Can adding treatments that increase substance-free reward and pleasure enhance intensive outpatient treatment?
Interventions for substance use disorder that try to increase patients’ substance-free reward and pleasure, thereby making recovery efforts more sustainable long-term, are often referred to as “behavioral activation” treatments. This study tested the effects of adding behavioral activation with and without a smartphone app to an existing intensive outpatient treatment to see if it improved outcomes.
Substance use disorder can disrupt the brain’s reward circuitry. This can make it difficult for people with, or seeking recovery from, substance use disorders to access the rewarding and pleasurable experiences needed to replace and compete with the more predictable, potent rewards of substance use. Behavioral activation treatment aims to increase people’s substance-free rewarding and pleasurable experiences, thereby helping provide alternatives to substance use and promoting recovery both in the immediate and long-term. Studies have shown that behavioral activation treatment can be helpful in treating substance use disorders.
The theory underlying behavioral activation is consistent with that of a treatment known as the community reinforcement approach. The theory underlying this clinical approach suggests that by helping people with substance use disorders identify more rewarding activities in their environment, they will learn to associate them with pleasure over time, thereby competing with and eventually replacing their use of substances. Treatment using this approach involves helping patients to examine the functions that are served by substance use and find healthier alternatives that serve similar functions. Likewise, behavioral economics theory also predicts that substance use will decrease if more substance-free rewards are available.
One way to decrease the likelihood of returning to substance use may involve increasing access to relapse prevention information outside of treatment sessions via smartphone apps, which can help patients practice relapse prevention skills and complete daily activity planning. Patients have found smartphone apps to be accessible and helpful in changing substance use behaviors. Further, as a growing number of people with substance use disorder receive outpatient treatment instead of inpatient or residential treatment, it is important to investigate approaches such as these for improving recovery outcomes following this type of treatment.
This study tested the effects of LETS ACT with and without a smartphone app on recovery outcomes compared to publicly funded evidence-based intensive outpatient treatment. Such research can help shed light on the clinical utility of behavioral activation treatment as compared to an intensive outpatient program (i.e., treatment as usual).
HOW WAS THIS STUDY CONDUCTED?
The research team tested the effects of the behavioral activation treatment program LETS ACT with and without a smartphone app compared to publicly funded, abstinence-based, intensive outpatient treatment using a randomized controlled trial design. The researchers were primarily interested in the recovery outcomes of substance use days and related problems.
Participants were deemed not eligible for the study if they: (1) were older than 65 or younger than 18; (2) had less than a fifth-grade English reading level; (3) were experiencing current psychotic symptoms, as measured by the Mini-International Neuropsychiatric Interview; (4) completed more than four weeks of the outpatient program, or (5) were not able to provide written informed consent to participate.
In total, 206 participants were recruited from the outpatient treatment program and randomized to 1 of 3 groups. All participants received treatment as usual, which was the intensive outpatient treatment program. This program is based on the Matrix Model of Intensive Outpatient Treatment – a manualized, evidence-based program that promotes abstinence from substances, teaches skills to prevent returning to use, and introduces patients to mutual support groups.
Through the program, patients received 12 weeks of group therapy for three hours per day, three days per week, in addition to weekly individual case management appointments and up to two optional individual counseling sessions per week. The program required that patients maintain abstinence, which was corroborated by urine toxicology screens during treatment.
In addition to this treatment as usual condition, participants randomized to the LETS ACT behavioral activation treatment group were provided with six 1-hour sessions, delivered twice a week over 3 weeks, that occurred in small groups of 6 or fewer participants. During these sessions, participants were first provided with the treatment’s rationale and goals, which involves strategies for breaking the cycle of negative mood, urges, and maladaptive behaviors by engaging in rewarding behaviors. They were then asked to record daily activities, rate how enjoyable and important they found them to be, and identify activities that are consistent with their values. Finally, they learned to plan and implement these activities in a daily plan, along with planning for solutions to problems they may have adhering to their plan.
In addition to treatment as usual and the LETS ACT program, participants randomized to the smartphone-enhanced group were provided with smartphones and installed the LETS ACT app during the second treatment session. The research team paid for a phone plan and participants could use the phones up through 3 months post-treatment. They were asked to use the app to complete treatment homework and were able to use app features to help with this, such as identifying activities and saving them in a library, making a daily plan, and viewing weekly progress.
The main outcomes of interest were substance use days and substance-related problems. Substance use days were defined as the number of days of any substance use within each assessment period for substances for which participants met a substance use disorder diagnosis as per the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5). Substance-related problems were assessed using the Short Inventory of Problems-Alcohol and Drugs, which is a 15-tem questionnaire that assesses the extent to which participants experienced problems from substance use on a daily basis, from never to daily, across a variety of life areas, including personal, impulse control, and social responsibility.
Participants were assessed prior to and after treatment, as well as every 3 months for 12 months post-treatment, for a total of 6 assessments. Of the randomized participants, 83.98% attended at least 1 post-treatment or follow-up assessment and 64.83% of those retained beyond the pre-treatment assessment attended all 6 follow-ups. Researchers tested the effects of the 3 different conditions (Treatment as Usual vs. Treatment as Usual + LETS ACT vs. Treatment as Usual + LETS ACT + Smartphone app add-on) on the primary outcomes of substance use days and substance-related problems from the pre-treatment assessment to the 12-month assessment.
Of the 206 participants who were randomized, most identified as White (53.9%) and as male (66.6%), with a mean age of 40.29. Many of the participants met criteria for 2 more substance use disorder diagnoses (76.7%) and 2 or more non-substance use disorders (57.3%). On average, participants had not used any substances for approximately 58 days prior to entering treatment, although this number varied widely.
WHAT DID THIS STUDY FIND?
Groups had similar substance use at the 12-month follow-up.
Across all groups, there was an immediate decrease in substance use days from the pre-treatment assessment to the first post-treatment assessment of approximately 10%, but this increased to, or exceeded, the level it was prior to treatment by the 12-month follow-up assessment.
Statistically, across all groups, there was an effect of time on substance use days. Specifically, patients had a lower likelihood of using substances over time relative to when they entered treatment and up through 6-months after starting the study. There was no difference between the study group conditions, however, meaning that all 3 groups had a similar chance of substance use, regardless of which treatment they received.
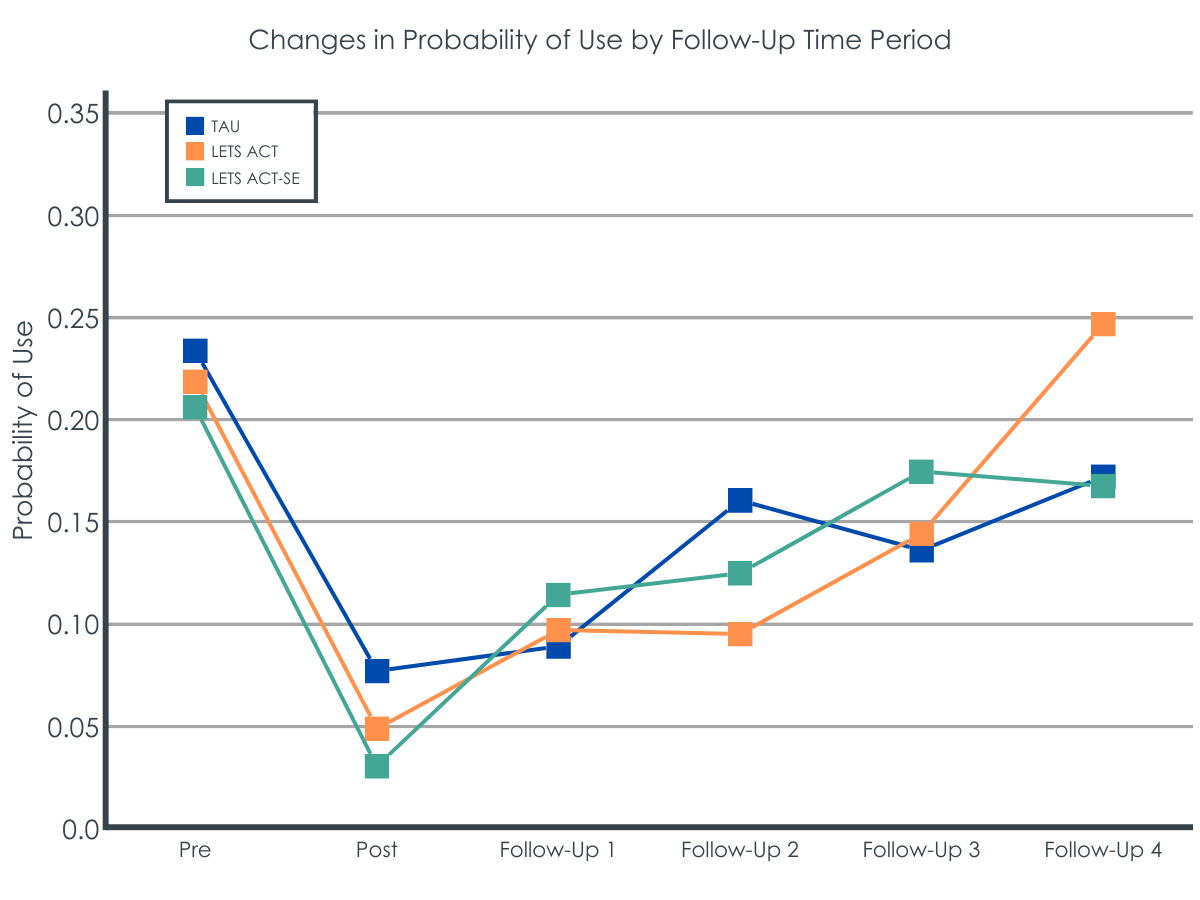
LETS ACT initially reduced the chances of substance use.
Across all groups, there was an immediate decrease in the chances of substance use on any given day from the pre-treatment assessment to the first post-treatment assessment.
However, there were some short-term differences between groups. The chances of substance use on any given day remained lower than pre-treatment until the 1-month follow-up for the treatment as usual group, until the 3-month follow-up for the smartphone-enhanced LETS ACT group, and until the 6-month follow-up for the LETS ACT group. Though interestingly, patients receiving the treatment as usual condition without the behavioral activation had reduced chances of substance use at the 6-month follow-up, despite having less of an effect at the 3-month follow-up. None of these decreases were sustained through the 12-month follow-up across all groups.
Groups reported a similar number of substance-use related problems at the 12-month follow-up.
The type of treatment that patients received also made no difference in the degree to which they experienced substance-related problems over time. Across all groups, the study participants showed a decrease in substance-related problems from the pre-treatment assessment to the 1-month follow-up, and these reductions were sustained until the 12-month follow-up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study tested the effects of LETS ACT and LETS ACT enhanced with a smartphone app on recovery outcomes compared to intensive outpatient treatment. Results showed that there were no differences between these 3 groups in the number of substance use days and substance use-related problems at 12 months following treatment. However, there were decreases in substance use-related problems overall and some initial short-term group differences related to these differing treatment conditions to which patients were randomly assigned. This suggests that adding a behavioral activation treatment to an evidence-based intensive outpatient treatment program and adding a smartphone enhancement to the behavioral activation treatment on top of this kind of outpatient treatment, do not appear to produce any additional benefits over the long-term, but may potentially have some variable short-term beneficial effects.
One likely explanation for these unexpected findings (i.e., similar recovery outcomes across all 3 study groups) is that treatment as usual was an evidence-based and intensive Matrix Model. This model is a comprehensive and empirically-supported treatment that includes introducing patients to mutual support groups, such as 12-step groups, which are themselves a source of behavioral activation. Accordingly, it is possible that the Matrix Model on its own may have produced a kind of “ceiling” for behavioral activation effects, wherein the addition of anything else was unlikely to beat it.
It is often very difficult to show incremental benefits when adding a treatment component to an existing empirically-supported treatment within the same episode of care of the same duration, as was done in this study. Where benefits are observed in treatment studies, they tend to happen more when treatments of longer duration are implemented and compared to shorter treatments (e.g., a treatment is spread out over 6 months instead of 3 months). These longer duration treatments tend to be a better match for the similarly enduring relapse risk associated with meeting the demanding changes that are necessary particularly during the first year of recovery.
In addition, participants entered the intensive outpatient program with an average of 23 days of abstinence in the past 30, and then entered the trial 20 days after starting the outpatient program, resulting in 50+ days of abstinence on average when they started the trial. It is likely that many of the participants were in a higher-level treatment program before stepping down into the intensive outpatient program, which is a common trajectory for individuals seeking recovery. This made the outpatient program an even higher bar for the LETS ACT groups with and without the smartphone to show additional benefit. It is possible that the LETS ACT groups might have added benefit if: (1) the treatment as usual condition was not as comprehensive and empirically-supported as the Matrix Model is; (2) the participants were beginning their recovery at the same time as starting the study instead of 2 months later, or (3) both of these scenarios were true.
Regarding the smartphone-enhanced group, specifically, it is possible that the app did not perform as well as the researchers expected because the phones were provided to the participants and paid for by the research team. It may be that the participants did not use the app as much as they would have if it had been installed on their primary smartphones. Additionally, if they were unable to afford a smartphone prior to joining the study, they may not be accustomed to using smartphone apps in general. Both of these factors may have diluted any potential benefits of the app.
It is quite possible that some patients may have benefitted from the behavioral activation approach more (or less) than others, and these so-called “moderator” effects would not be captured by the average group effects reported in this study. Future research should examine which patient subgroups, if any, may benefit from this additional feature more than others.
Another potential explanation for the unexpected lack of difference between groups on recovery outcomes involves the number of treatment sessions attended, which is especially important for outpatient settings. As with most studies investigating treatments for substance use disorders, the number of treatment sessions attended predicts better outcomes for a longer time. Participants in this study randomized to the LETS ACT group attended 4 of the 6 sessions on average, but this varied considerably, with some only attending 1 session. As such, the lack of effect may be due to inadequate dosage of the behavioral activation treatment. Further, it may be that more than 6 sessions or different timing in the delivery of sessions are needed to achieve benefits. For comparison, some studies suggest that a minimum of 14 sessions of cognitive behavioral therapy are needed to see results.
Participants in the study were also mostly men. It is unclear if the results will generalize to women.
Researchers in the study did not consider differences between specific substances that participants met criteria for their substance use disorders. It is possible that behavioral activation treatments may be more or less effective for one substance versus another.
There was a usually large average amount of abstinent days reported prior to entering the study and being randomized to the studied treatments, suggesting that there may have been only marginal room for improvements in substance use days and problems on the whole. This may have potentially diminished the chances of detecting meaningful differential treatment effects, especially when coupled with the fact that everyone received an already strong and intensive outpatient treatment (Matrix Model).
BOTTOM LINE
This study that compared the effects of adding behavioral activation treatment with and without a smartphone app to an intensive outpatient program showed that there were no meaningful differences between the 3 groups in the number of substance use days and substance use-related problems at 12 months following treatment, but there were decreases in problems overall and some short-term differences. This suggests that adding a behavioral activation treatment program, with or without a smartphone app, to comprehensive, empirically-supported intensive outpatient treatment program, may not improve recovery outcomes long-term.
For individuals and families seeking recovery: Results from this study suggest that behavioral activation treatment is no better than the treatment as usual outpatient treatment program in promoting improved recovery outcomes long-term, but there were decreases in substance use-related problems overall. Accordingly, individuals seeking recovery may be likely to benefit regardless of which treatment program they choose. In the short-term, however, results show that behavioral activation may be helpful for some individuals, suggesting that increasing substance-free rewarding experiences can be helpful early in substance use treatment.
For treatment professionals and treatment systems: This study’s results suggest that behavioral activation treatment and treatment as usual outpatient programs can both be helpful in decreasing substance-use related problems. Treatment professionals and systems that offer patients with substance use disorder different treatment programs may therefore see their patients benefit regardless of which program they choose. However, results also show that there may be small, short-term effects from behavioral activation treatment, suggesting this type of treatment may be helpful for some individuals more immediately, but will need additional support longer term.
For scientists:This study showed no differences between the behavioral activation treatment, behavioral activation treatment with smartphone app, and treatment as usual outpatient groups in the number of substance use days and substance use-related problems at 12 months following treatment. There were, however, short-term effects observed in both of the behavioral activation groups, pointing to the need for additional research to investigate what mechanisms are contributing to the short- and long-term effects. Additional research that examines strategies for enhancing substance-free rewarding activities beyond those supported by LETS ACT could help to improve treatment outcomes. More broadly, future research that investigates approaches for supporting people following outpatient treatment to sustain recovery benefits can improve recovery outcomes in the long-term.
For policy makers: The current study showed that behavioral activation treatment is no better than the treatment as usual outpatient treatment program in promoting improved recovery outcomes long-term, but there were decreases in substance use and related problems overall regardless. As such, if policymakers support policies that promote better access to treatment broadly, there are likely to be public health benefits. Further, there is a broader need for strategies that support people following outpatient treatment in sustaining recovery benefits over time. Funding for such studies can shed light on what approaches are most helpful for the long term and which can improve recovery outcomes.
Substance use disorder can disrupt the brain’s reward circuitry. This can make it difficult for people with, or seeking recovery from, substance use disorders to access the rewarding and pleasurable experiences needed to replace and compete with the more predictable, potent rewards of substance use. Behavioral activation treatment aims to increase people’s substance-free rewarding and pleasurable experiences, thereby helping provide alternatives to substance use and promoting recovery both in the immediate and long-term. Studies have shown that behavioral activation treatment can be helpful in treating substance use disorders.
The theory underlying behavioral activation is consistent with that of a treatment known as the community reinforcement approach. The theory underlying this clinical approach suggests that by helping people with substance use disorders identify more rewarding activities in their environment, they will learn to associate them with pleasure over time, thereby competing with and eventually replacing their use of substances. Treatment using this approach involves helping patients to examine the functions that are served by substance use and find healthier alternatives that serve similar functions. Likewise, behavioral economics theory also predicts that substance use will decrease if more substance-free rewards are available.
One way to decrease the likelihood of returning to substance use may involve increasing access to relapse prevention information outside of treatment sessions via smartphone apps, which can help patients practice relapse prevention skills and complete daily activity planning. Patients have found smartphone apps to be accessible and helpful in changing substance use behaviors. Further, as a growing number of people with substance use disorder receive outpatient treatment instead of inpatient or residential treatment, it is important to investigate approaches such as these for improving recovery outcomes following this type of treatment.
This study tested the effects of LETS ACT with and without a smartphone app on recovery outcomes compared to publicly funded evidence-based intensive outpatient treatment. Such research can help shed light on the clinical utility of behavioral activation treatment as compared to an intensive outpatient program (i.e., treatment as usual).
HOW WAS THIS STUDY CONDUCTED?
The research team tested the effects of the behavioral activation treatment program LETS ACT with and without a smartphone app compared to publicly funded, abstinence-based, intensive outpatient treatment using a randomized controlled trial design. The researchers were primarily interested in the recovery outcomes of substance use days and related problems.
Participants were deemed not eligible for the study if they: (1) were older than 65 or younger than 18; (2) had less than a fifth-grade English reading level; (3) were experiencing current psychotic symptoms, as measured by the Mini-International Neuropsychiatric Interview; (4) completed more than four weeks of the outpatient program, or (5) were not able to provide written informed consent to participate.
In total, 206 participants were recruited from the outpatient treatment program and randomized to 1 of 3 groups. All participants received treatment as usual, which was the intensive outpatient treatment program. This program is based on the Matrix Model of Intensive Outpatient Treatment – a manualized, evidence-based program that promotes abstinence from substances, teaches skills to prevent returning to use, and introduces patients to mutual support groups.
Through the program, patients received 12 weeks of group therapy for three hours per day, three days per week, in addition to weekly individual case management appointments and up to two optional individual counseling sessions per week. The program required that patients maintain abstinence, which was corroborated by urine toxicology screens during treatment.
In addition to this treatment as usual condition, participants randomized to the LETS ACT behavioral activation treatment group were provided with six 1-hour sessions, delivered twice a week over 3 weeks, that occurred in small groups of 6 or fewer participants. During these sessions, participants were first provided with the treatment’s rationale and goals, which involves strategies for breaking the cycle of negative mood, urges, and maladaptive behaviors by engaging in rewarding behaviors. They were then asked to record daily activities, rate how enjoyable and important they found them to be, and identify activities that are consistent with their values. Finally, they learned to plan and implement these activities in a daily plan, along with planning for solutions to problems they may have adhering to their plan.
In addition to treatment as usual and the LETS ACT program, participants randomized to the smartphone-enhanced group were provided with smartphones and installed the LETS ACT app during the second treatment session. The research team paid for a phone plan and participants could use the phones up through 3 months post-treatment. They were asked to use the app to complete treatment homework and were able to use app features to help with this, such as identifying activities and saving them in a library, making a daily plan, and viewing weekly progress.
The main outcomes of interest were substance use days and substance-related problems. Substance use days were defined as the number of days of any substance use within each assessment period for substances for which participants met a substance use disorder diagnosis as per the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5). Substance-related problems were assessed using the Short Inventory of Problems-Alcohol and Drugs, which is a 15-tem questionnaire that assesses the extent to which participants experienced problems from substance use on a daily basis, from never to daily, across a variety of life areas, including personal, impulse control, and social responsibility.
Participants were assessed prior to and after treatment, as well as every 3 months for 12 months post-treatment, for a total of 6 assessments. Of the randomized participants, 83.98% attended at least 1 post-treatment or follow-up assessment and 64.83% of those retained beyond the pre-treatment assessment attended all 6 follow-ups. Researchers tested the effects of the 3 different conditions (Treatment as Usual vs. Treatment as Usual + LETS ACT vs. Treatment as Usual + LETS ACT + Smartphone app add-on) on the primary outcomes of substance use days and substance-related problems from the pre-treatment assessment to the 12-month assessment.
Of the 206 participants who were randomized, most identified as White (53.9%) and as male (66.6%), with a mean age of 40.29. Many of the participants met criteria for 2 more substance use disorder diagnoses (76.7%) and 2 or more non-substance use disorders (57.3%). On average, participants had not used any substances for approximately 58 days prior to entering treatment, although this number varied widely.
WHAT DID THIS STUDY FIND?
Groups had similar substance use at the 12-month follow-up.
Across all groups, there was an immediate decrease in substance use days from the pre-treatment assessment to the first post-treatment assessment of approximately 10%, but this increased to, or exceeded, the level it was prior to treatment by the 12-month follow-up assessment.
Statistically, across all groups, there was an effect of time on substance use days. Specifically, patients had a lower likelihood of using substances over time relative to when they entered treatment and up through 6-months after starting the study. There was no difference between the study group conditions, however, meaning that all 3 groups had a similar chance of substance use, regardless of which treatment they received.
LETS ACT initially reduced the chances of substance use.
Across all groups, there was an immediate decrease in the chances of substance use on any given day from the pre-treatment assessment to the first post-treatment assessment.
However, there were some short-term differences between groups. The chances of substance use on any given day remained lower than pre-treatment until the 1-month follow-up for the treatment as usual group, until the 3-month follow-up for the smartphone-enhanced LETS ACT group, and until the 6-month follow-up for the LETS ACT group. Though interestingly, patients receiving the treatment as usual condition without the behavioral activation had reduced chances of substance use at the 6-month follow-up, despite having less of an effect at the 3-month follow-up. None of these decreases were sustained through the 12-month follow-up across all groups.
Groups reported a similar number of substance-use related problems at the 12-month follow-up.
The type of treatment that patients received also made no difference in the degree to which they experienced substance-related problems over time. Across all groups, the study participants showed a decrease in substance-related problems from the pre-treatment assessment to the 1-month follow-up, and these reductions were sustained until the 12-month follow-up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study tested the effects of LETS ACT and LETS ACT enhanced with a smartphone app on recovery outcomes compared to intensive outpatient treatment. Results showed that there were no differences between these 3 groups in the number of substance use days and substance use-related problems at 12 months following treatment. However, there were decreases in substance use-related problems overall and some initial short-term group differences related to these differing treatment conditions to which patients were randomly assigned. This suggests that adding a behavioral activation treatment to an evidence-based intensive outpatient treatment program and adding a smartphone enhancement to the behavioral activation treatment on top of this kind of outpatient treatment, do not appear to produce any additional benefits over the long-term, but may potentially have some variable short-term beneficial effects.
One likely explanation for these unexpected findings (i.e., similar recovery outcomes across all 3 study groups) is that treatment as usual was an evidence-based and intensive Matrix Model. This model is a comprehensive and empirically-supported treatment that includes introducing patients to mutual support groups, such as 12-step groups, which are themselves a source of behavioral activation. Accordingly, it is possible that the Matrix Model on its own may have produced a kind of “ceiling” for behavioral activation effects, wherein the addition of anything else was unlikely to beat it.
It is often very difficult to show incremental benefits when adding a treatment component to an existing empirically-supported treatment within the same episode of care of the same duration, as was done in this study. Where benefits are observed in treatment studies, they tend to happen more when treatments of longer duration are implemented and compared to shorter treatments (e.g., a treatment is spread out over 6 months instead of 3 months). These longer duration treatments tend to be a better match for the similarly enduring relapse risk associated with meeting the demanding changes that are necessary particularly during the first year of recovery.
In addition, participants entered the intensive outpatient program with an average of 23 days of abstinence in the past 30, and then entered the trial 20 days after starting the outpatient program, resulting in 50+ days of abstinence on average when they started the trial. It is likely that many of the participants were in a higher-level treatment program before stepping down into the intensive outpatient program, which is a common trajectory for individuals seeking recovery. This made the outpatient program an even higher bar for the LETS ACT groups with and without the smartphone to show additional benefit. It is possible that the LETS ACT groups might have added benefit if: (1) the treatment as usual condition was not as comprehensive and empirically-supported as the Matrix Model is; (2) the participants were beginning their recovery at the same time as starting the study instead of 2 months later, or (3) both of these scenarios were true.
Regarding the smartphone-enhanced group, specifically, it is possible that the app did not perform as well as the researchers expected because the phones were provided to the participants and paid for by the research team. It may be that the participants did not use the app as much as they would have if it had been installed on their primary smartphones. Additionally, if they were unable to afford a smartphone prior to joining the study, they may not be accustomed to using smartphone apps in general. Both of these factors may have diluted any potential benefits of the app.
It is quite possible that some patients may have benefitted from the behavioral activation approach more (or less) than others, and these so-called “moderator” effects would not be captured by the average group effects reported in this study. Future research should examine which patient subgroups, if any, may benefit from this additional feature more than others.
Another potential explanation for the unexpected lack of difference between groups on recovery outcomes involves the number of treatment sessions attended, which is especially important for outpatient settings. As with most studies investigating treatments for substance use disorders, the number of treatment sessions attended predicts better outcomes for a longer time. Participants in this study randomized to the LETS ACT group attended 4 of the 6 sessions on average, but this varied considerably, with some only attending 1 session. As such, the lack of effect may be due to inadequate dosage of the behavioral activation treatment. Further, it may be that more than 6 sessions or different timing in the delivery of sessions are needed to achieve benefits. For comparison, some studies suggest that a minimum of 14 sessions of cognitive behavioral therapy are needed to see results.
Participants in the study were also mostly men. It is unclear if the results will generalize to women.
Researchers in the study did not consider differences between specific substances that participants met criteria for their substance use disorders. It is possible that behavioral activation treatments may be more or less effective for one substance versus another.
There was a usually large average amount of abstinent days reported prior to entering the study and being randomized to the studied treatments, suggesting that there may have been only marginal room for improvements in substance use days and problems on the whole. This may have potentially diminished the chances of detecting meaningful differential treatment effects, especially when coupled with the fact that everyone received an already strong and intensive outpatient treatment (Matrix Model).
BOTTOM LINE
This study that compared the effects of adding behavioral activation treatment with and without a smartphone app to an intensive outpatient program showed that there were no meaningful differences between the 3 groups in the number of substance use days and substance use-related problems at 12 months following treatment, but there were decreases in problems overall and some short-term differences. This suggests that adding a behavioral activation treatment program, with or without a smartphone app, to comprehensive, empirically-supported intensive outpatient treatment program, may not improve recovery outcomes long-term.
For individuals and families seeking recovery: Results from this study suggest that behavioral activation treatment is no better than the treatment as usual outpatient treatment program in promoting improved recovery outcomes long-term, but there were decreases in substance use-related problems overall. Accordingly, individuals seeking recovery may be likely to benefit regardless of which treatment program they choose. In the short-term, however, results show that behavioral activation may be helpful for some individuals, suggesting that increasing substance-free rewarding experiences can be helpful early in substance use treatment.
For treatment professionals and treatment systems: This study’s results suggest that behavioral activation treatment and treatment as usual outpatient programs can both be helpful in decreasing substance-use related problems. Treatment professionals and systems that offer patients with substance use disorder different treatment programs may therefore see their patients benefit regardless of which program they choose. However, results also show that there may be small, short-term effects from behavioral activation treatment, suggesting this type of treatment may be helpful for some individuals more immediately, but will need additional support longer term.
For scientists:This study showed no differences between the behavioral activation treatment, behavioral activation treatment with smartphone app, and treatment as usual outpatient groups in the number of substance use days and substance use-related problems at 12 months following treatment. There were, however, short-term effects observed in both of the behavioral activation groups, pointing to the need for additional research to investigate what mechanisms are contributing to the short- and long-term effects. Additional research that examines strategies for enhancing substance-free rewarding activities beyond those supported by LETS ACT could help to improve treatment outcomes. More broadly, future research that investigates approaches for supporting people following outpatient treatment to sustain recovery benefits can improve recovery outcomes in the long-term.
For policy makers: The current study showed that behavioral activation treatment is no better than the treatment as usual outpatient treatment program in promoting improved recovery outcomes long-term, but there were decreases in substance use and related problems overall regardless. As such, if policymakers support policies that promote better access to treatment broadly, there are likely to be public health benefits. Further, there is a broader need for strategies that support people following outpatient treatment in sustaining recovery benefits over time. Funding for such studies can shed light on what approaches are most helpful for the long term and which can improve recovery outcomes.
Substance use disorder can disrupt the brain’s reward circuitry. This can make it difficult for people with, or seeking recovery from, substance use disorders to access the rewarding and pleasurable experiences needed to replace and compete with the more predictable, potent rewards of substance use. Behavioral activation treatment aims to increase people’s substance-free rewarding and pleasurable experiences, thereby helping provide alternatives to substance use and promoting recovery both in the immediate and long-term. Studies have shown that behavioral activation treatment can be helpful in treating substance use disorders.
The theory underlying behavioral activation is consistent with that of a treatment known as the community reinforcement approach. The theory underlying this clinical approach suggests that by helping people with substance use disorders identify more rewarding activities in their environment, they will learn to associate them with pleasure over time, thereby competing with and eventually replacing their use of substances. Treatment using this approach involves helping patients to examine the functions that are served by substance use and find healthier alternatives that serve similar functions. Likewise, behavioral economics theory also predicts that substance use will decrease if more substance-free rewards are available.
One way to decrease the likelihood of returning to substance use may involve increasing access to relapse prevention information outside of treatment sessions via smartphone apps, which can help patients practice relapse prevention skills and complete daily activity planning. Patients have found smartphone apps to be accessible and helpful in changing substance use behaviors. Further, as a growing number of people with substance use disorder receive outpatient treatment instead of inpatient or residential treatment, it is important to investigate approaches such as these for improving recovery outcomes following this type of treatment.
This study tested the effects of LETS ACT with and without a smartphone app on recovery outcomes compared to publicly funded evidence-based intensive outpatient treatment. Such research can help shed light on the clinical utility of behavioral activation treatment as compared to an intensive outpatient program (i.e., treatment as usual).
HOW WAS THIS STUDY CONDUCTED?
The research team tested the effects of the behavioral activation treatment program LETS ACT with and without a smartphone app compared to publicly funded, abstinence-based, intensive outpatient treatment using a randomized controlled trial design. The researchers were primarily interested in the recovery outcomes of substance use days and related problems.
Participants were deemed not eligible for the study if they: (1) were older than 65 or younger than 18; (2) had less than a fifth-grade English reading level; (3) were experiencing current psychotic symptoms, as measured by the Mini-International Neuropsychiatric Interview; (4) completed more than four weeks of the outpatient program, or (5) were not able to provide written informed consent to participate.
In total, 206 participants were recruited from the outpatient treatment program and randomized to 1 of 3 groups. All participants received treatment as usual, which was the intensive outpatient treatment program. This program is based on the Matrix Model of Intensive Outpatient Treatment – a manualized, evidence-based program that promotes abstinence from substances, teaches skills to prevent returning to use, and introduces patients to mutual support groups.
Through the program, patients received 12 weeks of group therapy for three hours per day, three days per week, in addition to weekly individual case management appointments and up to two optional individual counseling sessions per week. The program required that patients maintain abstinence, which was corroborated by urine toxicology screens during treatment.
In addition to this treatment as usual condition, participants randomized to the LETS ACT behavioral activation treatment group were provided with six 1-hour sessions, delivered twice a week over 3 weeks, that occurred in small groups of 6 or fewer participants. During these sessions, participants were first provided with the treatment’s rationale and goals, which involves strategies for breaking the cycle of negative mood, urges, and maladaptive behaviors by engaging in rewarding behaviors. They were then asked to record daily activities, rate how enjoyable and important they found them to be, and identify activities that are consistent with their values. Finally, they learned to plan and implement these activities in a daily plan, along with planning for solutions to problems they may have adhering to their plan.
In addition to treatment as usual and the LETS ACT program, participants randomized to the smartphone-enhanced group were provided with smartphones and installed the LETS ACT app during the second treatment session. The research team paid for a phone plan and participants could use the phones up through 3 months post-treatment. They were asked to use the app to complete treatment homework and were able to use app features to help with this, such as identifying activities and saving them in a library, making a daily plan, and viewing weekly progress.
The main outcomes of interest were substance use days and substance-related problems. Substance use days were defined as the number of days of any substance use within each assessment period for substances for which participants met a substance use disorder diagnosis as per the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5). Substance-related problems were assessed using the Short Inventory of Problems-Alcohol and Drugs, which is a 15-tem questionnaire that assesses the extent to which participants experienced problems from substance use on a daily basis, from never to daily, across a variety of life areas, including personal, impulse control, and social responsibility.
Participants were assessed prior to and after treatment, as well as every 3 months for 12 months post-treatment, for a total of 6 assessments. Of the randomized participants, 83.98% attended at least 1 post-treatment or follow-up assessment and 64.83% of those retained beyond the pre-treatment assessment attended all 6 follow-ups. Researchers tested the effects of the 3 different conditions (Treatment as Usual vs. Treatment as Usual + LETS ACT vs. Treatment as Usual + LETS ACT + Smartphone app add-on) on the primary outcomes of substance use days and substance-related problems from the pre-treatment assessment to the 12-month assessment.
Of the 206 participants who were randomized, most identified as White (53.9%) and as male (66.6%), with a mean age of 40.29. Many of the participants met criteria for 2 more substance use disorder diagnoses (76.7%) and 2 or more non-substance use disorders (57.3%). On average, participants had not used any substances for approximately 58 days prior to entering treatment, although this number varied widely.
WHAT DID THIS STUDY FIND?
Groups had similar substance use at the 12-month follow-up.
Across all groups, there was an immediate decrease in substance use days from the pre-treatment assessment to the first post-treatment assessment of approximately 10%, but this increased to, or exceeded, the level it was prior to treatment by the 12-month follow-up assessment.
Statistically, across all groups, there was an effect of time on substance use days. Specifically, patients had a lower likelihood of using substances over time relative to when they entered treatment and up through 6-months after starting the study. There was no difference between the study group conditions, however, meaning that all 3 groups had a similar chance of substance use, regardless of which treatment they received.
LETS ACT initially reduced the chances of substance use.
Across all groups, there was an immediate decrease in the chances of substance use on any given day from the pre-treatment assessment to the first post-treatment assessment.
However, there were some short-term differences between groups. The chances of substance use on any given day remained lower than pre-treatment until the 1-month follow-up for the treatment as usual group, until the 3-month follow-up for the smartphone-enhanced LETS ACT group, and until the 6-month follow-up for the LETS ACT group. Though interestingly, patients receiving the treatment as usual condition without the behavioral activation had reduced chances of substance use at the 6-month follow-up, despite having less of an effect at the 3-month follow-up. None of these decreases were sustained through the 12-month follow-up across all groups.
Groups reported a similar number of substance-use related problems at the 12-month follow-up.
The type of treatment that patients received also made no difference in the degree to which they experienced substance-related problems over time. Across all groups, the study participants showed a decrease in substance-related problems from the pre-treatment assessment to the 1-month follow-up, and these reductions were sustained until the 12-month follow-up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study tested the effects of LETS ACT and LETS ACT enhanced with a smartphone app on recovery outcomes compared to intensive outpatient treatment. Results showed that there were no differences between these 3 groups in the number of substance use days and substance use-related problems at 12 months following treatment. However, there were decreases in substance use-related problems overall and some initial short-term group differences related to these differing treatment conditions to which patients were randomly assigned. This suggests that adding a behavioral activation treatment to an evidence-based intensive outpatient treatment program and adding a smartphone enhancement to the behavioral activation treatment on top of this kind of outpatient treatment, do not appear to produce any additional benefits over the long-term, but may potentially have some variable short-term beneficial effects.
One likely explanation for these unexpected findings (i.e., similar recovery outcomes across all 3 study groups) is that treatment as usual was an evidence-based and intensive Matrix Model. This model is a comprehensive and empirically-supported treatment that includes introducing patients to mutual support groups, such as 12-step groups, which are themselves a source of behavioral activation. Accordingly, it is possible that the Matrix Model on its own may have produced a kind of “ceiling” for behavioral activation effects, wherein the addition of anything else was unlikely to beat it.
It is often very difficult to show incremental benefits when adding a treatment component to an existing empirically-supported treatment within the same episode of care of the same duration, as was done in this study. Where benefits are observed in treatment studies, they tend to happen more when treatments of longer duration are implemented and compared to shorter treatments (e.g., a treatment is spread out over 6 months instead of 3 months). These longer duration treatments tend to be a better match for the similarly enduring relapse risk associated with meeting the demanding changes that are necessary particularly during the first year of recovery.
In addition, participants entered the intensive outpatient program with an average of 23 days of abstinence in the past 30, and then entered the trial 20 days after starting the outpatient program, resulting in 50+ days of abstinence on average when they started the trial. It is likely that many of the participants were in a higher-level treatment program before stepping down into the intensive outpatient program, which is a common trajectory for individuals seeking recovery. This made the outpatient program an even higher bar for the LETS ACT groups with and without the smartphone to show additional benefit. It is possible that the LETS ACT groups might have added benefit if: (1) the treatment as usual condition was not as comprehensive and empirically-supported as the Matrix Model is; (2) the participants were beginning their recovery at the same time as starting the study instead of 2 months later, or (3) both of these scenarios were true.
Regarding the smartphone-enhanced group, specifically, it is possible that the app did not perform as well as the researchers expected because the phones were provided to the participants and paid for by the research team. It may be that the participants did not use the app as much as they would have if it had been installed on their primary smartphones. Additionally, if they were unable to afford a smartphone prior to joining the study, they may not be accustomed to using smartphone apps in general. Both of these factors may have diluted any potential benefits of the app.
It is quite possible that some patients may have benefitted from the behavioral activation approach more (or less) than others, and these so-called “moderator” effects would not be captured by the average group effects reported in this study. Future research should examine which patient subgroups, if any, may benefit from this additional feature more than others.
Another potential explanation for the unexpected lack of difference between groups on recovery outcomes involves the number of treatment sessions attended, which is especially important for outpatient settings. As with most studies investigating treatments for substance use disorders, the number of treatment sessions attended predicts better outcomes for a longer time. Participants in this study randomized to the LETS ACT group attended 4 of the 6 sessions on average, but this varied considerably, with some only attending 1 session. As such, the lack of effect may be due to inadequate dosage of the behavioral activation treatment. Further, it may be that more than 6 sessions or different timing in the delivery of sessions are needed to achieve benefits. For comparison, some studies suggest that a minimum of 14 sessions of cognitive behavioral therapy are needed to see results.
Participants in the study were also mostly men. It is unclear if the results will generalize to women.
Researchers in the study did not consider differences between specific substances that participants met criteria for their substance use disorders. It is possible that behavioral activation treatments may be more or less effective for one substance versus another.
There was a usually large average amount of abstinent days reported prior to entering the study and being randomized to the studied treatments, suggesting that there may have been only marginal room for improvements in substance use days and problems on the whole. This may have potentially diminished the chances of detecting meaningful differential treatment effects, especially when coupled with the fact that everyone received an already strong and intensive outpatient treatment (Matrix Model).
BOTTOM LINE
This study that compared the effects of adding behavioral activation treatment with and without a smartphone app to an intensive outpatient program showed that there were no meaningful differences between the 3 groups in the number of substance use days and substance use-related problems at 12 months following treatment, but there were decreases in problems overall and some short-term differences. This suggests that adding a behavioral activation treatment program, with or without a smartphone app, to comprehensive, empirically-supported intensive outpatient treatment program, may not improve recovery outcomes long-term.
For individuals and families seeking recovery: Results from this study suggest that behavioral activation treatment is no better than the treatment as usual outpatient treatment program in promoting improved recovery outcomes long-term, but there were decreases in substance use-related problems overall. Accordingly, individuals seeking recovery may be likely to benefit regardless of which treatment program they choose. In the short-term, however, results show that behavioral activation may be helpful for some individuals, suggesting that increasing substance-free rewarding experiences can be helpful early in substance use treatment.
For treatment professionals and treatment systems: This study’s results suggest that behavioral activation treatment and treatment as usual outpatient programs can both be helpful in decreasing substance-use related problems. Treatment professionals and systems that offer patients with substance use disorder different treatment programs may therefore see their patients benefit regardless of which program they choose. However, results also show that there may be small, short-term effects from behavioral activation treatment, suggesting this type of treatment may be helpful for some individuals more immediately, but will need additional support longer term.
For scientists:This study showed no differences between the behavioral activation treatment, behavioral activation treatment with smartphone app, and treatment as usual outpatient groups in the number of substance use days and substance use-related problems at 12 months following treatment. There were, however, short-term effects observed in both of the behavioral activation groups, pointing to the need for additional research to investigate what mechanisms are contributing to the short- and long-term effects. Additional research that examines strategies for enhancing substance-free rewarding activities beyond those supported by LETS ACT could help to improve treatment outcomes. More broadly, future research that investigates approaches for supporting people following outpatient treatment to sustain recovery benefits can improve recovery outcomes in the long-term.
For policy makers: The current study showed that behavioral activation treatment is no better than the treatment as usual outpatient treatment program in promoting improved recovery outcomes long-term, but there were decreases in substance use and related problems overall regardless. As such, if policymakers support policies that promote better access to treatment broadly, there are likely to be public health benefits. Further, there is a broader need for strategies that support people following outpatient treatment in sustaining recovery benefits over time. Funding for such studies can shed light on what approaches are most helpful for the long term and which can improve recovery outcomes.