Can gabapentin help people with alcohol use disorder by improving sleep?
Gabapentin is a commonly prescribed medication for alcohol use disorder, though it is not FDA approved to treat the disorder and its therapeutic mechanisms of action remain unclear. Heavy alcohol use is known to radically affect the nature, duration, and quality of sleep. Therefore, this study examined how gabapentin affected sleep in people seeking alcohol use disorder treatment, with the idea that this medication may be indirectly improving alcohol use outcomes by improving sleep.
In this study, using data from a clinical trial of gabapentin (also known by the brand name “Neurontin”) for alcohol use disorder, the researchers examined whether gabapentin aids alcohol use disorder recovery by reducing sleep problems. They assessed the effect of gabapentin on insomnia, as well as how participants’ history of alcohol withdrawal affects the gabapentin/insomnia relationship.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of data from a randomized controlled trial showing gabapentin outperformed placebo for individuals alcohol use disorder and current or past alcohol withdrawal, to determine whether gabapentin’s effects on alcohol use help by decreasing sleep problems, as well as how participants’ history of alcohol withdrawal affect the insomnia/gabapentin relationship.
In the initial clinical trial, participants were randomized to receive either gabapentin (with dose gradually increased over 5 days to target 1200mg) or placebo. Gabapentin is FDA approved for seizures and neuropathic pain, but is sometimes prescribed off-label to address anxiety in those with substance use disorder – typically “rebound” anxiety that emerges after someone quits or cuts back on alcohol.
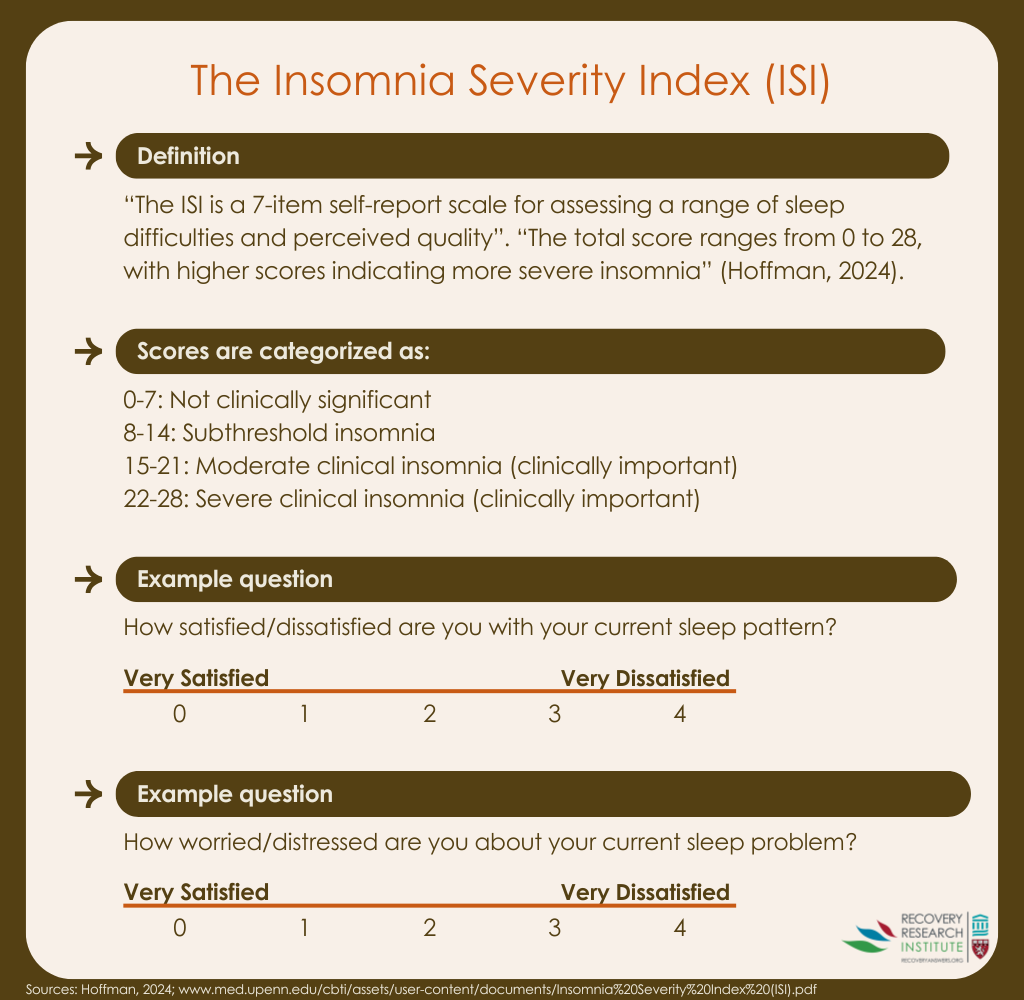
Participants were assessed on a range of outcome measures at treatment intake, and then at 2, 4, 6, 8, 10, 12, and 16 weeks. Primary outcome measures for this study included the Insomnia Severity Index (measuring sleep problems), the Alcohol Dependence Scale (measuring alcohol use disorder symptom severity), and the Alcohol Withdrawal Scale (measuring severity of alcohol withdrawal symptoms).
Drinking during treatment was also measured using a calendar-based self-report. The researchers explored gabapentin’s effects on sleep and drinking in the full study sample, and within a sub-sample of participants with moderate to severe insomnia symptoms based on Insomnia Severity Index scores at baseline.
The study sample of 90 individuals with alcohol use disorder was 77% male and 23% female, and on average, had symptoms consistent with moderate alcohol use disorder severity (4-5 out of 11), and subthreshold insomnia. Nearly half of the sample, however, had moderate to severe levels of clinically significant insomnia.
WHAT DID THIS STUDY FIND?
Gabapentin was associated with slightly better sleep outcomes
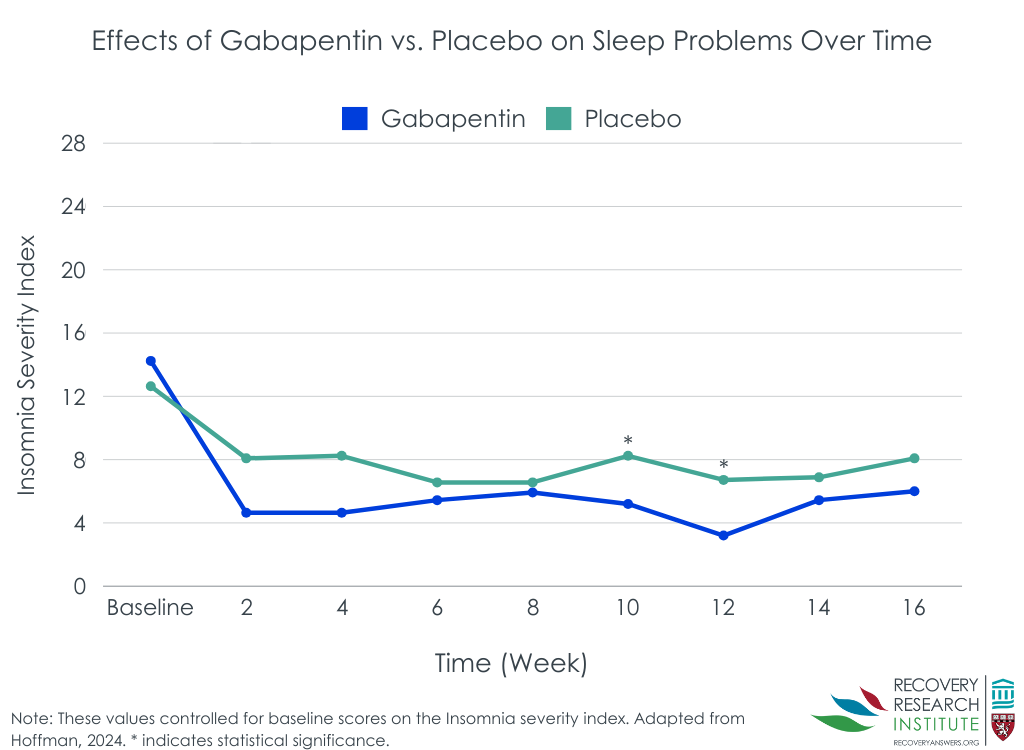
Over the course of the study, participants randomized to receive gabapentin reported slightly better sleep, with average Insomnia Severity Index scores of 5.5 versus 7.8 for controls. While these differences were statistically significant, indicating the differences were not likely to be due to chance, a difference of ~2 points on the Insomnia Severity Index, which ranges from 0-28.
Differences between groups on change in the Insomnia Severity Index scores from beginning to end of treatment were more notable, with participants receiving gabapentin showing a 61% improvement, and controls showing a 38% improvement.
When exploring between-group differences in sleep scores at each assessment time-point, groups were different on Insomnia Severity Index scores at weeks 10 and 12, but not at the other assessment time-points (see Figure below).
Participants with insomnia appeared to benefit more from gabapentin
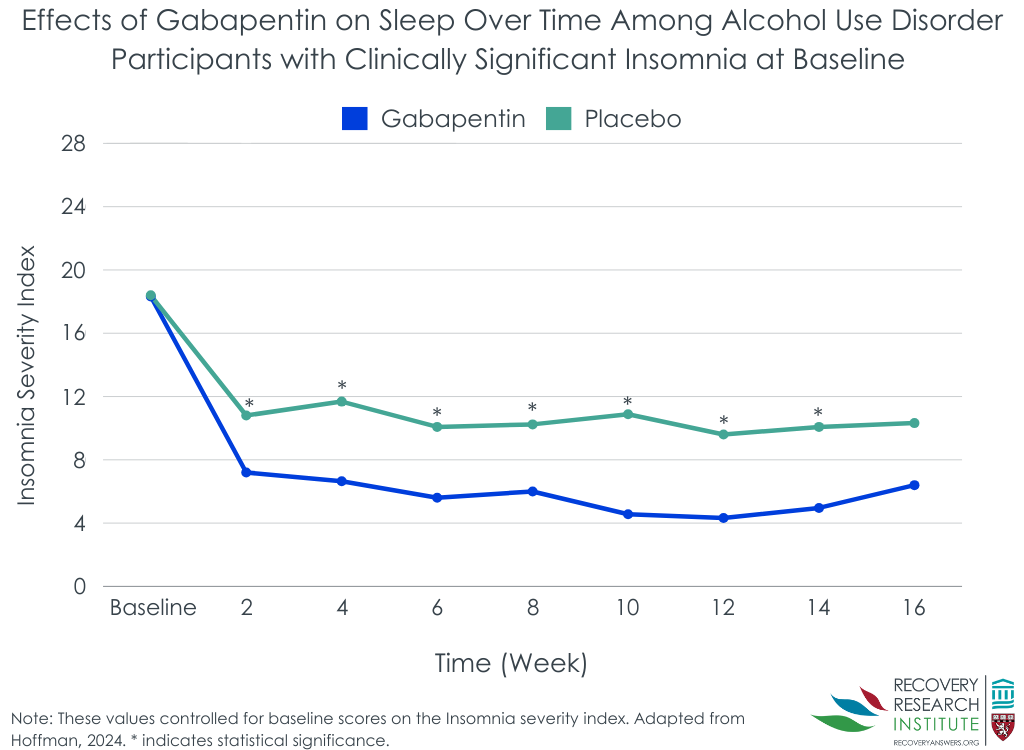
When considering just the 43 participants with moderate to severe insomnia at study baseline, participants receiving gabapentin had an average Insomnia Severity Index score across the study of 6.1, while controls’ average score was 10.6 . Though this is still a relatively small effect , it suggests gabapentin may benefit individuals with alcohol use disorder and insomnia more than those with alcohol use disorder alone, at least in terms of producing sleep benefits.
In terms of change in insomnia severity scores from the beginning to the end of treatment, between group differences were similar to those seen in the full sample. Those receiving gabapentin showed a 66% improvement in Insomnia Severity Index scores, while controls showed a 42% improvement.
Notably, when exploring between-group differences in sleep scores at each assessment time-point, in the insomnia sub-sample, groups were different on Insomnia Severity Index scores at all time-points except the final assessment at week 16.
Gabapentin was most effective among those with insomnia but did not work by improving sleep problems as expected
Gabapentin was found to reduce within-treatment alcohol consumption regardless of participants’ baseline insomnia status; however, it had a greater impact on reducing within-treatment drinking among participants with higher baseline insomnia severity.
The researchers had previously shown that participants with greater baseline alcohol withdrawal severity benefited more from gabapentin in terms of drinking reductions than participants with lower baseline alcohol withdrawal severity. However, this relationship was not markedly affected when Insomnia Severity Index scores were considered.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Gabapentin may lead to marginal improvements in sleep problems in people seeking treatment for alcohol use disorder, and possibly larger improvements for those with clinically significant insomnia at baseline. However, the stronger benefit of gabapentin on alcohol use outcomes compared to placebo, among those with more alcohol withdrawal symptoms was not explained by reductions in insomnia symptoms. While gabapentin may help address both alcohol use and sleep, it does not appear to improve alcohol use by improving sleep. The sample size in this study was small, however, and formal mediation tests were not conducted – which examine how an intervention works (also sometimes referred to as potential “mechanisms”). Future research with larger samples designed specifically to test whether gabapentin improves alcohol use, in part, by addressing sleep problems is needed.
These findings come with other caveats. First, though insomnia severity was notably reduced from beginning to end of treatment in this study, such reductions are to be expected regardless of treatment type. Even without medications, insomnia tends to improve as people with alcohol use disorder stop or reduce their drinking. This was evidenced by notable reductions in insomnia scores from beginning to end of treatment in both the gabapentin and placebo conditions in this study.
Second, it is possible that the greater reductions insomnia scores in participants with clinically significant insomnia was at least in part a statistical function of these participants having more room for improvement (i.e., “regression to the mean”).
Third, it is also important to note that gabapentin has psychoactive effects and therefore participants may have known if they were prescribed gabapentin or placebo – if more people in the gabapentin group thought they were receiving the study medication it could be that their positive expectancies, rather than the medication’s effects, explained better sleep outcomes. In the initial trial, however, more side effects in the gabapentin group (an indication that someone is receiving the active medication) did not explain its positive effects on alcohol use. Thus it is unlikely – though still possible – that positive expectancies are accounting for observed medication benefit.
Fourth, a 2-point improvement in the gabapentin group was statistically significant but it is unclear whether a patient would actually feel they slept better at that level of improvement. Indeed, the direction is encouraging, but future work should examine whether this is sufficient magnitude to result in patients’ perceived change – e.g. feeling better rested.
Finally, though the Insomnia Severity Index is a validated measure and is a reasonable way to assess sleep problems in a clinical trial, it does not include an assessment of how long the individual has been experiencing sleep problems – a 3-month duration is needed for DSM diagnosis of insomnia disorder. Ideally future studies exploring gabapentin’s effects on sleep in this population will also include objective measures of sleep functioning like polysomnography.
Clinically, it is important to note that although gabapentin is commonly prescribed to treat alcohol use disorder, it is not Food and Drug Administration (FDA) approved for this indication and has the potential for non-medical use. As such, any observed benefits of gabapentin should be balanced against its risks, and whether another alcohol use disorder medication that addresses “rebound anxiety” and is FDA approved like acamprosate is a better fit clinically.
The Insomnia Severity Index is a validated measure but does not include an assessment of how long the individual has been experiencing sleep problems – a 3-month duration is needed for DSM diagnosis of insomnia disorder. See Implications section above for more detail.
This study did not include formal statistical tests of mediation to determine a causal relationship between treatment with gabapentin, and changes in insomnia severity and alcohol use. Future studies will ideally test the gabapentin/insomnia/alcohol use relationship in a larger sample designed specifically to test whether gabapentin works by reducing sleep problems.
In the primary clinical trials this study was based on, all participants receiving gabapentin were dosed at 1200 mg/day. Future studies may explore the effects of gabapentin on insomnia and alcohol use at differing doses.
BOTTOM LINE
Findings from this study replicate previous studies showing a benefit of gabapentin on alcohol use in individuals seeking treatment for alcohol use disorder, while also showing this medication may support better sleep, especially in those with insomnia. Early indications are that the medication may not work, however, by decreasing sleep problems, though a larger trial that tests how the medication works is warranted.
For individuals and families seeking recovery: Gabapentin may help individuals seeking alcohol use disorder recovery reduce their drinking and get better sleep. While gabapentin is commonly prescribed for the treatment of alcohol use disorder, it should be noted that it is not Food and Drug Administration (FDA) approved for this condition and does have some potential for non-medical use – that is, using the medication for reasons or at doses that do not align with the doctor’s prescription.
For treatment professionals and treatment systems: Gabapentin may help individuals seeking alcohol use disorder recovery reduce their drinking and get better sleep. While gabapentin is commonly prescribed for the treatment of alcohol use disorder, it is not Food and Drug Administration (FDA) approved and does have some potential for non-medical/diverted use, necessitating consideration of the risk-benefit ratio when prescribing.
For scientists: Gabapentin may help individuals seeking alcohol use disorder recovery reduce their drinking and get better sleep. More research is needed to test for causality in the gabapentin/alcohol use/insomnia relationship. A larger trial powered specifically to test whether insomnia symptom reductions mediate the advantage of gabapentin vs. placebo on alcohol use outcomes. More work is also needed to tease out the dose relationship between gabapentin and sleep in this population.
For policy makers: Medications like gabapentin, as well as FDA-approved medications for alcohol use disorder that include naltrexone, acamprosate, and disulfiram, can be potent tools that support alcohol use disorder recovery. Policies that ensure individuals have access to medications for alcohol use disorder can help address the individual and societal harms associated with alcohol use disorder and other forms of harmful and hazardous drinking.
In this study, using data from a clinical trial of gabapentin (also known by the brand name “Neurontin”) for alcohol use disorder, the researchers examined whether gabapentin aids alcohol use disorder recovery by reducing sleep problems. They assessed the effect of gabapentin on insomnia, as well as how participants’ history of alcohol withdrawal affects the gabapentin/insomnia relationship.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of data from a randomized controlled trial showing gabapentin outperformed placebo for individuals alcohol use disorder and current or past alcohol withdrawal, to determine whether gabapentin’s effects on alcohol use help by decreasing sleep problems, as well as how participants’ history of alcohol withdrawal affect the insomnia/gabapentin relationship.
In the initial clinical trial, participants were randomized to receive either gabapentin (with dose gradually increased over 5 days to target 1200mg) or placebo. Gabapentin is FDA approved for seizures and neuropathic pain, but is sometimes prescribed off-label to address anxiety in those with substance use disorder – typically “rebound” anxiety that emerges after someone quits or cuts back on alcohol.
Participants were assessed on a range of outcome measures at treatment intake, and then at 2, 4, 6, 8, 10, 12, and 16 weeks. Primary outcome measures for this study included the Insomnia Severity Index (measuring sleep problems), the Alcohol Dependence Scale (measuring alcohol use disorder symptom severity), and the Alcohol Withdrawal Scale (measuring severity of alcohol withdrawal symptoms).
Drinking during treatment was also measured using a calendar-based self-report. The researchers explored gabapentin’s effects on sleep and drinking in the full study sample, and within a sub-sample of participants with moderate to severe insomnia symptoms based on Insomnia Severity Index scores at baseline.
The study sample of 90 individuals with alcohol use disorder was 77% male and 23% female, and on average, had symptoms consistent with moderate alcohol use disorder severity (4-5 out of 11), and subthreshold insomnia. Nearly half of the sample, however, had moderate to severe levels of clinically significant insomnia.
WHAT DID THIS STUDY FIND?
Gabapentin was associated with slightly better sleep outcomes
Over the course of the study, participants randomized to receive gabapentin reported slightly better sleep, with average Insomnia Severity Index scores of 5.5 versus 7.8 for controls. While these differences were statistically significant, indicating the differences were not likely to be due to chance, a difference of ~2 points on the Insomnia Severity Index, which ranges from 0-28.
Differences between groups on change in the Insomnia Severity Index scores from beginning to end of treatment were more notable, with participants receiving gabapentin showing a 61% improvement, and controls showing a 38% improvement.
When exploring between-group differences in sleep scores at each assessment time-point, groups were different on Insomnia Severity Index scores at weeks 10 and 12, but not at the other assessment time-points (see Figure below).
Participants with insomnia appeared to benefit more from gabapentin
When considering just the 43 participants with moderate to severe insomnia at study baseline, participants receiving gabapentin had an average Insomnia Severity Index score across the study of 6.1, while controls’ average score was 10.6 . Though this is still a relatively small effect , it suggests gabapentin may benefit individuals with alcohol use disorder and insomnia more than those with alcohol use disorder alone, at least in terms of producing sleep benefits.
In terms of change in insomnia severity scores from the beginning to the end of treatment, between group differences were similar to those seen in the full sample. Those receiving gabapentin showed a 66% improvement in Insomnia Severity Index scores, while controls showed a 42% improvement.
Notably, when exploring between-group differences in sleep scores at each assessment time-point, in the insomnia sub-sample, groups were different on Insomnia Severity Index scores at all time-points except the final assessment at week 16.
Gabapentin was most effective among those with insomnia but did not work by improving sleep problems as expected
Gabapentin was found to reduce within-treatment alcohol consumption regardless of participants’ baseline insomnia status; however, it had a greater impact on reducing within-treatment drinking among participants with higher baseline insomnia severity.
The researchers had previously shown that participants with greater baseline alcohol withdrawal severity benefited more from gabapentin in terms of drinking reductions than participants with lower baseline alcohol withdrawal severity. However, this relationship was not markedly affected when Insomnia Severity Index scores were considered.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Gabapentin may lead to marginal improvements in sleep problems in people seeking treatment for alcohol use disorder, and possibly larger improvements for those with clinically significant insomnia at baseline. However, the stronger benefit of gabapentin on alcohol use outcomes compared to placebo, among those with more alcohol withdrawal symptoms was not explained by reductions in insomnia symptoms. While gabapentin may help address both alcohol use and sleep, it does not appear to improve alcohol use by improving sleep. The sample size in this study was small, however, and formal mediation tests were not conducted – which examine how an intervention works (also sometimes referred to as potential “mechanisms”). Future research with larger samples designed specifically to test whether gabapentin improves alcohol use, in part, by addressing sleep problems is needed.
These findings come with other caveats. First, though insomnia severity was notably reduced from beginning to end of treatment in this study, such reductions are to be expected regardless of treatment type. Even without medications, insomnia tends to improve as people with alcohol use disorder stop or reduce their drinking. This was evidenced by notable reductions in insomnia scores from beginning to end of treatment in both the gabapentin and placebo conditions in this study.
Second, it is possible that the greater reductions insomnia scores in participants with clinically significant insomnia was at least in part a statistical function of these participants having more room for improvement (i.e., “regression to the mean”).
Third, it is also important to note that gabapentin has psychoactive effects and therefore participants may have known if they were prescribed gabapentin or placebo – if more people in the gabapentin group thought they were receiving the study medication it could be that their positive expectancies, rather than the medication’s effects, explained better sleep outcomes. In the initial trial, however, more side effects in the gabapentin group (an indication that someone is receiving the active medication) did not explain its positive effects on alcohol use. Thus it is unlikely – though still possible – that positive expectancies are accounting for observed medication benefit.
Fourth, a 2-point improvement in the gabapentin group was statistically significant but it is unclear whether a patient would actually feel they slept better at that level of improvement. Indeed, the direction is encouraging, but future work should examine whether this is sufficient magnitude to result in patients’ perceived change – e.g. feeling better rested.
Finally, though the Insomnia Severity Index is a validated measure and is a reasonable way to assess sleep problems in a clinical trial, it does not include an assessment of how long the individual has been experiencing sleep problems – a 3-month duration is needed for DSM diagnosis of insomnia disorder. Ideally future studies exploring gabapentin’s effects on sleep in this population will also include objective measures of sleep functioning like polysomnography.
Clinically, it is important to note that although gabapentin is commonly prescribed to treat alcohol use disorder, it is not Food and Drug Administration (FDA) approved for this indication and has the potential for non-medical use. As such, any observed benefits of gabapentin should be balanced against its risks, and whether another alcohol use disorder medication that addresses “rebound anxiety” and is FDA approved like acamprosate is a better fit clinically.
The Insomnia Severity Index is a validated measure but does not include an assessment of how long the individual has been experiencing sleep problems – a 3-month duration is needed for DSM diagnosis of insomnia disorder. See Implications section above for more detail.
This study did not include formal statistical tests of mediation to determine a causal relationship between treatment with gabapentin, and changes in insomnia severity and alcohol use. Future studies will ideally test the gabapentin/insomnia/alcohol use relationship in a larger sample designed specifically to test whether gabapentin works by reducing sleep problems.
In the primary clinical trials this study was based on, all participants receiving gabapentin were dosed at 1200 mg/day. Future studies may explore the effects of gabapentin on insomnia and alcohol use at differing doses.
BOTTOM LINE
Findings from this study replicate previous studies showing a benefit of gabapentin on alcohol use in individuals seeking treatment for alcohol use disorder, while also showing this medication may support better sleep, especially in those with insomnia. Early indications are that the medication may not work, however, by decreasing sleep problems, though a larger trial that tests how the medication works is warranted.
For individuals and families seeking recovery: Gabapentin may help individuals seeking alcohol use disorder recovery reduce their drinking and get better sleep. While gabapentin is commonly prescribed for the treatment of alcohol use disorder, it should be noted that it is not Food and Drug Administration (FDA) approved for this condition and does have some potential for non-medical use – that is, using the medication for reasons or at doses that do not align with the doctor’s prescription.
For treatment professionals and treatment systems: Gabapentin may help individuals seeking alcohol use disorder recovery reduce their drinking and get better sleep. While gabapentin is commonly prescribed for the treatment of alcohol use disorder, it is not Food and Drug Administration (FDA) approved and does have some potential for non-medical/diverted use, necessitating consideration of the risk-benefit ratio when prescribing.
For scientists: Gabapentin may help individuals seeking alcohol use disorder recovery reduce their drinking and get better sleep. More research is needed to test for causality in the gabapentin/alcohol use/insomnia relationship. A larger trial powered specifically to test whether insomnia symptom reductions mediate the advantage of gabapentin vs. placebo on alcohol use outcomes. More work is also needed to tease out the dose relationship between gabapentin and sleep in this population.
For policy makers: Medications like gabapentin, as well as FDA-approved medications for alcohol use disorder that include naltrexone, acamprosate, and disulfiram, can be potent tools that support alcohol use disorder recovery. Policies that ensure individuals have access to medications for alcohol use disorder can help address the individual and societal harms associated with alcohol use disorder and other forms of harmful and hazardous drinking.
In this study, using data from a clinical trial of gabapentin (also known by the brand name “Neurontin”) for alcohol use disorder, the researchers examined whether gabapentin aids alcohol use disorder recovery by reducing sleep problems. They assessed the effect of gabapentin on insomnia, as well as how participants’ history of alcohol withdrawal affects the gabapentin/insomnia relationship.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of data from a randomized controlled trial showing gabapentin outperformed placebo for individuals alcohol use disorder and current or past alcohol withdrawal, to determine whether gabapentin’s effects on alcohol use help by decreasing sleep problems, as well as how participants’ history of alcohol withdrawal affect the insomnia/gabapentin relationship.
In the initial clinical trial, participants were randomized to receive either gabapentin (with dose gradually increased over 5 days to target 1200mg) or placebo. Gabapentin is FDA approved for seizures and neuropathic pain, but is sometimes prescribed off-label to address anxiety in those with substance use disorder – typically “rebound” anxiety that emerges after someone quits or cuts back on alcohol.
Participants were assessed on a range of outcome measures at treatment intake, and then at 2, 4, 6, 8, 10, 12, and 16 weeks. Primary outcome measures for this study included the Insomnia Severity Index (measuring sleep problems), the Alcohol Dependence Scale (measuring alcohol use disorder symptom severity), and the Alcohol Withdrawal Scale (measuring severity of alcohol withdrawal symptoms).
Drinking during treatment was also measured using a calendar-based self-report. The researchers explored gabapentin’s effects on sleep and drinking in the full study sample, and within a sub-sample of participants with moderate to severe insomnia symptoms based on Insomnia Severity Index scores at baseline.
The study sample of 90 individuals with alcohol use disorder was 77% male and 23% female, and on average, had symptoms consistent with moderate alcohol use disorder severity (4-5 out of 11), and subthreshold insomnia. Nearly half of the sample, however, had moderate to severe levels of clinically significant insomnia.
WHAT DID THIS STUDY FIND?
Gabapentin was associated with slightly better sleep outcomes
Over the course of the study, participants randomized to receive gabapentin reported slightly better sleep, with average Insomnia Severity Index scores of 5.5 versus 7.8 for controls. While these differences were statistically significant, indicating the differences were not likely to be due to chance, a difference of ~2 points on the Insomnia Severity Index, which ranges from 0-28.
Differences between groups on change in the Insomnia Severity Index scores from beginning to end of treatment were more notable, with participants receiving gabapentin showing a 61% improvement, and controls showing a 38% improvement.
When exploring between-group differences in sleep scores at each assessment time-point, groups were different on Insomnia Severity Index scores at weeks 10 and 12, but not at the other assessment time-points (see Figure below).
Participants with insomnia appeared to benefit more from gabapentin
When considering just the 43 participants with moderate to severe insomnia at study baseline, participants receiving gabapentin had an average Insomnia Severity Index score across the study of 6.1, while controls’ average score was 10.6 . Though this is still a relatively small effect , it suggests gabapentin may benefit individuals with alcohol use disorder and insomnia more than those with alcohol use disorder alone, at least in terms of producing sleep benefits.
In terms of change in insomnia severity scores from the beginning to the end of treatment, between group differences were similar to those seen in the full sample. Those receiving gabapentin showed a 66% improvement in Insomnia Severity Index scores, while controls showed a 42% improvement.
Notably, when exploring between-group differences in sleep scores at each assessment time-point, in the insomnia sub-sample, groups were different on Insomnia Severity Index scores at all time-points except the final assessment at week 16.
Gabapentin was most effective among those with insomnia but did not work by improving sleep problems as expected
Gabapentin was found to reduce within-treatment alcohol consumption regardless of participants’ baseline insomnia status; however, it had a greater impact on reducing within-treatment drinking among participants with higher baseline insomnia severity.
The researchers had previously shown that participants with greater baseline alcohol withdrawal severity benefited more from gabapentin in terms of drinking reductions than participants with lower baseline alcohol withdrawal severity. However, this relationship was not markedly affected when Insomnia Severity Index scores were considered.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Gabapentin may lead to marginal improvements in sleep problems in people seeking treatment for alcohol use disorder, and possibly larger improvements for those with clinically significant insomnia at baseline. However, the stronger benefit of gabapentin on alcohol use outcomes compared to placebo, among those with more alcohol withdrawal symptoms was not explained by reductions in insomnia symptoms. While gabapentin may help address both alcohol use and sleep, it does not appear to improve alcohol use by improving sleep. The sample size in this study was small, however, and formal mediation tests were not conducted – which examine how an intervention works (also sometimes referred to as potential “mechanisms”). Future research with larger samples designed specifically to test whether gabapentin improves alcohol use, in part, by addressing sleep problems is needed.
These findings come with other caveats. First, though insomnia severity was notably reduced from beginning to end of treatment in this study, such reductions are to be expected regardless of treatment type. Even without medications, insomnia tends to improve as people with alcohol use disorder stop or reduce their drinking. This was evidenced by notable reductions in insomnia scores from beginning to end of treatment in both the gabapentin and placebo conditions in this study.
Second, it is possible that the greater reductions insomnia scores in participants with clinically significant insomnia was at least in part a statistical function of these participants having more room for improvement (i.e., “regression to the mean”).
Third, it is also important to note that gabapentin has psychoactive effects and therefore participants may have known if they were prescribed gabapentin or placebo – if more people in the gabapentin group thought they were receiving the study medication it could be that their positive expectancies, rather than the medication’s effects, explained better sleep outcomes. In the initial trial, however, more side effects in the gabapentin group (an indication that someone is receiving the active medication) did not explain its positive effects on alcohol use. Thus it is unlikely – though still possible – that positive expectancies are accounting for observed medication benefit.
Fourth, a 2-point improvement in the gabapentin group was statistically significant but it is unclear whether a patient would actually feel they slept better at that level of improvement. Indeed, the direction is encouraging, but future work should examine whether this is sufficient magnitude to result in patients’ perceived change – e.g. feeling better rested.
Finally, though the Insomnia Severity Index is a validated measure and is a reasonable way to assess sleep problems in a clinical trial, it does not include an assessment of how long the individual has been experiencing sleep problems – a 3-month duration is needed for DSM diagnosis of insomnia disorder. Ideally future studies exploring gabapentin’s effects on sleep in this population will also include objective measures of sleep functioning like polysomnography.
Clinically, it is important to note that although gabapentin is commonly prescribed to treat alcohol use disorder, it is not Food and Drug Administration (FDA) approved for this indication and has the potential for non-medical use. As such, any observed benefits of gabapentin should be balanced against its risks, and whether another alcohol use disorder medication that addresses “rebound anxiety” and is FDA approved like acamprosate is a better fit clinically.
The Insomnia Severity Index is a validated measure but does not include an assessment of how long the individual has been experiencing sleep problems – a 3-month duration is needed for DSM diagnosis of insomnia disorder. See Implications section above for more detail.
This study did not include formal statistical tests of mediation to determine a causal relationship between treatment with gabapentin, and changes in insomnia severity and alcohol use. Future studies will ideally test the gabapentin/insomnia/alcohol use relationship in a larger sample designed specifically to test whether gabapentin works by reducing sleep problems.
In the primary clinical trials this study was based on, all participants receiving gabapentin were dosed at 1200 mg/day. Future studies may explore the effects of gabapentin on insomnia and alcohol use at differing doses.
BOTTOM LINE
Findings from this study replicate previous studies showing a benefit of gabapentin on alcohol use in individuals seeking treatment for alcohol use disorder, while also showing this medication may support better sleep, especially in those with insomnia. Early indications are that the medication may not work, however, by decreasing sleep problems, though a larger trial that tests how the medication works is warranted.
For individuals and families seeking recovery: Gabapentin may help individuals seeking alcohol use disorder recovery reduce their drinking and get better sleep. While gabapentin is commonly prescribed for the treatment of alcohol use disorder, it should be noted that it is not Food and Drug Administration (FDA) approved for this condition and does have some potential for non-medical use – that is, using the medication for reasons or at doses that do not align with the doctor’s prescription.
For treatment professionals and treatment systems: Gabapentin may help individuals seeking alcohol use disorder recovery reduce their drinking and get better sleep. While gabapentin is commonly prescribed for the treatment of alcohol use disorder, it is not Food and Drug Administration (FDA) approved and does have some potential for non-medical/diverted use, necessitating consideration of the risk-benefit ratio when prescribing.
For scientists: Gabapentin may help individuals seeking alcohol use disorder recovery reduce their drinking and get better sleep. More research is needed to test for causality in the gabapentin/alcohol use/insomnia relationship. A larger trial powered specifically to test whether insomnia symptom reductions mediate the advantage of gabapentin vs. placebo on alcohol use outcomes. More work is also needed to tease out the dose relationship between gabapentin and sleep in this population.
For policy makers: Medications like gabapentin, as well as FDA-approved medications for alcohol use disorder that include naltrexone, acamprosate, and disulfiram, can be potent tools that support alcohol use disorder recovery. Policies that ensure individuals have access to medications for alcohol use disorder can help address the individual and societal harms associated with alcohol use disorder and other forms of harmful and hazardous drinking.
 Gabapentin is a commonly prescribed medication for alcohol use disorder, though it is not FDA approved to treat the disorder and its therapeutic mechanisms of action remain unclear. Heavy alcohol use is known to radically affect the nature, duration, and quality of sleep. Therefore, this study examined how gabapentin affected sleep in people seeking alcohol use disorder treatment, with the idea that this medication may be indirectly improving alcohol use outcomes by improving sleep.
Gabapentin is a commonly prescribed medication for alcohol use disorder, though it is not FDA approved to treat the disorder and its therapeutic mechanisms of action remain unclear. Heavy alcohol use is known to radically affect the nature, duration, and quality of sleep. Therefore, this study examined how gabapentin affected sleep in people seeking alcohol use disorder treatment, with the idea that this medication may be indirectly improving alcohol use outcomes by improving sleep.