Addressing the mental health of patients’ family and friends
Alcohol use disorder conveys direct harms to individual sufferers, but also to family and friends. This study examined alcohol use disorder patients’, and their concerned others’, characteristics and behaviors that were associated with better mental health among family and friends in the year following treatment.
The financial, health care, and criminal justice impacts of alcohol use disorder and other harmful alcohol use are borne by the individual with the disorder, as well as others in their family and community. More than half of US adults reported that a family member had experienced addiction to alcohol. Family or friends may experience direct harms from alcohol intoxication, which increases risk of physical or interpersonal conflict, such as harassment, physical aggression and violence, and driving-related injuries. Alcohol use can lead also to financial or legal strains, often absorbed by the family unit.
More generally, family and friends – sometimes referred to as “concerned significant others” or “concerned others” – may spend substantial time and energy worried or upset regarding their loved one using the substance, which can interfere with functioning and increase the likelihood of mental health challenges such as insomnia, depression or anxiety.
While not all experience significant harms, family and friends are at an increased risk of experiencing a range of harms and need their own support throughout not only when symptoms are at their worst, but also throughout treatment and into the early months and years of recovery.
Clearly, not all concerned others are impacted equally, with some particularly vulnerable to the mental health impacts of their loved one’s alcohol use disorder. Better understanding of the factors that might influence this vulnerability may help inform strategies that specifically target family and friends’ well-being.
This study examined characteristics of concerned others and of patients with alcohol use disorder that impact quality of life and mental health over the first year of a recovery attempt following treatment.
HOW WAS THIS STUDY CONDUCTED?
The current study recruited 279 pairs of patients enrolled in residential alcohol use disorder treatment and their concerned others to complete surveys 4 times over 1 year. Patients were asked to name potential concerned others that were at least 18 years old and supportive of the patient’s treatment attendance. There were no requirements about the type of relationship (partner, family member, friend, coworker). Patients and concerned others then completed surveys at baseline, and 3, 6, and 12-month follow-ups.
The researchers examined which patient and concerned other characteristics and behaviors predicted changes in concerned other mental health and quality of life over time. Patient characteristics and behaviors included substance use severity, treatment and Alcoholic Anonymous (AA) participation, relationship satisfaction and conflict (from the patient’s perspective), mental health, and criminal justice involvement. Concerned other characteristics included their age, gender, marital status, race, education, income, employment status, relationship to the patient, social support, past 30-day alcohol use status, perceived stigma toward patient’s alcohol use, type of communication to the patient about alcohol use (e.g., controlling and nurturing), and coping skills.
The researchers evaluated associations between all predictors and outcomes separately, and all that were significant were included in a larger model to determine whether each factor was an independent predictor of concerned others’ a) mental health, and b) quality of life over time combining 3, 6, and 12-month follow-ups after holding the other important patient and concerned other factors at baseline constant, increasing confidence that these factors might be causally-related to the concerned others’ mental health.
The patients and their concerned others were recruited as a part of a randomized controlled trial evaluating the efficacy of a 4-session intensive referral program to, Al-Anon , the 12-step mutual-help group for family and friends of individuals with alcohol and other drug use disorders. The initial study found no effect of the intervention on Al-anon attendance (28% in the Al-anon Intensive Referral, and 21% in the usual care condition). All analyses in this concerned other study controlled for intervention condition.
Concerned others were approximately 52 years of age on average and mostly female (77%), and white (66%). Most had completed at least 13 years of education (68%) and were employed (58%) and approximately half reported greater than $30,000 per year in income. Concerned other relationship types included current or former spouse (33%), parents (25%), siblings (13%) child (11%), friends (15%), and other relatives (3%). Almost two-thirds of the concerned others did not live with the patients (64%). Patients were primarily men (76%), white (69%), unmarried (75%) and unemployed (75%). Patients were 43 years of age on average and reported an average annual income of approximately $25,000.
WHAT DID THIS STUDY FIND?
Family and friends’ mental health improved over the course of the year
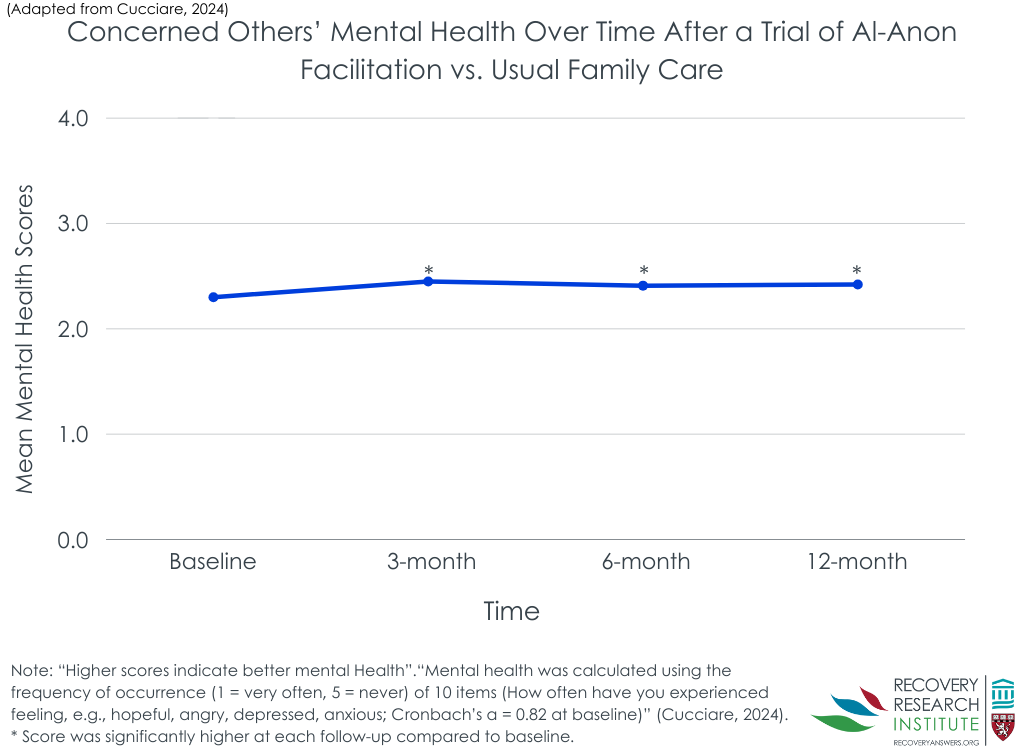
Concerned others’ mental health improved at each subsequent follow up relative to baseline, though only slightly so (see Figure below). Concerned others’ mental health was independently higher for those with greater social support and when patients’ current treatment episode was prompted through criminal justice involvement, controlling for all other variables that were correlated with mental health (e.g., relationship stressors) as well as the concerned others’ age and treatment condition. On the other hand, concerned others’ mental health was independently lower when the concerned other reported higher discrimination stigma and more avoidance coping.
Concerned other quality of life did not improve over the course of the year
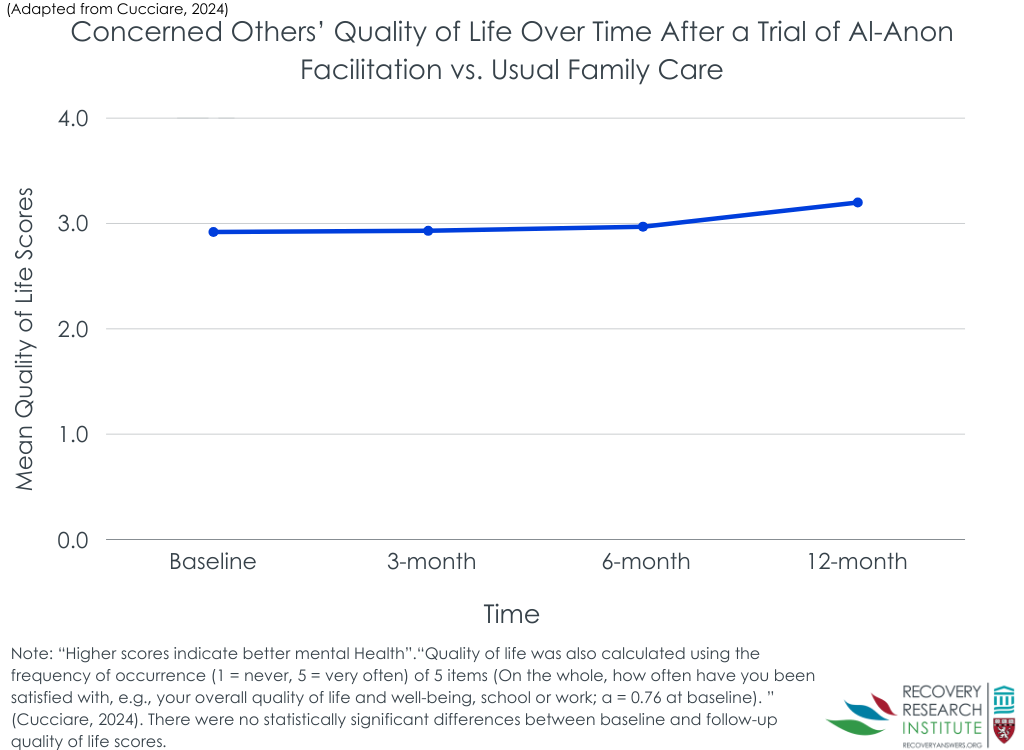
Unlike mental health, concerned others’ quality of life did not improve significantly in general over the course of the year compared to baseline. Being married and having a higher income however, was associated with higher quality of life reported by the concerned other. Also, having higher levels of discrimination stigma (the concerned others’ own experienced stigma regarding their loved one’s alcohol use) was independently associated with lower quality of life.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that concerned other mental health improved significantly over the course of the first year after a loved one entered residential alcohol use disorder treatment. This improvement, however, was relatively modest – about an average of 2.3 to 2.5 on symptom frequency from 1 (very often) to 5 (never). Concerned others’ quality of life did not change over time. Some individuals in the study may have had larger increases in mental health and others decreases or no change – to produce this modest benefit. Thus, understanding what predicts better mental health was a critical question answered here. For example, more social support and less avoidance coping were associated with better mental health. Taken together, when concerned others face their love one’s alcohol use disorder “head on”, but with ample social support themselves, they may have the best chance of improved mental health.
Discrimination stigma, which measures the concerned others’ own experience of discrimination due to their loved one’s alcohol use (e.g., “People have insulted me because of my drinker’s alcohol use.”), was associated with worse mental health and quality of life, even after controlling for substance use severity of the patient. Stigma is associated with worse outcomes for the individual, and this study builds on these findings by suggesting that this stigma may also harm the individual who perpetuates the stigma. Future studies may consider targeted stigma in concerned others – for example, through communication skills training on how to talk with others about their loved one’s drinking or cognitive strategies to reduce potential self-blame.
There are a number of resources that have been developed to support family and friends of people who use substances. Perhaps the most widely known is Al-Anon, which supports concerned others through a 12-step lens. Other mutual-help groups for family and friends are becoming increasingly popular alternatives for those with loved ones who prefer a more secular approach to recovery, like SMART recovery. Just as AA groups have Al-Anon family parallels, so too do SMART groups have a parallel SMART Family and Friends designed to help facilitate social support and coping skills for concerned others. Also, Learn2Cope caters primarily to parents of young people with opioid and other substance use disorders. Importantly, however, given that all patients in this study received either usual care – psychoeducation for family members delivered by the patient’s treatment program – or an Al-Anon facilitation, and mental health gains were modest while quality of life did not change over time – additional help (e.g., individual therapy tailored specifically to concerned others) may be needed.
The study measures quality of life and mental health 4 times over a 1 year period. However, mental health may more broadly shift along smaller timescales, and future research may consider measuring factors weekly or daily to understand whether activities at that scale – e.g., on a given day – may boost adaptive coping and mental health.
Also, as study authors note, this residential alcohol use disorder treatment sample – which had low recovery capital and high clinical severity – may not generalize to individuals with lower severity or recruited from outpatient treatment.
BOTTOM LINE
If you are a concerned other struggling with your loved one’s alcohol use disorder, the first year following treatment may be associated with some modest improvements in mental health, but not always other broader areas of life quality, for close supports. Not avoiding, but rather facing a loved one’s substance use “head on”, while seeking social support to cope with the increased stress this may provoke, may help improve mental health over time. Further, identifying and addressing stigmatizing beliefs about a loved one’s alcohol use, in addition to finding healthy ways to cope with discrimination from others, may improve outcomes.
For individuals and families seeking recovery: Alcohol use disorder can be difficult for concerned others. If you have a loved one who is experiencing harms from alcohol use, you may also be impacted, and you are not alone. Not avoiding, but rather, facing a loved one’s substance use “head on”, while seeking social support to cope with the increased stress this may provoke, may help improve your mental health over time. There are resources, such as Al-Anon or SMART Family and Friends, to support a concerned other through their loved one’s substance use disorder, though some often benefit from their own individual therapy alone or in addition to participation in one of these community peer-led resources.
For treatment professionals and treatment systems: Some of your patients may be experiencing lower levels of mental health and quality of life in part due to concern for personal safety or the safety of a loved one who has alcohol and other drug use disorders. It is important to assess substance use for the individual but also whether the individual is experiencing any stress from a loved one’s substance use. While there are community resources available, such as Al-Anon and SMART Family and Friends, if seeing a patient like this in individual therapy, helping equip them with strategies to help their loved one and to seek out their own social support will likely yield important benefits.
For scientists: These findings provide the foundation for future research exploring individual differences, some of which may be addressed through intervention, that predict concerned other mental health and quality of life over the course of remission from alcohol use disorder. Future studies might consider targeting some of these factors through intervention. Qualitative studies that ask concerned others what they think they need, and what types of resources may be or have been, most useful, may be help facilitate more rapid development of resources.
For policy makers: Substance use impacts the individual, concerned others, and broader communities. Continued public health attention to, and, earmarking scientific funding for, concerned others can help address indirect harms that an individuals’ alcohol use disorder has on their friends and family. Strategies that warrant funding include, but are not limited to, those addressing concerned others’ own mental health and those which equip concerned others with skills to support their loved one’s treatment and recovery engagement.
The financial, health care, and criminal justice impacts of alcohol use disorder and other harmful alcohol use are borne by the individual with the disorder, as well as others in their family and community. More than half of US adults reported that a family member had experienced addiction to alcohol. Family or friends may experience direct harms from alcohol intoxication, which increases risk of physical or interpersonal conflict, such as harassment, physical aggression and violence, and driving-related injuries. Alcohol use can lead also to financial or legal strains, often absorbed by the family unit.
More generally, family and friends – sometimes referred to as “concerned significant others” or “concerned others” – may spend substantial time and energy worried or upset regarding their loved one using the substance, which can interfere with functioning and increase the likelihood of mental health challenges such as insomnia, depression or anxiety.
While not all experience significant harms, family and friends are at an increased risk of experiencing a range of harms and need their own support throughout not only when symptoms are at their worst, but also throughout treatment and into the early months and years of recovery.
Clearly, not all concerned others are impacted equally, with some particularly vulnerable to the mental health impacts of their loved one’s alcohol use disorder. Better understanding of the factors that might influence this vulnerability may help inform strategies that specifically target family and friends’ well-being.
This study examined characteristics of concerned others and of patients with alcohol use disorder that impact quality of life and mental health over the first year of a recovery attempt following treatment.
HOW WAS THIS STUDY CONDUCTED?
The current study recruited 279 pairs of patients enrolled in residential alcohol use disorder treatment and their concerned others to complete surveys 4 times over 1 year. Patients were asked to name potential concerned others that were at least 18 years old and supportive of the patient’s treatment attendance. There were no requirements about the type of relationship (partner, family member, friend, coworker). Patients and concerned others then completed surveys at baseline, and 3, 6, and 12-month follow-ups.
The researchers examined which patient and concerned other characteristics and behaviors predicted changes in concerned other mental health and quality of life over time. Patient characteristics and behaviors included substance use severity, treatment and Alcoholic Anonymous (AA) participation, relationship satisfaction and conflict (from the patient’s perspective), mental health, and criminal justice involvement. Concerned other characteristics included their age, gender, marital status, race, education, income, employment status, relationship to the patient, social support, past 30-day alcohol use status, perceived stigma toward patient’s alcohol use, type of communication to the patient about alcohol use (e.g., controlling and nurturing), and coping skills.
The researchers evaluated associations between all predictors and outcomes separately, and all that were significant were included in a larger model to determine whether each factor was an independent predictor of concerned others’ a) mental health, and b) quality of life over time combining 3, 6, and 12-month follow-ups after holding the other important patient and concerned other factors at baseline constant, increasing confidence that these factors might be causally-related to the concerned others’ mental health.
The patients and their concerned others were recruited as a part of a randomized controlled trial evaluating the efficacy of a 4-session intensive referral program to, Al-Anon , the 12-step mutual-help group for family and friends of individuals with alcohol and other drug use disorders. The initial study found no effect of the intervention on Al-anon attendance (28% in the Al-anon Intensive Referral, and 21% in the usual care condition). All analyses in this concerned other study controlled for intervention condition.
Concerned others were approximately 52 years of age on average and mostly female (77%), and white (66%). Most had completed at least 13 years of education (68%) and were employed (58%) and approximately half reported greater than $30,000 per year in income. Concerned other relationship types included current or former spouse (33%), parents (25%), siblings (13%) child (11%), friends (15%), and other relatives (3%). Almost two-thirds of the concerned others did not live with the patients (64%). Patients were primarily men (76%), white (69%), unmarried (75%) and unemployed (75%). Patients were 43 years of age on average and reported an average annual income of approximately $25,000.
WHAT DID THIS STUDY FIND?
Family and friends’ mental health improved over the course of the year
Concerned others’ mental health improved at each subsequent follow up relative to baseline, though only slightly so (see Figure below). Concerned others’ mental health was independently higher for those with greater social support and when patients’ current treatment episode was prompted through criminal justice involvement, controlling for all other variables that were correlated with mental health (e.g., relationship stressors) as well as the concerned others’ age and treatment condition. On the other hand, concerned others’ mental health was independently lower when the concerned other reported higher discrimination stigma and more avoidance coping.
Concerned other quality of life did not improve over the course of the year
Unlike mental health, concerned others’ quality of life did not improve significantly in general over the course of the year compared to baseline. Being married and having a higher income however, was associated with higher quality of life reported by the concerned other. Also, having higher levels of discrimination stigma (the concerned others’ own experienced stigma regarding their loved one’s alcohol use) was independently associated with lower quality of life.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that concerned other mental health improved significantly over the course of the first year after a loved one entered residential alcohol use disorder treatment. This improvement, however, was relatively modest – about an average of 2.3 to 2.5 on symptom frequency from 1 (very often) to 5 (never). Concerned others’ quality of life did not change over time. Some individuals in the study may have had larger increases in mental health and others decreases or no change – to produce this modest benefit. Thus, understanding what predicts better mental health was a critical question answered here. For example, more social support and less avoidance coping were associated with better mental health. Taken together, when concerned others face their love one’s alcohol use disorder “head on”, but with ample social support themselves, they may have the best chance of improved mental health.
Discrimination stigma, which measures the concerned others’ own experience of discrimination due to their loved one’s alcohol use (e.g., “People have insulted me because of my drinker’s alcohol use.”), was associated with worse mental health and quality of life, even after controlling for substance use severity of the patient. Stigma is associated with worse outcomes for the individual, and this study builds on these findings by suggesting that this stigma may also harm the individual who perpetuates the stigma. Future studies may consider targeted stigma in concerned others – for example, through communication skills training on how to talk with others about their loved one’s drinking or cognitive strategies to reduce potential self-blame.
There are a number of resources that have been developed to support family and friends of people who use substances. Perhaps the most widely known is Al-Anon, which supports concerned others through a 12-step lens. Other mutual-help groups for family and friends are becoming increasingly popular alternatives for those with loved ones who prefer a more secular approach to recovery, like SMART recovery. Just as AA groups have Al-Anon family parallels, so too do SMART groups have a parallel SMART Family and Friends designed to help facilitate social support and coping skills for concerned others. Also, Learn2Cope caters primarily to parents of young people with opioid and other substance use disorders. Importantly, however, given that all patients in this study received either usual care – psychoeducation for family members delivered by the patient’s treatment program – or an Al-Anon facilitation, and mental health gains were modest while quality of life did not change over time – additional help (e.g., individual therapy tailored specifically to concerned others) may be needed.
The study measures quality of life and mental health 4 times over a 1 year period. However, mental health may more broadly shift along smaller timescales, and future research may consider measuring factors weekly or daily to understand whether activities at that scale – e.g., on a given day – may boost adaptive coping and mental health.
Also, as study authors note, this residential alcohol use disorder treatment sample – which had low recovery capital and high clinical severity – may not generalize to individuals with lower severity or recruited from outpatient treatment.
BOTTOM LINE
If you are a concerned other struggling with your loved one’s alcohol use disorder, the first year following treatment may be associated with some modest improvements in mental health, but not always other broader areas of life quality, for close supports. Not avoiding, but rather facing a loved one’s substance use “head on”, while seeking social support to cope with the increased stress this may provoke, may help improve mental health over time. Further, identifying and addressing stigmatizing beliefs about a loved one’s alcohol use, in addition to finding healthy ways to cope with discrimination from others, may improve outcomes.
For individuals and families seeking recovery: Alcohol use disorder can be difficult for concerned others. If you have a loved one who is experiencing harms from alcohol use, you may also be impacted, and you are not alone. Not avoiding, but rather, facing a loved one’s substance use “head on”, while seeking social support to cope with the increased stress this may provoke, may help improve your mental health over time. There are resources, such as Al-Anon or SMART Family and Friends, to support a concerned other through their loved one’s substance use disorder, though some often benefit from their own individual therapy alone or in addition to participation in one of these community peer-led resources.
For treatment professionals and treatment systems: Some of your patients may be experiencing lower levels of mental health and quality of life in part due to concern for personal safety or the safety of a loved one who has alcohol and other drug use disorders. It is important to assess substance use for the individual but also whether the individual is experiencing any stress from a loved one’s substance use. While there are community resources available, such as Al-Anon and SMART Family and Friends, if seeing a patient like this in individual therapy, helping equip them with strategies to help their loved one and to seek out their own social support will likely yield important benefits.
For scientists: These findings provide the foundation for future research exploring individual differences, some of which may be addressed through intervention, that predict concerned other mental health and quality of life over the course of remission from alcohol use disorder. Future studies might consider targeting some of these factors through intervention. Qualitative studies that ask concerned others what they think they need, and what types of resources may be or have been, most useful, may be help facilitate more rapid development of resources.
For policy makers: Substance use impacts the individual, concerned others, and broader communities. Continued public health attention to, and, earmarking scientific funding for, concerned others can help address indirect harms that an individuals’ alcohol use disorder has on their friends and family. Strategies that warrant funding include, but are not limited to, those addressing concerned others’ own mental health and those which equip concerned others with skills to support their loved one’s treatment and recovery engagement.
The financial, health care, and criminal justice impacts of alcohol use disorder and other harmful alcohol use are borne by the individual with the disorder, as well as others in their family and community. More than half of US adults reported that a family member had experienced addiction to alcohol. Family or friends may experience direct harms from alcohol intoxication, which increases risk of physical or interpersonal conflict, such as harassment, physical aggression and violence, and driving-related injuries. Alcohol use can lead also to financial or legal strains, often absorbed by the family unit.
More generally, family and friends – sometimes referred to as “concerned significant others” or “concerned others” – may spend substantial time and energy worried or upset regarding their loved one using the substance, which can interfere with functioning and increase the likelihood of mental health challenges such as insomnia, depression or anxiety.
While not all experience significant harms, family and friends are at an increased risk of experiencing a range of harms and need their own support throughout not only when symptoms are at their worst, but also throughout treatment and into the early months and years of recovery.
Clearly, not all concerned others are impacted equally, with some particularly vulnerable to the mental health impacts of their loved one’s alcohol use disorder. Better understanding of the factors that might influence this vulnerability may help inform strategies that specifically target family and friends’ well-being.
This study examined characteristics of concerned others and of patients with alcohol use disorder that impact quality of life and mental health over the first year of a recovery attempt following treatment.
HOW WAS THIS STUDY CONDUCTED?
The current study recruited 279 pairs of patients enrolled in residential alcohol use disorder treatment and their concerned others to complete surveys 4 times over 1 year. Patients were asked to name potential concerned others that were at least 18 years old and supportive of the patient’s treatment attendance. There were no requirements about the type of relationship (partner, family member, friend, coworker). Patients and concerned others then completed surveys at baseline, and 3, 6, and 12-month follow-ups.
The researchers examined which patient and concerned other characteristics and behaviors predicted changes in concerned other mental health and quality of life over time. Patient characteristics and behaviors included substance use severity, treatment and Alcoholic Anonymous (AA) participation, relationship satisfaction and conflict (from the patient’s perspective), mental health, and criminal justice involvement. Concerned other characteristics included their age, gender, marital status, race, education, income, employment status, relationship to the patient, social support, past 30-day alcohol use status, perceived stigma toward patient’s alcohol use, type of communication to the patient about alcohol use (e.g., controlling and nurturing), and coping skills.
The researchers evaluated associations between all predictors and outcomes separately, and all that were significant were included in a larger model to determine whether each factor was an independent predictor of concerned others’ a) mental health, and b) quality of life over time combining 3, 6, and 12-month follow-ups after holding the other important patient and concerned other factors at baseline constant, increasing confidence that these factors might be causally-related to the concerned others’ mental health.
The patients and their concerned others were recruited as a part of a randomized controlled trial evaluating the efficacy of a 4-session intensive referral program to, Al-Anon , the 12-step mutual-help group for family and friends of individuals with alcohol and other drug use disorders. The initial study found no effect of the intervention on Al-anon attendance (28% in the Al-anon Intensive Referral, and 21% in the usual care condition). All analyses in this concerned other study controlled for intervention condition.
Concerned others were approximately 52 years of age on average and mostly female (77%), and white (66%). Most had completed at least 13 years of education (68%) and were employed (58%) and approximately half reported greater than $30,000 per year in income. Concerned other relationship types included current or former spouse (33%), parents (25%), siblings (13%) child (11%), friends (15%), and other relatives (3%). Almost two-thirds of the concerned others did not live with the patients (64%). Patients were primarily men (76%), white (69%), unmarried (75%) and unemployed (75%). Patients were 43 years of age on average and reported an average annual income of approximately $25,000.
WHAT DID THIS STUDY FIND?
Family and friends’ mental health improved over the course of the year
Concerned others’ mental health improved at each subsequent follow up relative to baseline, though only slightly so (see Figure below). Concerned others’ mental health was independently higher for those with greater social support and when patients’ current treatment episode was prompted through criminal justice involvement, controlling for all other variables that were correlated with mental health (e.g., relationship stressors) as well as the concerned others’ age and treatment condition. On the other hand, concerned others’ mental health was independently lower when the concerned other reported higher discrimination stigma and more avoidance coping.
Concerned other quality of life did not improve over the course of the year
Unlike mental health, concerned others’ quality of life did not improve significantly in general over the course of the year compared to baseline. Being married and having a higher income however, was associated with higher quality of life reported by the concerned other. Also, having higher levels of discrimination stigma (the concerned others’ own experienced stigma regarding their loved one’s alcohol use) was independently associated with lower quality of life.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that concerned other mental health improved significantly over the course of the first year after a loved one entered residential alcohol use disorder treatment. This improvement, however, was relatively modest – about an average of 2.3 to 2.5 on symptom frequency from 1 (very often) to 5 (never). Concerned others’ quality of life did not change over time. Some individuals in the study may have had larger increases in mental health and others decreases or no change – to produce this modest benefit. Thus, understanding what predicts better mental health was a critical question answered here. For example, more social support and less avoidance coping were associated with better mental health. Taken together, when concerned others face their love one’s alcohol use disorder “head on”, but with ample social support themselves, they may have the best chance of improved mental health.
Discrimination stigma, which measures the concerned others’ own experience of discrimination due to their loved one’s alcohol use (e.g., “People have insulted me because of my drinker’s alcohol use.”), was associated with worse mental health and quality of life, even after controlling for substance use severity of the patient. Stigma is associated with worse outcomes for the individual, and this study builds on these findings by suggesting that this stigma may also harm the individual who perpetuates the stigma. Future studies may consider targeted stigma in concerned others – for example, through communication skills training on how to talk with others about their loved one’s drinking or cognitive strategies to reduce potential self-blame.
There are a number of resources that have been developed to support family and friends of people who use substances. Perhaps the most widely known is Al-Anon, which supports concerned others through a 12-step lens. Other mutual-help groups for family and friends are becoming increasingly popular alternatives for those with loved ones who prefer a more secular approach to recovery, like SMART recovery. Just as AA groups have Al-Anon family parallels, so too do SMART groups have a parallel SMART Family and Friends designed to help facilitate social support and coping skills for concerned others. Also, Learn2Cope caters primarily to parents of young people with opioid and other substance use disorders. Importantly, however, given that all patients in this study received either usual care – psychoeducation for family members delivered by the patient’s treatment program – or an Al-Anon facilitation, and mental health gains were modest while quality of life did not change over time – additional help (e.g., individual therapy tailored specifically to concerned others) may be needed.
The study measures quality of life and mental health 4 times over a 1 year period. However, mental health may more broadly shift along smaller timescales, and future research may consider measuring factors weekly or daily to understand whether activities at that scale – e.g., on a given day – may boost adaptive coping and mental health.
Also, as study authors note, this residential alcohol use disorder treatment sample – which had low recovery capital and high clinical severity – may not generalize to individuals with lower severity or recruited from outpatient treatment.
BOTTOM LINE
If you are a concerned other struggling with your loved one’s alcohol use disorder, the first year following treatment may be associated with some modest improvements in mental health, but not always other broader areas of life quality, for close supports. Not avoiding, but rather facing a loved one’s substance use “head on”, while seeking social support to cope with the increased stress this may provoke, may help improve mental health over time. Further, identifying and addressing stigmatizing beliefs about a loved one’s alcohol use, in addition to finding healthy ways to cope with discrimination from others, may improve outcomes.
For individuals and families seeking recovery: Alcohol use disorder can be difficult for concerned others. If you have a loved one who is experiencing harms from alcohol use, you may also be impacted, and you are not alone. Not avoiding, but rather, facing a loved one’s substance use “head on”, while seeking social support to cope with the increased stress this may provoke, may help improve your mental health over time. There are resources, such as Al-Anon or SMART Family and Friends, to support a concerned other through their loved one’s substance use disorder, though some often benefit from their own individual therapy alone or in addition to participation in one of these community peer-led resources.
For treatment professionals and treatment systems: Some of your patients may be experiencing lower levels of mental health and quality of life in part due to concern for personal safety or the safety of a loved one who has alcohol and other drug use disorders. It is important to assess substance use for the individual but also whether the individual is experiencing any stress from a loved one’s substance use. While there are community resources available, such as Al-Anon and SMART Family and Friends, if seeing a patient like this in individual therapy, helping equip them with strategies to help their loved one and to seek out their own social support will likely yield important benefits.
For scientists: These findings provide the foundation for future research exploring individual differences, some of which may be addressed through intervention, that predict concerned other mental health and quality of life over the course of remission from alcohol use disorder. Future studies might consider targeting some of these factors through intervention. Qualitative studies that ask concerned others what they think they need, and what types of resources may be or have been, most useful, may be help facilitate more rapid development of resources.
For policy makers: Substance use impacts the individual, concerned others, and broader communities. Continued public health attention to, and, earmarking scientific funding for, concerned others can help address indirect harms that an individuals’ alcohol use disorder has on their friends and family. Strategies that warrant funding include, but are not limited to, those addressing concerned others’ own mental health and those which equip concerned others with skills to support their loved one’s treatment and recovery engagement.