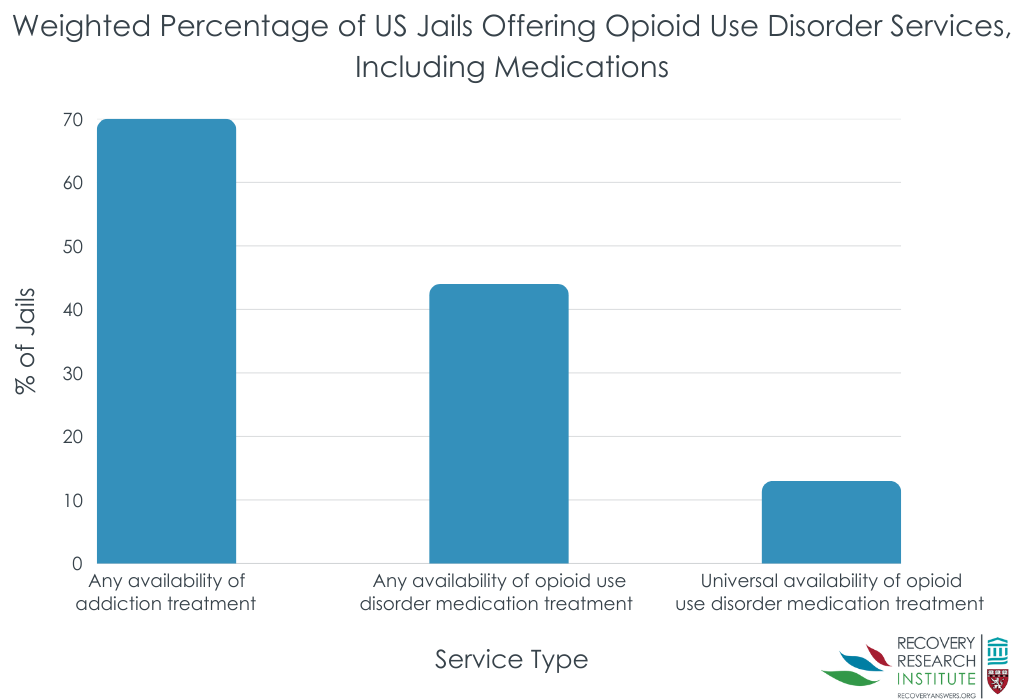
The majority of jails offered some kind of addiction treatment or recovery support services (70%), with mutual-help meetings (e.g., 12-step meetings like Narcotics Anonymous, or NA) being the most commonly offered service (63%), followed by co-occurring addiction and mental health services delivered by a licensed clinician (48%).
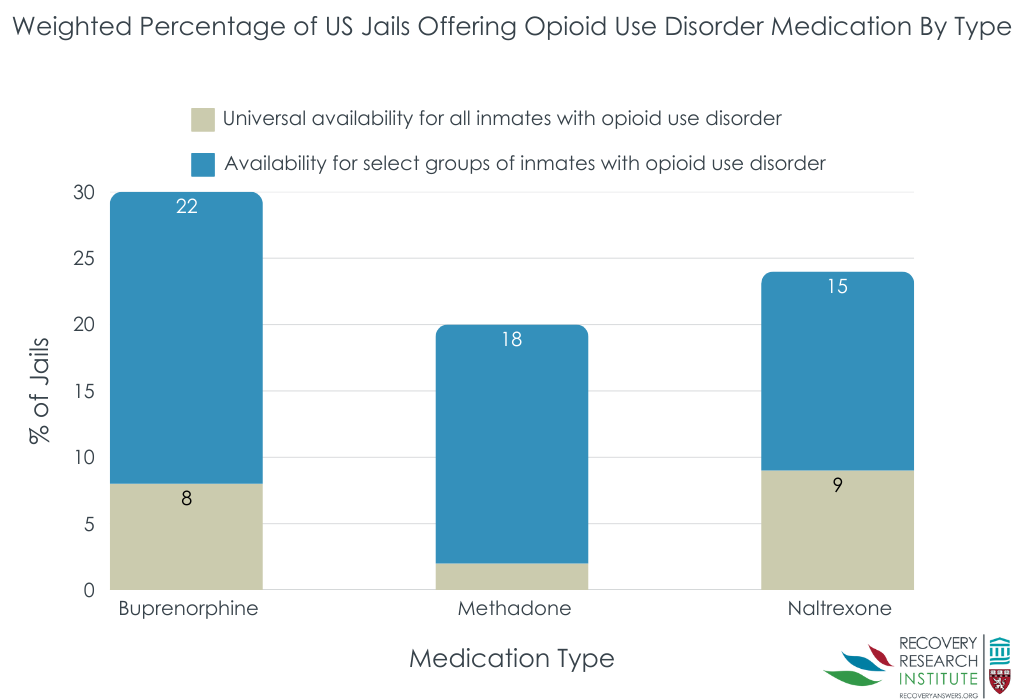
As illustrated below, 44% percent of jails offered opioid use disorder medication treatment to at least some incarcerated individuals with opioid use disorder. Among the jails that offered medication, 70% offered buprenorphine, 47% offered methadone, and 55% offered naltrexone .
Far fewer jails offered medication treatment to all individuals with opioid use disorder (13%). The most common reason for not offering medication treatment was jails not having adequate licensed staff (50%).
Jails were more likely to offer medication treatment if located in less socially vulnerable communities with nearby medication treatment facilities
Jails located in more socially vulnerable counties were less likely to offer any opioid use disorder medication treatment; for each percentile increase in a jail’s social vulnerability ranking (an index of several factors like housing, transportation, etc.), the odds of offering medication decreased by 55%.
Jails were also less likely to offer medication treatment when they were located further from the nearest facility offering opioid use disorder medication treatment, with the odds of medication treatment provision decreasing by 28% with every additional 18 minutes of drive time to the nearest medication treatment facility.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand the availability of opioid use disorder medication treatment, and factors associated with it, in criminal justice settings. Though periods of incarceration may be opportune times to offer opioid use disorder medications, this study suggests the vast majority of jails in the US do not offer these treatments. Consistent withprior research, only about 2 out of 5 jails offered one or more opioid use disorder medication treatment to at least a subset of incarcerated individuals.
Importantly, the most common reason for not offering medication treatment in jails was inadequate licensed staff to implement treatments. Findings also suggest that jails located further from community-based treatment facilities were less likely to offer medication treatment. Jails in communities with greater social vulnerability (e.g., more poverty, lower employment, etc.) were also less likely to offer medication treatment, highlighting the community-based factors that have a direct effect on medication treatment access in jails. These findings highlight the importance of surrounding community resources. They also point toward potential opportunities for partnerships with community-based medical professionals in neighboring regions to facilitate and promote adoption of medication treatment in jail-based settings. If regulations permit, video visits via telemedicine may also be a potential solution for jails located in more rural regions with fewer clinical and community resources.
Buprenorphine was the most commonly offered medication treatment across jails in this study, though some prior studies suggest naltrexone is the most common, and still others report equal distribution of all three types of FDA-approved medications. Inconsistent outcomes are likely attributable to relatively low survey response rates in criminal justice settings, with the majority of studies obtaining completed surveys from less than 50% of jails. This study used statistical analyses to account for expected low responses rates, suggesting while imperfect findings here may be the most rigorously-derived set of estimates. Medication treatment guidelines and patterns have also changed rapidly and frequently over the past several years, which may also account for inconsistencies across studies. Future investigations will further our understanding of criminal justice and treatment outcomes when inmates are offered multiple types of medication and when receiving different medication treatments.
Given that only 13% of jails offered medication treatment to all individuals with opioid use disorder during incarceration, additional efforts are needed to expand access to medication treatments in jails. Limiting medication treatment access to select groups reduces the availability of first-line treatments to opioid use disorder populations, and limits the reach of efforts to curb overdose death rates. By offering medication treatment to all individuals with opioid use disorder, and during multiple stages of incarceration (upon entry, release, etc.), we may be able to improve individual outcomes and help prevent overdose. Given common concerns around diversion of opioid agonist treatments, additional research is needed to determine optimal programmatic regulations and procedures for jail-based pharmacotherapy to help avoid diversion while enhancing access to treatment.
This survey had a particularly low response rate – despite efforts to account for this nonresponse, the findings may still not be entirely representative of US jails. The findings described here therefore may have overestimated the prevalence of medication treatment provision in jail settings.
Moreover, surveys did not verify that the jail-staff members who completed the surveys were knowledgeable about substance use disorder services available in their jails, demanding additional research.
This study did not assess the availability of medication treatment across all stages of incarceration (entry, linkage to community treatment upon release), which is an important component of overdose prevention requiring additional study.
BOTTOM LINE
The majority of jails offered some kind of addiction treatment or recovery support service, but only 2 in 5 offered any opioid use disorder medication treatment and only 13% offered medication treatment to all incarcerated individuals with opioid use disorder. Limited access to licensed prescribers was the most common reason for not offering medication treatment. Jails located in less socially vulnerable communities with nearby medication treatment facilities were most likely to offer medication treatment to individuals during incarceration. Findings emphasize the ongoing need to further expand opioid use disorder treatment access to adequately address the opioid overdose epidemic, as well as the need for increased financial and personnel resources within jails to overcome barriers to providing medication treatment during incarceration.
For individuals and families seeking recovery: Currently, medication treatments for opioid use disorder, including methadone, buprenorphine, and extended-release naltrexone, are not widely available for individuals with opioid use disorders while incarcerated. The availability of programs that offer such medications during incarceration are beginning to expand but additional work is needed to increase jail resources to do this. Medication is a helpful treatment option to seek out during incarceration, as well as after release from jail or prison, for individuals with opioid use disorder.
For treatment professionals and treatment systems: Given that the most common reason for not offering medication treatment in jails was inadequate resources (no access to licensed prescribers), and that jails located further from community-treatment facilities were less likely to offer medication treatment, treatment professionals might consider supporting the expansion of such jail-based treatment by forming partnerships with their local correctional system. Partnering with jails located further from treatment facilities may be particularly warranted for helping inmates initiate medication treatment in more rural counties and for ensuring inmate transitions to community-based care upon release, which could ultimately reduce post-incarceration overdose rates.
For scientists: Naturalistic longitudinal investigations of jails that are newly implementing treatment programs may help determine which program and treatment characteristics maximize benefits and minimize costs (reduced recidivism, positive treatment outcomes). Comparing outcomes of jail-based treatment programs with different program characteristics can also help to inform policy and best practices.
For policy makers: New initiatives and policies are necessary to increase the availability of opioid use disorder medication treatment in criminal justice settings, and to ensure ongoing low-barrier access to these treatments upon transition to the community. Additional research funding to study the effects of these policies and programs within jails and prisons will clarify their risks, benefits, and cost-effectiveness to help better inform future initiatives aimed at curbing the overdose epidemic.
Two-thirds of the US jail population has a current substance use disorder, and about one-quarter has an opioid use disorder. When individuals with opioid use disorder enter jail, lose access to illicit opioids, and begin a period of abstinence, their physiological tolerance to opioids decreases, which increases their risk of overdose if they return to illicit opioid use (e.g., upon release from jail).
Criminal justice settings offer an ideal opportunity to provide medication treatment for opioid use disorder, as a means to help reduce overdose risk and to help individuals initiate their path to wellness. Medications for opioid use disorder help prevent overdose and studies suggest that receiving medication treatment during and after incarceration is just as beneficial for incarcerated individuals as receiving community-based medication treatment is for non-incarcerated individuals.
Despite their benefits, studies have estimated that less than one-half of US jails offer medication treatment to all incarcerated individuals with an opioid use disorder, with many jails citing financial and regulatory factors as reasons for not providing it. There have been recent callsto action from federal institutions and other public health organizations, for increased access to opioid use disorder medication and other treatment services within jails and prisons, as well as coordinated treatment and services after release. This makes good sense from a societal perspective as well because assuming that at least a portion of this population’s crime is driven/related to their opioid use disorder, adequately treating it could go a long way to reducing or eradicating criminal recidivism on release.
As more jails and prisons answer this call to action, it is important to continue to evaluate the prevalence of providing medication treatment in jail as well as the factors that might influence their provision. Further understanding of jail-based treatment programs can help to better address potential barriers to their implementation, and ultimately expand access to medication treatment to help reduce post-incarceration overdose. This study examined the prevalence of US jails providing opioid use disorder medication treatment, and the county-level factors associated with it.
HOW WAS THIS STUDY CONDUCTED?
This study was a nationally representative cross-sectional survey study that examined prevalence and correlates of the provision of substance use disorder treatment services, including opioid use disorder medications, across 1,028 United States jails between 2022 and 2023.
A random sample of 2791 federally-listed jails, stratified by US Census region and selected to represent over 3,500 US jails, was invited to participate in the survey. Jails and detention facilities (not prisons) that hold individuals before and after sentencing were eligible. Survey data were linked to county-level data obtained from the Opioid Environment Policy Scan (OEPS) database, which offers a variety of opioid-related and county-level data. The researchers analyzed the prevalence of medication treatment provision and its relationship to county-level characteristics.
There was a modest survey response rate, with only 37% of jails responding (1028 out of 3500) and county-level data being available only for 927 jails. Like other nationally representative surveys, findings were weighted statistically to increase their fit with the overall distribution of jails in each Census region while also accounting for the reality that many individuals (jails in this case) will not respond to a survey despite being asked to do so. Ultimately, these weighted findings are the best, unbiased estimate of US jails.
Surveys were administered by mail, phone, and internet, and instructed recipients that the survey should be completed by jail staff who were knowledgeable about substance use disorder services available in their jails.
Surveys consisted of 23 multiple choice questions developed for this study that addressed jail characteristics and procedures for substance use disorder screening and treatment, including medication treatment for opioid use disorder. For the survey, medication treatment was defined as “the use of medications, often in combination with behavioral therapies, to provide a whole-patient approach to the treatment of opioid use disorder. Medications used include buprenorphine, methadone, and naltrexone.”
Primary outcomes included:
1. Any availability of addiction services, defined as jails currently having any kind of substance use treatment or recovery support for people during incarceration (available vs. not available).
2. Any availability of medication treatment, defined as jails that offered opioid use disorder medication treatment over the past year to at least some incarcerated people with opioid use disorder, meaning to specific groups like pregnant individuals, for example, but not to all inmates (available vs. not available).
3. Universal availability of medication treatment, defined as jails that offered opioid use disorder medication treatment over the past year to all incarcerated people with opioid use disorder (available vs. not available).
County-level characteristics of interest included:
1. Access to treatment: Jail’s driving distance to the nearest facility providing one or more medication treatments for opioid use disorder, according to SAMHSA’s treatment locator.
2. Jail-county’s social vulnerability: Measured with the CDC Social Vulnerability Index, which ranks counties based on 16 social factors (e.g., housing, transport, poverty). A lower percentile ranking reflects a less socially vulnerable county.
The majority of jails were located in non-metropolitan counties (56%) and had contracted healthcare-service delivery models (60%), wherein all health care services were provided by contracted vendors or clinicians. Twenty-one percent had hybrid models where healthcare was provided by a combination of contracted vendors, contracted clinicians, and jail employees. Fewer jails in the South completed the survey than did jails in other regions.
WHAT DID THIS STUDY FIND?
Fewer than half of the jails offered any opioid use disorder medication treatment
The majority of jails offered some kind of addiction treatment or recovery support services (70%), with mutual-help meetings (e.g., 12-step meetings like Narcotics Anonymous, or NA) being the most commonly offered service (63%), followed by co-occurring addiction and mental health services delivered by a licensed clinician (48%).
As illustrated below, 44% percent of jails offered opioid use disorder medication treatment to at least some incarcerated individuals with opioid use disorder. Among the jails that offered medication, 70% offered buprenorphine, 47% offered methadone, and 55% offered naltrexone .
Far fewer jails offered medication treatment to all individuals with opioid use disorder (13%). The most common reason for not offering medication treatment was jails not having adequate licensed staff (50%).
Jails were more likely to offer medication treatment if located in less socially vulnerable communities with nearby medication treatment facilities
Jails located in more socially vulnerable counties were less likely to offer any opioid use disorder medication treatment; for each percentile increase in a jail’s social vulnerability ranking (an index of several factors like housing, transportation, etc.), the odds of offering medication decreased by 55%.
Jails were also less likely to offer medication treatment when they were located further from the nearest facility offering opioid use disorder medication treatment, with the odds of medication treatment provision decreasing by 28% with every additional 18 minutes of drive time to the nearest medication treatment facility.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand the availability of opioid use disorder medication treatment, and factors associated with it, in criminal justice settings. Though periods of incarceration may be opportune times to offer opioid use disorder medications, this study suggests the vast majority of jails in the US do not offer these treatments. Consistent withprior research, only about 2 out of 5 jails offered one or more opioid use disorder medication treatment to at least a subset of incarcerated individuals.
Importantly, the most common reason for not offering medication treatment in jails was inadequate licensed staff to implement treatments. Findings also suggest that jails located further from community-based treatment facilities were less likely to offer medication treatment. Jails in communities with greater social vulnerability (e.g., more poverty, lower employment, etc.) were also less likely to offer medication treatment, highlighting the community-based factors that have a direct effect on medication treatment access in jails. These findings highlight the importance of surrounding community resources. They also point toward potential opportunities for partnerships with community-based medical professionals in neighboring regions to facilitate and promote adoption of medication treatment in jail-based settings. If regulations permit, video visits via telemedicine may also be a potential solution for jails located in more rural regions with fewer clinical and community resources.
Buprenorphine was the most commonly offered medication treatment across jails in this study, though some prior studies suggest naltrexone is the most common, and still others report equal distribution of all three types of FDA-approved medications. Inconsistent outcomes are likely attributable to relatively low survey response rates in criminal justice settings, with the majority of studies obtaining completed surveys from less than 50% of jails. This study used statistical analyses to account for expected low responses rates, suggesting while imperfect findings here may be the most rigorously-derived set of estimates. Medication treatment guidelines and patterns have also changed rapidly and frequently over the past several years, which may also account for inconsistencies across studies. Future investigations will further our understanding of criminal justice and treatment outcomes when inmates are offered multiple types of medication and when receiving different medication treatments.
Given that only 13% of jails offered medication treatment to all individuals with opioid use disorder during incarceration, additional efforts are needed to expand access to medication treatments in jails. Limiting medication treatment access to select groups reduces the availability of first-line treatments to opioid use disorder populations, and limits the reach of efforts to curb overdose death rates. By offering medication treatment to all individuals with opioid use disorder, and during multiple stages of incarceration (upon entry, release, etc.), we may be able to improve individual outcomes and help prevent overdose. Given common concerns around diversion of opioid agonist treatments, additional research is needed to determine optimal programmatic regulations and procedures for jail-based pharmacotherapy to help avoid diversion while enhancing access to treatment.
This survey had a particularly low response rate – despite efforts to account for this nonresponse, the findings may still not be entirely representative of US jails. The findings described here therefore may have overestimated the prevalence of medication treatment provision in jail settings.
Moreover, surveys did not verify that the jail-staff members who completed the surveys were knowledgeable about substance use disorder services available in their jails, demanding additional research.
This study did not assess the availability of medication treatment across all stages of incarceration (entry, linkage to community treatment upon release), which is an important component of overdose prevention requiring additional study.
BOTTOM LINE
The majority of jails offered some kind of addiction treatment or recovery support service, but only 2 in 5 offered any opioid use disorder medication treatment and only 13% offered medication treatment to all incarcerated individuals with opioid use disorder. Limited access to licensed prescribers was the most common reason for not offering medication treatment. Jails located in less socially vulnerable communities with nearby medication treatment facilities were most likely to offer medication treatment to individuals during incarceration. Findings emphasize the ongoing need to further expand opioid use disorder treatment access to adequately address the opioid overdose epidemic, as well as the need for increased financial and personnel resources within jails to overcome barriers to providing medication treatment during incarceration.
For individuals and families seeking recovery: Currently, medication treatments for opioid use disorder, including methadone, buprenorphine, and extended-release naltrexone, are not widely available for individuals with opioid use disorders while incarcerated. The availability of programs that offer such medications during incarceration are beginning to expand but additional work is needed to increase jail resources to do this. Medication is a helpful treatment option to seek out during incarceration, as well as after release from jail or prison, for individuals with opioid use disorder.
For treatment professionals and treatment systems: Given that the most common reason for not offering medication treatment in jails was inadequate resources (no access to licensed prescribers), and that jails located further from community-treatment facilities were less likely to offer medication treatment, treatment professionals might consider supporting the expansion of such jail-based treatment by forming partnerships with their local correctional system. Partnering with jails located further from treatment facilities may be particularly warranted for helping inmates initiate medication treatment in more rural counties and for ensuring inmate transitions to community-based care upon release, which could ultimately reduce post-incarceration overdose rates.
For scientists: Naturalistic longitudinal investigations of jails that are newly implementing treatment programs may help determine which program and treatment characteristics maximize benefits and minimize costs (reduced recidivism, positive treatment outcomes). Comparing outcomes of jail-based treatment programs with different program characteristics can also help to inform policy and best practices.
For policy makers: New initiatives and policies are necessary to increase the availability of opioid use disorder medication treatment in criminal justice settings, and to ensure ongoing low-barrier access to these treatments upon transition to the community. Additional research funding to study the effects of these policies and programs within jails and prisons will clarify their risks, benefits, and cost-effectiveness to help better inform future initiatives aimed at curbing the overdose epidemic.
Two-thirds of the US jail population has a current substance use disorder, and about one-quarter has an opioid use disorder. When individuals with opioid use disorder enter jail, lose access to illicit opioids, and begin a period of abstinence, their physiological tolerance to opioids decreases, which increases their risk of overdose if they return to illicit opioid use (e.g., upon release from jail).
Criminal justice settings offer an ideal opportunity to provide medication treatment for opioid use disorder, as a means to help reduce overdose risk and to help individuals initiate their path to wellness. Medications for opioid use disorder help prevent overdose and studies suggest that receiving medication treatment during and after incarceration is just as beneficial for incarcerated individuals as receiving community-based medication treatment is for non-incarcerated individuals.
Despite their benefits, studies have estimated that less than one-half of US jails offer medication treatment to all incarcerated individuals with an opioid use disorder, with many jails citing financial and regulatory factors as reasons for not providing it. There have been recent callsto action from federal institutions and other public health organizations, for increased access to opioid use disorder medication and other treatment services within jails and prisons, as well as coordinated treatment and services after release. This makes good sense from a societal perspective as well because assuming that at least a portion of this population’s crime is driven/related to their opioid use disorder, adequately treating it could go a long way to reducing or eradicating criminal recidivism on release.
As more jails and prisons answer this call to action, it is important to continue to evaluate the prevalence of providing medication treatment in jail as well as the factors that might influence their provision. Further understanding of jail-based treatment programs can help to better address potential barriers to their implementation, and ultimately expand access to medication treatment to help reduce post-incarceration overdose. This study examined the prevalence of US jails providing opioid use disorder medication treatment, and the county-level factors associated with it.
HOW WAS THIS STUDY CONDUCTED?
This study was a nationally representative cross-sectional survey study that examined prevalence and correlates of the provision of substance use disorder treatment services, including opioid use disorder medications, across 1,028 United States jails between 2022 and 2023.
A random sample of 2791 federally-listed jails, stratified by US Census region and selected to represent over 3,500 US jails, was invited to participate in the survey. Jails and detention facilities (not prisons) that hold individuals before and after sentencing were eligible. Survey data were linked to county-level data obtained from the Opioid Environment Policy Scan (OEPS) database, which offers a variety of opioid-related and county-level data. The researchers analyzed the prevalence of medication treatment provision and its relationship to county-level characteristics.
There was a modest survey response rate, with only 37% of jails responding (1028 out of 3500) and county-level data being available only for 927 jails. Like other nationally representative surveys, findings were weighted statistically to increase their fit with the overall distribution of jails in each Census region while also accounting for the reality that many individuals (jails in this case) will not respond to a survey despite being asked to do so. Ultimately, these weighted findings are the best, unbiased estimate of US jails.
Surveys were administered by mail, phone, and internet, and instructed recipients that the survey should be completed by jail staff who were knowledgeable about substance use disorder services available in their jails.
Surveys consisted of 23 multiple choice questions developed for this study that addressed jail characteristics and procedures for substance use disorder screening and treatment, including medication treatment for opioid use disorder. For the survey, medication treatment was defined as “the use of medications, often in combination with behavioral therapies, to provide a whole-patient approach to the treatment of opioid use disorder. Medications used include buprenorphine, methadone, and naltrexone.”
Primary outcomes included:
1. Any availability of addiction services, defined as jails currently having any kind of substance use treatment or recovery support for people during incarceration (available vs. not available).
2. Any availability of medication treatment, defined as jails that offered opioid use disorder medication treatment over the past year to at least some incarcerated people with opioid use disorder, meaning to specific groups like pregnant individuals, for example, but not to all inmates (available vs. not available).
3. Universal availability of medication treatment, defined as jails that offered opioid use disorder medication treatment over the past year to all incarcerated people with opioid use disorder (available vs. not available).
County-level characteristics of interest included:
1. Access to treatment: Jail’s driving distance to the nearest facility providing one or more medication treatments for opioid use disorder, according to SAMHSA’s treatment locator.
2. Jail-county’s social vulnerability: Measured with the CDC Social Vulnerability Index, which ranks counties based on 16 social factors (e.g., housing, transport, poverty). A lower percentile ranking reflects a less socially vulnerable county.
The majority of jails were located in non-metropolitan counties (56%) and had contracted healthcare-service delivery models (60%), wherein all health care services were provided by contracted vendors or clinicians. Twenty-one percent had hybrid models where healthcare was provided by a combination of contracted vendors, contracted clinicians, and jail employees. Fewer jails in the South completed the survey than did jails in other regions.
WHAT DID THIS STUDY FIND?
Fewer than half of the jails offered any opioid use disorder medication treatment
The majority of jails offered some kind of addiction treatment or recovery support services (70%), with mutual-help meetings (e.g., 12-step meetings like Narcotics Anonymous, or NA) being the most commonly offered service (63%), followed by co-occurring addiction and mental health services delivered by a licensed clinician (48%).
As illustrated below, 44% percent of jails offered opioid use disorder medication treatment to at least some incarcerated individuals with opioid use disorder. Among the jails that offered medication, 70% offered buprenorphine, 47% offered methadone, and 55% offered naltrexone .
Far fewer jails offered medication treatment to all individuals with opioid use disorder (13%). The most common reason for not offering medication treatment was jails not having adequate licensed staff (50%).
Jails were more likely to offer medication treatment if located in less socially vulnerable communities with nearby medication treatment facilities
Jails located in more socially vulnerable counties were less likely to offer any opioid use disorder medication treatment; for each percentile increase in a jail’s social vulnerability ranking (an index of several factors like housing, transportation, etc.), the odds of offering medication decreased by 55%.
Jails were also less likely to offer medication treatment when they were located further from the nearest facility offering opioid use disorder medication treatment, with the odds of medication treatment provision decreasing by 28% with every additional 18 minutes of drive time to the nearest medication treatment facility.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand the availability of opioid use disorder medication treatment, and factors associated with it, in criminal justice settings. Though periods of incarceration may be opportune times to offer opioid use disorder medications, this study suggests the vast majority of jails in the US do not offer these treatments. Consistent withprior research, only about 2 out of 5 jails offered one or more opioid use disorder medication treatment to at least a subset of incarcerated individuals.
Importantly, the most common reason for not offering medication treatment in jails was inadequate licensed staff to implement treatments. Findings also suggest that jails located further from community-based treatment facilities were less likely to offer medication treatment. Jails in communities with greater social vulnerability (e.g., more poverty, lower employment, etc.) were also less likely to offer medication treatment, highlighting the community-based factors that have a direct effect on medication treatment access in jails. These findings highlight the importance of surrounding community resources. They also point toward potential opportunities for partnerships with community-based medical professionals in neighboring regions to facilitate and promote adoption of medication treatment in jail-based settings. If regulations permit, video visits via telemedicine may also be a potential solution for jails located in more rural regions with fewer clinical and community resources.
Buprenorphine was the most commonly offered medication treatment across jails in this study, though some prior studies suggest naltrexone is the most common, and still others report equal distribution of all three types of FDA-approved medications. Inconsistent outcomes are likely attributable to relatively low survey response rates in criminal justice settings, with the majority of studies obtaining completed surveys from less than 50% of jails. This study used statistical analyses to account for expected low responses rates, suggesting while imperfect findings here may be the most rigorously-derived set of estimates. Medication treatment guidelines and patterns have also changed rapidly and frequently over the past several years, which may also account for inconsistencies across studies. Future investigations will further our understanding of criminal justice and treatment outcomes when inmates are offered multiple types of medication and when receiving different medication treatments.
Given that only 13% of jails offered medication treatment to all individuals with opioid use disorder during incarceration, additional efforts are needed to expand access to medication treatments in jails. Limiting medication treatment access to select groups reduces the availability of first-line treatments to opioid use disorder populations, and limits the reach of efforts to curb overdose death rates. By offering medication treatment to all individuals with opioid use disorder, and during multiple stages of incarceration (upon entry, release, etc.), we may be able to improve individual outcomes and help prevent overdose. Given common concerns around diversion of opioid agonist treatments, additional research is needed to determine optimal programmatic regulations and procedures for jail-based pharmacotherapy to help avoid diversion while enhancing access to treatment.
This survey had a particularly low response rate – despite efforts to account for this nonresponse, the findings may still not be entirely representative of US jails. The findings described here therefore may have overestimated the prevalence of medication treatment provision in jail settings.
Moreover, surveys did not verify that the jail-staff members who completed the surveys were knowledgeable about substance use disorder services available in their jails, demanding additional research.
This study did not assess the availability of medication treatment across all stages of incarceration (entry, linkage to community treatment upon release), which is an important component of overdose prevention requiring additional study.
BOTTOM LINE
The majority of jails offered some kind of addiction treatment or recovery support service, but only 2 in 5 offered any opioid use disorder medication treatment and only 13% offered medication treatment to all incarcerated individuals with opioid use disorder. Limited access to licensed prescribers was the most common reason for not offering medication treatment. Jails located in less socially vulnerable communities with nearby medication treatment facilities were most likely to offer medication treatment to individuals during incarceration. Findings emphasize the ongoing need to further expand opioid use disorder treatment access to adequately address the opioid overdose epidemic, as well as the need for increased financial and personnel resources within jails to overcome barriers to providing medication treatment during incarceration.
For individuals and families seeking recovery: Currently, medication treatments for opioid use disorder, including methadone, buprenorphine, and extended-release naltrexone, are not widely available for individuals with opioid use disorders while incarcerated. The availability of programs that offer such medications during incarceration are beginning to expand but additional work is needed to increase jail resources to do this. Medication is a helpful treatment option to seek out during incarceration, as well as after release from jail or prison, for individuals with opioid use disorder.
For treatment professionals and treatment systems: Given that the most common reason for not offering medication treatment in jails was inadequate resources (no access to licensed prescribers), and that jails located further from community-treatment facilities were less likely to offer medication treatment, treatment professionals might consider supporting the expansion of such jail-based treatment by forming partnerships with their local correctional system. Partnering with jails located further from treatment facilities may be particularly warranted for helping inmates initiate medication treatment in more rural counties and for ensuring inmate transitions to community-based care upon release, which could ultimately reduce post-incarceration overdose rates.
For scientists: Naturalistic longitudinal investigations of jails that are newly implementing treatment programs may help determine which program and treatment characteristics maximize benefits and minimize costs (reduced recidivism, positive treatment outcomes). Comparing outcomes of jail-based treatment programs with different program characteristics can also help to inform policy and best practices.
For policy makers: New initiatives and policies are necessary to increase the availability of opioid use disorder medication treatment in criminal justice settings, and to ensure ongoing low-barrier access to these treatments upon transition to the community. Additional research funding to study the effects of these policies and programs within jails and prisons will clarify their risks, benefits, and cost-effectiveness to help better inform future initiatives aimed at curbing the overdose epidemic.