
Active strategies to enhance young adults’ medication adherence also reduce opioid use
The opioid use disorder medication, extended-release naltrexone, protects against a return to opioid use. Yet, it is often difficult to initiate and sustain use of medication, especially for youth and young adults. This randomized controlled trial examined whether an intervention consisting of multiple strategies to enhance medication adherence increased receipt of medication and improved opioid use outcomes among young adults after residential treatment.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Empirically-supported medicines can support recovery from opioid use disorder (OUD) by increasing an individual’s ability to engage and stay in treatment, protecting against opioid use, and by reducing risk for adverse consequences such as overdose. Individuals with an OUD who remain in treatment and receive the planned dose of medication have better outcomes.
One such medication, extended-release depot injection naltrexone (also known and marketed by the brand name Vivitrol), is considered especially helpful as it reduces barriers to accessing treatment by allowing individuals to make monthly clinic visits (versus daily or weekly). Yet, despite reducing one barrier to access that supports some populations in receiving medication, youth and young adult patients often do not initiate or persist in these treatments. Examining which components of clinical interventions will work to increase treatment retention may also help achieve better recovery outcomes. To address these gaps, this pilot study compared individuals receiving standard care with individuals receiving a multicomponent intervention, comprised of several evidence-based strategies (family treatment, assertive outreach, home delivery, contingency management) to see whether the multicomponent intervention could increase treatment retention and improve substance use outcomes.
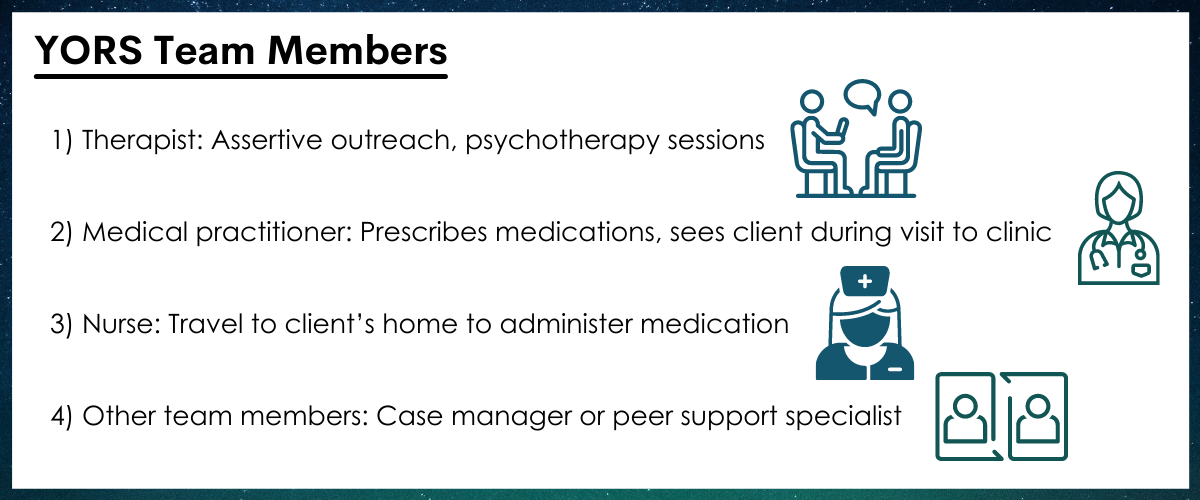
Figure 1.
HOW WAS THIS STUDY CONDUCTED?
This was a pilot randomized controlled trial with 41 emerging adults (ages 18-26) diagnosed with opioid use disorder in inpatient treatment at a community substance use disorder treatment center in Baltimore, MD. The study involved randomizing participants interested in receiving medication treatment during outpatient treatment (following their inpatient treatment) to two groups, one which received standard treatment (TAU) and the other which received a multi component intervention (YORS) for 24 weeks. The study aimed to assess differences between the two groups in the number of medication doses received and in return to opioid use. Patients with unstable medical or psychiatric disorders were excluded from the study. Due to study dropout or prolonged incarceration, only 38 participants were included in the analysis.
All participants received an initial first dose of extended-release naltrexone before they were discharged from inpatient treatment. The Standard Treatment (TAU) group received standard referrals to continuing substance use disorder care, including extended-release naltrexone received at a doctor’s office. The Intervention (YORS) condition included four parts: (1) Home delivery of medication + counseling, (2) Family component, (3) Contingency management (monetary incentive for each received dose), and (4) Assertive outreach and ongoing contact from treatment providers to the patient and a chosen family member, called a “treatment significant other”. The family component included OUD education, treatment planning, and a written family plan.
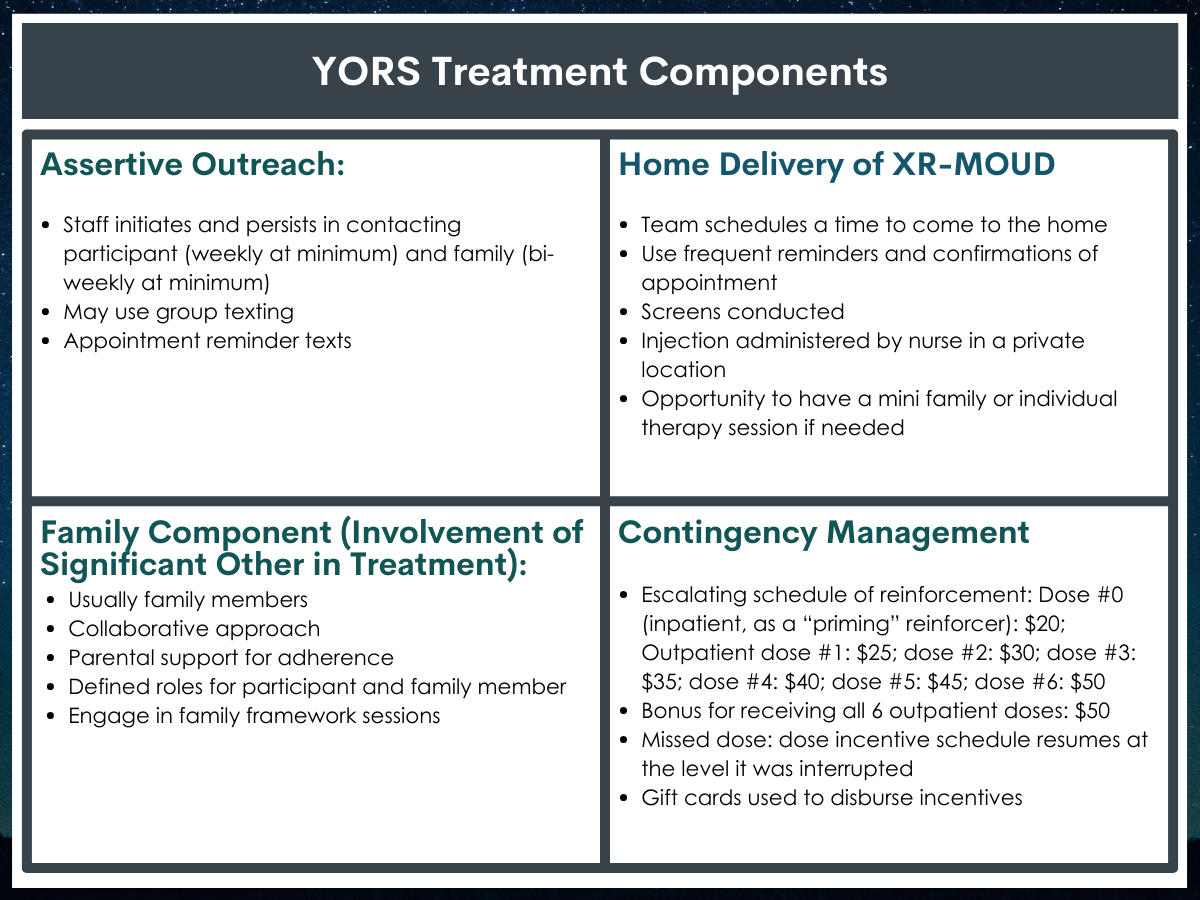
Figure 2.
Participants were followed for a 6-month period. During this period, they answered questions on their substance use and provided urine screens every 2 weeks. Treatment service usage data were collected from the clinics. The 2 primary outcomes were the (1) total number of doses received (out of the 7 possible including the dose received at end of inpatient stay) and (2) relapse to opioid use over 24 weeks. A relapse to use was considered use of opioids for 10 or more days within a 4-week period. Each missing or positive urine screen was entered as positive for 5 days of opioid use per each 2-week period. Other outcomes the authors examined included the number of days of opioid use, opioid abstinence, other substance use, and readmittance to treatment.
This study sample included 41(38 participants were eligible and included in the analysis) emerging adults in Baltimore, MD, who were seeking treatment for OUD; on average participants were 23 years of age; roughly two-thirds were male (65%) and most were on Medicaid (84%). The majority of participants designated a parent (81%) as their treatment significant other, while the remaining had other family members, a romantic partner, or sponsor/mentor.
WHAT DID THIS STUDY FIND?
Intervention participants had higher levels of treatment engagement compared to standard treatment.
Participants in the intervention group (YORS) received 4.3 doses of medication whereas those in the standard treatment group (TAU) only received 0.70 (i.e., less than 1 dose per participant, on average).
Participants in the intervention group (YORS) remained in outpatient treatment for a median (i.e., 50th percentile) of 9 weeks whereas those in the standard treatment group (TAU) remained in outpatient treatment for only 3 weeks. These findings indicate that only participants in the intervention (YORS) group were likely to continue in outpatient treatment until (and following) their second dose of medication.
Intervention participants had lower return to opioid use rates at 24 weeks than standard treatment participants, but levels of abstinence did not differ between groups.
Intervention (YORS) participants were significantly less likely to relapse (i.e., use of opioids for 10 or more days within a 4-week period) than standard treatment (TAU) participants: 61% versus 95%.
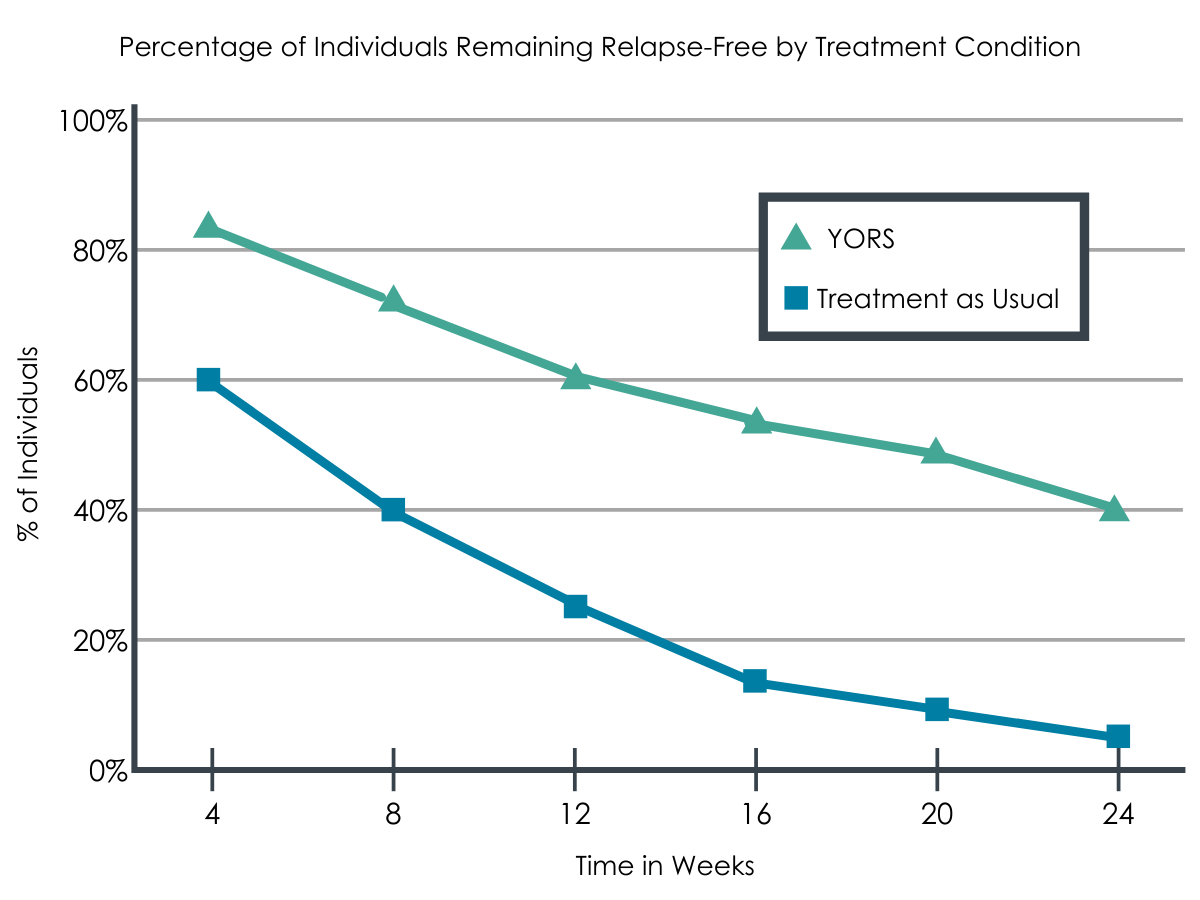
Figure 3.
Overall, as medication use increased, opioid relapse and overall days of use decreased, yet there were no differences between the groups in time to first opioid use or in rates of complete opioid abstinence over the course of the entire 24-week follow-up. Only 1 participant stayed completely abstinent until 24 weeks.
1/3 were readmitted to inpatient treatment.
About 37% of participants were readmitted to inpatient treatment during the study, although this did not significantly differ between the two groups (9 YORS, 5 TAU).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Through this study, the researchers demonstrated that the multicomponent intervention, which included home delivery of medication and counseling, a family component, contingency management, and assertive outreach resulted in significantly more medication doses than standard treatment. As well, members of this multicomponent group were retained in treatment longer and had a significantly lower rate of return to opioids during the course of the study. These findings support the approach of offering young adults a comprehensive and diverse set of outpatient supports after an initial bout of inpatient treatment: Incorporating significant others, such as family, may be a key component to success in a multi-component intervention. Although the study cannot address which of these supports were most effective, the intervention components are all based on existing evidence; together, they may work in a way to build recovery capital that sole-component interventions may not be able to do. While this is an encouraging effect, the intervention approach was resource-intensive, and it is unclear the extent to which programs may be able to implement the intervention package in standard treatment. That said, if these effects are replicated in larger samples and are shown to be cost-effective, the extra effort involved could yield important recovery dividends for emerging adults.
Approximately 1/3 of participants returned to inpatient treatment during the study, following typical cycles of recovery among this age group and among those who use opioids; the authors suggest that the multicomponent group was more easily and quickly identified for a return to treatment, but this perception should be confirmed in additional, larger, studies of the intervention.
Despite these promising findings only one participant remained abstinent during the trial, suggesting further research into other barriers and facilitators for this age group may be necessary. Indeed, this is similar to other research, which suggests that the use of extended-release naltrexone does not work for everyone. As well, it is important to note that while extended-release naltrexone may be easier to adhere to for participants given it only requires a monthly dose, only its alternative, buprenorphine, is associated with reduced overdose risk.
- LIMITATIONS
-
- This was a small pilot study, and although the study was randomized, it could still mean the intervention groups differed in important ways that could have affected the estimated effects of the interventions.
- The small sample may also mean that the estimate of the benefits of the intervention may be unstable. Findings may also not generalize to broader or more diverse populations of young adults or to other age groups.
- This study utilized a variety of treatment components, so it is difficult to understand which ones in particular were the most important in contributing to the observed benefits (i.e., mechanisms of behavior change). It is also unclear how feasible it may be to implement this treatment package in real-world settings.
- There was a greater degree of missing urine screen data from the standard treatment (TAU) versus the intervention (YORS) groups (60% and 26%, respectively), and since missing data were entered as positive for drug use for the analysis (as is typically done), the analysis nevertheless could have been biased to favor the intervention (YORS) group
- The extent of family incorporation throughout the trial, while described as an important component of the intervention, is unclear; that is, although family members may have been involved, the study did not capture to what degree the families were involved beyond the average number of family sessions or how the young adult participants perceived the involvement. It seems possible that some participants succeeded in the trial because their families were more supportive than others.
BOTTOM LINE
In this study, the research team used a randomized controlled trial with young adults in a community SUD residential treatment program and found that a multicomponent intervention produced greater treatment continuing care retention in terms of number of doses received and duration of weeks in outpatient treatment, and lower likelihood of relapse (defined in this study as 10 days of opioid use in a 4-week period) compared to standard treatment. However, the study also highlights the difficult nature of retaining young adults in OUD treatment, even with some of the primary barriers removed through home delivery and monthly (versus daily) dosing and some evidence-based supports incorporated (family involvement, assertive outreach). Overall, this looks to be a promising approach worthy of further study.
- For individuals and families seeking recovery: Recovery from an OUD is a difficult process and one that can require many sources of tangible and intangible support (recovery capital). Although using extended-release opioid antagonist medication treatment (i.e., naltrexone) can be highly effective, it is only effective if individuals receive it and there may be a variety of barriers to returning to receive the medication, including shame or stigma, or more practical barriers such as ensuring transportation to the clinic. Understanding that those barriers exist and working with a family member to help identify and problem-solve these issues may be one way that families can actively support one’s recovery journey.
- For treatment professionals and treatment systems: This study incorporated a variety of components and it seems likely that some of these aspects might be feasible to implement in standard practice if youth and their families are willing. The study authors included as a supplement their treatment manual that provided additional descriptive details about the study so that those interested in learning from their experience could do so. In this document they describe the positive leverage that family members can provide, especially when their support is identified early and agreed to with the participant in a family letter or contract. Alternatively, some research suggests that including peer outreach workers is an effective tool and may be more effective for this age group; this may be another option to provide to individuals.
- For scientists: Although this study examines several components of evidence-based treatments, there is more research needed to address which of these components are most effective and if there are certain aspects that need to be modified to better reach this particular population. As well, additional research with a larger sample size and for a longer period of time is important to understanding whether these effects will generalize. Fortunately, the study authors included their treatment manual as a supplement that provides additional descriptive details about the study so that those interested in replicating or extending the study could do so.
- For policy makers: Although this study examines a variety of individual and interpersonal factors in treatment retention, there may be larger, structural factors to address such as by implementing statewide policies. For example, policies can increase access to treatment coverage by reducing financial barriers. Other policies could help ensure adequate training and increase provider capacity so that individuals can access treatment in a timely manner and without encountering additional logistical barriers (location, transportation, etc.). As well, funding research that allows an examination of barriers to treatment as well as specific mechanisms of behavior change of opioid use disorder treatment for emerging adults may shed more light on how to address this pervasive issue.
CITATIONS
Fishman, M., Wenzel, K., Vo, H., Wildberger, J., & Burgower, R. (2021). A pilot randomized controlled trial of assertive treatment including family involvement and home delivery of medication for young adults with opioid use disorder. Addiction, 116(3), 548-557. DOI: 10.1111/add.15181
