Access to recovery residences limited for those taking buprenorphine: Results from South Florida
Evidence suggests that, despite federal policy to the contrary, those seeking care at recovery residences may have constrained access if taking buprenorphine – the most commonly prescribed medication for opioid use disorder. The present study investigated buprenorphine-related policies of recovery residences in South Florida, an area with a high density of treatment and recovery supports.
In 2022, 81,806 people died due to opioid-involved overdose. The impact of the overdose epidemic has been uneven across the US with states such as Florida exceeding the national averages in opioid overdose deaths. Medications for opioid use disorder (e.g., buprenorphine, often prescribed in formulation with naloxone known by the brand name Suboxone) are effective at reducing the risk of overdose and improving opioid use over time. Research regarding ways to augment the benefits of opioid use disorder medications, with both professional-clinical and non-professional recovery supports, are ongoing. While research suggests cognitive-behavioral therapy may not improve on buprenorphine’s benefits, community-based mutual-help group participation (e.g., in Narcotics Anonymous) is associated with improved outcomes. In addition, recovery residences may be particularly valuable resources; research on Oxford House recovery residences suggest they improve substance use outcomes and are cost-effective.
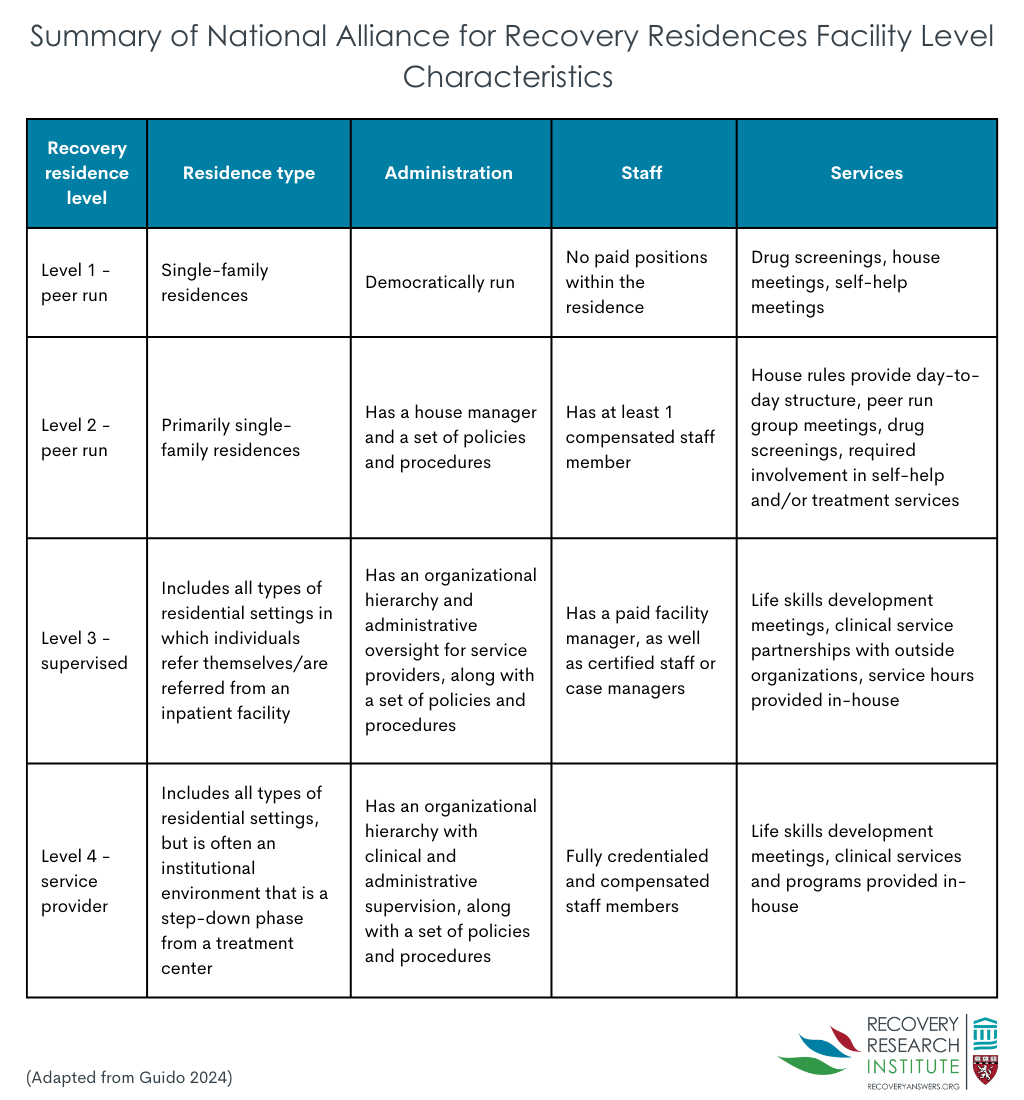
Recovery residences (sometimes also called sober living homes) provide a safe living environment in which individuals can begin to transition back to their daily lives. The characteristics of recovery residences are variable, offering different lengths of stay, levels of monitoring and support, and have different requirements (e.g., for mutual-help attendance and employment). Overall, recovery residences are categorized into 1 of 4 levels based on services provided (see figure below) with level 1 homes being peer-run and offering minimal services to level 4 being closer to a institutional environment.
Rules and regulations for recovery residences vary widely. Despite organizations such as the National Alliance for Recovery Residences providing certification and guidance for recovery residence operations, the day-to-day operations of residences is at the discretion of individual residence owners/operators. This can become problematic as some of these operators have misconceptions about medications for opioid use disorder (e.g., that such medications are “replacing one drug for another” and are therefore not helpful). This has resulted in some seeking care at recovery residences being denied access due to taking medications for opioid use disorder. This is noteworthy given that, technically, federal guidelines prohibit this kind of discrimination.
It is unclear how common recovery residence admission is denied due to opioid disorder medication use. To examine this question, the present study investigated the buprenorphine policies of recovery residences in South Florida, an area with high density of residential treatment programs and common continuing care options like recovery residences.
HOW WAS THIS STUDY CONDUCTED?
This was a quantitative cross-sectional descriptive study in which the research team contacted recovery residences listed in the Florida Association of Recovery Residences directory. The primary goal was to determine if recovery residences in South Florida accepted individuals currently prescribed buprenorphine. Descriptive statistics were used to characterize the outcome of inquiries into admission at recovery residences. The study also examined if any restrictions were placed on such admissions of those prescribed buprenorphine (e.g., dosage limitations).
The authors downloaded the contact information for a list of recovery residences posted publicly on the Florida Association of Recovery Residences website. This resulted in a list of 141 Florida Association of Recovery Residences certified recovery residences. Researchers contacted recovery residences during business hours (between 8 AM and 6 PM Monday – Friday). When speaking to residence staff researchers followed a script where they pretended to be a person with an opioid use disorder prescribed buprenorphine who was seeking admission to the recovery residence. The scripted call included the following questions: “Hi, good morning/afternoon/evening. How are you? My name is ____. I am calling to find out a bit more information about your program. Is it okay if I ask some questions?” and “I am super excited to get my life on track. I recently just went into recovery, and I am taking buprenorphine 8 mg two times a day. Do you accept people taking buprenorphine into your program?”. If the residence staff indicated they either did not or conditionally allowed residents to take buprenorphine, the research team member inquired further with: “Okay, can you clarify for me why you do not accept individuals taking buprenorphine? I am no longer currently using any street drugs.” Responses on specific policies, including dose limitations, tapering requirements, and necessary documentation from providers were recorded. Researchers did not ask residence staff members to disclose any personal information (e.g., names). Each facility was contacted up to 3 times before being excluded from analyses.
All facilities were contacted between July 15, 2022 and December 30, 2022. The research team randomly contacted recovery residences until they reached 100 total (71% of the 141 certified in Florida) were contacted. Of the facilities reached, most (67%) were in Palm Beach County, followed by Broward County (31%) and Miami-Dade County (2%). Most were designated as level 2 (55%) followed by level 4 (26%), level 1 (14%), and level 3 (5%).
WHAT DID THIS STUDY FIND?
Most recovery residences denied access due to buprenorphine prescription
Of the 100 residences contacted, 53 did not accept residents if they were prescribed buprenorphine (regardless of dosage). The remaining residences either permitted individuals taking buprenorphine on a conditional basis (31 of 100; see below for specific conditions) or allowed admission regardless of buprenorphine prescription (16 of 100).
Conditional admission due to buprenorphine prescription varied widely across residences
Of the 31 residences with conditional acceptance of individuals taking buprenorphine, 8 (25.8%) required individuals to completely taper off buprenorphine (no data on taper timeframe were collected), 12 (38.7 %) allowed a maximum buprenorphine dosage of 8 mg daily, 4 (12.9 %) had a maximum 12 mg daily dosage, 2 (6.5 %) had a maximum 16 mg daily dosage, and 2 (6.5%) required a provider letter for admission. The remaining 3 (9.7%) residences did not to disclose their conditional admission policies.
Differences in admission policies did not vary by recovery residence county or level
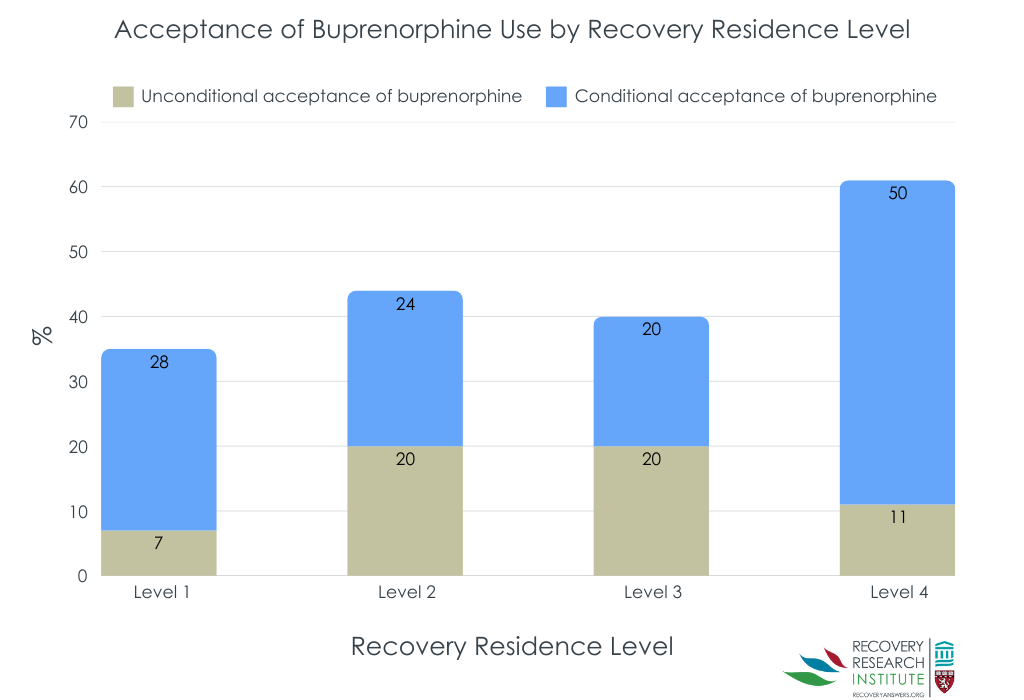
No significant differences were found in recovery residence policies based on where the residences were located (county) or level. Though descriptively, level 4 facilities – which are typically part of larger clinical organizations – had higher levels of conditional acceptance than facilities with other levels (see figure below).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that recovery residences are denying admission to potential residents based on being prescribed the agonist medication buprenorphine for opioid use disorder. Of the recovery residences contacted by research staff, only 16% allowed individuals taking buprenorphine regardless of dosage. The remaining residences either barred admission entirely or only admitted those taking buprenorphine on a conditional basis (e.g., after tapering off). While data were not collected on the nature of the conditional taper, tacitly encouraging patients to taper off buprenorphine – by making residence contingent on such a taper – is likely to produce harms.
At the same time, some consider that there can be other types of concerns regarding buprenorphine’s risks. As an agonist that can produce euphoria and be intoxicating, it is prone to diversion. Relatedly, some individuals starting a recovery attempt who are not taking buprenorphine and do not want to take it may find that the presence of this medication (or any medication with psychoactive properties) triggers drug cravings. Another policy option, therefore, might support access both to recovery residences that serve individuals who take agonist medications and also to recovery residences where people would not be exposed to agonists like buprenorphine. The types of residences could be clearly designated. To be sure, such an option would not be without controversy – there would be many nuances to address. Given the empirical support for buprenorphine as well as worries about the risks of buprenorphine among some individuals seeking recovery, all in context of the public health need to address opioid use disorder, increased availability of person-centered options may help engage and attract the largest possible number of individuals that need it to recovery residences.
This all being said, it is unclear how representative the sample was in the present research. At the time of the publication of this study, the authors report there were 2042 recovery residences in Florida. However, the present study only contacted 100 total recovery residences (~5% of the residences in Florida). This small sample may not provide the most accurate view of the state of recovery residences in South Florida.
It is unclear how representative the sample was in the present research. At the time of the publication of this study the authors report there were 2042 recovery residences in Florida. However, the present study only contacted 100 total recovery residences (~5% of the residences in Florida). This small sample may not provide the most accurate view of the state of recovery residences in South Florida.
Admission policy information collected was limited to the knowledge of staff members who answered the phone at each recovery residence. The authors state that they were unable to obtain verification of policies from other sources. It is possible that information provided by residence staff was inaccurate.
BOTTOM LINE
Results of this study suggest that individuals taking buprenorphine have reduced access to recovery residences in South Florida. Results of this study found that 53% of contacted recovery residences deny admission to those prescribed buprenorphine. Additionally, 31% of recovery residences had conditional buprenorphine policies, including requiring potential residents to taper off buprenorphine. Tacitly encouraging individuals to discontinue buprenorphine (i.e., by requiring taper to obtain residence) can increase risk of relapse and potential overdose. Residences affiliated with clinical providers (Level IV) may be more accepting of individuals taking medications. Although the present study did not explore why such policies were in place, it is possible that stigma towards/misinformation about buprenorphine among staff and leadership may be a reason. It is critical for more research to be conducted investigating possible reasons for such policies and how barriers to access can be addressed.
For individuals and families seeking recovery: The present study suggests that recovery residences may deny potential residents admission based on their use of prescribed buprenorphine. Individuals and families seeking recovery from opioid use disorder should be aware of such potential barriers to accessing recovery residences. It is important for those seeking recovery for themselves or others to be aware of recovery residence policies beforehand to identify facilities that accept medications for opioid use disorder without restrictive conditions. This could entail perusing residences’ websites (if possible), contacting the National Alliance for Recovery Residences affiliates to locate certified facilities (that comply with federal guidelines), and/or contacting residences directly. It may also be necessary for those seeking recovery for themselves or others advocate for their individual needs to ensure they receive care that is best for them.
For treatment professionals and treatment systems: The present study suggests that recovery residences in South Florida may deny potential residents admission based on their use of prescribed buprenorphine. This may be due to misperceptions of the efficacy of buprenorphine and/or stigma towards opioid use disorder medications. Therefore, it is important for those working within recovery residences to ensure policies align with evidence-based practices and federal guidelines. Furthermore, it may be necessary to provide ongoing training to address stigma and misinformation about medications for opioid use disorder, including the misconception that medications for opioid use disorder are analogous to recreational drugs.
For scientists: Scientists would do well to expand upon the present work and explore potential reasons why recovery residences may be denying admission based on buprenorphine prescription. For example, research studies could investigate the role of stigma, misinformation, and/or organizational culture within recovery residences on admission policies. Additionally, research could explore the impact of how admission policies specific to medication for opioid use disorder prescription impact patient outcomes (e.g., relapse rates, treatment retention, and overdose risk). Researchers could also develop, and test interventions aimed at reducing stigma toward medications like buprenorphine among recovery residence staff and leadership. Finally, longitudinal studies assessing the experiences of individuals using medications like buprenorphine in recovery residences could provide valuable insights into how to create inclusive, evidence-based environments that support long-term recovery.
For policy makers: The present study suggests that despite potentially being in violation of federal law, recovery residences in South Florida are denying admission to individuals taking buprenorphine for opioid use disorder. This suggests that certifying organizations, such as the National Alliance for Recovery Residences, might enhance oversight by conducting regular audits of recovery residences and revoking certifications from facilities that deny admission based on opioid disorder medication use. Additionally, this work suggests that policymakers may consider mandating that recovery residences receiving federal or state funding demonstrate adherence to best-policies in treating substance use disorder (i.e., supporting use of medications such as buprenorphine).
In 2022, 81,806 people died due to opioid-involved overdose. The impact of the overdose epidemic has been uneven across the US with states such as Florida exceeding the national averages in opioid overdose deaths. Medications for opioid use disorder (e.g., buprenorphine, often prescribed in formulation with naloxone known by the brand name Suboxone) are effective at reducing the risk of overdose and improving opioid use over time. Research regarding ways to augment the benefits of opioid use disorder medications, with both professional-clinical and non-professional recovery supports, are ongoing. While research suggests cognitive-behavioral therapy may not improve on buprenorphine’s benefits, community-based mutual-help group participation (e.g., in Narcotics Anonymous) is associated with improved outcomes. In addition, recovery residences may be particularly valuable resources; research on Oxford House recovery residences suggest they improve substance use outcomes and are cost-effective.
Recovery residences (sometimes also called sober living homes) provide a safe living environment in which individuals can begin to transition back to their daily lives. The characteristics of recovery residences are variable, offering different lengths of stay, levels of monitoring and support, and have different requirements (e.g., for mutual-help attendance and employment). Overall, recovery residences are categorized into 1 of 4 levels based on services provided (see figure below) with level 1 homes being peer-run and offering minimal services to level 4 being closer to a institutional environment.
Rules and regulations for recovery residences vary widely. Despite organizations such as the National Alliance for Recovery Residences providing certification and guidance for recovery residence operations, the day-to-day operations of residences is at the discretion of individual residence owners/operators. This can become problematic as some of these operators have misconceptions about medications for opioid use disorder (e.g., that such medications are “replacing one drug for another” and are therefore not helpful). This has resulted in some seeking care at recovery residences being denied access due to taking medications for opioid use disorder. This is noteworthy given that, technically, federal guidelines prohibit this kind of discrimination.
It is unclear how common recovery residence admission is denied due to opioid disorder medication use. To examine this question, the present study investigated the buprenorphine policies of recovery residences in South Florida, an area with high density of residential treatment programs and common continuing care options like recovery residences.
HOW WAS THIS STUDY CONDUCTED?
This was a quantitative cross-sectional descriptive study in which the research team contacted recovery residences listed in the Florida Association of Recovery Residences directory. The primary goal was to determine if recovery residences in South Florida accepted individuals currently prescribed buprenorphine. Descriptive statistics were used to characterize the outcome of inquiries into admission at recovery residences. The study also examined if any restrictions were placed on such admissions of those prescribed buprenorphine (e.g., dosage limitations).
The authors downloaded the contact information for a list of recovery residences posted publicly on the Florida Association of Recovery Residences website. This resulted in a list of 141 Florida Association of Recovery Residences certified recovery residences. Researchers contacted recovery residences during business hours (between 8 AM and 6 PM Monday – Friday). When speaking to residence staff researchers followed a script where they pretended to be a person with an opioid use disorder prescribed buprenorphine who was seeking admission to the recovery residence. The scripted call included the following questions: “Hi, good morning/afternoon/evening. How are you? My name is ____. I am calling to find out a bit more information about your program. Is it okay if I ask some questions?” and “I am super excited to get my life on track. I recently just went into recovery, and I am taking buprenorphine 8 mg two times a day. Do you accept people taking buprenorphine into your program?”. If the residence staff indicated they either did not or conditionally allowed residents to take buprenorphine, the research team member inquired further with: “Okay, can you clarify for me why you do not accept individuals taking buprenorphine? I am no longer currently using any street drugs.” Responses on specific policies, including dose limitations, tapering requirements, and necessary documentation from providers were recorded. Researchers did not ask residence staff members to disclose any personal information (e.g., names). Each facility was contacted up to 3 times before being excluded from analyses.
All facilities were contacted between July 15, 2022 and December 30, 2022. The research team randomly contacted recovery residences until they reached 100 total (71% of the 141 certified in Florida) were contacted. Of the facilities reached, most (67%) were in Palm Beach County, followed by Broward County (31%) and Miami-Dade County (2%). Most were designated as level 2 (55%) followed by level 4 (26%), level 1 (14%), and level 3 (5%).
WHAT DID THIS STUDY FIND?
Most recovery residences denied access due to buprenorphine prescription
Of the 100 residences contacted, 53 did not accept residents if they were prescribed buprenorphine (regardless of dosage). The remaining residences either permitted individuals taking buprenorphine on a conditional basis (31 of 100; see below for specific conditions) or allowed admission regardless of buprenorphine prescription (16 of 100).
Conditional admission due to buprenorphine prescription varied widely across residences
Of the 31 residences with conditional acceptance of individuals taking buprenorphine, 8 (25.8%) required individuals to completely taper off buprenorphine (no data on taper timeframe were collected), 12 (38.7 %) allowed a maximum buprenorphine dosage of 8 mg daily, 4 (12.9 %) had a maximum 12 mg daily dosage, 2 (6.5 %) had a maximum 16 mg daily dosage, and 2 (6.5%) required a provider letter for admission. The remaining 3 (9.7%) residences did not to disclose their conditional admission policies.
Differences in admission policies did not vary by recovery residence county or level
No significant differences were found in recovery residence policies based on where the residences were located (county) or level. Though descriptively, level 4 facilities – which are typically part of larger clinical organizations – had higher levels of conditional acceptance than facilities with other levels (see figure below).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that recovery residences are denying admission to potential residents based on being prescribed the agonist medication buprenorphine for opioid use disorder. Of the recovery residences contacted by research staff, only 16% allowed individuals taking buprenorphine regardless of dosage. The remaining residences either barred admission entirely or only admitted those taking buprenorphine on a conditional basis (e.g., after tapering off). While data were not collected on the nature of the conditional taper, tacitly encouraging patients to taper off buprenorphine – by making residence contingent on such a taper – is likely to produce harms.
At the same time, some consider that there can be other types of concerns regarding buprenorphine’s risks. As an agonist that can produce euphoria and be intoxicating, it is prone to diversion. Relatedly, some individuals starting a recovery attempt who are not taking buprenorphine and do not want to take it may find that the presence of this medication (or any medication with psychoactive properties) triggers drug cravings. Another policy option, therefore, might support access both to recovery residences that serve individuals who take agonist medications and also to recovery residences where people would not be exposed to agonists like buprenorphine. The types of residences could be clearly designated. To be sure, such an option would not be without controversy – there would be many nuances to address. Given the empirical support for buprenorphine as well as worries about the risks of buprenorphine among some individuals seeking recovery, all in context of the public health need to address opioid use disorder, increased availability of person-centered options may help engage and attract the largest possible number of individuals that need it to recovery residences.
This all being said, it is unclear how representative the sample was in the present research. At the time of the publication of this study, the authors report there were 2042 recovery residences in Florida. However, the present study only contacted 100 total recovery residences (~5% of the residences in Florida). This small sample may not provide the most accurate view of the state of recovery residences in South Florida.
It is unclear how representative the sample was in the present research. At the time of the publication of this study the authors report there were 2042 recovery residences in Florida. However, the present study only contacted 100 total recovery residences (~5% of the residences in Florida). This small sample may not provide the most accurate view of the state of recovery residences in South Florida.
Admission policy information collected was limited to the knowledge of staff members who answered the phone at each recovery residence. The authors state that they were unable to obtain verification of policies from other sources. It is possible that information provided by residence staff was inaccurate.
BOTTOM LINE
Results of this study suggest that individuals taking buprenorphine have reduced access to recovery residences in South Florida. Results of this study found that 53% of contacted recovery residences deny admission to those prescribed buprenorphine. Additionally, 31% of recovery residences had conditional buprenorphine policies, including requiring potential residents to taper off buprenorphine. Tacitly encouraging individuals to discontinue buprenorphine (i.e., by requiring taper to obtain residence) can increase risk of relapse and potential overdose. Residences affiliated with clinical providers (Level IV) may be more accepting of individuals taking medications. Although the present study did not explore why such policies were in place, it is possible that stigma towards/misinformation about buprenorphine among staff and leadership may be a reason. It is critical for more research to be conducted investigating possible reasons for such policies and how barriers to access can be addressed.
For individuals and families seeking recovery: The present study suggests that recovery residences may deny potential residents admission based on their use of prescribed buprenorphine. Individuals and families seeking recovery from opioid use disorder should be aware of such potential barriers to accessing recovery residences. It is important for those seeking recovery for themselves or others to be aware of recovery residence policies beforehand to identify facilities that accept medications for opioid use disorder without restrictive conditions. This could entail perusing residences’ websites (if possible), contacting the National Alliance for Recovery Residences affiliates to locate certified facilities (that comply with federal guidelines), and/or contacting residences directly. It may also be necessary for those seeking recovery for themselves or others advocate for their individual needs to ensure they receive care that is best for them.
For treatment professionals and treatment systems: The present study suggests that recovery residences in South Florida may deny potential residents admission based on their use of prescribed buprenorphine. This may be due to misperceptions of the efficacy of buprenorphine and/or stigma towards opioid use disorder medications. Therefore, it is important for those working within recovery residences to ensure policies align with evidence-based practices and federal guidelines. Furthermore, it may be necessary to provide ongoing training to address stigma and misinformation about medications for opioid use disorder, including the misconception that medications for opioid use disorder are analogous to recreational drugs.
For scientists: Scientists would do well to expand upon the present work and explore potential reasons why recovery residences may be denying admission based on buprenorphine prescription. For example, research studies could investigate the role of stigma, misinformation, and/or organizational culture within recovery residences on admission policies. Additionally, research could explore the impact of how admission policies specific to medication for opioid use disorder prescription impact patient outcomes (e.g., relapse rates, treatment retention, and overdose risk). Researchers could also develop, and test interventions aimed at reducing stigma toward medications like buprenorphine among recovery residence staff and leadership. Finally, longitudinal studies assessing the experiences of individuals using medications like buprenorphine in recovery residences could provide valuable insights into how to create inclusive, evidence-based environments that support long-term recovery.
For policy makers: The present study suggests that despite potentially being in violation of federal law, recovery residences in South Florida are denying admission to individuals taking buprenorphine for opioid use disorder. This suggests that certifying organizations, such as the National Alliance for Recovery Residences, might enhance oversight by conducting regular audits of recovery residences and revoking certifications from facilities that deny admission based on opioid disorder medication use. Additionally, this work suggests that policymakers may consider mandating that recovery residences receiving federal or state funding demonstrate adherence to best-policies in treating substance use disorder (i.e., supporting use of medications such as buprenorphine).
In 2022, 81,806 people died due to opioid-involved overdose. The impact of the overdose epidemic has been uneven across the US with states such as Florida exceeding the national averages in opioid overdose deaths. Medications for opioid use disorder (e.g., buprenorphine, often prescribed in formulation with naloxone known by the brand name Suboxone) are effective at reducing the risk of overdose and improving opioid use over time. Research regarding ways to augment the benefits of opioid use disorder medications, with both professional-clinical and non-professional recovery supports, are ongoing. While research suggests cognitive-behavioral therapy may not improve on buprenorphine’s benefits, community-based mutual-help group participation (e.g., in Narcotics Anonymous) is associated with improved outcomes. In addition, recovery residences may be particularly valuable resources; research on Oxford House recovery residences suggest they improve substance use outcomes and are cost-effective.
Recovery residences (sometimes also called sober living homes) provide a safe living environment in which individuals can begin to transition back to their daily lives. The characteristics of recovery residences are variable, offering different lengths of stay, levels of monitoring and support, and have different requirements (e.g., for mutual-help attendance and employment). Overall, recovery residences are categorized into 1 of 4 levels based on services provided (see figure below) with level 1 homes being peer-run and offering minimal services to level 4 being closer to a institutional environment.
Rules and regulations for recovery residences vary widely. Despite organizations such as the National Alliance for Recovery Residences providing certification and guidance for recovery residence operations, the day-to-day operations of residences is at the discretion of individual residence owners/operators. This can become problematic as some of these operators have misconceptions about medications for opioid use disorder (e.g., that such medications are “replacing one drug for another” and are therefore not helpful). This has resulted in some seeking care at recovery residences being denied access due to taking medications for opioid use disorder. This is noteworthy given that, technically, federal guidelines prohibit this kind of discrimination.
It is unclear how common recovery residence admission is denied due to opioid disorder medication use. To examine this question, the present study investigated the buprenorphine policies of recovery residences in South Florida, an area with high density of residential treatment programs and common continuing care options like recovery residences.
HOW WAS THIS STUDY CONDUCTED?
This was a quantitative cross-sectional descriptive study in which the research team contacted recovery residences listed in the Florida Association of Recovery Residences directory. The primary goal was to determine if recovery residences in South Florida accepted individuals currently prescribed buprenorphine. Descriptive statistics were used to characterize the outcome of inquiries into admission at recovery residences. The study also examined if any restrictions were placed on such admissions of those prescribed buprenorphine (e.g., dosage limitations).
The authors downloaded the contact information for a list of recovery residences posted publicly on the Florida Association of Recovery Residences website. This resulted in a list of 141 Florida Association of Recovery Residences certified recovery residences. Researchers contacted recovery residences during business hours (between 8 AM and 6 PM Monday – Friday). When speaking to residence staff researchers followed a script where they pretended to be a person with an opioid use disorder prescribed buprenorphine who was seeking admission to the recovery residence. The scripted call included the following questions: “Hi, good morning/afternoon/evening. How are you? My name is ____. I am calling to find out a bit more information about your program. Is it okay if I ask some questions?” and “I am super excited to get my life on track. I recently just went into recovery, and I am taking buprenorphine 8 mg two times a day. Do you accept people taking buprenorphine into your program?”. If the residence staff indicated they either did not or conditionally allowed residents to take buprenorphine, the research team member inquired further with: “Okay, can you clarify for me why you do not accept individuals taking buprenorphine? I am no longer currently using any street drugs.” Responses on specific policies, including dose limitations, tapering requirements, and necessary documentation from providers were recorded. Researchers did not ask residence staff members to disclose any personal information (e.g., names). Each facility was contacted up to 3 times before being excluded from analyses.
All facilities were contacted between July 15, 2022 and December 30, 2022. The research team randomly contacted recovery residences until they reached 100 total (71% of the 141 certified in Florida) were contacted. Of the facilities reached, most (67%) were in Palm Beach County, followed by Broward County (31%) and Miami-Dade County (2%). Most were designated as level 2 (55%) followed by level 4 (26%), level 1 (14%), and level 3 (5%).
WHAT DID THIS STUDY FIND?
Most recovery residences denied access due to buprenorphine prescription
Of the 100 residences contacted, 53 did not accept residents if they were prescribed buprenorphine (regardless of dosage). The remaining residences either permitted individuals taking buprenorphine on a conditional basis (31 of 100; see below for specific conditions) or allowed admission regardless of buprenorphine prescription (16 of 100).
Conditional admission due to buprenorphine prescription varied widely across residences
Of the 31 residences with conditional acceptance of individuals taking buprenorphine, 8 (25.8%) required individuals to completely taper off buprenorphine (no data on taper timeframe were collected), 12 (38.7 %) allowed a maximum buprenorphine dosage of 8 mg daily, 4 (12.9 %) had a maximum 12 mg daily dosage, 2 (6.5 %) had a maximum 16 mg daily dosage, and 2 (6.5%) required a provider letter for admission. The remaining 3 (9.7%) residences did not to disclose their conditional admission policies.
Differences in admission policies did not vary by recovery residence county or level
No significant differences were found in recovery residence policies based on where the residences were located (county) or level. Though descriptively, level 4 facilities – which are typically part of larger clinical organizations – had higher levels of conditional acceptance than facilities with other levels (see figure below).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that recovery residences are denying admission to potential residents based on being prescribed the agonist medication buprenorphine for opioid use disorder. Of the recovery residences contacted by research staff, only 16% allowed individuals taking buprenorphine regardless of dosage. The remaining residences either barred admission entirely or only admitted those taking buprenorphine on a conditional basis (e.g., after tapering off). While data were not collected on the nature of the conditional taper, tacitly encouraging patients to taper off buprenorphine – by making residence contingent on such a taper – is likely to produce harms.
At the same time, some consider that there can be other types of concerns regarding buprenorphine’s risks. As an agonist that can produce euphoria and be intoxicating, it is prone to diversion. Relatedly, some individuals starting a recovery attempt who are not taking buprenorphine and do not want to take it may find that the presence of this medication (or any medication with psychoactive properties) triggers drug cravings. Another policy option, therefore, might support access both to recovery residences that serve individuals who take agonist medications and also to recovery residences where people would not be exposed to agonists like buprenorphine. The types of residences could be clearly designated. To be sure, such an option would not be without controversy – there would be many nuances to address. Given the empirical support for buprenorphine as well as worries about the risks of buprenorphine among some individuals seeking recovery, all in context of the public health need to address opioid use disorder, increased availability of person-centered options may help engage and attract the largest possible number of individuals that need it to recovery residences.
This all being said, it is unclear how representative the sample was in the present research. At the time of the publication of this study, the authors report there were 2042 recovery residences in Florida. However, the present study only contacted 100 total recovery residences (~5% of the residences in Florida). This small sample may not provide the most accurate view of the state of recovery residences in South Florida.
It is unclear how representative the sample was in the present research. At the time of the publication of this study the authors report there were 2042 recovery residences in Florida. However, the present study only contacted 100 total recovery residences (~5% of the residences in Florida). This small sample may not provide the most accurate view of the state of recovery residences in South Florida.
Admission policy information collected was limited to the knowledge of staff members who answered the phone at each recovery residence. The authors state that they were unable to obtain verification of policies from other sources. It is possible that information provided by residence staff was inaccurate.
BOTTOM LINE
Results of this study suggest that individuals taking buprenorphine have reduced access to recovery residences in South Florida. Results of this study found that 53% of contacted recovery residences deny admission to those prescribed buprenorphine. Additionally, 31% of recovery residences had conditional buprenorphine policies, including requiring potential residents to taper off buprenorphine. Tacitly encouraging individuals to discontinue buprenorphine (i.e., by requiring taper to obtain residence) can increase risk of relapse and potential overdose. Residences affiliated with clinical providers (Level IV) may be more accepting of individuals taking medications. Although the present study did not explore why such policies were in place, it is possible that stigma towards/misinformation about buprenorphine among staff and leadership may be a reason. It is critical for more research to be conducted investigating possible reasons for such policies and how barriers to access can be addressed.
For individuals and families seeking recovery: The present study suggests that recovery residences may deny potential residents admission based on their use of prescribed buprenorphine. Individuals and families seeking recovery from opioid use disorder should be aware of such potential barriers to accessing recovery residences. It is important for those seeking recovery for themselves or others to be aware of recovery residence policies beforehand to identify facilities that accept medications for opioid use disorder without restrictive conditions. This could entail perusing residences’ websites (if possible), contacting the National Alliance for Recovery Residences affiliates to locate certified facilities (that comply with federal guidelines), and/or contacting residences directly. It may also be necessary for those seeking recovery for themselves or others advocate for their individual needs to ensure they receive care that is best for them.
For treatment professionals and treatment systems: The present study suggests that recovery residences in South Florida may deny potential residents admission based on their use of prescribed buprenorphine. This may be due to misperceptions of the efficacy of buprenorphine and/or stigma towards opioid use disorder medications. Therefore, it is important for those working within recovery residences to ensure policies align with evidence-based practices and federal guidelines. Furthermore, it may be necessary to provide ongoing training to address stigma and misinformation about medications for opioid use disorder, including the misconception that medications for opioid use disorder are analogous to recreational drugs.
For scientists: Scientists would do well to expand upon the present work and explore potential reasons why recovery residences may be denying admission based on buprenorphine prescription. For example, research studies could investigate the role of stigma, misinformation, and/or organizational culture within recovery residences on admission policies. Additionally, research could explore the impact of how admission policies specific to medication for opioid use disorder prescription impact patient outcomes (e.g., relapse rates, treatment retention, and overdose risk). Researchers could also develop, and test interventions aimed at reducing stigma toward medications like buprenorphine among recovery residence staff and leadership. Finally, longitudinal studies assessing the experiences of individuals using medications like buprenorphine in recovery residences could provide valuable insights into how to create inclusive, evidence-based environments that support long-term recovery.
For policy makers: The present study suggests that despite potentially being in violation of federal law, recovery residences in South Florida are denying admission to individuals taking buprenorphine for opioid use disorder. This suggests that certifying organizations, such as the National Alliance for Recovery Residences, might enhance oversight by conducting regular audits of recovery residences and revoking certifications from facilities that deny admission based on opioid disorder medication use. Additionally, this work suggests that policymakers may consider mandating that recovery residences receiving federal or state funding demonstrate adherence to best-policies in treating substance use disorder (i.e., supporting use of medications such as buprenorphine).