“One-size-fits some”: Can tailored cognitive-behavioral therapy for alcohol use disorder improve on the standard version
Cognitive-behavioral therapy (CBT) is widely used, but not everybody benefits who receives it. This study tested whether a highly personalized CBT approach – tailored to individuals’ real-time experiences with alcohol use and coping dynamically over time – leads to better outcomes than standard CBT or case management. Researchers also went one step further to investigate whether improvements in coping skills explained why the tailored approach may have been helpful.
Cognitive-behavioral therapy (CBT) is one of the most widely used treatments for alcohol use disorder, thought to work by helping individuals develop coping skills to manage cravings and high-risk drinking situations that may lead to relapse. Overall, research supports the utility of CBT-based approaches, yet its efficacy varies across individuals. One potential limitation is that standard CBT as tested in clinical trials follows a standardized, one-size-fits-all approach, which may not fully address the unique coping challenges each person faces. While many therapists in treatment programs and in private practice individualize care to meet the needs of their patients, whether this approach actually improves upon the structured manuals is an empirical question.
Understanding how treatments work is also important to scaling them so that, if effective, providers can hone in on the most critical aspects of the approach. A key assumption of coping skills training is that deficits in coping ability contribute to relapse. However, research on whether improvements in coping skills actually mediate treatment success has yielded mixed results. One reason for this may be the lack of individualized assessment – most standard CBT trials do not systematically incorporate a person’s specific coping deficits into the treatment approach. As a result, individuals may receive training in coping strategies that are not as relevant to their particular challenges, potentially reducing treatment efficacy. Additionally, retrospective self-reports of coping behaviors may be unreliable, making it difficult to tailor therapy in real-time.
To address these limitations, this study examined an individualized assessment and treatment program – a novel, tailored CBT approach that personalizes coping skills training based on real-time ecological momentary assessment data. This study tested whether tailored CBT improves drinking outcomes in individuals with moderate-to-severe alcohol use disorder compared to standard CBT and a case management control condition. The researchers also examined whether the situational use of coping strategies mediated the effects of tailored CBT on drinking outcomes.
HOW WAS THIS STUDY CONDUCTED?
This study was a randomized controlled trial evaluating the efficacy of an individually tailored CBT program for alcohol use disorder compared to standard CBT or a case management control condition. This study enrolled 173 adults meeting DSM-5 diagnostic criteria for moderate-to-severe alcohol use disorder recruited from radio and newspaper advertisements, social service agencies, and detoxification centers. The sample was predominantly White (93%), just over half were male (56%), and was around 50 years old on average. Participants were randomly assigned to one of three 12-session, manualized treatment conditions, delivered over 14 weeks:
1) Tailored CBT (n = 59): A highly personalized CBT program that adapted coping skills training to each participant’s real-time needs. Therapists used experience sampling data (self-reported desire to drink, high-risk situations, and coping behaviors; see below for more detail) collected from participants 4 times daily in the 2 weeks preceding treatment, during treatment (weeks 4, 6, and 10), and post-treatment (weeks 15 and 16). This data was summarized by a research assistant and provided to the therapist for use in tailoring individualized coping strategies. Therapy sessions focused on reviewing specific drinking episodes, identifying specific coping deficits, and developing strategies to manage future high-risk situations.
2) Standard CBT (n = 57): A standard, manualized CBT program that provided fixed coping skills training to address interpersonal (e.g., social pressure, conflict with others) and intrapersonal (e.g., cravings, negative emotions) triggers for drinking. The program followed structured manuals adapted from prior clinical trials and included didactic presentations, behavioral rehearsal, and homework assignments. Participants could choose from a set of elective topics (e.g., scheduling pleasant activities).
3) Case management control (n = 57): A supportive intervention without structured coping skills training. Therapists helped patients identify problems in daily living (e.g., housing, employment, family issues), including drinking, and discussed personal and community resources (e.g., Alcoholics Anonymous, psychiatric referrals). The focus was on problem-solving and support rather than direct coping skills training.
To capture real-time coping behaviors and alcohol use, the study employed an ecological momentary assessment method called experience sampling using phone call prompts 4 times daily at random intervals before, during, and after treatment. During each call, participants verbally reported current desire to drink, current situational details (e.g., location, activity), their alcohol consumption in the previous 30 minutes, and coping behaviors, if any, used to resist drinking. Each 5- to 7-minute call was audio-recorded, and research assistants coded participants’ coping strategies used (e.g., active coping, avoidance). Ecological momentary assessment data were collected before treatment (weeks 1 and 2 after baseline, but before treatment start), during treatment (in weeks 4, 6, and 10), post-treatment (in weeks 15 and 16), and for a 1-week period during 9 and 15-month follow-up periods.
In-person survey assessments were administered at baseline and every 3 months for 21 months. Primary outcomes were proportion of heavy drinking days (3+ drinks for women, 4+ drinks for men) and proportion of abstinent days reported at each 90-day period measured using the Form-90, based on the timeline follow-back method. Secondary outcomes included coping strategies (Coping Strategies Scale), alcohol abstinence self-efficacy (Alcohol Abstinence Self-Efficacy Scale), and negative consequences of drinking (Drinker Inventory of Consequences). Self-reports of alcohol and drug use were verified with breathalyzer readings at every treatment session and urine drug tests at baseline and follow-up assessments.
Statistical analyses tested whether there were group differences on percent days abstinent from alcohol and on percent days with heavy drinking over time. Analyses also examined whether coping skills explained any potential advantage for the tailored CBT on drinking outcomes compared to standard CBT and case management. The study employed an intent-to-treat approach, meaning all participants who were randomized into on of the 3 treatment conditions were included in the final analysis regardless of whether and how much treatment they received.
WHAT DID THIS STUDY FIND?
Tailored CBT led to greater reductions in drinking than standard CBT or case management
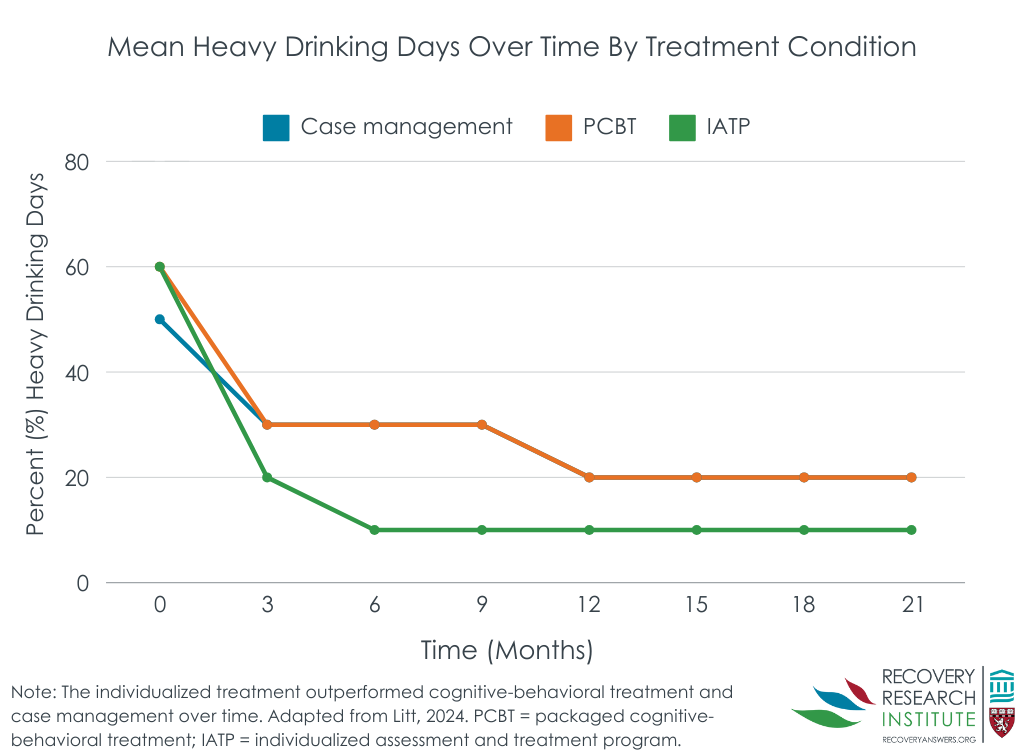
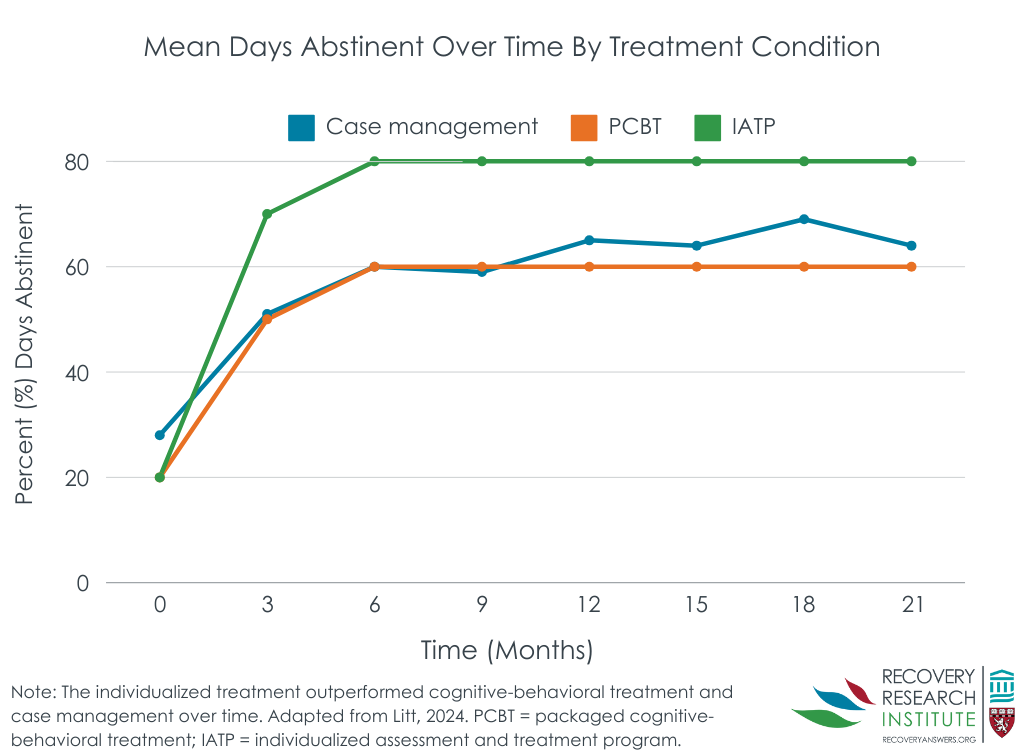
Participants who received tailored CBT reported significantly fewer heavy drinking days and a higher proportion of abstinent days compared both to those who received standard CBT and case management (see Figure below). These drinking reductions within participants who received tailored CBT were sustained up to 21 months post-treatment. Notably, standard CBT did not significantly outperform case management in reducing heavy drinking days or increasing percent days abstinent.
Coping skills and self-efficacy mediated treatment effects
Participants in the tailored CBT condition showed greater improvements in active coping strategies (e.g., seeking social support) and higher abstinence self-efficacy compared to those in standard CBT or case management conditions. Mediation analyses revealed that increases in active coping skills at least partially explained the beneficial effects of tailored CBT on drinking outcomes. Additionally, enhancements in abstinence self-efficacy also mediated the relationship between tailored CBT and long-term drinking reductions.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Tailored CBT – personalized to individuals’ coping strengths and deficits – outperformed standard CBT and case management in reducing heavy drinking days and increasing alcohol abstinent days. These effects were partially explained by improvements in active coping strategies (e.g., seeking social support, problem-solving) and abstinence self-efficacy, underscoring the critical role of coping skills in sustained recovery. Notably, the benefits of tailored CBT on drinking outcomes persisted up to 21 months post-treatment, highlighting its long-term potential to help individuals with moderate-to-severe alcohol use disorder. Unexpectedly, standard CBT did not do any better than standard case management. As study authors note, up to a point, individuals increase coping skills (e.g., seeking social support) even in the absence of specific skills training. Overall, these findings align with broader research on relapse prevention, emphasizing the critical role of coping skills as a key mechanism of behavior change in alcohol use disorder treatment. Specifically, findings suggest that dynamically strengthening active coping strategies over time equips individuals to navigate changing high-risk situations, manage cravings, and seek support – ultimately reducing relapse risk.
Unlike standard CBT, tailored CBT dynamically adjusts to each patient’s coping deficits in real-time, potentially offering a more responsive and individualized approach to treatment. Such an approach may resemble the way CBT is delivered in “real-world” settings rather than clinical trials. The integration of real-time “experience sampling” methodologies, such as ecological momentary assessment, does not, however, resemble CBT as typically delivered. It is possible that these ongoing, daily check-ins during several weeks of treatment and follow-up helped remind participants about the value of coping strategies, and potentially helping them deploy better coping skills, accounting for some of the individualized approach’s benefit. Therefore, these check-ins are best understood as part of the individualized approach. Indeed, this approach could both enhance treatment precision by allowing clinicians to track real-time coping experiences and deliver adaptive, data-driven interventions and also function as skill reminders for patients. Regarding the former, this approach aligns with research on just-in-time adaptive interventions, which leverage real-time data to provide tailored support at critical moments – such as when individuals experience cravings, stress, or exposure to high-risk situations. Although just-in-time adaptive interventions hold promise for improving engagement and long-term recovery outcomes, evidence for their effectiveness in alcohol use disorder treatment remains limited. While more research is needed, integrating experience sampling methodologies and just-in-time adaptive interventions represents a promising step toward making alcohol use disorder treatment more personalized and responsive.
Moreover, advancements in digital health tools, including mobile apps, wearable biosensors, and artificial intelligence-powered interventions, offer new opportunities to scale personalized treatment and could make tailored interventions more widely available beyond standard in-person therapy. However, additional research is needed to determine the most effective ways to implement these solutions, ensuring they enhance patient engagement and outcomes. Moreover, future studies could compare tailored CBT with other empirically supported treatment models, such as motivational enhancement therapy, 12-step facilitation, and pharmacotherapy, to identify the most effective strategies for diverse populations. Understanding which individuals benefit most from tailored CBT versus other approaches could further refine personalized treatment models for alcohol use disorder.
The study sample was relatively homogenous, consisting of primarily White, middle-aged men recruited from a single metropolitan area. This limits generalizability of the findings to more diverse populations and different cultural and healthcare settings.
Completion rates for ecological momentary assessments declined over time, with only 42% of prompts completed at month 15. This missing data may introduce measurement bias (e.g., where individuals doing better are more likely to respond to prompts), potentially affecting the accuracy of findings regarding real-time coping behaviors.
While breathalyzer and urine tests were used during treatment to verify alcohol and drug use, long-term drinking outcomes relied on self-report data. As a result, findings may be subject to recall bias or social desirability bias, potentially overestimating treatment effects.
BOTTOM LINE
This study found that tailored CBT – personalized to individuals’ real-time coping experiences – significantly improved drinking outcomes compared to standard CBT or case management. Use of active coping skills like problem solving explained the tailored approach’s advantage, highlighting the value of personalized interventions that address individual coping deficits. Rather than relying on a standardized one-size-fits all approach, assessing for, and tailoring treatment to, each person’s unique challenges dynamically over time may enhance the long-term effectiveness of alcohol use disorder treatment.
For individuals and families seeking recovery: Personalized therapy approaches, such as tailored CBT, may provide more effective long-term solutions than one-size-fits all treatments. By identifying and strengthening an individual’s unique coping skills, dynamically tailored CBT helps people navigate personal challenges more effectively and develop strategies suited to their specific needs over time. When seeking treatment, individuals and families may benefit from exploring options that assess real-time drinking triggers and coping responses.
For treatment professionals and treatment systems: Clinicians could consider adopting personalized treatment approaches that tailor coping skills training based on real-time assessments. Integrating experience sampling methods, such as ecological momentary assessment, into therapy might offer valuable insights into patients’ high-risk situations and coping behaviors. This approach enables more dynamically responsive and adaptive interventions, and could improve patient engagement and outcomes. Similarly, treatment systems could invest in infrastructure – such as technological capabilities and clinician training programs – to support the effective implementation of these personalized approaches.
For scientists: This study underscores the critical role of active coping skills as a mediator in alcohol use disorder treatment, emphasizing the importance of personalized, dynamic and adaptive interventions. Interestingly, coping skills more generally did not mediate the benefit conferred by tailored CBT. Future research is needed to explore how tailored approaches, incorporating experience sampling and real-time coping assessments, can be applied across different substance use disorders. Additionally, further studies are needed to determine which populations benefit most from tailored CBT compared to other treatment approaches.
For policy makers: Investing in dynamic, adaptive, data-driven personalized interventions could enhance long-term treatment and recovery outcomes for alcohol use disorder. Supporting research and the implementation of real-time assessment tools, such as ecological momentary assessment and just-in-time adaptive interventions, may improve treatment precision, patient engagement, and overall outcomes. Additionally, funding initiatives to integrate personalized approaches into clinical practice – such as clinician training programs and the development of digital health infrastructure – could expand access to more effective, tailored care. This, in turn, could help reduce the societal burden of alcohol use disorder.
Cognitive-behavioral therapy (CBT) is one of the most widely used treatments for alcohol use disorder, thought to work by helping individuals develop coping skills to manage cravings and high-risk drinking situations that may lead to relapse. Overall, research supports the utility of CBT-based approaches, yet its efficacy varies across individuals. One potential limitation is that standard CBT as tested in clinical trials follows a standardized, one-size-fits-all approach, which may not fully address the unique coping challenges each person faces. While many therapists in treatment programs and in private practice individualize care to meet the needs of their patients, whether this approach actually improves upon the structured manuals is an empirical question.
Understanding how treatments work is also important to scaling them so that, if effective, providers can hone in on the most critical aspects of the approach. A key assumption of coping skills training is that deficits in coping ability contribute to relapse. However, research on whether improvements in coping skills actually mediate treatment success has yielded mixed results. One reason for this may be the lack of individualized assessment – most standard CBT trials do not systematically incorporate a person’s specific coping deficits into the treatment approach. As a result, individuals may receive training in coping strategies that are not as relevant to their particular challenges, potentially reducing treatment efficacy. Additionally, retrospective self-reports of coping behaviors may be unreliable, making it difficult to tailor therapy in real-time.
To address these limitations, this study examined an individualized assessment and treatment program – a novel, tailored CBT approach that personalizes coping skills training based on real-time ecological momentary assessment data. This study tested whether tailored CBT improves drinking outcomes in individuals with moderate-to-severe alcohol use disorder compared to standard CBT and a case management control condition. The researchers also examined whether the situational use of coping strategies mediated the effects of tailored CBT on drinking outcomes.
HOW WAS THIS STUDY CONDUCTED?
This study was a randomized controlled trial evaluating the efficacy of an individually tailored CBT program for alcohol use disorder compared to standard CBT or a case management control condition. This study enrolled 173 adults meeting DSM-5 diagnostic criteria for moderate-to-severe alcohol use disorder recruited from radio and newspaper advertisements, social service agencies, and detoxification centers. The sample was predominantly White (93%), just over half were male (56%), and was around 50 years old on average. Participants were randomly assigned to one of three 12-session, manualized treatment conditions, delivered over 14 weeks:
1) Tailored CBT (n = 59): A highly personalized CBT program that adapted coping skills training to each participant’s real-time needs. Therapists used experience sampling data (self-reported desire to drink, high-risk situations, and coping behaviors; see below for more detail) collected from participants 4 times daily in the 2 weeks preceding treatment, during treatment (weeks 4, 6, and 10), and post-treatment (weeks 15 and 16). This data was summarized by a research assistant and provided to the therapist for use in tailoring individualized coping strategies. Therapy sessions focused on reviewing specific drinking episodes, identifying specific coping deficits, and developing strategies to manage future high-risk situations.
2) Standard CBT (n = 57): A standard, manualized CBT program that provided fixed coping skills training to address interpersonal (e.g., social pressure, conflict with others) and intrapersonal (e.g., cravings, negative emotions) triggers for drinking. The program followed structured manuals adapted from prior clinical trials and included didactic presentations, behavioral rehearsal, and homework assignments. Participants could choose from a set of elective topics (e.g., scheduling pleasant activities).
3) Case management control (n = 57): A supportive intervention without structured coping skills training. Therapists helped patients identify problems in daily living (e.g., housing, employment, family issues), including drinking, and discussed personal and community resources (e.g., Alcoholics Anonymous, psychiatric referrals). The focus was on problem-solving and support rather than direct coping skills training.
To capture real-time coping behaviors and alcohol use, the study employed an ecological momentary assessment method called experience sampling using phone call prompts 4 times daily at random intervals before, during, and after treatment. During each call, participants verbally reported current desire to drink, current situational details (e.g., location, activity), their alcohol consumption in the previous 30 minutes, and coping behaviors, if any, used to resist drinking. Each 5- to 7-minute call was audio-recorded, and research assistants coded participants’ coping strategies used (e.g., active coping, avoidance). Ecological momentary assessment data were collected before treatment (weeks 1 and 2 after baseline, but before treatment start), during treatment (in weeks 4, 6, and 10), post-treatment (in weeks 15 and 16), and for a 1-week period during 9 and 15-month follow-up periods.
In-person survey assessments were administered at baseline and every 3 months for 21 months. Primary outcomes were proportion of heavy drinking days (3+ drinks for women, 4+ drinks for men) and proportion of abstinent days reported at each 90-day period measured using the Form-90, based on the timeline follow-back method. Secondary outcomes included coping strategies (Coping Strategies Scale), alcohol abstinence self-efficacy (Alcohol Abstinence Self-Efficacy Scale), and negative consequences of drinking (Drinker Inventory of Consequences). Self-reports of alcohol and drug use were verified with breathalyzer readings at every treatment session and urine drug tests at baseline and follow-up assessments.
Statistical analyses tested whether there were group differences on percent days abstinent from alcohol and on percent days with heavy drinking over time. Analyses also examined whether coping skills explained any potential advantage for the tailored CBT on drinking outcomes compared to standard CBT and case management. The study employed an intent-to-treat approach, meaning all participants who were randomized into on of the 3 treatment conditions were included in the final analysis regardless of whether and how much treatment they received.
WHAT DID THIS STUDY FIND?
Tailored CBT led to greater reductions in drinking than standard CBT or case management
Participants who received tailored CBT reported significantly fewer heavy drinking days and a higher proportion of abstinent days compared both to those who received standard CBT and case management (see Figure below). These drinking reductions within participants who received tailored CBT were sustained up to 21 months post-treatment. Notably, standard CBT did not significantly outperform case management in reducing heavy drinking days or increasing percent days abstinent.
Coping skills and self-efficacy mediated treatment effects
Participants in the tailored CBT condition showed greater improvements in active coping strategies (e.g., seeking social support) and higher abstinence self-efficacy compared to those in standard CBT or case management conditions. Mediation analyses revealed that increases in active coping skills at least partially explained the beneficial effects of tailored CBT on drinking outcomes. Additionally, enhancements in abstinence self-efficacy also mediated the relationship between tailored CBT and long-term drinking reductions.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Tailored CBT – personalized to individuals’ coping strengths and deficits – outperformed standard CBT and case management in reducing heavy drinking days and increasing alcohol abstinent days. These effects were partially explained by improvements in active coping strategies (e.g., seeking social support, problem-solving) and abstinence self-efficacy, underscoring the critical role of coping skills in sustained recovery. Notably, the benefits of tailored CBT on drinking outcomes persisted up to 21 months post-treatment, highlighting its long-term potential to help individuals with moderate-to-severe alcohol use disorder. Unexpectedly, standard CBT did not do any better than standard case management. As study authors note, up to a point, individuals increase coping skills (e.g., seeking social support) even in the absence of specific skills training. Overall, these findings align with broader research on relapse prevention, emphasizing the critical role of coping skills as a key mechanism of behavior change in alcohol use disorder treatment. Specifically, findings suggest that dynamically strengthening active coping strategies over time equips individuals to navigate changing high-risk situations, manage cravings, and seek support – ultimately reducing relapse risk.
Unlike standard CBT, tailored CBT dynamically adjusts to each patient’s coping deficits in real-time, potentially offering a more responsive and individualized approach to treatment. Such an approach may resemble the way CBT is delivered in “real-world” settings rather than clinical trials. The integration of real-time “experience sampling” methodologies, such as ecological momentary assessment, does not, however, resemble CBT as typically delivered. It is possible that these ongoing, daily check-ins during several weeks of treatment and follow-up helped remind participants about the value of coping strategies, and potentially helping them deploy better coping skills, accounting for some of the individualized approach’s benefit. Therefore, these check-ins are best understood as part of the individualized approach. Indeed, this approach could both enhance treatment precision by allowing clinicians to track real-time coping experiences and deliver adaptive, data-driven interventions and also function as skill reminders for patients. Regarding the former, this approach aligns with research on just-in-time adaptive interventions, which leverage real-time data to provide tailored support at critical moments – such as when individuals experience cravings, stress, or exposure to high-risk situations. Although just-in-time adaptive interventions hold promise for improving engagement and long-term recovery outcomes, evidence for their effectiveness in alcohol use disorder treatment remains limited. While more research is needed, integrating experience sampling methodologies and just-in-time adaptive interventions represents a promising step toward making alcohol use disorder treatment more personalized and responsive.
Moreover, advancements in digital health tools, including mobile apps, wearable biosensors, and artificial intelligence-powered interventions, offer new opportunities to scale personalized treatment and could make tailored interventions more widely available beyond standard in-person therapy. However, additional research is needed to determine the most effective ways to implement these solutions, ensuring they enhance patient engagement and outcomes. Moreover, future studies could compare tailored CBT with other empirically supported treatment models, such as motivational enhancement therapy, 12-step facilitation, and pharmacotherapy, to identify the most effective strategies for diverse populations. Understanding which individuals benefit most from tailored CBT versus other approaches could further refine personalized treatment models for alcohol use disorder.
The study sample was relatively homogenous, consisting of primarily White, middle-aged men recruited from a single metropolitan area. This limits generalizability of the findings to more diverse populations and different cultural and healthcare settings.
Completion rates for ecological momentary assessments declined over time, with only 42% of prompts completed at month 15. This missing data may introduce measurement bias (e.g., where individuals doing better are more likely to respond to prompts), potentially affecting the accuracy of findings regarding real-time coping behaviors.
While breathalyzer and urine tests were used during treatment to verify alcohol and drug use, long-term drinking outcomes relied on self-report data. As a result, findings may be subject to recall bias or social desirability bias, potentially overestimating treatment effects.
BOTTOM LINE
This study found that tailored CBT – personalized to individuals’ real-time coping experiences – significantly improved drinking outcomes compared to standard CBT or case management. Use of active coping skills like problem solving explained the tailored approach’s advantage, highlighting the value of personalized interventions that address individual coping deficits. Rather than relying on a standardized one-size-fits all approach, assessing for, and tailoring treatment to, each person’s unique challenges dynamically over time may enhance the long-term effectiveness of alcohol use disorder treatment.
For individuals and families seeking recovery: Personalized therapy approaches, such as tailored CBT, may provide more effective long-term solutions than one-size-fits all treatments. By identifying and strengthening an individual’s unique coping skills, dynamically tailored CBT helps people navigate personal challenges more effectively and develop strategies suited to their specific needs over time. When seeking treatment, individuals and families may benefit from exploring options that assess real-time drinking triggers and coping responses.
For treatment professionals and treatment systems: Clinicians could consider adopting personalized treatment approaches that tailor coping skills training based on real-time assessments. Integrating experience sampling methods, such as ecological momentary assessment, into therapy might offer valuable insights into patients’ high-risk situations and coping behaviors. This approach enables more dynamically responsive and adaptive interventions, and could improve patient engagement and outcomes. Similarly, treatment systems could invest in infrastructure – such as technological capabilities and clinician training programs – to support the effective implementation of these personalized approaches.
For scientists: This study underscores the critical role of active coping skills as a mediator in alcohol use disorder treatment, emphasizing the importance of personalized, dynamic and adaptive interventions. Interestingly, coping skills more generally did not mediate the benefit conferred by tailored CBT. Future research is needed to explore how tailored approaches, incorporating experience sampling and real-time coping assessments, can be applied across different substance use disorders. Additionally, further studies are needed to determine which populations benefit most from tailored CBT compared to other treatment approaches.
For policy makers: Investing in dynamic, adaptive, data-driven personalized interventions could enhance long-term treatment and recovery outcomes for alcohol use disorder. Supporting research and the implementation of real-time assessment tools, such as ecological momentary assessment and just-in-time adaptive interventions, may improve treatment precision, patient engagement, and overall outcomes. Additionally, funding initiatives to integrate personalized approaches into clinical practice – such as clinician training programs and the development of digital health infrastructure – could expand access to more effective, tailored care. This, in turn, could help reduce the societal burden of alcohol use disorder.
Cognitive-behavioral therapy (CBT) is one of the most widely used treatments for alcohol use disorder, thought to work by helping individuals develop coping skills to manage cravings and high-risk drinking situations that may lead to relapse. Overall, research supports the utility of CBT-based approaches, yet its efficacy varies across individuals. One potential limitation is that standard CBT as tested in clinical trials follows a standardized, one-size-fits-all approach, which may not fully address the unique coping challenges each person faces. While many therapists in treatment programs and in private practice individualize care to meet the needs of their patients, whether this approach actually improves upon the structured manuals is an empirical question.
Understanding how treatments work is also important to scaling them so that, if effective, providers can hone in on the most critical aspects of the approach. A key assumption of coping skills training is that deficits in coping ability contribute to relapse. However, research on whether improvements in coping skills actually mediate treatment success has yielded mixed results. One reason for this may be the lack of individualized assessment – most standard CBT trials do not systematically incorporate a person’s specific coping deficits into the treatment approach. As a result, individuals may receive training in coping strategies that are not as relevant to their particular challenges, potentially reducing treatment efficacy. Additionally, retrospective self-reports of coping behaviors may be unreliable, making it difficult to tailor therapy in real-time.
To address these limitations, this study examined an individualized assessment and treatment program – a novel, tailored CBT approach that personalizes coping skills training based on real-time ecological momentary assessment data. This study tested whether tailored CBT improves drinking outcomes in individuals with moderate-to-severe alcohol use disorder compared to standard CBT and a case management control condition. The researchers also examined whether the situational use of coping strategies mediated the effects of tailored CBT on drinking outcomes.
HOW WAS THIS STUDY CONDUCTED?
This study was a randomized controlled trial evaluating the efficacy of an individually tailored CBT program for alcohol use disorder compared to standard CBT or a case management control condition. This study enrolled 173 adults meeting DSM-5 diagnostic criteria for moderate-to-severe alcohol use disorder recruited from radio and newspaper advertisements, social service agencies, and detoxification centers. The sample was predominantly White (93%), just over half were male (56%), and was around 50 years old on average. Participants were randomly assigned to one of three 12-session, manualized treatment conditions, delivered over 14 weeks:
1) Tailored CBT (n = 59): A highly personalized CBT program that adapted coping skills training to each participant’s real-time needs. Therapists used experience sampling data (self-reported desire to drink, high-risk situations, and coping behaviors; see below for more detail) collected from participants 4 times daily in the 2 weeks preceding treatment, during treatment (weeks 4, 6, and 10), and post-treatment (weeks 15 and 16). This data was summarized by a research assistant and provided to the therapist for use in tailoring individualized coping strategies. Therapy sessions focused on reviewing specific drinking episodes, identifying specific coping deficits, and developing strategies to manage future high-risk situations.
2) Standard CBT (n = 57): A standard, manualized CBT program that provided fixed coping skills training to address interpersonal (e.g., social pressure, conflict with others) and intrapersonal (e.g., cravings, negative emotions) triggers for drinking. The program followed structured manuals adapted from prior clinical trials and included didactic presentations, behavioral rehearsal, and homework assignments. Participants could choose from a set of elective topics (e.g., scheduling pleasant activities).
3) Case management control (n = 57): A supportive intervention without structured coping skills training. Therapists helped patients identify problems in daily living (e.g., housing, employment, family issues), including drinking, and discussed personal and community resources (e.g., Alcoholics Anonymous, psychiatric referrals). The focus was on problem-solving and support rather than direct coping skills training.
To capture real-time coping behaviors and alcohol use, the study employed an ecological momentary assessment method called experience sampling using phone call prompts 4 times daily at random intervals before, during, and after treatment. During each call, participants verbally reported current desire to drink, current situational details (e.g., location, activity), their alcohol consumption in the previous 30 minutes, and coping behaviors, if any, used to resist drinking. Each 5- to 7-minute call was audio-recorded, and research assistants coded participants’ coping strategies used (e.g., active coping, avoidance). Ecological momentary assessment data were collected before treatment (weeks 1 and 2 after baseline, but before treatment start), during treatment (in weeks 4, 6, and 10), post-treatment (in weeks 15 and 16), and for a 1-week period during 9 and 15-month follow-up periods.
In-person survey assessments were administered at baseline and every 3 months for 21 months. Primary outcomes were proportion of heavy drinking days (3+ drinks for women, 4+ drinks for men) and proportion of abstinent days reported at each 90-day period measured using the Form-90, based on the timeline follow-back method. Secondary outcomes included coping strategies (Coping Strategies Scale), alcohol abstinence self-efficacy (Alcohol Abstinence Self-Efficacy Scale), and negative consequences of drinking (Drinker Inventory of Consequences). Self-reports of alcohol and drug use were verified with breathalyzer readings at every treatment session and urine drug tests at baseline and follow-up assessments.
Statistical analyses tested whether there were group differences on percent days abstinent from alcohol and on percent days with heavy drinking over time. Analyses also examined whether coping skills explained any potential advantage for the tailored CBT on drinking outcomes compared to standard CBT and case management. The study employed an intent-to-treat approach, meaning all participants who were randomized into on of the 3 treatment conditions were included in the final analysis regardless of whether and how much treatment they received.
WHAT DID THIS STUDY FIND?
Tailored CBT led to greater reductions in drinking than standard CBT or case management
Participants who received tailored CBT reported significantly fewer heavy drinking days and a higher proportion of abstinent days compared both to those who received standard CBT and case management (see Figure below). These drinking reductions within participants who received tailored CBT were sustained up to 21 months post-treatment. Notably, standard CBT did not significantly outperform case management in reducing heavy drinking days or increasing percent days abstinent.
Coping skills and self-efficacy mediated treatment effects
Participants in the tailored CBT condition showed greater improvements in active coping strategies (e.g., seeking social support) and higher abstinence self-efficacy compared to those in standard CBT or case management conditions. Mediation analyses revealed that increases in active coping skills at least partially explained the beneficial effects of tailored CBT on drinking outcomes. Additionally, enhancements in abstinence self-efficacy also mediated the relationship between tailored CBT and long-term drinking reductions.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Tailored CBT – personalized to individuals’ coping strengths and deficits – outperformed standard CBT and case management in reducing heavy drinking days and increasing alcohol abstinent days. These effects were partially explained by improvements in active coping strategies (e.g., seeking social support, problem-solving) and abstinence self-efficacy, underscoring the critical role of coping skills in sustained recovery. Notably, the benefits of tailored CBT on drinking outcomes persisted up to 21 months post-treatment, highlighting its long-term potential to help individuals with moderate-to-severe alcohol use disorder. Unexpectedly, standard CBT did not do any better than standard case management. As study authors note, up to a point, individuals increase coping skills (e.g., seeking social support) even in the absence of specific skills training. Overall, these findings align with broader research on relapse prevention, emphasizing the critical role of coping skills as a key mechanism of behavior change in alcohol use disorder treatment. Specifically, findings suggest that dynamically strengthening active coping strategies over time equips individuals to navigate changing high-risk situations, manage cravings, and seek support – ultimately reducing relapse risk.
Unlike standard CBT, tailored CBT dynamically adjusts to each patient’s coping deficits in real-time, potentially offering a more responsive and individualized approach to treatment. Such an approach may resemble the way CBT is delivered in “real-world” settings rather than clinical trials. The integration of real-time “experience sampling” methodologies, such as ecological momentary assessment, does not, however, resemble CBT as typically delivered. It is possible that these ongoing, daily check-ins during several weeks of treatment and follow-up helped remind participants about the value of coping strategies, and potentially helping them deploy better coping skills, accounting for some of the individualized approach’s benefit. Therefore, these check-ins are best understood as part of the individualized approach. Indeed, this approach could both enhance treatment precision by allowing clinicians to track real-time coping experiences and deliver adaptive, data-driven interventions and also function as skill reminders for patients. Regarding the former, this approach aligns with research on just-in-time adaptive interventions, which leverage real-time data to provide tailored support at critical moments – such as when individuals experience cravings, stress, or exposure to high-risk situations. Although just-in-time adaptive interventions hold promise for improving engagement and long-term recovery outcomes, evidence for their effectiveness in alcohol use disorder treatment remains limited. While more research is needed, integrating experience sampling methodologies and just-in-time adaptive interventions represents a promising step toward making alcohol use disorder treatment more personalized and responsive.
Moreover, advancements in digital health tools, including mobile apps, wearable biosensors, and artificial intelligence-powered interventions, offer new opportunities to scale personalized treatment and could make tailored interventions more widely available beyond standard in-person therapy. However, additional research is needed to determine the most effective ways to implement these solutions, ensuring they enhance patient engagement and outcomes. Moreover, future studies could compare tailored CBT with other empirically supported treatment models, such as motivational enhancement therapy, 12-step facilitation, and pharmacotherapy, to identify the most effective strategies for diverse populations. Understanding which individuals benefit most from tailored CBT versus other approaches could further refine personalized treatment models for alcohol use disorder.
The study sample was relatively homogenous, consisting of primarily White, middle-aged men recruited from a single metropolitan area. This limits generalizability of the findings to more diverse populations and different cultural and healthcare settings.
Completion rates for ecological momentary assessments declined over time, with only 42% of prompts completed at month 15. This missing data may introduce measurement bias (e.g., where individuals doing better are more likely to respond to prompts), potentially affecting the accuracy of findings regarding real-time coping behaviors.
While breathalyzer and urine tests were used during treatment to verify alcohol and drug use, long-term drinking outcomes relied on self-report data. As a result, findings may be subject to recall bias or social desirability bias, potentially overestimating treatment effects.
BOTTOM LINE
This study found that tailored CBT – personalized to individuals’ real-time coping experiences – significantly improved drinking outcomes compared to standard CBT or case management. Use of active coping skills like problem solving explained the tailored approach’s advantage, highlighting the value of personalized interventions that address individual coping deficits. Rather than relying on a standardized one-size-fits all approach, assessing for, and tailoring treatment to, each person’s unique challenges dynamically over time may enhance the long-term effectiveness of alcohol use disorder treatment.
For individuals and families seeking recovery: Personalized therapy approaches, such as tailored CBT, may provide more effective long-term solutions than one-size-fits all treatments. By identifying and strengthening an individual’s unique coping skills, dynamically tailored CBT helps people navigate personal challenges more effectively and develop strategies suited to their specific needs over time. When seeking treatment, individuals and families may benefit from exploring options that assess real-time drinking triggers and coping responses.
For treatment professionals and treatment systems: Clinicians could consider adopting personalized treatment approaches that tailor coping skills training based on real-time assessments. Integrating experience sampling methods, such as ecological momentary assessment, into therapy might offer valuable insights into patients’ high-risk situations and coping behaviors. This approach enables more dynamically responsive and adaptive interventions, and could improve patient engagement and outcomes. Similarly, treatment systems could invest in infrastructure – such as technological capabilities and clinician training programs – to support the effective implementation of these personalized approaches.
For scientists: This study underscores the critical role of active coping skills as a mediator in alcohol use disorder treatment, emphasizing the importance of personalized, dynamic and adaptive interventions. Interestingly, coping skills more generally did not mediate the benefit conferred by tailored CBT. Future research is needed to explore how tailored approaches, incorporating experience sampling and real-time coping assessments, can be applied across different substance use disorders. Additionally, further studies are needed to determine which populations benefit most from tailored CBT compared to other treatment approaches.
For policy makers: Investing in dynamic, adaptive, data-driven personalized interventions could enhance long-term treatment and recovery outcomes for alcohol use disorder. Supporting research and the implementation of real-time assessment tools, such as ecological momentary assessment and just-in-time adaptive interventions, may improve treatment precision, patient engagement, and overall outcomes. Additionally, funding initiatives to integrate personalized approaches into clinical practice – such as clinician training programs and the development of digital health infrastructure – could expand access to more effective, tailored care. This, in turn, could help reduce the societal burden of alcohol use disorder.