Does adding phone check-ins and digital recovery support services to conventional alcohol use disorder treatment improve outcomes?
Ongoing patient support after formal addiction treatment produces better outcomes than treatment on its own. This ongoing support, called “continuing care”, has traditionally been delivered through in-person or remote check-ins with providers. Continuing care can also be delivered through innovative smartphone apps that do not rely on live-time therapist interactions. This study compared traditional telephone-based continuing care, a modern smartphone app, and a combination of the two on alcohol use disorder patient outcomes after treatment.
Individuals with alcohol use disorder typically require continuing care to achieve stable remission. There are however numerous barriers that impede individuals’ access to continuing care, such as employment or family responsibilities, limited access to transportation, illness or disabilities, and for some, geographic isolation.
In this study, the researchers compared cognitive behavioral therapy-based telephone monitoring and counseling, ACHESS, and the integrated combination of both interventions to intensive outpatient programs (commonly referred to as IOPs) to determine if these continuing care add-ons improve alcohol use disorder outcomes over treatment as usual. This study also examined whether telephone monitoring and counseling, ACHESS, or the combination of these interventions were superior to one another.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized controlled trial with 262 participants who received either telephone monitoring and counseling + treatment as usual, ACHESS + treatment as usual, the integrated combination of both interventions + treatment as usual, or treatment as usual only over a 12-month period. Groups were compared during the 12-month treatment phase and at post-treatment follow-up (18 months post-baseline). The primary study outcome was percentage heavy drinking days over the 12-month treatment period. Secondary outcomes included percentage heavy drinking days at 18-month follow-up, any alcohol use within a given follow-up period (yes/no), any drug use (yes/no), and alcohol use related negative consequences and quality of life during study months 3, 6, 9, 12 and 18.
All participants received intensive outpatient treatment, which provided 9 hours of group counseling per week for up to 3 months, plus up to 3 months of weekly continuing care. For the treatment as usual group, this was the only treatment received.
Telephone monitoring and counseling included one initial in-person session with a counselor to establish a relationship. Telephone calls then occurred weekly in month 1, twice monthly in months 2–4, monthly in months 5–7, and every other month in months 8–12 for a total of 16 possible calls. Each call lasted 15–30 minutes. At the beginning of each call, participants completed a brief assessment of substance use, and risk and protective factors. Cognitive behavioral therapy-based counseling was provided based on the results of these assessments. Potential coping strategies and behaviors were practiced, and participants were reinforced for engagement in pro-recovery activities. Participants without reliable access to a telephone were given a smartphone.
The ACHESS app offered connections to online peer support, access to audio and written information on addiction, recovery related web links, global positioning system-driven information on mutual-help meetings, and inspirational messages. If needed, participants were provided with a smartphone and data plan. Study staff trained the participants to use the ACHESS app. ACHESS collected information on confidence for maintaining abstinence (daily) and on 10 risk and protective factors (weekly) via surveys delivered through the app. When data indicated that relapse risk was high, participants were encouraged via automatic text messages to seek additional support. Also, following 7 days of inactivity, ACHESS automatically sent a message to participants and alerted ACHESS support staff, who encouraged use of ACHESS via text messaging.
For the combined telephone monitoring and counseling and ACHESS group, telephone monitoring and counseling and ACHESS were provided. In addition, in the event a participant reported something clinically concerning through ACHESS, the telephone counselors received an alert. Counselors could also view a graph with current and past assessment scores in a clinician dashboard. The idea here was that these features would support faster outreach to patients when risk increased.
The primary outcome measure was percentage of days of heavy drinking (defined as 5 or more drinks/day for men, 4 or more drinks/day for women) during the 12-month treatment phase of the study. Secondary outcomes measured during study months 3, 6, 9, 12 and 18 months were: Percentage of days of heavy drinking at 18 months, any alcohol use within a given follow-up period (yes/no), any drug use within a given follow-up period (yes/no, as determined by self-report measures, and urine drug screens at 18-month follow-up), alcohol use related negative consequences measured by the short inventory of problems, and quality of life measured by the short form survey.
Participants were 262 adults recruited from four publicly funded intensive outpatient programs in Philadelphia, USA. To be included in the study, participants had to: 1) Have a Diagnostic and Statistical Manual of Mental Disorders-5 (DSM 5) diagnosis of current, moderate to severe alcohol use disorder, 2) have completed 3 weeks of an intensive outpatient treatment, 3) be aged 18–75 years, 4) have no current psychotic disorder or dementia, 5) have no acute medical problem requiring inpatient treatment, and 6) be not receiving other addiction treatment.
Participants, on average, were 47 years old, had 12 years of education. Most were male (71%), African American (82%) and never married (67%). Current co-occurring disorders included cocaine use disorder (39%), anxiety disorders (35%), and major depression (26%). Participants drank alcohol on 45% of the days in the 3 months prior to baseline, which included 3–4 weeks of intensive outpatient program.
WHAT DID THIS STUDY FIND?
Adherence to ACHESS app usage was generally better than for telephone monitoring and counseling.
In the ACHESS only group, participants used the ACHESS app an average of 20 days per month in months 1 and 2, but subsequently declined in usage to around14 days per month. In telephone monitoring and counseling + ACHESS group, ACHESS was used an average of 16 days per month in months 1 and 2 and subsequently declined to around 10 days per month for the remainder of the study.
The telephone monitoring and counseling group completed, on average, 8.1 counseling sessions, while the telephone monitoring and counseling + ACHESS group completed 10.7. Notably, among the participants who completed the in-person orientation session, counseling sessions were slightly better attended, with a mean of 10.2 in the telephone monitoring and counseling group and 11.0 in telephone monitoring and counseling + ACHESS group.
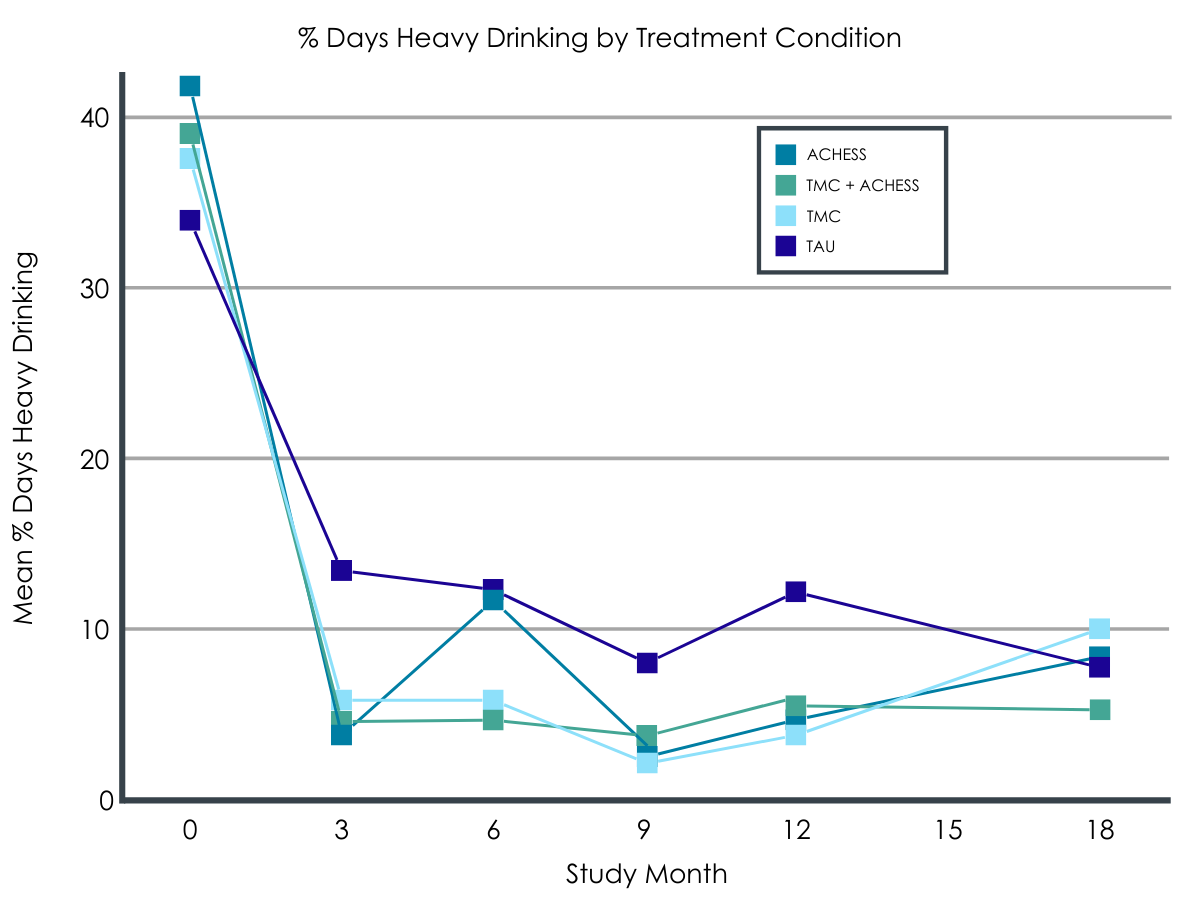
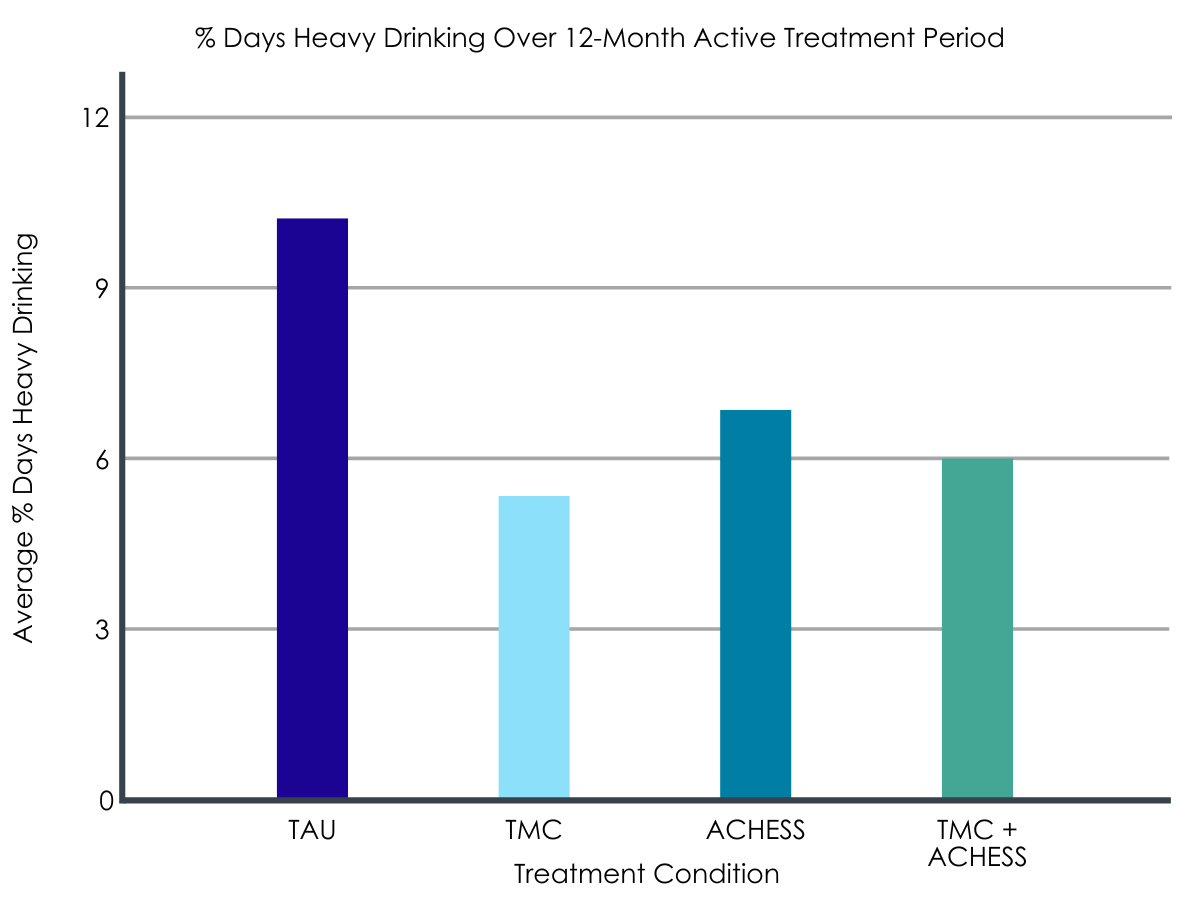
Telephone monitoring and counseling, ACHESS, and telephone monitoring and counseling + ACHESS all outperformed treatment as usual in terms of percentage of days of heavy drinking over the 12-month active treatment period.
Average percentage of days of heavy drinking in study months 1–12 was significantly lower in the three treatment groups compared to treatment as usual only group. Specifically, the telephone monitoring and counseling group had on average 5.4 percent days of heavy drinking, the ACHESS group 6.8, the combined telephone monitoring and counseling + ACHESS group had 6.0, while the treatment as usual only group had 10.3. However, none of the active treatments markedly outperformed the other in terms of percentage of days of heavy drinking.
Telephone monitoring and counseling, ACHESS, and telephone monitoring and counseling + ACHESS outperformed treatment as usual in terms of any drinking, but not drug use, negative consequences, or well-being.
Those in the treatment as usual group were 3 times more likely to drink any alcohol in study months 1–12 compared to the telephone monitoring and counseling group, and 2.4 times more likely to drink any alcohol than the telephone monitoring and counseling + ACHESS group. However, the treatment as usual group was not meaningfully more likely to drink than the ACHESS group, although in absolute terms, the treatment as usual group did more poorly on this measure.
In terms of other secondary study outcomes including drug use, negative consequences, and quality of life, there were no meaningful between group differences.
There were no between group differences at 18-month follow-up.
Groups were not meaningfully different on any of the primary or secondary study outcome measures at 18-month follow-up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study replicated findings from prior research which has found that telephone monitoring and counseling and ACHESS can improve alcohol use outcomes for individuals seeking recovery from alcohol use disorder when added to treatment as usual. In addition, this study was the first to compare these two approaches, and the first to determine whether combining these interventions improved outcomes over either intervention alone.
Although none of the interventions in this study added to treatment as usual (i.e., telephone monitoring and counseling, ACHESS, and their combination) performed markedly better than the other, findings are notable that all outperformed treatment as usual alone in terms of the primary study outcome – percentage days heavy drinking.
What is perhaps most notable among these findings is that a ‘therapist in the pocket app’, ACHESS, with minimal monitoring by trained personnel, performed about as well as more costly telephone monitoring and counseling. This is exciting, because it suggests that a relatively low cost, high-accessibility intervention might be enough to produce the improvements in drinking outcomes previously observed for more intensive and expensive counseling follow-up approaches.
At the same time, it’s important to note that the study groups were not markedly different in terms of drug use, negative consequences, or well-being over the 12-month treatment period, or on any study measure at 18-month follow-up. This highlights potential limitations of telephone monitoring and counseling, apps like ACHESS, and their combination, both during outpatient treatment, and over the longer-term. While the researchers’ findings suggest that patients seeking recovery from alcohol use disorder might experience better alcohol use outcomes with continued counseling or app use (e.g., continued use of these through the 18-month follow up might have showed benefits at this longer follow-up), these results may not be sustained when counseling or app use is discontinued as was found this study at the 18-month follow-up. Also, benefits related to reduced drug use, negative consequences, and improved well-being may not follow from these interventions. It could be that additional resources are needed to confer such benefits, especially for individuals with limited resources and recovery capital.
As noted by the researchers:
More than 80% of participants in this study were African American, which although representative of clients in treatment for substance use disorders in publicly funded programs in Philadelphia, USA, may not be representative of other treatment settings and locations. While there is no reason to believe that these effects would not generalize to other patient populations, different findings might be obtained in different patient populations and replication studies are needed.
Biological measures of drinking outcome were obtained only at the 18-month follow-up, meaning the researchers relied solely on self-report to assess drinking outcomes throughout the active treatment period of the study. Though there is no reason to suspect participants did not report any alcohol use accurately, self-report can be prone to certain kinds of biases.
Also:
The authors focused on percentage days heavy drinking and any drinking (yes/no). While these are important measures of alcohol use outcomes for people in treatment for alcohol use disorder, they don’t paint the full picture of alcohol use. Percentage days abstinent, for instance, is a commonly used measure that characterizes overall alcohol use over a monitoring period, which was not reported in this study.
BOTTOM LINE
Results from this randomized controlled trial indicate that adding telephone monitoring and counseling, ACHESS and the combination of telephone monitoring and counseling and ACHESS to intensive outpatient treatment reduced heavy drinking by approximately 50% over 12 months of active treatment. However, those receiving these interventions were not markedly different from those receiving treatment as usual only in terms of drug use, negative consequences, or well-being over the 12-month treatment period, and no meaningful differences were observed at 18-month follow-up occurring 6 months after the conclusion of treatment.
For individuals and families seeking recovery: The findings here build on previous studies showing follow-up care for individuals in substance use disorder treatment improves treatment outcomes. Results from this study suggest that telephone counseling and apps like ACHESS can enhance recovery outcomes when added to conventional outpatient treatment. Currently, follow-up counseling and support is not widely practiced in addiction treatment, except perhaps in some higher quality programs. When researching treatment program options, ask if follow-up care is provided. Additionally, apps like ACHESS will also likely confer benefit, whether used alone or in conjunction with follow-up counseling.
For treatment professionals and treatment systems: The researchers’ findings build on previous studies showing follow-up care for individuals in substance use disorder treatment improves treatment outcomes. Results from this study suggest that telephone counseling and apps like ACHESS can enhance recovery outcomes when added to conventional outpatient treatment. Adding follow-up counseling and support to treatment programs is likely to improve patient outcomes. Additionally, apps like ACHESS will also likely confer benefit, whether alone or in conjunction with follow-up counseling.
For scientists:The researchers’ findings build on previous studies showing follow-up care for individuals in substance use disorder treatment improves treatment outcomes. Results from this study suggest that telephone counseling and apps like ACHESS can enhance recovery outcomes when added to conventional outpatient treatment. More work is needed, however, to determine for whom, and under what conditions these supplemental interventions confer the most benefit.
For policy makers: The researchers’ findings build on previous studies showing follow-up care for individuals in substance use disorder treatment improves treatment outcomes. Results from this study suggest that telephone counseling and apps like ACHESS can enhance recovery outcomes when added to conventional outpatient treatment. Reducing barriers to follow-up care such as phone counseling and relapse prevention apps by requiring insurers to reimburse for these services will improve public health and reduce costs to healthcare systems in the long run.
Individuals with alcohol use disorder typically require continuing care to achieve stable remission. There are however numerous barriers that impede individuals’ access to continuing care, such as employment or family responsibilities, limited access to transportation, illness or disabilities, and for some, geographic isolation.
In this study, the researchers compared cognitive behavioral therapy-based telephone monitoring and counseling, ACHESS, and the integrated combination of both interventions to intensive outpatient programs (commonly referred to as IOPs) to determine if these continuing care add-ons improve alcohol use disorder outcomes over treatment as usual. This study also examined whether telephone monitoring and counseling, ACHESS, or the combination of these interventions were superior to one another.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized controlled trial with 262 participants who received either telephone monitoring and counseling + treatment as usual, ACHESS + treatment as usual, the integrated combination of both interventions + treatment as usual, or treatment as usual only over a 12-month period. Groups were compared during the 12-month treatment phase and at post-treatment follow-up (18 months post-baseline). The primary study outcome was percentage heavy drinking days over the 12-month treatment period. Secondary outcomes included percentage heavy drinking days at 18-month follow-up, any alcohol use within a given follow-up period (yes/no), any drug use (yes/no), and alcohol use related negative consequences and quality of life during study months 3, 6, 9, 12 and 18.
All participants received intensive outpatient treatment, which provided 9 hours of group counseling per week for up to 3 months, plus up to 3 months of weekly continuing care. For the treatment as usual group, this was the only treatment received.
Telephone monitoring and counseling included one initial in-person session with a counselor to establish a relationship. Telephone calls then occurred weekly in month 1, twice monthly in months 2–4, monthly in months 5–7, and every other month in months 8–12 for a total of 16 possible calls. Each call lasted 15–30 minutes. At the beginning of each call, participants completed a brief assessment of substance use, and risk and protective factors. Cognitive behavioral therapy-based counseling was provided based on the results of these assessments. Potential coping strategies and behaviors were practiced, and participants were reinforced for engagement in pro-recovery activities. Participants without reliable access to a telephone were given a smartphone.
The ACHESS app offered connections to online peer support, access to audio and written information on addiction, recovery related web links, global positioning system-driven information on mutual-help meetings, and inspirational messages. If needed, participants were provided with a smartphone and data plan. Study staff trained the participants to use the ACHESS app. ACHESS collected information on confidence for maintaining abstinence (daily) and on 10 risk and protective factors (weekly) via surveys delivered through the app. When data indicated that relapse risk was high, participants were encouraged via automatic text messages to seek additional support. Also, following 7 days of inactivity, ACHESS automatically sent a message to participants and alerted ACHESS support staff, who encouraged use of ACHESS via text messaging.
For the combined telephone monitoring and counseling and ACHESS group, telephone monitoring and counseling and ACHESS were provided. In addition, in the event a participant reported something clinically concerning through ACHESS, the telephone counselors received an alert. Counselors could also view a graph with current and past assessment scores in a clinician dashboard. The idea here was that these features would support faster outreach to patients when risk increased.
The primary outcome measure was percentage of days of heavy drinking (defined as 5 or more drinks/day for men, 4 or more drinks/day for women) during the 12-month treatment phase of the study. Secondary outcomes measured during study months 3, 6, 9, 12 and 18 months were: Percentage of days of heavy drinking at 18 months, any alcohol use within a given follow-up period (yes/no), any drug use within a given follow-up period (yes/no, as determined by self-report measures, and urine drug screens at 18-month follow-up), alcohol use related negative consequences measured by the short inventory of problems, and quality of life measured by the short form survey.
Participants were 262 adults recruited from four publicly funded intensive outpatient programs in Philadelphia, USA. To be included in the study, participants had to: 1) Have a Diagnostic and Statistical Manual of Mental Disorders-5 (DSM 5) diagnosis of current, moderate to severe alcohol use disorder, 2) have completed 3 weeks of an intensive outpatient treatment, 3) be aged 18–75 years, 4) have no current psychotic disorder or dementia, 5) have no acute medical problem requiring inpatient treatment, and 6) be not receiving other addiction treatment.
Participants, on average, were 47 years old, had 12 years of education. Most were male (71%), African American (82%) and never married (67%). Current co-occurring disorders included cocaine use disorder (39%), anxiety disorders (35%), and major depression (26%). Participants drank alcohol on 45% of the days in the 3 months prior to baseline, which included 3–4 weeks of intensive outpatient program.
WHAT DID THIS STUDY FIND?
Adherence to ACHESS app usage was generally better than for telephone monitoring and counseling.
In the ACHESS only group, participants used the ACHESS app an average of 20 days per month in months 1 and 2, but subsequently declined in usage to around14 days per month. In telephone monitoring and counseling + ACHESS group, ACHESS was used an average of 16 days per month in months 1 and 2 and subsequently declined to around 10 days per month for the remainder of the study.
The telephone monitoring and counseling group completed, on average, 8.1 counseling sessions, while the telephone monitoring and counseling + ACHESS group completed 10.7. Notably, among the participants who completed the in-person orientation session, counseling sessions were slightly better attended, with a mean of 10.2 in the telephone monitoring and counseling group and 11.0 in telephone monitoring and counseling + ACHESS group.
Telephone monitoring and counseling, ACHESS, and telephone monitoring and counseling + ACHESS all outperformed treatment as usual in terms of percentage of days of heavy drinking over the 12-month active treatment period.
Average percentage of days of heavy drinking in study months 1–12 was significantly lower in the three treatment groups compared to treatment as usual only group. Specifically, the telephone monitoring and counseling group had on average 5.4 percent days of heavy drinking, the ACHESS group 6.8, the combined telephone monitoring and counseling + ACHESS group had 6.0, while the treatment as usual only group had 10.3. However, none of the active treatments markedly outperformed the other in terms of percentage of days of heavy drinking.
Telephone monitoring and counseling, ACHESS, and telephone monitoring and counseling + ACHESS outperformed treatment as usual in terms of any drinking, but not drug use, negative consequences, or well-being.
Those in the treatment as usual group were 3 times more likely to drink any alcohol in study months 1–12 compared to the telephone monitoring and counseling group, and 2.4 times more likely to drink any alcohol than the telephone monitoring and counseling + ACHESS group. However, the treatment as usual group was not meaningfully more likely to drink than the ACHESS group, although in absolute terms, the treatment as usual group did more poorly on this measure.
In terms of other secondary study outcomes including drug use, negative consequences, and quality of life, there were no meaningful between group differences.
There were no between group differences at 18-month follow-up.
Groups were not meaningfully different on any of the primary or secondary study outcome measures at 18-month follow-up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study replicated findings from prior research which has found that telephone monitoring and counseling and ACHESS can improve alcohol use outcomes for individuals seeking recovery from alcohol use disorder when added to treatment as usual. In addition, this study was the first to compare these two approaches, and the first to determine whether combining these interventions improved outcomes over either intervention alone.
Although none of the interventions in this study added to treatment as usual (i.e., telephone monitoring and counseling, ACHESS, and their combination) performed markedly better than the other, findings are notable that all outperformed treatment as usual alone in terms of the primary study outcome – percentage days heavy drinking.
What is perhaps most notable among these findings is that a ‘therapist in the pocket app’, ACHESS, with minimal monitoring by trained personnel, performed about as well as more costly telephone monitoring and counseling. This is exciting, because it suggests that a relatively low cost, high-accessibility intervention might be enough to produce the improvements in drinking outcomes previously observed for more intensive and expensive counseling follow-up approaches.
At the same time, it’s important to note that the study groups were not markedly different in terms of drug use, negative consequences, or well-being over the 12-month treatment period, or on any study measure at 18-month follow-up. This highlights potential limitations of telephone monitoring and counseling, apps like ACHESS, and their combination, both during outpatient treatment, and over the longer-term. While the researchers’ findings suggest that patients seeking recovery from alcohol use disorder might experience better alcohol use outcomes with continued counseling or app use (e.g., continued use of these through the 18-month follow up might have showed benefits at this longer follow-up), these results may not be sustained when counseling or app use is discontinued as was found this study at the 18-month follow-up. Also, benefits related to reduced drug use, negative consequences, and improved well-being may not follow from these interventions. It could be that additional resources are needed to confer such benefits, especially for individuals with limited resources and recovery capital.
As noted by the researchers:
More than 80% of participants in this study were African American, which although representative of clients in treatment for substance use disorders in publicly funded programs in Philadelphia, USA, may not be representative of other treatment settings and locations. While there is no reason to believe that these effects would not generalize to other patient populations, different findings might be obtained in different patient populations and replication studies are needed.
Biological measures of drinking outcome were obtained only at the 18-month follow-up, meaning the researchers relied solely on self-report to assess drinking outcomes throughout the active treatment period of the study. Though there is no reason to suspect participants did not report any alcohol use accurately, self-report can be prone to certain kinds of biases.
Also:
The authors focused on percentage days heavy drinking and any drinking (yes/no). While these are important measures of alcohol use outcomes for people in treatment for alcohol use disorder, they don’t paint the full picture of alcohol use. Percentage days abstinent, for instance, is a commonly used measure that characterizes overall alcohol use over a monitoring period, which was not reported in this study.
BOTTOM LINE
Results from this randomized controlled trial indicate that adding telephone monitoring and counseling, ACHESS and the combination of telephone monitoring and counseling and ACHESS to intensive outpatient treatment reduced heavy drinking by approximately 50% over 12 months of active treatment. However, those receiving these interventions were not markedly different from those receiving treatment as usual only in terms of drug use, negative consequences, or well-being over the 12-month treatment period, and no meaningful differences were observed at 18-month follow-up occurring 6 months after the conclusion of treatment.
For individuals and families seeking recovery: The findings here build on previous studies showing follow-up care for individuals in substance use disorder treatment improves treatment outcomes. Results from this study suggest that telephone counseling and apps like ACHESS can enhance recovery outcomes when added to conventional outpatient treatment. Currently, follow-up counseling and support is not widely practiced in addiction treatment, except perhaps in some higher quality programs. When researching treatment program options, ask if follow-up care is provided. Additionally, apps like ACHESS will also likely confer benefit, whether used alone or in conjunction with follow-up counseling.
For treatment professionals and treatment systems: The researchers’ findings build on previous studies showing follow-up care for individuals in substance use disorder treatment improves treatment outcomes. Results from this study suggest that telephone counseling and apps like ACHESS can enhance recovery outcomes when added to conventional outpatient treatment. Adding follow-up counseling and support to treatment programs is likely to improve patient outcomes. Additionally, apps like ACHESS will also likely confer benefit, whether alone or in conjunction with follow-up counseling.
For scientists:The researchers’ findings build on previous studies showing follow-up care for individuals in substance use disorder treatment improves treatment outcomes. Results from this study suggest that telephone counseling and apps like ACHESS can enhance recovery outcomes when added to conventional outpatient treatment. More work is needed, however, to determine for whom, and under what conditions these supplemental interventions confer the most benefit.
For policy makers: The researchers’ findings build on previous studies showing follow-up care for individuals in substance use disorder treatment improves treatment outcomes. Results from this study suggest that telephone counseling and apps like ACHESS can enhance recovery outcomes when added to conventional outpatient treatment. Reducing barriers to follow-up care such as phone counseling and relapse prevention apps by requiring insurers to reimburse for these services will improve public health and reduce costs to healthcare systems in the long run.
Individuals with alcohol use disorder typically require continuing care to achieve stable remission. There are however numerous barriers that impede individuals’ access to continuing care, such as employment or family responsibilities, limited access to transportation, illness or disabilities, and for some, geographic isolation.
In this study, the researchers compared cognitive behavioral therapy-based telephone monitoring and counseling, ACHESS, and the integrated combination of both interventions to intensive outpatient programs (commonly referred to as IOPs) to determine if these continuing care add-ons improve alcohol use disorder outcomes over treatment as usual. This study also examined whether telephone monitoring and counseling, ACHESS, or the combination of these interventions were superior to one another.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized controlled trial with 262 participants who received either telephone monitoring and counseling + treatment as usual, ACHESS + treatment as usual, the integrated combination of both interventions + treatment as usual, or treatment as usual only over a 12-month period. Groups were compared during the 12-month treatment phase and at post-treatment follow-up (18 months post-baseline). The primary study outcome was percentage heavy drinking days over the 12-month treatment period. Secondary outcomes included percentage heavy drinking days at 18-month follow-up, any alcohol use within a given follow-up period (yes/no), any drug use (yes/no), and alcohol use related negative consequences and quality of life during study months 3, 6, 9, 12 and 18.
All participants received intensive outpatient treatment, which provided 9 hours of group counseling per week for up to 3 months, plus up to 3 months of weekly continuing care. For the treatment as usual group, this was the only treatment received.
Telephone monitoring and counseling included one initial in-person session with a counselor to establish a relationship. Telephone calls then occurred weekly in month 1, twice monthly in months 2–4, monthly in months 5–7, and every other month in months 8–12 for a total of 16 possible calls. Each call lasted 15–30 minutes. At the beginning of each call, participants completed a brief assessment of substance use, and risk and protective factors. Cognitive behavioral therapy-based counseling was provided based on the results of these assessments. Potential coping strategies and behaviors were practiced, and participants were reinforced for engagement in pro-recovery activities. Participants without reliable access to a telephone were given a smartphone.
The ACHESS app offered connections to online peer support, access to audio and written information on addiction, recovery related web links, global positioning system-driven information on mutual-help meetings, and inspirational messages. If needed, participants were provided with a smartphone and data plan. Study staff trained the participants to use the ACHESS app. ACHESS collected information on confidence for maintaining abstinence (daily) and on 10 risk and protective factors (weekly) via surveys delivered through the app. When data indicated that relapse risk was high, participants were encouraged via automatic text messages to seek additional support. Also, following 7 days of inactivity, ACHESS automatically sent a message to participants and alerted ACHESS support staff, who encouraged use of ACHESS via text messaging.
For the combined telephone monitoring and counseling and ACHESS group, telephone monitoring and counseling and ACHESS were provided. In addition, in the event a participant reported something clinically concerning through ACHESS, the telephone counselors received an alert. Counselors could also view a graph with current and past assessment scores in a clinician dashboard. The idea here was that these features would support faster outreach to patients when risk increased.
The primary outcome measure was percentage of days of heavy drinking (defined as 5 or more drinks/day for men, 4 or more drinks/day for women) during the 12-month treatment phase of the study. Secondary outcomes measured during study months 3, 6, 9, 12 and 18 months were: Percentage of days of heavy drinking at 18 months, any alcohol use within a given follow-up period (yes/no), any drug use within a given follow-up period (yes/no, as determined by self-report measures, and urine drug screens at 18-month follow-up), alcohol use related negative consequences measured by the short inventory of problems, and quality of life measured by the short form survey.
Participants were 262 adults recruited from four publicly funded intensive outpatient programs in Philadelphia, USA. To be included in the study, participants had to: 1) Have a Diagnostic and Statistical Manual of Mental Disorders-5 (DSM 5) diagnosis of current, moderate to severe alcohol use disorder, 2) have completed 3 weeks of an intensive outpatient treatment, 3) be aged 18–75 years, 4) have no current psychotic disorder or dementia, 5) have no acute medical problem requiring inpatient treatment, and 6) be not receiving other addiction treatment.
Participants, on average, were 47 years old, had 12 years of education. Most were male (71%), African American (82%) and never married (67%). Current co-occurring disorders included cocaine use disorder (39%), anxiety disorders (35%), and major depression (26%). Participants drank alcohol on 45% of the days in the 3 months prior to baseline, which included 3–4 weeks of intensive outpatient program.
WHAT DID THIS STUDY FIND?
Adherence to ACHESS app usage was generally better than for telephone monitoring and counseling.
In the ACHESS only group, participants used the ACHESS app an average of 20 days per month in months 1 and 2, but subsequently declined in usage to around14 days per month. In telephone monitoring and counseling + ACHESS group, ACHESS was used an average of 16 days per month in months 1 and 2 and subsequently declined to around 10 days per month for the remainder of the study.
The telephone monitoring and counseling group completed, on average, 8.1 counseling sessions, while the telephone monitoring and counseling + ACHESS group completed 10.7. Notably, among the participants who completed the in-person orientation session, counseling sessions were slightly better attended, with a mean of 10.2 in the telephone monitoring and counseling group and 11.0 in telephone monitoring and counseling + ACHESS group.
Telephone monitoring and counseling, ACHESS, and telephone monitoring and counseling + ACHESS all outperformed treatment as usual in terms of percentage of days of heavy drinking over the 12-month active treatment period.
Average percentage of days of heavy drinking in study months 1–12 was significantly lower in the three treatment groups compared to treatment as usual only group. Specifically, the telephone monitoring and counseling group had on average 5.4 percent days of heavy drinking, the ACHESS group 6.8, the combined telephone monitoring and counseling + ACHESS group had 6.0, while the treatment as usual only group had 10.3. However, none of the active treatments markedly outperformed the other in terms of percentage of days of heavy drinking.
Telephone monitoring and counseling, ACHESS, and telephone monitoring and counseling + ACHESS outperformed treatment as usual in terms of any drinking, but not drug use, negative consequences, or well-being.
Those in the treatment as usual group were 3 times more likely to drink any alcohol in study months 1–12 compared to the telephone monitoring and counseling group, and 2.4 times more likely to drink any alcohol than the telephone monitoring and counseling + ACHESS group. However, the treatment as usual group was not meaningfully more likely to drink than the ACHESS group, although in absolute terms, the treatment as usual group did more poorly on this measure.
In terms of other secondary study outcomes including drug use, negative consequences, and quality of life, there were no meaningful between group differences.
There were no between group differences at 18-month follow-up.
Groups were not meaningfully different on any of the primary or secondary study outcome measures at 18-month follow-up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study replicated findings from prior research which has found that telephone monitoring and counseling and ACHESS can improve alcohol use outcomes for individuals seeking recovery from alcohol use disorder when added to treatment as usual. In addition, this study was the first to compare these two approaches, and the first to determine whether combining these interventions improved outcomes over either intervention alone.
Although none of the interventions in this study added to treatment as usual (i.e., telephone monitoring and counseling, ACHESS, and their combination) performed markedly better than the other, findings are notable that all outperformed treatment as usual alone in terms of the primary study outcome – percentage days heavy drinking.
What is perhaps most notable among these findings is that a ‘therapist in the pocket app’, ACHESS, with minimal monitoring by trained personnel, performed about as well as more costly telephone monitoring and counseling. This is exciting, because it suggests that a relatively low cost, high-accessibility intervention might be enough to produce the improvements in drinking outcomes previously observed for more intensive and expensive counseling follow-up approaches.
At the same time, it’s important to note that the study groups were not markedly different in terms of drug use, negative consequences, or well-being over the 12-month treatment period, or on any study measure at 18-month follow-up. This highlights potential limitations of telephone monitoring and counseling, apps like ACHESS, and their combination, both during outpatient treatment, and over the longer-term. While the researchers’ findings suggest that patients seeking recovery from alcohol use disorder might experience better alcohol use outcomes with continued counseling or app use (e.g., continued use of these through the 18-month follow up might have showed benefits at this longer follow-up), these results may not be sustained when counseling or app use is discontinued as was found this study at the 18-month follow-up. Also, benefits related to reduced drug use, negative consequences, and improved well-being may not follow from these interventions. It could be that additional resources are needed to confer such benefits, especially for individuals with limited resources and recovery capital.
As noted by the researchers:
More than 80% of participants in this study were African American, which although representative of clients in treatment for substance use disorders in publicly funded programs in Philadelphia, USA, may not be representative of other treatment settings and locations. While there is no reason to believe that these effects would not generalize to other patient populations, different findings might be obtained in different patient populations and replication studies are needed.
Biological measures of drinking outcome were obtained only at the 18-month follow-up, meaning the researchers relied solely on self-report to assess drinking outcomes throughout the active treatment period of the study. Though there is no reason to suspect participants did not report any alcohol use accurately, self-report can be prone to certain kinds of biases.
Also:
The authors focused on percentage days heavy drinking and any drinking (yes/no). While these are important measures of alcohol use outcomes for people in treatment for alcohol use disorder, they don’t paint the full picture of alcohol use. Percentage days abstinent, for instance, is a commonly used measure that characterizes overall alcohol use over a monitoring period, which was not reported in this study.
BOTTOM LINE
Results from this randomized controlled trial indicate that adding telephone monitoring and counseling, ACHESS and the combination of telephone monitoring and counseling and ACHESS to intensive outpatient treatment reduced heavy drinking by approximately 50% over 12 months of active treatment. However, those receiving these interventions were not markedly different from those receiving treatment as usual only in terms of drug use, negative consequences, or well-being over the 12-month treatment period, and no meaningful differences were observed at 18-month follow-up occurring 6 months after the conclusion of treatment.
For individuals and families seeking recovery: The findings here build on previous studies showing follow-up care for individuals in substance use disorder treatment improves treatment outcomes. Results from this study suggest that telephone counseling and apps like ACHESS can enhance recovery outcomes when added to conventional outpatient treatment. Currently, follow-up counseling and support is not widely practiced in addiction treatment, except perhaps in some higher quality programs. When researching treatment program options, ask if follow-up care is provided. Additionally, apps like ACHESS will also likely confer benefit, whether used alone or in conjunction with follow-up counseling.
For treatment professionals and treatment systems: The researchers’ findings build on previous studies showing follow-up care for individuals in substance use disorder treatment improves treatment outcomes. Results from this study suggest that telephone counseling and apps like ACHESS can enhance recovery outcomes when added to conventional outpatient treatment. Adding follow-up counseling and support to treatment programs is likely to improve patient outcomes. Additionally, apps like ACHESS will also likely confer benefit, whether alone or in conjunction with follow-up counseling.
For scientists:The researchers’ findings build on previous studies showing follow-up care for individuals in substance use disorder treatment improves treatment outcomes. Results from this study suggest that telephone counseling and apps like ACHESS can enhance recovery outcomes when added to conventional outpatient treatment. More work is needed, however, to determine for whom, and under what conditions these supplemental interventions confer the most benefit.
For policy makers: The researchers’ findings build on previous studies showing follow-up care for individuals in substance use disorder treatment improves treatment outcomes. Results from this study suggest that telephone counseling and apps like ACHESS can enhance recovery outcomes when added to conventional outpatient treatment. Reducing barriers to follow-up care such as phone counseling and relapse prevention apps by requiring insurers to reimburse for these services will improve public health and reduce costs to healthcare systems in the long run.