Adding psilocybin to talk therapy improves outcomes, but differentiating from placebo effects proves challenging
Psilocybin, a type of hallucinogen, may help in the treatment of alcohol use disorder, but there has only been one study published since 1971 investigating its efficacy. This study rigorously examined whether adding psilocybin to talk therapy improved drinking outcomes in people with alcohol use disorder.
Hallucinogens (also known as “psychedelics”) are a class of drugs that alter people’s perceptions and sensations. Psilocybin is a type of hallucinogen that can be made synthetically, or found in wild mushrooms (more commonly known by their street names as “magic mushrooms” or “shrooms”). While these drugs are often taken recreationally or as part of religious or healing ceremonies, they may also have clinical utility in treating a variety of conditions, including mental health and substance use disorders.
The reasons for these therapeutic effects in treating such conditions are not yet well understood, but possible mechanisms of action include biological and psychological models. Biological models suggest that the therapeutic effects of psilocybin are the result of a complex alteration of communication in brain networks and changes in how serotonin is produced and regulated. Serotonin is a brain chemical that plays a key role in boosting moods. Psychological models suggest that psilocybin allows therapeutic processes to be enhanced and more easily accessible. For instance, psychoanalytic perspectives propose that the therapeutic effects are due to a psychological transformation, deeper insights on alcohol use harms and behaviors, or spiritual awakenings that occur through the intensification of accessing the unconscious and allowing repressed traumas to resurface. Similarly, cognitive-behavioral perspectives propose that psilocybin’s beneficial effects result from destabilizing dysfunctional beliefs and facilitating new learning processes
During the 1950s through the 1970s, studies examined the use of psilocybin as treatments for mental health and substance use disorders, including six randomized trials examining the use of hallucinogens for treating alcohol use disorder (specifically lysergic acid diethylamide, or LSD). Despite early promising results, LSD was outlawed in 1968 and then in 1970, Congress passed the Controlled Substances Act, which classified psilocybin and other hallucinogens in the schedule I category. Schedule I drugs have been determined to have high potential to be misused and no medical use. Accordingly, most research on hallucinogens stopped.
However, this topic was revisited in the year 2000 by researchers at Johns Hopkins University. Since then, a number of research studies have published on the effectiveness and safety of hallucinogens in treating a wide range of conditions. These include a study that analyzed the results of the six alcohol use disorder trials together to determine an overall effect (i.e., meta-analysis), which showed some beneficial effects of LSD on alcohol use disorder outcomes and that it was generally safe (i.e., few adverse events were reported). Similarly, psilocybin has shown striking results for smoking cessation, with an 80% abstinence rate at 6-month follow-up, albeit the study was a small pilot without a control group that needs replicated in a larger randomized controlled trial
The first (and only) study to investigate the effects of psilocybin on alcohol use disorder and demonstrate its feasibility was conducted in 2015. Although the study did not include a comparison group, results showed improvements in drinking outcomes, providing a rationale for future experimental studies. This study aimed to build on this work by experimentally evaluating whether psilocybin-assisted treatment improved drinking outcomes in people with alcohol use disorder.
HOW WAS THIS STUDY CONDUCTED?
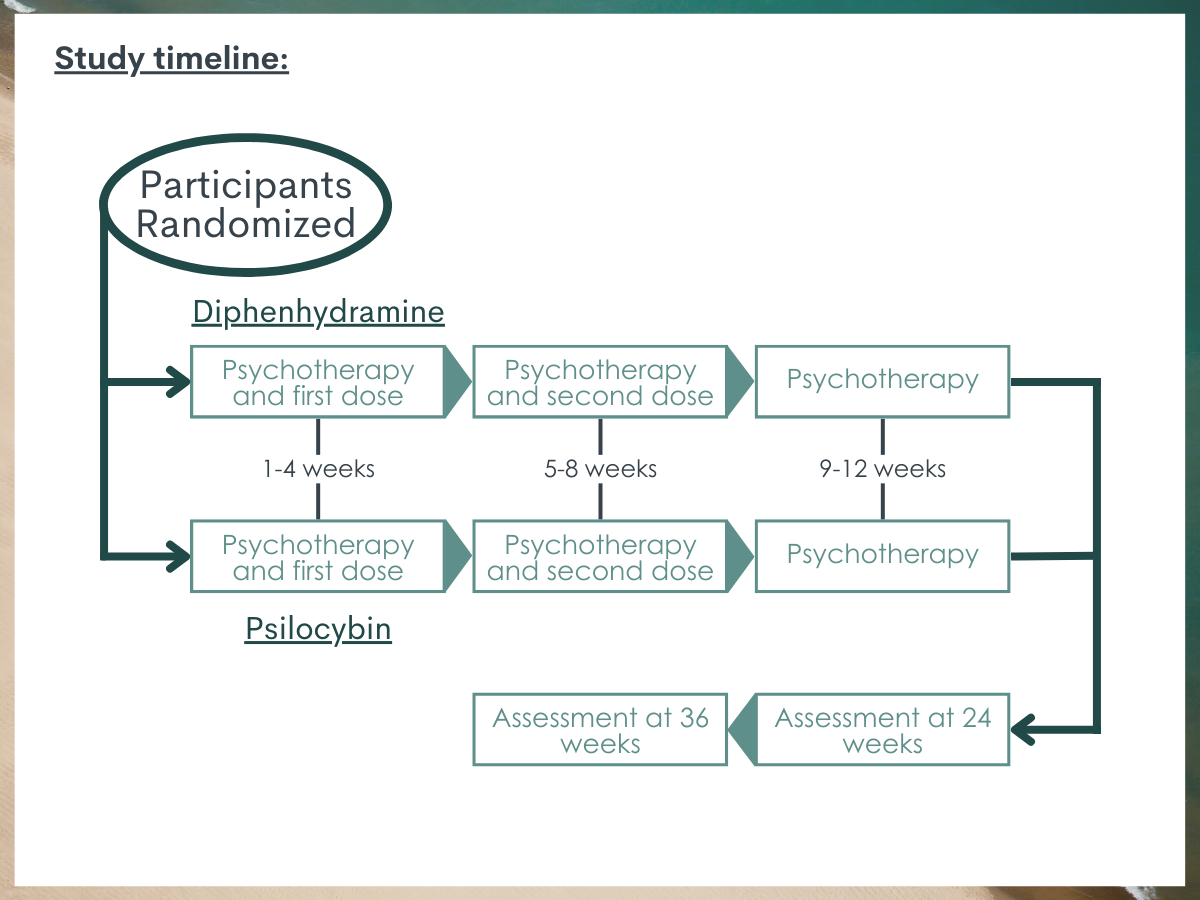
The research team conducted a randomized clinical trial to evaluate whether psilocybin reduced harmful alcohol use in participants with alcohol use disorder. Participants were randomized to receive either psilocybin or an allergy medication (diphenhydramine, better known by its brand name “Benadryl”) that was intended to serve as an active placebo. The use of Benadryl (diphenhydramine) was used to help with the problem of “unblinding,” which can occur in clinical trials when participants can clearly tell which medication they are getting and undermines the purpose of placebo. In this case, compared to a more classic placebo (e.g., a sugar pill), psilocybin produces profound psychological effects and thus almost certainly unblinds the study. Hence, the use of some kind of sedating and psychologically noticeable medication such as Benadryl was supposed to limit the unblinding by hopefully giving participants the idea that they may be receiving the active medication but not knowing for sure.
Participants between the ages of 25 and 65 were recruited from the community at the University of New Mexico and New York University. They were eligible for the study if they had a diagnosis of alcohol dependence based on a DSM-IV structured clinical interview and at least 4 heavy drinking days during the 30 days prior to screening (i.e., 5 or more drinks/day for men and 4 or more drinks/day for women). They were not eligible if they had a major psychiatric or other drug use disorder (apart from alcohol), used hallucinogens recreationally, had a medical condition that contraindicated the study medications, used other medications that could interfere with psilocybin’s proposed therapeutic effects, or were in current treatment for alcohol use disorder.
Participants were assessed at the initial screening, baseline (week 0), and weeks 4, 5, 8, 9, 12, 24, and 36. They received their first dose of psilocybin or placebo during week 4 and their second, increased dose during week 8. Several steps were taken to ensure participants’ safety during medication administrations, including having a therapist be with them the entire time and having medications readily available to treat any anxiety, hypertension, or other symptoms that may have occurred during the administration. After each session, participants were asked whether they thought they received psilocybin or the placebo and rate their degree of certainty on a 100-point scale, with 0 reflecting “not at all confident” and 100 reflecting “extremely confident.”
Both groups were also offered 12 weeks of psychotherapy (i.e., motivational interviewing and cognitive behavioral therapy) during the 4 weeks before the first medication session, the 4 weeks between the first and second medication sessions, and the 4 weeks in the month following the second medication session.
Outcomes were assessed over 32 weeks following the first dose of the medication (weeks 5-36).The primary outcome the researchers were interested in was the percentage of heavy drinking days. As secondary outcomes, they were also interested in overall percentage of drinking days, mean standard drinks per day, abstinence, absence of heavy drinking days, and a reduction in World Health Organization (WHO) risk level.WHO risk levels are defined by grams of alcohol consumed per day and range from level 0, defined as no alcohol consumed, to level 4 (the highest risk level), defined as more than 100 grams of alcohol per day for men (7.14 U.S. standard drinks) and more than 60 grams per day for women (4.3 U.S. standard drinks).
Finally, they assessed drinking-related problems at weeks 12, 24, and 36 using the Short Index of Problems, which assesses problems across the categories of physical, inter-personal, intra-personal, and impulse control problems, as well as difficulty with social responsibility.
In total, 95 participants were randomized, with 49 randomized to the psilocybin group and 46 to the placebo group. Among these, the mean age was 45.8 years, 44.2% were women, and the majority identified as non-Hispanic White (78.9%). They had a mean of 5.3 alcohol dependence criteria out of the 7 and had a diagnosis of alcohol dependence for an average of 14.2 years.
WHAT DID THIS STUDY FIND?
There were no differences between the psilocybin and placebo groups in drinking outcomes prior to the first medication session.
Prior to receiving the medication or placebo, participants were assessed on their alcohol use while receiving the psychotherapy interventions alone. During this time, both groups showed similar decreases in alcohol use between screening and week 4. Those who would ultimately receive psilocybin showed a 32.4% decrease in the percentage of heavy drinking days. This was similar to what was observed in the placebo group, which showed a 27.3% decrease. Similarly, both groups of patients showed decreases in the percentage of days on which they drank any alcohol and the number of drinks per day that they consumed.
The psilocybin group showed greater drinking improvements than the control group.
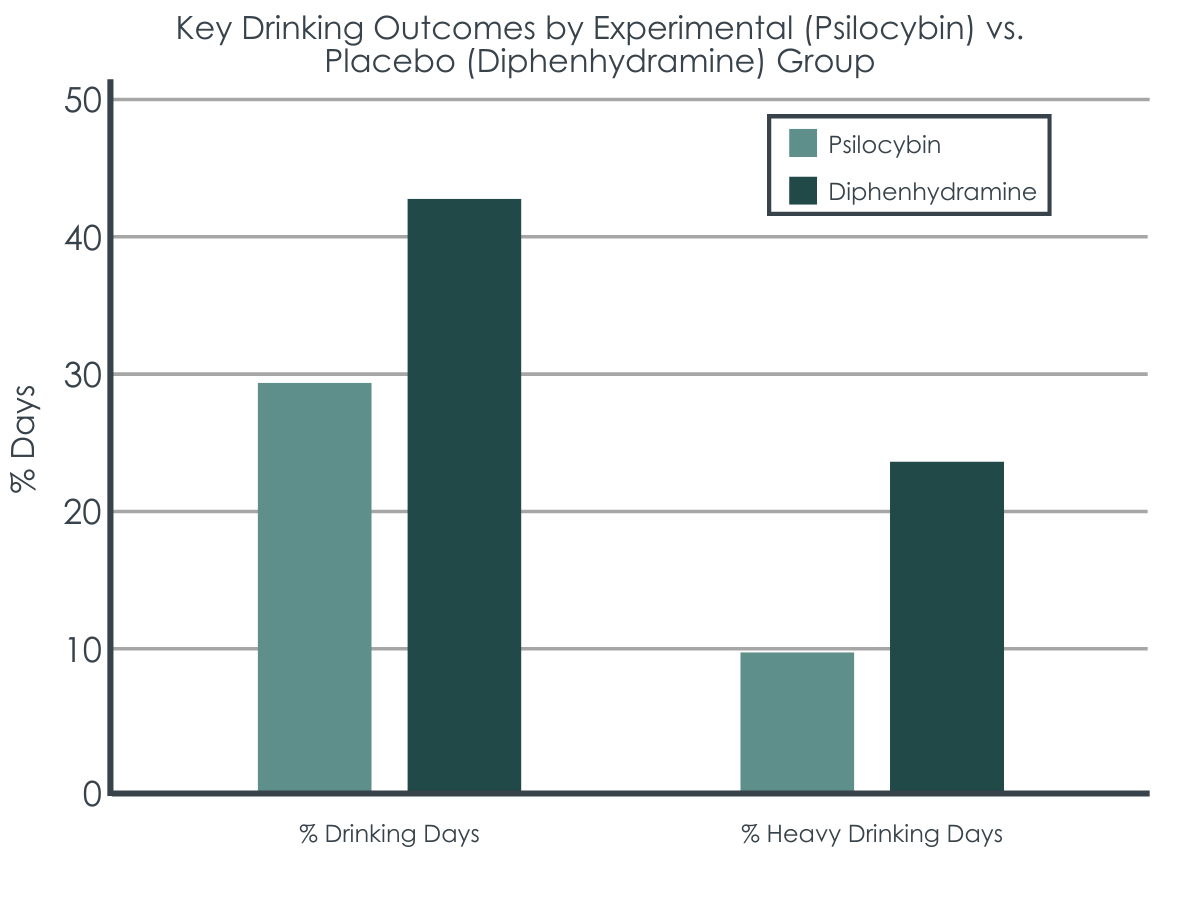
After the first medication session (weeks 5 to 36), during the 32-week follow-up period, participants who received psilocybin showed a greater decrease in percent of heavy drinking days than those in the placebo group. Those who received psilocybin had a mean of 9.71% of heavy drinking days, compared to the mean of 23.57% observed in the placebo group.
There were also greater decreases observed in the psilocybin group compared to the placebo group among the secondary outcomes during follow-up. For percentage of drinking days, the effect did not quite reach statistical significance, but there was a potentially meaningful difference, with a mean of 29.29% of drinking days observed among those who received psilocybin, compared to the 42.83% observed in the placebo group.
Figure 2. The “% Drinking Days” outcome was not a statistically significant difference.
Further, the psilocybin group had a mean of 1.17 drinks per day, 16 participants who had no heavy drinking days, and 29 participants who had a 2-level reduction in the WHO risk level, while the placebo group had a mean of 2.26 drinks per day, 5 participants who had no heavy drinking days, and 18 participants who had a 2-level reduction in the WHO risk level. The effects on heavy drinking days and WHO risk levels persisted during the final month of follow-up (weeks 33-36).
There were no differences in abstinence rates between the groups, but the psilocybin group had fewer drinking-related problems than the placebo group. Those in the psilocybin group reported a total problems score of 6.59, compared to the score of 13.00 reported by the placebo group.
The majority of participants knew if they were in the psilocybin or placebo group.
Despite the use of Benadryl as the placebo in an attempt to maintain “the blind” and disguise the fact as to who may be getting the active medication (psilocybin) or not, participants were able to correctly guess after the first medication administration whether they received psilocybin or the placebo in 93.6% of sessions with a mean certainty level of 88.5% (i.e., the degree to which they felt confident in their guess, with higher ratings reflecting more confidence). Among the second medication sessions, participants were able to correctly guess their group in 94.7% of sessions, with a mean certainty level of 90.6%. Accordingly, the study was essentially unblinded.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study conducted a randomized controlled trial to evaluate the effects of systematically adding psilocybin treatment to psychotherapy on a range of drinking outcomes among participants with alcohol use disorder in comparison to a placebo medication and psychotherapy.
There were no differences between groups before the first medication session, consistent with the absence of a psilocybin effect during therapy before it was administered. During the follow-up period, however, participants who received psilocybin had on average about 14% fewer heavy drinking days than those receiving placebo. Participants who received psilocybin also showed greater reductions in the secondary outcomes of percentage of drinking days, drinks per day, absence of heavy drinking days, and WHO risk level than the placebo group.
These results are consistent with the recent combinedanalysis of the six randomized controlled trials that were conducted throughout the 1960sshowing some beneficial effects of LSD on alcohol use disorder outcomes. Additionally, these results build upon the initial feasibility study conducted in 2015 that was one of the first to show that treating alcohol use disorder with psilocybin is possible and may help improve drinking outcomes. Together, these research studies suggest that hallucinogens may be a usefuladd-on to therapy for alcohol use disorder. However, given that this area of research is in its infancy, more experimental studies are needed with a larger number of participants to understand the effects of hallucinogens on alcohol use disorder outcomes.
Importantly, there were few serious adverse events reported. The adverse events that were reported were mostly mild and were comparable to what has been observed in other studies investigating the effects of psilocybin. While researchers in the study took several steps to ensure safety, results of this study suggest that the use of psilocybin can generally be considered safe if similar steps are used.
Of note, although the psilocybin group showed greater reductions in drinking outcomes than the placebo group, both groups showed reductions overall prior to and after receiving medication, which is likely due to the psychotherapy both groups were offered. Participation in the psychotherapy sessions was almost 100% in both groups. This underscores the importance of psychotherapy for participants with alcohol use disorder.
Additionally, because participants knew whether they received psilocybin or the placebo in most of the medication sessions, it is unclear whether the benefits observed in the psilocybin group are fully explained by the drug or by so-called “expectancy effects.” If participants knew they received the placebo, they may be less likely to expect and therefore report improved outcomes. On the other hand, if participants knew they received psilocybin, they may be more likely to expect and report improved outcomes. This is a very common and ongoing problem encountered when studying the effects of hallucinogens, however, given the big challenge in finding some kind of active placebo medication to compete with the profound and obvious effects of hallucinogens.
Participants nearly always knew whether they received psilocybin or the placebo. This knowledge could have influenced their expectations of how effective treatment is, as described above, and may have affected results.
Given the small number of participants, the researchers may not have been able to detect smaller effects, such as differences between abstinence rates. Further, they were not able to examine subgroup differences, such as between women or racial minority groups.
Participants were recruited from the community and had lower drinking levels at screening than in other research studies investigating the effects of medications on alcohol use disorder. Accordingly, the results may not apply to people with more severe alcohol use disorder.
Because the researchers did not continue to investigate the effects of psilocybin beyond the 32-week follow-up period, it is unknown whether the beneficial effects observed in the psilocybin group persist.
BOTTOM LINE
Psilocybin should be investigated further as this study’s findings suggested that psilocybin may be a helpful add-on to therapy for alcohol use disorder. Participants who received psilocybin reduced their drinking and had fewer drinking-related problems than those who received a placebo with psychotherapy.
For individuals and families seeking recovery: While these results are novel and encouraging, psilocybin remainsillegal nationally (although a few states are beginning to decriminalize it or make certain exceptions), and is not yet offered as a standard treatment for alcohol use disorder. However, although people who received psilocybin showed greater reductions in drinking outcomes than those who received placebo, reductions were still observed in both groups prior to and after receiving medication. These reductions in both groups are likely due to psychotherapy. Accordingly, people seeking recovery are encouraged to take advantage of currently available and effective psychotherapy treatment, as well as existingFDA-approved medications for alcohol use disorder, untilresearch on the effectiveness of psilocybin progresses to a point where it is an available treatment.
For treatment professionals and treatment systems: The study findings showed greater reductions in drinking outcomes with psilocybin and psychotherapy compared to placebo and psychotherapy. However, because psilocybin is not yet an available treatment for alcohol use disorder, treatment professionals who continue to offer currently available and effective psychotherapy treatments are likely to still see improvements in their patients with alcohol use disorder. Further, the study findings also highlight the potential role of expectations, since participants often knew which medication they received. Professionals who use that information to promote positive expectations of treatment among their patients therefore may observe better outcomes.
For scientists:The current study suggests there are some potential benefits of treating alcohol use disorder with psilocybin. However, this was the first recent study conducted to experimentally evaluate the effects of psilocybin on alcohol use disorder and there was a small sample size with almost universal unblinding of the participants to their study condition. Accordingly, more rigorous experimental studies are needed with larger sample sizes to more thoroughly investigate efficacy, as well as the optimal dosage and conditions for administration, subgroup differences, and potential harms. Such research will help the field to understand the effects of psilocybin on alcohol use disorder. Keeping participants blinded to study condition remains a challenge.
For policy makers: Given the potential benefits of psilocybin for alcohol use disorder, re-classifying hallucinogens as drugs that may have medicinal purposes could help to facilitate public support and ignite additional research on its effects. Further, funding for more research on the potential utility of psilocybin and other hallucinogens for treating alcohol and other substance use disorders could shed light on its effectiveness, mechanisms of action, and optimal strategies for administration to enhance safety and promote the best possible outcomes.
Hallucinogens (also known as “psychedelics”) are a class of drugs that alter people’s perceptions and sensations. Psilocybin is a type of hallucinogen that can be made synthetically, or found in wild mushrooms (more commonly known by their street names as “magic mushrooms” or “shrooms”). While these drugs are often taken recreationally or as part of religious or healing ceremonies, they may also have clinical utility in treating a variety of conditions, including mental health and substance use disorders.
The reasons for these therapeutic effects in treating such conditions are not yet well understood, but possible mechanisms of action include biological and psychological models. Biological models suggest that the therapeutic effects of psilocybin are the result of a complex alteration of communication in brain networks and changes in how serotonin is produced and regulated. Serotonin is a brain chemical that plays a key role in boosting moods. Psychological models suggest that psilocybin allows therapeutic processes to be enhanced and more easily accessible. For instance, psychoanalytic perspectives propose that the therapeutic effects are due to a psychological transformation, deeper insights on alcohol use harms and behaviors, or spiritual awakenings that occur through the intensification of accessing the unconscious and allowing repressed traumas to resurface. Similarly, cognitive-behavioral perspectives propose that psilocybin’s beneficial effects result from destabilizing dysfunctional beliefs and facilitating new learning processes
During the 1950s through the 1970s, studies examined the use of psilocybin as treatments for mental health and substance use disorders, including six randomized trials examining the use of hallucinogens for treating alcohol use disorder (specifically lysergic acid diethylamide, or LSD). Despite early promising results, LSD was outlawed in 1968 and then in 1970, Congress passed the Controlled Substances Act, which classified psilocybin and other hallucinogens in the schedule I category. Schedule I drugs have been determined to have high potential to be misused and no medical use. Accordingly, most research on hallucinogens stopped.
However, this topic was revisited in the year 2000 by researchers at Johns Hopkins University. Since then, a number of research studies have published on the effectiveness and safety of hallucinogens in treating a wide range of conditions. These include a study that analyzed the results of the six alcohol use disorder trials together to determine an overall effect (i.e., meta-analysis), which showed some beneficial effects of LSD on alcohol use disorder outcomes and that it was generally safe (i.e., few adverse events were reported). Similarly, psilocybin has shown striking results for smoking cessation, with an 80% abstinence rate at 6-month follow-up, albeit the study was a small pilot without a control group that needs replicated in a larger randomized controlled trial
The first (and only) study to investigate the effects of psilocybin on alcohol use disorder and demonstrate its feasibility was conducted in 2015. Although the study did not include a comparison group, results showed improvements in drinking outcomes, providing a rationale for future experimental studies. This study aimed to build on this work by experimentally evaluating whether psilocybin-assisted treatment improved drinking outcomes in people with alcohol use disorder.
HOW WAS THIS STUDY CONDUCTED?
The research team conducted a randomized clinical trial to evaluate whether psilocybin reduced harmful alcohol use in participants with alcohol use disorder. Participants were randomized to receive either psilocybin or an allergy medication (diphenhydramine, better known by its brand name “Benadryl”) that was intended to serve as an active placebo. The use of Benadryl (diphenhydramine) was used to help with the problem of “unblinding,” which can occur in clinical trials when participants can clearly tell which medication they are getting and undermines the purpose of placebo. In this case, compared to a more classic placebo (e.g., a sugar pill), psilocybin produces profound psychological effects and thus almost certainly unblinds the study. Hence, the use of some kind of sedating and psychologically noticeable medication such as Benadryl was supposed to limit the unblinding by hopefully giving participants the idea that they may be receiving the active medication but not knowing for sure.
Participants between the ages of 25 and 65 were recruited from the community at the University of New Mexico and New York University. They were eligible for the study if they had a diagnosis of alcohol dependence based on a DSM-IV structured clinical interview and at least 4 heavy drinking days during the 30 days prior to screening (i.e., 5 or more drinks/day for men and 4 or more drinks/day for women). They were not eligible if they had a major psychiatric or other drug use disorder (apart from alcohol), used hallucinogens recreationally, had a medical condition that contraindicated the study medications, used other medications that could interfere with psilocybin’s proposed therapeutic effects, or were in current treatment for alcohol use disorder.
Participants were assessed at the initial screening, baseline (week 0), and weeks 4, 5, 8, 9, 12, 24, and 36. They received their first dose of psilocybin or placebo during week 4 and their second, increased dose during week 8. Several steps were taken to ensure participants’ safety during medication administrations, including having a therapist be with them the entire time and having medications readily available to treat any anxiety, hypertension, or other symptoms that may have occurred during the administration. After each session, participants were asked whether they thought they received psilocybin or the placebo and rate their degree of certainty on a 100-point scale, with 0 reflecting “not at all confident” and 100 reflecting “extremely confident.”
Both groups were also offered 12 weeks of psychotherapy (i.e., motivational interviewing and cognitive behavioral therapy) during the 4 weeks before the first medication session, the 4 weeks between the first and second medication sessions, and the 4 weeks in the month following the second medication session.
Outcomes were assessed over 32 weeks following the first dose of the medication (weeks 5-36).The primary outcome the researchers were interested in was the percentage of heavy drinking days. As secondary outcomes, they were also interested in overall percentage of drinking days, mean standard drinks per day, abstinence, absence of heavy drinking days, and a reduction in World Health Organization (WHO) risk level.WHO risk levels are defined by grams of alcohol consumed per day and range from level 0, defined as no alcohol consumed, to level 4 (the highest risk level), defined as more than 100 grams of alcohol per day for men (7.14 U.S. standard drinks) and more than 60 grams per day for women (4.3 U.S. standard drinks).
Finally, they assessed drinking-related problems at weeks 12, 24, and 36 using the Short Index of Problems, which assesses problems across the categories of physical, inter-personal, intra-personal, and impulse control problems, as well as difficulty with social responsibility.
In total, 95 participants were randomized, with 49 randomized to the psilocybin group and 46 to the placebo group. Among these, the mean age was 45.8 years, 44.2% were women, and the majority identified as non-Hispanic White (78.9%). They had a mean of 5.3 alcohol dependence criteria out of the 7 and had a diagnosis of alcohol dependence for an average of 14.2 years.
WHAT DID THIS STUDY FIND?
There were no differences between the psilocybin and placebo groups in drinking outcomes prior to the first medication session.
Prior to receiving the medication or placebo, participants were assessed on their alcohol use while receiving the psychotherapy interventions alone. During this time, both groups showed similar decreases in alcohol use between screening and week 4. Those who would ultimately receive psilocybin showed a 32.4% decrease in the percentage of heavy drinking days. This was similar to what was observed in the placebo group, which showed a 27.3% decrease. Similarly, both groups of patients showed decreases in the percentage of days on which they drank any alcohol and the number of drinks per day that they consumed.
The psilocybin group showed greater drinking improvements than the control group.
After the first medication session (weeks 5 to 36), during the 32-week follow-up period, participants who received psilocybin showed a greater decrease in percent of heavy drinking days than those in the placebo group. Those who received psilocybin had a mean of 9.71% of heavy drinking days, compared to the mean of 23.57% observed in the placebo group.
There were also greater decreases observed in the psilocybin group compared to the placebo group among the secondary outcomes during follow-up. For percentage of drinking days, the effect did not quite reach statistical significance, but there was a potentially meaningful difference, with a mean of 29.29% of drinking days observed among those who received psilocybin, compared to the 42.83% observed in the placebo group.
Figure 2. The “% Drinking Days” outcome was not a statistically significant difference.
Further, the psilocybin group had a mean of 1.17 drinks per day, 16 participants who had no heavy drinking days, and 29 participants who had a 2-level reduction in the WHO risk level, while the placebo group had a mean of 2.26 drinks per day, 5 participants who had no heavy drinking days, and 18 participants who had a 2-level reduction in the WHO risk level. The effects on heavy drinking days and WHO risk levels persisted during the final month of follow-up (weeks 33-36).
There were no differences in abstinence rates between the groups, but the psilocybin group had fewer drinking-related problems than the placebo group. Those in the psilocybin group reported a total problems score of 6.59, compared to the score of 13.00 reported by the placebo group.
The majority of participants knew if they were in the psilocybin or placebo group.
Despite the use of Benadryl as the placebo in an attempt to maintain “the blind” and disguise the fact as to who may be getting the active medication (psilocybin) or not, participants were able to correctly guess after the first medication administration whether they received psilocybin or the placebo in 93.6% of sessions with a mean certainty level of 88.5% (i.e., the degree to which they felt confident in their guess, with higher ratings reflecting more confidence). Among the second medication sessions, participants were able to correctly guess their group in 94.7% of sessions, with a mean certainty level of 90.6%. Accordingly, the study was essentially unblinded.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study conducted a randomized controlled trial to evaluate the effects of systematically adding psilocybin treatment to psychotherapy on a range of drinking outcomes among participants with alcohol use disorder in comparison to a placebo medication and psychotherapy.
There were no differences between groups before the first medication session, consistent with the absence of a psilocybin effect during therapy before it was administered. During the follow-up period, however, participants who received psilocybin had on average about 14% fewer heavy drinking days than those receiving placebo. Participants who received psilocybin also showed greater reductions in the secondary outcomes of percentage of drinking days, drinks per day, absence of heavy drinking days, and WHO risk level than the placebo group.
These results are consistent with the recent combinedanalysis of the six randomized controlled trials that were conducted throughout the 1960sshowing some beneficial effects of LSD on alcohol use disorder outcomes. Additionally, these results build upon the initial feasibility study conducted in 2015 that was one of the first to show that treating alcohol use disorder with psilocybin is possible and may help improve drinking outcomes. Together, these research studies suggest that hallucinogens may be a usefuladd-on to therapy for alcohol use disorder. However, given that this area of research is in its infancy, more experimental studies are needed with a larger number of participants to understand the effects of hallucinogens on alcohol use disorder outcomes.
Importantly, there were few serious adverse events reported. The adverse events that were reported were mostly mild and were comparable to what has been observed in other studies investigating the effects of psilocybin. While researchers in the study took several steps to ensure safety, results of this study suggest that the use of psilocybin can generally be considered safe if similar steps are used.
Of note, although the psilocybin group showed greater reductions in drinking outcomes than the placebo group, both groups showed reductions overall prior to and after receiving medication, which is likely due to the psychotherapy both groups were offered. Participation in the psychotherapy sessions was almost 100% in both groups. This underscores the importance of psychotherapy for participants with alcohol use disorder.
Additionally, because participants knew whether they received psilocybin or the placebo in most of the medication sessions, it is unclear whether the benefits observed in the psilocybin group are fully explained by the drug or by so-called “expectancy effects.” If participants knew they received the placebo, they may be less likely to expect and therefore report improved outcomes. On the other hand, if participants knew they received psilocybin, they may be more likely to expect and report improved outcomes. This is a very common and ongoing problem encountered when studying the effects of hallucinogens, however, given the big challenge in finding some kind of active placebo medication to compete with the profound and obvious effects of hallucinogens.
Participants nearly always knew whether they received psilocybin or the placebo. This knowledge could have influenced their expectations of how effective treatment is, as described above, and may have affected results.
Given the small number of participants, the researchers may not have been able to detect smaller effects, such as differences between abstinence rates. Further, they were not able to examine subgroup differences, such as between women or racial minority groups.
Participants were recruited from the community and had lower drinking levels at screening than in other research studies investigating the effects of medications on alcohol use disorder. Accordingly, the results may not apply to people with more severe alcohol use disorder.
Because the researchers did not continue to investigate the effects of psilocybin beyond the 32-week follow-up period, it is unknown whether the beneficial effects observed in the psilocybin group persist.
BOTTOM LINE
Psilocybin should be investigated further as this study’s findings suggested that psilocybin may be a helpful add-on to therapy for alcohol use disorder. Participants who received psilocybin reduced their drinking and had fewer drinking-related problems than those who received a placebo with psychotherapy.
For individuals and families seeking recovery: While these results are novel and encouraging, psilocybin remainsillegal nationally (although a few states are beginning to decriminalize it or make certain exceptions), and is not yet offered as a standard treatment for alcohol use disorder. However, although people who received psilocybin showed greater reductions in drinking outcomes than those who received placebo, reductions were still observed in both groups prior to and after receiving medication. These reductions in both groups are likely due to psychotherapy. Accordingly, people seeking recovery are encouraged to take advantage of currently available and effective psychotherapy treatment, as well as existingFDA-approved medications for alcohol use disorder, untilresearch on the effectiveness of psilocybin progresses to a point where it is an available treatment.
For treatment professionals and treatment systems: The study findings showed greater reductions in drinking outcomes with psilocybin and psychotherapy compared to placebo and psychotherapy. However, because psilocybin is not yet an available treatment for alcohol use disorder, treatment professionals who continue to offer currently available and effective psychotherapy treatments are likely to still see improvements in their patients with alcohol use disorder. Further, the study findings also highlight the potential role of expectations, since participants often knew which medication they received. Professionals who use that information to promote positive expectations of treatment among their patients therefore may observe better outcomes.
For scientists:The current study suggests there are some potential benefits of treating alcohol use disorder with psilocybin. However, this was the first recent study conducted to experimentally evaluate the effects of psilocybin on alcohol use disorder and there was a small sample size with almost universal unblinding of the participants to their study condition. Accordingly, more rigorous experimental studies are needed with larger sample sizes to more thoroughly investigate efficacy, as well as the optimal dosage and conditions for administration, subgroup differences, and potential harms. Such research will help the field to understand the effects of psilocybin on alcohol use disorder. Keeping participants blinded to study condition remains a challenge.
For policy makers: Given the potential benefits of psilocybin for alcohol use disorder, re-classifying hallucinogens as drugs that may have medicinal purposes could help to facilitate public support and ignite additional research on its effects. Further, funding for more research on the potential utility of psilocybin and other hallucinogens for treating alcohol and other substance use disorders could shed light on its effectiveness, mechanisms of action, and optimal strategies for administration to enhance safety and promote the best possible outcomes.
Hallucinogens (also known as “psychedelics”) are a class of drugs that alter people’s perceptions and sensations. Psilocybin is a type of hallucinogen that can be made synthetically, or found in wild mushrooms (more commonly known by their street names as “magic mushrooms” or “shrooms”). While these drugs are often taken recreationally or as part of religious or healing ceremonies, they may also have clinical utility in treating a variety of conditions, including mental health and substance use disorders.
The reasons for these therapeutic effects in treating such conditions are not yet well understood, but possible mechanisms of action include biological and psychological models. Biological models suggest that the therapeutic effects of psilocybin are the result of a complex alteration of communication in brain networks and changes in how serotonin is produced and regulated. Serotonin is a brain chemical that plays a key role in boosting moods. Psychological models suggest that psilocybin allows therapeutic processes to be enhanced and more easily accessible. For instance, psychoanalytic perspectives propose that the therapeutic effects are due to a psychological transformation, deeper insights on alcohol use harms and behaviors, or spiritual awakenings that occur through the intensification of accessing the unconscious and allowing repressed traumas to resurface. Similarly, cognitive-behavioral perspectives propose that psilocybin’s beneficial effects result from destabilizing dysfunctional beliefs and facilitating new learning processes
During the 1950s through the 1970s, studies examined the use of psilocybin as treatments for mental health and substance use disorders, including six randomized trials examining the use of hallucinogens for treating alcohol use disorder (specifically lysergic acid diethylamide, or LSD). Despite early promising results, LSD was outlawed in 1968 and then in 1970, Congress passed the Controlled Substances Act, which classified psilocybin and other hallucinogens in the schedule I category. Schedule I drugs have been determined to have high potential to be misused and no medical use. Accordingly, most research on hallucinogens stopped.
However, this topic was revisited in the year 2000 by researchers at Johns Hopkins University. Since then, a number of research studies have published on the effectiveness and safety of hallucinogens in treating a wide range of conditions. These include a study that analyzed the results of the six alcohol use disorder trials together to determine an overall effect (i.e., meta-analysis), which showed some beneficial effects of LSD on alcohol use disorder outcomes and that it was generally safe (i.e., few adverse events were reported). Similarly, psilocybin has shown striking results for smoking cessation, with an 80% abstinence rate at 6-month follow-up, albeit the study was a small pilot without a control group that needs replicated in a larger randomized controlled trial
The first (and only) study to investigate the effects of psilocybin on alcohol use disorder and demonstrate its feasibility was conducted in 2015. Although the study did not include a comparison group, results showed improvements in drinking outcomes, providing a rationale for future experimental studies. This study aimed to build on this work by experimentally evaluating whether psilocybin-assisted treatment improved drinking outcomes in people with alcohol use disorder.
HOW WAS THIS STUDY CONDUCTED?
The research team conducted a randomized clinical trial to evaluate whether psilocybin reduced harmful alcohol use in participants with alcohol use disorder. Participants were randomized to receive either psilocybin or an allergy medication (diphenhydramine, better known by its brand name “Benadryl”) that was intended to serve as an active placebo. The use of Benadryl (diphenhydramine) was used to help with the problem of “unblinding,” which can occur in clinical trials when participants can clearly tell which medication they are getting and undermines the purpose of placebo. In this case, compared to a more classic placebo (e.g., a sugar pill), psilocybin produces profound psychological effects and thus almost certainly unblinds the study. Hence, the use of some kind of sedating and psychologically noticeable medication such as Benadryl was supposed to limit the unblinding by hopefully giving participants the idea that they may be receiving the active medication but not knowing for sure.
Participants between the ages of 25 and 65 were recruited from the community at the University of New Mexico and New York University. They were eligible for the study if they had a diagnosis of alcohol dependence based on a DSM-IV structured clinical interview and at least 4 heavy drinking days during the 30 days prior to screening (i.e., 5 or more drinks/day for men and 4 or more drinks/day for women). They were not eligible if they had a major psychiatric or other drug use disorder (apart from alcohol), used hallucinogens recreationally, had a medical condition that contraindicated the study medications, used other medications that could interfere with psilocybin’s proposed therapeutic effects, or were in current treatment for alcohol use disorder.
Participants were assessed at the initial screening, baseline (week 0), and weeks 4, 5, 8, 9, 12, 24, and 36. They received their first dose of psilocybin or placebo during week 4 and their second, increased dose during week 8. Several steps were taken to ensure participants’ safety during medication administrations, including having a therapist be with them the entire time and having medications readily available to treat any anxiety, hypertension, or other symptoms that may have occurred during the administration. After each session, participants were asked whether they thought they received psilocybin or the placebo and rate their degree of certainty on a 100-point scale, with 0 reflecting “not at all confident” and 100 reflecting “extremely confident.”
Both groups were also offered 12 weeks of psychotherapy (i.e., motivational interviewing and cognitive behavioral therapy) during the 4 weeks before the first medication session, the 4 weeks between the first and second medication sessions, and the 4 weeks in the month following the second medication session.
Outcomes were assessed over 32 weeks following the first dose of the medication (weeks 5-36).The primary outcome the researchers were interested in was the percentage of heavy drinking days. As secondary outcomes, they were also interested in overall percentage of drinking days, mean standard drinks per day, abstinence, absence of heavy drinking days, and a reduction in World Health Organization (WHO) risk level.WHO risk levels are defined by grams of alcohol consumed per day and range from level 0, defined as no alcohol consumed, to level 4 (the highest risk level), defined as more than 100 grams of alcohol per day for men (7.14 U.S. standard drinks) and more than 60 grams per day for women (4.3 U.S. standard drinks).
Finally, they assessed drinking-related problems at weeks 12, 24, and 36 using the Short Index of Problems, which assesses problems across the categories of physical, inter-personal, intra-personal, and impulse control problems, as well as difficulty with social responsibility.
In total, 95 participants were randomized, with 49 randomized to the psilocybin group and 46 to the placebo group. Among these, the mean age was 45.8 years, 44.2% were women, and the majority identified as non-Hispanic White (78.9%). They had a mean of 5.3 alcohol dependence criteria out of the 7 and had a diagnosis of alcohol dependence for an average of 14.2 years.
WHAT DID THIS STUDY FIND?
There were no differences between the psilocybin and placebo groups in drinking outcomes prior to the first medication session.
Prior to receiving the medication or placebo, participants were assessed on their alcohol use while receiving the psychotherapy interventions alone. During this time, both groups showed similar decreases in alcohol use between screening and week 4. Those who would ultimately receive psilocybin showed a 32.4% decrease in the percentage of heavy drinking days. This was similar to what was observed in the placebo group, which showed a 27.3% decrease. Similarly, both groups of patients showed decreases in the percentage of days on which they drank any alcohol and the number of drinks per day that they consumed.
The psilocybin group showed greater drinking improvements than the control group.
After the first medication session (weeks 5 to 36), during the 32-week follow-up period, participants who received psilocybin showed a greater decrease in percent of heavy drinking days than those in the placebo group. Those who received psilocybin had a mean of 9.71% of heavy drinking days, compared to the mean of 23.57% observed in the placebo group.
There were also greater decreases observed in the psilocybin group compared to the placebo group among the secondary outcomes during follow-up. For percentage of drinking days, the effect did not quite reach statistical significance, but there was a potentially meaningful difference, with a mean of 29.29% of drinking days observed among those who received psilocybin, compared to the 42.83% observed in the placebo group.
Figure 2. The “% Drinking Days” outcome was not a statistically significant difference.
Further, the psilocybin group had a mean of 1.17 drinks per day, 16 participants who had no heavy drinking days, and 29 participants who had a 2-level reduction in the WHO risk level, while the placebo group had a mean of 2.26 drinks per day, 5 participants who had no heavy drinking days, and 18 participants who had a 2-level reduction in the WHO risk level. The effects on heavy drinking days and WHO risk levels persisted during the final month of follow-up (weeks 33-36).
There were no differences in abstinence rates between the groups, but the psilocybin group had fewer drinking-related problems than the placebo group. Those in the psilocybin group reported a total problems score of 6.59, compared to the score of 13.00 reported by the placebo group.
The majority of participants knew if they were in the psilocybin or placebo group.
Despite the use of Benadryl as the placebo in an attempt to maintain “the blind” and disguise the fact as to who may be getting the active medication (psilocybin) or not, participants were able to correctly guess after the first medication administration whether they received psilocybin or the placebo in 93.6% of sessions with a mean certainty level of 88.5% (i.e., the degree to which they felt confident in their guess, with higher ratings reflecting more confidence). Among the second medication sessions, participants were able to correctly guess their group in 94.7% of sessions, with a mean certainty level of 90.6%. Accordingly, the study was essentially unblinded.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study conducted a randomized controlled trial to evaluate the effects of systematically adding psilocybin treatment to psychotherapy on a range of drinking outcomes among participants with alcohol use disorder in comparison to a placebo medication and psychotherapy.
There were no differences between groups before the first medication session, consistent with the absence of a psilocybin effect during therapy before it was administered. During the follow-up period, however, participants who received psilocybin had on average about 14% fewer heavy drinking days than those receiving placebo. Participants who received psilocybin also showed greater reductions in the secondary outcomes of percentage of drinking days, drinks per day, absence of heavy drinking days, and WHO risk level than the placebo group.
These results are consistent with the recent combinedanalysis of the six randomized controlled trials that were conducted throughout the 1960sshowing some beneficial effects of LSD on alcohol use disorder outcomes. Additionally, these results build upon the initial feasibility study conducted in 2015 that was one of the first to show that treating alcohol use disorder with psilocybin is possible and may help improve drinking outcomes. Together, these research studies suggest that hallucinogens may be a usefuladd-on to therapy for alcohol use disorder. However, given that this area of research is in its infancy, more experimental studies are needed with a larger number of participants to understand the effects of hallucinogens on alcohol use disorder outcomes.
Importantly, there were few serious adverse events reported. The adverse events that were reported were mostly mild and were comparable to what has been observed in other studies investigating the effects of psilocybin. While researchers in the study took several steps to ensure safety, results of this study suggest that the use of psilocybin can generally be considered safe if similar steps are used.
Of note, although the psilocybin group showed greater reductions in drinking outcomes than the placebo group, both groups showed reductions overall prior to and after receiving medication, which is likely due to the psychotherapy both groups were offered. Participation in the psychotherapy sessions was almost 100% in both groups. This underscores the importance of psychotherapy for participants with alcohol use disorder.
Additionally, because participants knew whether they received psilocybin or the placebo in most of the medication sessions, it is unclear whether the benefits observed in the psilocybin group are fully explained by the drug or by so-called “expectancy effects.” If participants knew they received the placebo, they may be less likely to expect and therefore report improved outcomes. On the other hand, if participants knew they received psilocybin, they may be more likely to expect and report improved outcomes. This is a very common and ongoing problem encountered when studying the effects of hallucinogens, however, given the big challenge in finding some kind of active placebo medication to compete with the profound and obvious effects of hallucinogens.
Participants nearly always knew whether they received psilocybin or the placebo. This knowledge could have influenced their expectations of how effective treatment is, as described above, and may have affected results.
Given the small number of participants, the researchers may not have been able to detect smaller effects, such as differences between abstinence rates. Further, they were not able to examine subgroup differences, such as between women or racial minority groups.
Participants were recruited from the community and had lower drinking levels at screening than in other research studies investigating the effects of medications on alcohol use disorder. Accordingly, the results may not apply to people with more severe alcohol use disorder.
Because the researchers did not continue to investigate the effects of psilocybin beyond the 32-week follow-up period, it is unknown whether the beneficial effects observed in the psilocybin group persist.
BOTTOM LINE
Psilocybin should be investigated further as this study’s findings suggested that psilocybin may be a helpful add-on to therapy for alcohol use disorder. Participants who received psilocybin reduced their drinking and had fewer drinking-related problems than those who received a placebo with psychotherapy.
For individuals and families seeking recovery: While these results are novel and encouraging, psilocybin remainsillegal nationally (although a few states are beginning to decriminalize it or make certain exceptions), and is not yet offered as a standard treatment for alcohol use disorder. However, although people who received psilocybin showed greater reductions in drinking outcomes than those who received placebo, reductions were still observed in both groups prior to and after receiving medication. These reductions in both groups are likely due to psychotherapy. Accordingly, people seeking recovery are encouraged to take advantage of currently available and effective psychotherapy treatment, as well as existingFDA-approved medications for alcohol use disorder, untilresearch on the effectiveness of psilocybin progresses to a point where it is an available treatment.
For treatment professionals and treatment systems: The study findings showed greater reductions in drinking outcomes with psilocybin and psychotherapy compared to placebo and psychotherapy. However, because psilocybin is not yet an available treatment for alcohol use disorder, treatment professionals who continue to offer currently available and effective psychotherapy treatments are likely to still see improvements in their patients with alcohol use disorder. Further, the study findings also highlight the potential role of expectations, since participants often knew which medication they received. Professionals who use that information to promote positive expectations of treatment among their patients therefore may observe better outcomes.
For scientists:The current study suggests there are some potential benefits of treating alcohol use disorder with psilocybin. However, this was the first recent study conducted to experimentally evaluate the effects of psilocybin on alcohol use disorder and there was a small sample size with almost universal unblinding of the participants to their study condition. Accordingly, more rigorous experimental studies are needed with larger sample sizes to more thoroughly investigate efficacy, as well as the optimal dosage and conditions for administration, subgroup differences, and potential harms. Such research will help the field to understand the effects of psilocybin on alcohol use disorder. Keeping participants blinded to study condition remains a challenge.
For policy makers: Given the potential benefits of psilocybin for alcohol use disorder, re-classifying hallucinogens as drugs that may have medicinal purposes could help to facilitate public support and ignite additional research on its effects. Further, funding for more research on the potential utility of psilocybin and other hallucinogens for treating alcohol and other substance use disorders could shed light on its effectiveness, mechanisms of action, and optimal strategies for administration to enhance safety and promote the best possible outcomes.