A 20-year study of people who received services for heroin use disorder
Knowledge about long-term trajectories of individuals suffering from heroin addiction is quite rare. This study looked at this over an unusually long 20-year period with a focus on patterns of treatment and other service utilization in relation to recovery outcomes as well as individuals’ characteristics.
For people with heroin use disorder who seek treatment and other services, multiple treatment episodes and a return to harmful substance use are relatively common. For people who have resolved an heroin use problem, they continue to face social and mental health challenges, which can make it difficult to sustain recovery. Also, similar to other severe substance use disorders, many people with heroin addiction experience a chronic course of the disorder that cycles between periods of active addiction, treatment, and remission across one’s lifespan. Understanding the long-term trajectory of those with heroin use disorder can inform practices and policies to help these individuals maintain treatment gains over the long term.
Priorstudies examining heroin use disorder treatment have revealed several factors associated with treatment retention or engagement, including older age and stable housing. However, these studies have largely focused on discrete treatment episodes rather than the long-term course of treatment utilization. Studying trajectories of treatment use and their correlates can ultimately inform individualized healthcare service delivery models that promote treatment success and help to identify patients who may be at greater risk for worse treatment and recovery outcomes. Leveraging 20-year follow up data from the Australian Treatment Outcome Study, this longitudinal naturalistic study characterized the long-term trajectories of individuals with heroin use disorder after receiving treatment and other substance use services, and evaluated their relationship to patients’ baseline characteristics and 20-year recovery outcomes.
HOW WAS THIS STUDY CONDUCTED?
This study was a 20-year naturalistic longitudinal cohort study of 615 adults with heroin use disorder recruited from addiction treatment programs including methadone maintenance treatment programs, detoxification, residential rehabilitation, and needle exchange programs (n=80) in Sydney, Australia. The study characterized treatment trajectories and their relationship to participant characteristics at baseline, as well as participant outcomes 18 to 20 years thereafter.
Participants completed questionnaires at one baseline assessment (upon enrolling in the study, between 2001 and 2002), and at 6 follow-up assessments that occurred at 3 months, 12 months, 24 months, 36 months, 10-11 years, and 18-20 years after baseline. Of the participants that enrolled in the study, 393provided complete treatment-related data at all time points and were included in the current study analyses. Retention rates at follow up included 89%, 81%, 76%, 70%, 70%, and 65% at 3-month, 12-month, 24-month, 36-month, 10-11 year, and 18-20 year follow-ups, respectively. Eighteen percent of the sample was deceased at the 18-20 year follow-up.
Measures collected at baseline and follow-up concerned demographics, criminal justice involvement, type of treatment used at baseline, past-month substance use, overdose history and injection-related harms, mental/physical health, history of suicide, and comorbid psychiatric disorders.
The authors conducted model-based analyses of treatment-use patterns to identify distinct treatment trajectory groups. To do this, treatment use was evaluated as the use of any type of treatment at least once in a given year. Next, they evaluated whether treatment-trajectory group was correlated with the baseline and follow-up measures noted above. In correlation analyses conducted with baseline characteristics and treatment trajectory group, receipt of methadone and use of residential rehabilitation treatment at baseline emerged as significant correlates of treatment group, and were included in the final model . For correlation analyses conducted with 18-20 year follow-up characteristics and treatment trajectory group, several factors were identified as significant correlates of treatment group, and were included in the final model: (1) main source of income (work-related wages vs. other source of income); (2) accommodation (owning or renting a home vs. other); (3) lifetime history of prison (yes/no); (4) past-month use of heroin, benzodiazepines, alcohol, amphetamines, and/or antidepressants (yes/no).
Significant correlates were then analyzed together in collective models to identify: (1) baseline characteristics that emerge as independent predictors of treatment trajectory group, controlling for all other significant correlates, and (2) whether treatment trajectory group independently predicted participant outcomes at 18-20 year follow-up, controlling for all other significant correlates.
None of the participants had received treatment for heroin use disorder in the month preceding study enrollment. Two-thirds of participants were men (66%) in their late twenties (average age = 29 years) who were using at least one other substance besides heroin (93%). At baseline, 87% of participants were initiating treatment (34% medication treatment for heroin use disorder, 33% detoxification program, 20% residential rehabilitation), while 13% were not initiating treatment and were instead receiving services from needle exchange programs. All analyses controlled for participant age, sex, county of birth, source of income, and past-month accommodations, as reported at baseline.
WHAT DID THIS STUDY FIND?
Five trajectories of treatment use were identified
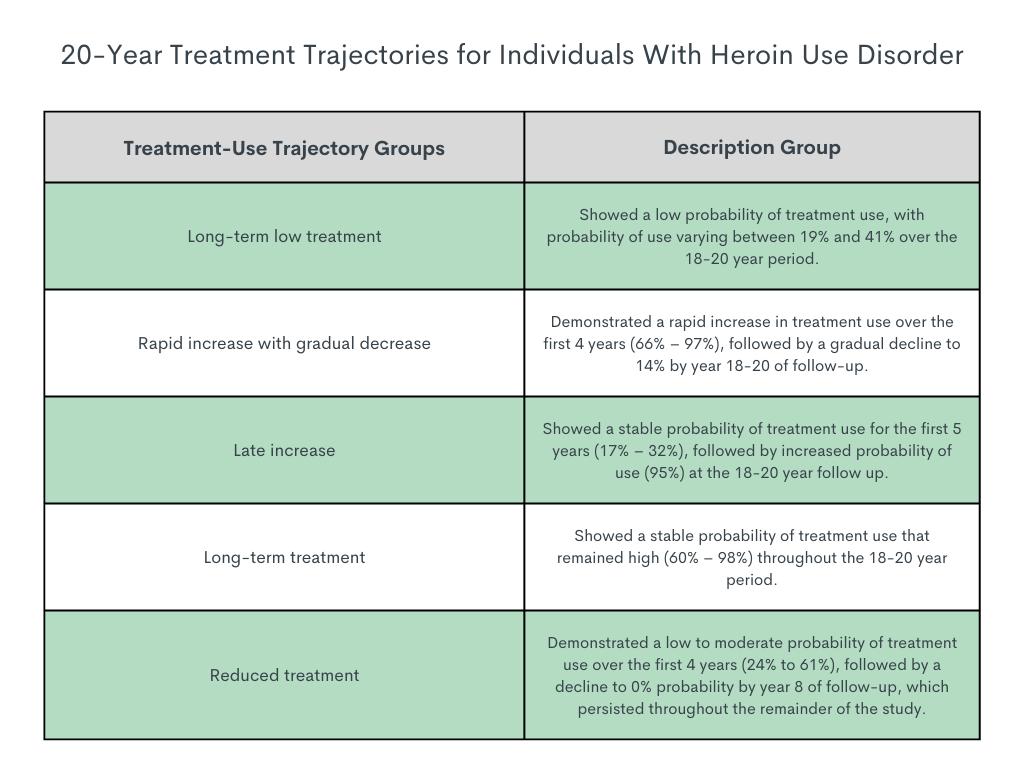
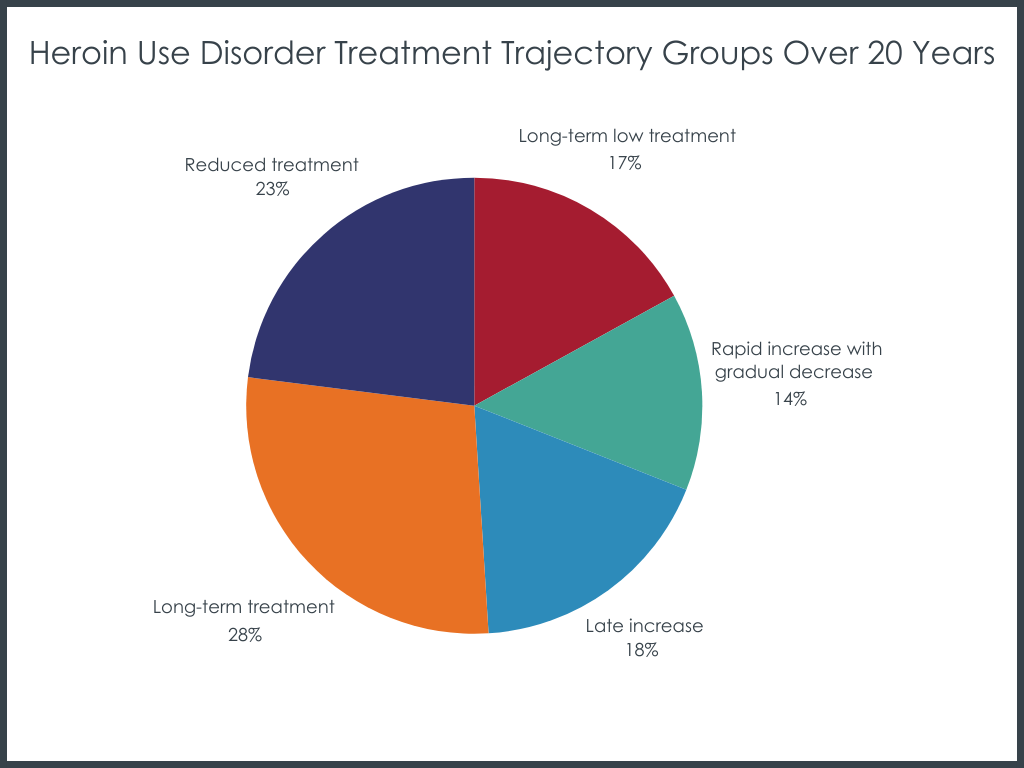
Over the 18-20 year follow-up period, there were five treatment-use trajectories identified.
Receiving methadone at baseline predicted a ‘long-term treatment’ trajectory
Individuals in methadone treatment at baseline had 3 times greater odds of being in the ‘long-term treatment’ trajectory compared both to ‘long-term low treatment’ and ‘late increase’ trajectories. No other baseline characteristics were associated with treatment trajectories.
Treatment trajectories associated withsource of income, criminal justice involvement, and drug use at 18-20 year follow up
Income & Criminal Justice Involvement: Compared to the ‘late increase’ treatment trajectory group, individuals who followed the ‘reduced treatment’ trajectory had 2.5 times greater odds of earning work-related wages as their primary source of income at the 18-20 year follow up and were less likely to have been in prison at least one time (75% lower odds) by the end of the study. The other groups didn’t differ with regard to criminal justice involvement and source of income.
Heroin Use: The ‘reduced treatment’ group was less likely to report past-month heroin use than all other groups, including the ‘long-term low treatment’ group (97% lower odds), ‘rapid increase with gradual decrease’ group (97% lower odds), ‘late increase’ group (97% lower odds), and ‘long-term treatment’ group (98% lower odds). In addition, the ‘long-term treatment’ group had 3 times greater odds of past-month heroin use than the ‘rapid increase with gradual decrease’ group.
Alcohol Use:The ‘reduced treatment’ group had 3 times greater odds of past-month alcohol use than most other treatment trajectory groups, including the ‘late increase’ group, ‘long-term low treatment’ group, and ‘long-term treatment’ group.
Amphetamine Use:The ‘rapid increase with gradual decrease’ treatment trajectory group had 3 times greater odds of past-month amphetamine use than the ‘late increase’ group and 4.56 times greater odds than the ‘long-term treatment’ group.
Benzodiazepine Use: The ‘reduced treatment’ group had lower odds of past-month benzodiazepine use than the ‘long-term treatment’ (82% lower odds) and ‘late increase’ (74% lower odds) groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study identified five distinct long-term treatment trajectories among individuals with heroin use disorder, and suggests that these trajectories are associated with baseline patient characteristics and long-term recovery outcomes.
Interestingly, only one baseline patient characteristic was found to be associated with treatment trajectory – receiving methadone treatment at baseline were most likely to follow the ‘long-term treatment’ trajectory, characterized by stable, high rates of treatment use throughout the 20-year period. Though little research has been conducted to-date, prior studies of opioid-related treatment trajectories have found other patient characteristics as potentially relevant predictors of treatment-use patterns. Among a US sample of pregnant people receiving buprenorphine treatment, patient age, race, and co-occurring substance use disorders predicted patterns of treatment adherence over a 9-month period. A Canadian study of individuals who use illicit drugs also found that non-employment was associated with retention in opioid use disorder medication treatment. Given that few studies have examined long-term opioid use disorder treatment trajectories, mixed outcomes are likely due to investigation of different patient populations, follow-up durations, and outcomes of interest. Worth special mention, for example is that this study was conducted in Australia, where universal free healthcare is available and accessible and where opioid use disorder treatment models and practices may differ in other ways from other countries. Also, treatment type (e.g., detoxification, residential) was not considered when modeling treatment-use trajectories while treatment use was coded as any use of treatment within a given year. As such, the trajectories did not reflect variability in the modality or duration of treatment episodes, an important caveat to these findings.
Nonetheless, this ‘long-term treatment’ group appears to be a more chronic sub-population. They were most likely to be receiving methadone at baseline and most likely to be using heroin and other drugs like benzodiazepines at the 20-year follow up. Therefore, this group may represent a more chronic disorder phenotype or possibly more severe end of the opioid use disorder spectrum, in which the relapse-remitting course of their disorder is associated with intermittent opioid use problems and multiple repeated treatment episodes across their lifetime. While the group assessed at 18-20 year follow-up was similar at baseline to those who were not followed-up long-term, given those not followed up are likely to be functioning more poorly, it is possible that outcomes would have been even worse if data were available on how this group fared 20 years after an initial engagement with services.
The ‘late increase’ treatment trajectory group may represent another potential at-risk sub-population, as they were least likely to have work-related wages as their primary source of income and most likely to have been in prison by follow up. In addition to the societal economic burden caused by criminal justice involvement, criminal offenders are particularly vulnerable to relapse. In line with this, the ‘late increase’ group appeared to struggle with increased likelihood of heroin and benzodiazepine use at follow up. Criminal justice involvement and illicit drug use can hinder a person’s ability to obtain employment and lack of income-based wages can increase stress and lead to engagement in illegitimate or illegal jobs. Individuals who follow this treatment trajectory and have ongoing substance use and psychosocial problems might also benefit from greater psychosocial and recovery supports (e.g., in the United States through RecoveryCommunityCenters) during and after treatment episodes to destabilize these negative long-term risk trajectories. Although all individuals with heroin use disorder could benefit from ongoing clinical outreach after completing an initial treatment episode in the form of recovery management check-ups – proven, cost-effective approaches that get people back into treatment sooner when they need it – strategies like this may be especially helpful for the ‘late increase’ group.
In contrast, individuals with a ‘reduced treatment’ trajectory, were the least likely to be using heroin and benzodiazepines at the 20-year follow up. This group slowly reduced their treatment use over the first 8 years of follow-up and did not engage in treatment thereafter. They were most likely to have work-related wages as their primary source of income and least likely to report having been to prison at the 18-20 year follow-up. This sub-population reflects a less chronic phenotype of potential treatment responders with treatment use possibly declining because remission was achieved and treatment was no longer needed. Interestingly, this group was most likely to use alcohol at follow up. Other long-term studies show that for individuals functioning well at later follow-ups, those with some alcohol use began treatment with more resources and fewer challenges from the outset, possibly reflecting a less severe addiction phenotype. However, it is unclear exactly how much this group was drinking at follow-up or if they were experiencing alcohol problems, and additional research is needed to clarify the substance use patterns that accompany this treatment trajectory.
As mentioned above, this study was conducted in Australia, where universal free healthcare is available and accessible and where opioid use disorder treatment models and practices may differ in other ways from other countries.Findings may not apply to other countries with different opioid use disorder treatment and healthcare models.
This study only included individuals who completed all study assessments over the 18-20 year follow-up period. These participants may underestimate rates of long-term substance use.
As mentioned above, given that treatment type (e.g., detoxification, residential) was not considered when modeling treatment-use trajectories and that treatmentuse was coded as any use of treatment within a given year, the trajectories did not reflect variability in the modality or duration of treatment episodes, limiting interpretation.
BOTTOM LINE
At a 20-year follow-up of heroin use disorder service engagement, long-term treatment trajectories were related tosource of income, criminal justice involvement, and drug use. Over 50% of participants had treatment involvement many years later, seemingly in response to greater challenges and poorer levels of functioning. Many strategies designed to address the chronic nature of substance use disorder could be helpful for these individuals. While recovery management check ups are proven, cost-effective strategies to aid recovery management, others like recovery community centers warrant investigation regarding their clinical and public health utilities for these at-risk individuals.
For individuals and families seeking recovery: Though additional research is needed to better understand how treatment trajectories influence recovery outcomes, several treatment modalities exist for opioid use disorder, including medication treatments, therapeutic communities, and behavioral therapies. Timely engagement in treatment can promote positive treatment and recovery outcomes. Engaging in the use of recovery support services may also help individuals achieve and maintain recovery. Future research will help identifywhetherand how recovery management approaches can destabilize these long term, negative risk trajectories.
For treatment professionals and treatment systems: Patient’s long-term treatment use patterns are likely to reflecttheir treatment success and recovery outcomes. Though additional research is needed to clarify the exact treatment patterns that pose a risk to patients, this study highlights the importance of timely intervention for early treatment engagement, continuing care and recovery support services use to help prevent relapse and promote psychosocial gains, and consideration of substance use apart from opioidsuse when treating patients for opioid use disorder.
For scientists:Evaluation of additional treatment modalities and unassisted recovery pathways, additional patient outcomes, as well as clinical and demographic moderators in additional countries are neededto enhance our understanding of treatment patterns and their impact on patient outcomes for opioid as well as other substance use disorders. The relatively small sample sizes and high amount of variability in dependent measures of interest in this study, demand additional research in larger samples. It is difficult to draw recommendations from this study. Investigations that consider treatment modality when modeling treatment-use trajectories, and that code treatment-use with consideration of frequency and duration may help inform best practices for long-term management of opioid use disorder.
For policy makers: Gaining a better understanding of long-term opioid use disorder treatment patterns and their relationship to recovery outcomes can ultimately help reveal optimal treatment pathways for successful recovery, as well as patient sub-populations that might experience increased risk of relapse. This information can ultimately guide treatment approaches to help address the public health burden of opioid and other substance use disorders. However, we still have a limited understanding of treatment-use trajectories and their impact on recovery from opioid use disorder. Additional research funding will help identify common treatment trajectories, their relationship to recovery outcomes, and the patient and provider characteristics that moderate this relationship to inform individualized treatment approaches and timely interventions that support patients at increased risk of experiencing more turbulent treatment and recovery trajectories.
For people with heroin use disorder who seek treatment and other services, multiple treatment episodes and a return to harmful substance use are relatively common. For people who have resolved an heroin use problem, they continue to face social and mental health challenges, which can make it difficult to sustain recovery. Also, similar to other severe substance use disorders, many people with heroin addiction experience a chronic course of the disorder that cycles between periods of active addiction, treatment, and remission across one’s lifespan. Understanding the long-term trajectory of those with heroin use disorder can inform practices and policies to help these individuals maintain treatment gains over the long term.
Priorstudies examining heroin use disorder treatment have revealed several factors associated with treatment retention or engagement, including older age and stable housing. However, these studies have largely focused on discrete treatment episodes rather than the long-term course of treatment utilization. Studying trajectories of treatment use and their correlates can ultimately inform individualized healthcare service delivery models that promote treatment success and help to identify patients who may be at greater risk for worse treatment and recovery outcomes. Leveraging 20-year follow up data from the Australian Treatment Outcome Study, this longitudinal naturalistic study characterized the long-term trajectories of individuals with heroin use disorder after receiving treatment and other substance use services, and evaluated their relationship to patients’ baseline characteristics and 20-year recovery outcomes.
HOW WAS THIS STUDY CONDUCTED?
This study was a 20-year naturalistic longitudinal cohort study of 615 adults with heroin use disorder recruited from addiction treatment programs including methadone maintenance treatment programs, detoxification, residential rehabilitation, and needle exchange programs (n=80) in Sydney, Australia. The study characterized treatment trajectories and their relationship to participant characteristics at baseline, as well as participant outcomes 18 to 20 years thereafter.
Participants completed questionnaires at one baseline assessment (upon enrolling in the study, between 2001 and 2002), and at 6 follow-up assessments that occurred at 3 months, 12 months, 24 months, 36 months, 10-11 years, and 18-20 years after baseline. Of the participants that enrolled in the study, 393provided complete treatment-related data at all time points and were included in the current study analyses. Retention rates at follow up included 89%, 81%, 76%, 70%, 70%, and 65% at 3-month, 12-month, 24-month, 36-month, 10-11 year, and 18-20 year follow-ups, respectively. Eighteen percent of the sample was deceased at the 18-20 year follow-up.
Measures collected at baseline and follow-up concerned demographics, criminal justice involvement, type of treatment used at baseline, past-month substance use, overdose history and injection-related harms, mental/physical health, history of suicide, and comorbid psychiatric disorders.
The authors conducted model-based analyses of treatment-use patterns to identify distinct treatment trajectory groups. To do this, treatment use was evaluated as the use of any type of treatment at least once in a given year. Next, they evaluated whether treatment-trajectory group was correlated with the baseline and follow-up measures noted above. In correlation analyses conducted with baseline characteristics and treatment trajectory group, receipt of methadone and use of residential rehabilitation treatment at baseline emerged as significant correlates of treatment group, and were included in the final model . For correlation analyses conducted with 18-20 year follow-up characteristics and treatment trajectory group, several factors were identified as significant correlates of treatment group, and were included in the final model: (1) main source of income (work-related wages vs. other source of income); (2) accommodation (owning or renting a home vs. other); (3) lifetime history of prison (yes/no); (4) past-month use of heroin, benzodiazepines, alcohol, amphetamines, and/or antidepressants (yes/no).
Significant correlates were then analyzed together in collective models to identify: (1) baseline characteristics that emerge as independent predictors of treatment trajectory group, controlling for all other significant correlates, and (2) whether treatment trajectory group independently predicted participant outcomes at 18-20 year follow-up, controlling for all other significant correlates.
None of the participants had received treatment for heroin use disorder in the month preceding study enrollment. Two-thirds of participants were men (66%) in their late twenties (average age = 29 years) who were using at least one other substance besides heroin (93%). At baseline, 87% of participants were initiating treatment (34% medication treatment for heroin use disorder, 33% detoxification program, 20% residential rehabilitation), while 13% were not initiating treatment and were instead receiving services from needle exchange programs. All analyses controlled for participant age, sex, county of birth, source of income, and past-month accommodations, as reported at baseline.
WHAT DID THIS STUDY FIND?
Five trajectories of treatment use were identified
Over the 18-20 year follow-up period, there were five treatment-use trajectories identified.
Receiving methadone at baseline predicted a ‘long-term treatment’ trajectory
Individuals in methadone treatment at baseline had 3 times greater odds of being in the ‘long-term treatment’ trajectory compared both to ‘long-term low treatment’ and ‘late increase’ trajectories. No other baseline characteristics were associated with treatment trajectories.
Treatment trajectories associated withsource of income, criminal justice involvement, and drug use at 18-20 year follow up
Income & Criminal Justice Involvement: Compared to the ‘late increase’ treatment trajectory group, individuals who followed the ‘reduced treatment’ trajectory had 2.5 times greater odds of earning work-related wages as their primary source of income at the 18-20 year follow up and were less likely to have been in prison at least one time (75% lower odds) by the end of the study. The other groups didn’t differ with regard to criminal justice involvement and source of income.
Heroin Use: The ‘reduced treatment’ group was less likely to report past-month heroin use than all other groups, including the ‘long-term low treatment’ group (97% lower odds), ‘rapid increase with gradual decrease’ group (97% lower odds), ‘late increase’ group (97% lower odds), and ‘long-term treatment’ group (98% lower odds). In addition, the ‘long-term treatment’ group had 3 times greater odds of past-month heroin use than the ‘rapid increase with gradual decrease’ group.
Alcohol Use:The ‘reduced treatment’ group had 3 times greater odds of past-month alcohol use than most other treatment trajectory groups, including the ‘late increase’ group, ‘long-term low treatment’ group, and ‘long-term treatment’ group.
Amphetamine Use:The ‘rapid increase with gradual decrease’ treatment trajectory group had 3 times greater odds of past-month amphetamine use than the ‘late increase’ group and 4.56 times greater odds than the ‘long-term treatment’ group.
Benzodiazepine Use: The ‘reduced treatment’ group had lower odds of past-month benzodiazepine use than the ‘long-term treatment’ (82% lower odds) and ‘late increase’ (74% lower odds) groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study identified five distinct long-term treatment trajectories among individuals with heroin use disorder, and suggests that these trajectories are associated with baseline patient characteristics and long-term recovery outcomes.
Interestingly, only one baseline patient characteristic was found to be associated with treatment trajectory – receiving methadone treatment at baseline were most likely to follow the ‘long-term treatment’ trajectory, characterized by stable, high rates of treatment use throughout the 20-year period. Though little research has been conducted to-date, prior studies of opioid-related treatment trajectories have found other patient characteristics as potentially relevant predictors of treatment-use patterns. Among a US sample of pregnant people receiving buprenorphine treatment, patient age, race, and co-occurring substance use disorders predicted patterns of treatment adherence over a 9-month period. A Canadian study of individuals who use illicit drugs also found that non-employment was associated with retention in opioid use disorder medication treatment. Given that few studies have examined long-term opioid use disorder treatment trajectories, mixed outcomes are likely due to investigation of different patient populations, follow-up durations, and outcomes of interest. Worth special mention, for example is that this study was conducted in Australia, where universal free healthcare is available and accessible and where opioid use disorder treatment models and practices may differ in other ways from other countries. Also, treatment type (e.g., detoxification, residential) was not considered when modeling treatment-use trajectories while treatment use was coded as any use of treatment within a given year. As such, the trajectories did not reflect variability in the modality or duration of treatment episodes, an important caveat to these findings.
Nonetheless, this ‘long-term treatment’ group appears to be a more chronic sub-population. They were most likely to be receiving methadone at baseline and most likely to be using heroin and other drugs like benzodiazepines at the 20-year follow up. Therefore, this group may represent a more chronic disorder phenotype or possibly more severe end of the opioid use disorder spectrum, in which the relapse-remitting course of their disorder is associated with intermittent opioid use problems and multiple repeated treatment episodes across their lifetime. While the group assessed at 18-20 year follow-up was similar at baseline to those who were not followed-up long-term, given those not followed up are likely to be functioning more poorly, it is possible that outcomes would have been even worse if data were available on how this group fared 20 years after an initial engagement with services.
The ‘late increase’ treatment trajectory group may represent another potential at-risk sub-population, as they were least likely to have work-related wages as their primary source of income and most likely to have been in prison by follow up. In addition to the societal economic burden caused by criminal justice involvement, criminal offenders are particularly vulnerable to relapse. In line with this, the ‘late increase’ group appeared to struggle with increased likelihood of heroin and benzodiazepine use at follow up. Criminal justice involvement and illicit drug use can hinder a person’s ability to obtain employment and lack of income-based wages can increase stress and lead to engagement in illegitimate or illegal jobs. Individuals who follow this treatment trajectory and have ongoing substance use and psychosocial problems might also benefit from greater psychosocial and recovery supports (e.g., in the United States through RecoveryCommunityCenters) during and after treatment episodes to destabilize these negative long-term risk trajectories. Although all individuals with heroin use disorder could benefit from ongoing clinical outreach after completing an initial treatment episode in the form of recovery management check-ups – proven, cost-effective approaches that get people back into treatment sooner when they need it – strategies like this may be especially helpful for the ‘late increase’ group.
In contrast, individuals with a ‘reduced treatment’ trajectory, were the least likely to be using heroin and benzodiazepines at the 20-year follow up. This group slowly reduced their treatment use over the first 8 years of follow-up and did not engage in treatment thereafter. They were most likely to have work-related wages as their primary source of income and least likely to report having been to prison at the 18-20 year follow-up. This sub-population reflects a less chronic phenotype of potential treatment responders with treatment use possibly declining because remission was achieved and treatment was no longer needed. Interestingly, this group was most likely to use alcohol at follow up. Other long-term studies show that for individuals functioning well at later follow-ups, those with some alcohol use began treatment with more resources and fewer challenges from the outset, possibly reflecting a less severe addiction phenotype. However, it is unclear exactly how much this group was drinking at follow-up or if they were experiencing alcohol problems, and additional research is needed to clarify the substance use patterns that accompany this treatment trajectory.
As mentioned above, this study was conducted in Australia, where universal free healthcare is available and accessible and where opioid use disorder treatment models and practices may differ in other ways from other countries.Findings may not apply to other countries with different opioid use disorder treatment and healthcare models.
This study only included individuals who completed all study assessments over the 18-20 year follow-up period. These participants may underestimate rates of long-term substance use.
As mentioned above, given that treatment type (e.g., detoxification, residential) was not considered when modeling treatment-use trajectories and that treatmentuse was coded as any use of treatment within a given year, the trajectories did not reflect variability in the modality or duration of treatment episodes, limiting interpretation.
BOTTOM LINE
At a 20-year follow-up of heroin use disorder service engagement, long-term treatment trajectories were related tosource of income, criminal justice involvement, and drug use. Over 50% of participants had treatment involvement many years later, seemingly in response to greater challenges and poorer levels of functioning. Many strategies designed to address the chronic nature of substance use disorder could be helpful for these individuals. While recovery management check ups are proven, cost-effective strategies to aid recovery management, others like recovery community centers warrant investigation regarding their clinical and public health utilities for these at-risk individuals.
For individuals and families seeking recovery: Though additional research is needed to better understand how treatment trajectories influence recovery outcomes, several treatment modalities exist for opioid use disorder, including medication treatments, therapeutic communities, and behavioral therapies. Timely engagement in treatment can promote positive treatment and recovery outcomes. Engaging in the use of recovery support services may also help individuals achieve and maintain recovery. Future research will help identifywhetherand how recovery management approaches can destabilize these long term, negative risk trajectories.
For treatment professionals and treatment systems: Patient’s long-term treatment use patterns are likely to reflecttheir treatment success and recovery outcomes. Though additional research is needed to clarify the exact treatment patterns that pose a risk to patients, this study highlights the importance of timely intervention for early treatment engagement, continuing care and recovery support services use to help prevent relapse and promote psychosocial gains, and consideration of substance use apart from opioidsuse when treating patients for opioid use disorder.
For scientists:Evaluation of additional treatment modalities and unassisted recovery pathways, additional patient outcomes, as well as clinical and demographic moderators in additional countries are neededto enhance our understanding of treatment patterns and their impact on patient outcomes for opioid as well as other substance use disorders. The relatively small sample sizes and high amount of variability in dependent measures of interest in this study, demand additional research in larger samples. It is difficult to draw recommendations from this study. Investigations that consider treatment modality when modeling treatment-use trajectories, and that code treatment-use with consideration of frequency and duration may help inform best practices for long-term management of opioid use disorder.
For policy makers: Gaining a better understanding of long-term opioid use disorder treatment patterns and their relationship to recovery outcomes can ultimately help reveal optimal treatment pathways for successful recovery, as well as patient sub-populations that might experience increased risk of relapse. This information can ultimately guide treatment approaches to help address the public health burden of opioid and other substance use disorders. However, we still have a limited understanding of treatment-use trajectories and their impact on recovery from opioid use disorder. Additional research funding will help identify common treatment trajectories, their relationship to recovery outcomes, and the patient and provider characteristics that moderate this relationship to inform individualized treatment approaches and timely interventions that support patients at increased risk of experiencing more turbulent treatment and recovery trajectories.
For people with heroin use disorder who seek treatment and other services, multiple treatment episodes and a return to harmful substance use are relatively common. For people who have resolved an heroin use problem, they continue to face social and mental health challenges, which can make it difficult to sustain recovery. Also, similar to other severe substance use disorders, many people with heroin addiction experience a chronic course of the disorder that cycles between periods of active addiction, treatment, and remission across one’s lifespan. Understanding the long-term trajectory of those with heroin use disorder can inform practices and policies to help these individuals maintain treatment gains over the long term.
Priorstudies examining heroin use disorder treatment have revealed several factors associated with treatment retention or engagement, including older age and stable housing. However, these studies have largely focused on discrete treatment episodes rather than the long-term course of treatment utilization. Studying trajectories of treatment use and their correlates can ultimately inform individualized healthcare service delivery models that promote treatment success and help to identify patients who may be at greater risk for worse treatment and recovery outcomes. Leveraging 20-year follow up data from the Australian Treatment Outcome Study, this longitudinal naturalistic study characterized the long-term trajectories of individuals with heroin use disorder after receiving treatment and other substance use services, and evaluated their relationship to patients’ baseline characteristics and 20-year recovery outcomes.
HOW WAS THIS STUDY CONDUCTED?
This study was a 20-year naturalistic longitudinal cohort study of 615 adults with heroin use disorder recruited from addiction treatment programs including methadone maintenance treatment programs, detoxification, residential rehabilitation, and needle exchange programs (n=80) in Sydney, Australia. The study characterized treatment trajectories and their relationship to participant characteristics at baseline, as well as participant outcomes 18 to 20 years thereafter.
Participants completed questionnaires at one baseline assessment (upon enrolling in the study, between 2001 and 2002), and at 6 follow-up assessments that occurred at 3 months, 12 months, 24 months, 36 months, 10-11 years, and 18-20 years after baseline. Of the participants that enrolled in the study, 393provided complete treatment-related data at all time points and were included in the current study analyses. Retention rates at follow up included 89%, 81%, 76%, 70%, 70%, and 65% at 3-month, 12-month, 24-month, 36-month, 10-11 year, and 18-20 year follow-ups, respectively. Eighteen percent of the sample was deceased at the 18-20 year follow-up.
Measures collected at baseline and follow-up concerned demographics, criminal justice involvement, type of treatment used at baseline, past-month substance use, overdose history and injection-related harms, mental/physical health, history of suicide, and comorbid psychiatric disorders.
The authors conducted model-based analyses of treatment-use patterns to identify distinct treatment trajectory groups. To do this, treatment use was evaluated as the use of any type of treatment at least once in a given year. Next, they evaluated whether treatment-trajectory group was correlated with the baseline and follow-up measures noted above. In correlation analyses conducted with baseline characteristics and treatment trajectory group, receipt of methadone and use of residential rehabilitation treatment at baseline emerged as significant correlates of treatment group, and were included in the final model . For correlation analyses conducted with 18-20 year follow-up characteristics and treatment trajectory group, several factors were identified as significant correlates of treatment group, and were included in the final model: (1) main source of income (work-related wages vs. other source of income); (2) accommodation (owning or renting a home vs. other); (3) lifetime history of prison (yes/no); (4) past-month use of heroin, benzodiazepines, alcohol, amphetamines, and/or antidepressants (yes/no).
Significant correlates were then analyzed together in collective models to identify: (1) baseline characteristics that emerge as independent predictors of treatment trajectory group, controlling for all other significant correlates, and (2) whether treatment trajectory group independently predicted participant outcomes at 18-20 year follow-up, controlling for all other significant correlates.
None of the participants had received treatment for heroin use disorder in the month preceding study enrollment. Two-thirds of participants were men (66%) in their late twenties (average age = 29 years) who were using at least one other substance besides heroin (93%). At baseline, 87% of participants were initiating treatment (34% medication treatment for heroin use disorder, 33% detoxification program, 20% residential rehabilitation), while 13% were not initiating treatment and were instead receiving services from needle exchange programs. All analyses controlled for participant age, sex, county of birth, source of income, and past-month accommodations, as reported at baseline.
WHAT DID THIS STUDY FIND?
Five trajectories of treatment use were identified
Over the 18-20 year follow-up period, there were five treatment-use trajectories identified.
Receiving methadone at baseline predicted a ‘long-term treatment’ trajectory
Individuals in methadone treatment at baseline had 3 times greater odds of being in the ‘long-term treatment’ trajectory compared both to ‘long-term low treatment’ and ‘late increase’ trajectories. No other baseline characteristics were associated with treatment trajectories.
Treatment trajectories associated withsource of income, criminal justice involvement, and drug use at 18-20 year follow up
Income & Criminal Justice Involvement: Compared to the ‘late increase’ treatment trajectory group, individuals who followed the ‘reduced treatment’ trajectory had 2.5 times greater odds of earning work-related wages as their primary source of income at the 18-20 year follow up and were less likely to have been in prison at least one time (75% lower odds) by the end of the study. The other groups didn’t differ with regard to criminal justice involvement and source of income.
Heroin Use: The ‘reduced treatment’ group was less likely to report past-month heroin use than all other groups, including the ‘long-term low treatment’ group (97% lower odds), ‘rapid increase with gradual decrease’ group (97% lower odds), ‘late increase’ group (97% lower odds), and ‘long-term treatment’ group (98% lower odds). In addition, the ‘long-term treatment’ group had 3 times greater odds of past-month heroin use than the ‘rapid increase with gradual decrease’ group.
Alcohol Use:The ‘reduced treatment’ group had 3 times greater odds of past-month alcohol use than most other treatment trajectory groups, including the ‘late increase’ group, ‘long-term low treatment’ group, and ‘long-term treatment’ group.
Amphetamine Use:The ‘rapid increase with gradual decrease’ treatment trajectory group had 3 times greater odds of past-month amphetamine use than the ‘late increase’ group and 4.56 times greater odds than the ‘long-term treatment’ group.
Benzodiazepine Use: The ‘reduced treatment’ group had lower odds of past-month benzodiazepine use than the ‘long-term treatment’ (82% lower odds) and ‘late increase’ (74% lower odds) groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study identified five distinct long-term treatment trajectories among individuals with heroin use disorder, and suggests that these trajectories are associated with baseline patient characteristics and long-term recovery outcomes.
Interestingly, only one baseline patient characteristic was found to be associated with treatment trajectory – receiving methadone treatment at baseline were most likely to follow the ‘long-term treatment’ trajectory, characterized by stable, high rates of treatment use throughout the 20-year period. Though little research has been conducted to-date, prior studies of opioid-related treatment trajectories have found other patient characteristics as potentially relevant predictors of treatment-use patterns. Among a US sample of pregnant people receiving buprenorphine treatment, patient age, race, and co-occurring substance use disorders predicted patterns of treatment adherence over a 9-month period. A Canadian study of individuals who use illicit drugs also found that non-employment was associated with retention in opioid use disorder medication treatment. Given that few studies have examined long-term opioid use disorder treatment trajectories, mixed outcomes are likely due to investigation of different patient populations, follow-up durations, and outcomes of interest. Worth special mention, for example is that this study was conducted in Australia, where universal free healthcare is available and accessible and where opioid use disorder treatment models and practices may differ in other ways from other countries. Also, treatment type (e.g., detoxification, residential) was not considered when modeling treatment-use trajectories while treatment use was coded as any use of treatment within a given year. As such, the trajectories did not reflect variability in the modality or duration of treatment episodes, an important caveat to these findings.
Nonetheless, this ‘long-term treatment’ group appears to be a more chronic sub-population. They were most likely to be receiving methadone at baseline and most likely to be using heroin and other drugs like benzodiazepines at the 20-year follow up. Therefore, this group may represent a more chronic disorder phenotype or possibly more severe end of the opioid use disorder spectrum, in which the relapse-remitting course of their disorder is associated with intermittent opioid use problems and multiple repeated treatment episodes across their lifetime. While the group assessed at 18-20 year follow-up was similar at baseline to those who were not followed-up long-term, given those not followed up are likely to be functioning more poorly, it is possible that outcomes would have been even worse if data were available on how this group fared 20 years after an initial engagement with services.
The ‘late increase’ treatment trajectory group may represent another potential at-risk sub-population, as they were least likely to have work-related wages as their primary source of income and most likely to have been in prison by follow up. In addition to the societal economic burden caused by criminal justice involvement, criminal offenders are particularly vulnerable to relapse. In line with this, the ‘late increase’ group appeared to struggle with increased likelihood of heroin and benzodiazepine use at follow up. Criminal justice involvement and illicit drug use can hinder a person’s ability to obtain employment and lack of income-based wages can increase stress and lead to engagement in illegitimate or illegal jobs. Individuals who follow this treatment trajectory and have ongoing substance use and psychosocial problems might also benefit from greater psychosocial and recovery supports (e.g., in the United States through RecoveryCommunityCenters) during and after treatment episodes to destabilize these negative long-term risk trajectories. Although all individuals with heroin use disorder could benefit from ongoing clinical outreach after completing an initial treatment episode in the form of recovery management check-ups – proven, cost-effective approaches that get people back into treatment sooner when they need it – strategies like this may be especially helpful for the ‘late increase’ group.
In contrast, individuals with a ‘reduced treatment’ trajectory, were the least likely to be using heroin and benzodiazepines at the 20-year follow up. This group slowly reduced their treatment use over the first 8 years of follow-up and did not engage in treatment thereafter. They were most likely to have work-related wages as their primary source of income and least likely to report having been to prison at the 18-20 year follow-up. This sub-population reflects a less chronic phenotype of potential treatment responders with treatment use possibly declining because remission was achieved and treatment was no longer needed. Interestingly, this group was most likely to use alcohol at follow up. Other long-term studies show that for individuals functioning well at later follow-ups, those with some alcohol use began treatment with more resources and fewer challenges from the outset, possibly reflecting a less severe addiction phenotype. However, it is unclear exactly how much this group was drinking at follow-up or if they were experiencing alcohol problems, and additional research is needed to clarify the substance use patterns that accompany this treatment trajectory.
As mentioned above, this study was conducted in Australia, where universal free healthcare is available and accessible and where opioid use disorder treatment models and practices may differ in other ways from other countries.Findings may not apply to other countries with different opioid use disorder treatment and healthcare models.
This study only included individuals who completed all study assessments over the 18-20 year follow-up period. These participants may underestimate rates of long-term substance use.
As mentioned above, given that treatment type (e.g., detoxification, residential) was not considered when modeling treatment-use trajectories and that treatmentuse was coded as any use of treatment within a given year, the trajectories did not reflect variability in the modality or duration of treatment episodes, limiting interpretation.
BOTTOM LINE
At a 20-year follow-up of heroin use disorder service engagement, long-term treatment trajectories were related tosource of income, criminal justice involvement, and drug use. Over 50% of participants had treatment involvement many years later, seemingly in response to greater challenges and poorer levels of functioning. Many strategies designed to address the chronic nature of substance use disorder could be helpful for these individuals. While recovery management check ups are proven, cost-effective strategies to aid recovery management, others like recovery community centers warrant investigation regarding their clinical and public health utilities for these at-risk individuals.
For individuals and families seeking recovery: Though additional research is needed to better understand how treatment trajectories influence recovery outcomes, several treatment modalities exist for opioid use disorder, including medication treatments, therapeutic communities, and behavioral therapies. Timely engagement in treatment can promote positive treatment and recovery outcomes. Engaging in the use of recovery support services may also help individuals achieve and maintain recovery. Future research will help identifywhetherand how recovery management approaches can destabilize these long term, negative risk trajectories.
For treatment professionals and treatment systems: Patient’s long-term treatment use patterns are likely to reflecttheir treatment success and recovery outcomes. Though additional research is needed to clarify the exact treatment patterns that pose a risk to patients, this study highlights the importance of timely intervention for early treatment engagement, continuing care and recovery support services use to help prevent relapse and promote psychosocial gains, and consideration of substance use apart from opioidsuse when treating patients for opioid use disorder.
For scientists:Evaluation of additional treatment modalities and unassisted recovery pathways, additional patient outcomes, as well as clinical and demographic moderators in additional countries are neededto enhance our understanding of treatment patterns and their impact on patient outcomes for opioid as well as other substance use disorders. The relatively small sample sizes and high amount of variability in dependent measures of interest in this study, demand additional research in larger samples. It is difficult to draw recommendations from this study. Investigations that consider treatment modality when modeling treatment-use trajectories, and that code treatment-use with consideration of frequency and duration may help inform best practices for long-term management of opioid use disorder.
For policy makers: Gaining a better understanding of long-term opioid use disorder treatment patterns and their relationship to recovery outcomes can ultimately help reveal optimal treatment pathways for successful recovery, as well as patient sub-populations that might experience increased risk of relapse. This information can ultimately guide treatment approaches to help address the public health burden of opioid and other substance use disorders. However, we still have a limited understanding of treatment-use trajectories and their impact on recovery from opioid use disorder. Additional research funding will help identify common treatment trajectories, their relationship to recovery outcomes, and the patient and provider characteristics that moderate this relationship to inform individualized treatment approaches and timely interventions that support patients at increased risk of experiencing more turbulent treatment and recovery trajectories.