Alcohol-related harms continue to be common and deadly in patients treated for other primary drug problems
Despite the many risks related to alcohol in addiction patients, treatment providers may overlook it if patients enter treatment with a different primary substance, like opioids or stimulants. This study examined how self-reported alcohol use at treatment entry among patients entering treatment for another drug use disorder predicted long-term health risks and mortality, highlighting the urgent need for more comprehensive alcohol screening and broader intervention.
Despite these risks, alcohol use may be overlooked in substance use disorder treatment when another drug, like opioids or stimulants, are a patient’s primary substance, leaving many individuals vulnerable to preventable health complications and premature death. In addition to this critical gap in care, there has been a lack of research on alcohol-related health risks in drug use disorder treatment populations, limiting the development of targeted interventions.
Addressing this gap is essential for improving screening, treatment, and harm reduction strategies, as well as clinical and public health recommendations. In this study, researchers assessed the relationship between self-reported alcohol use at admission and future alcohol-related health risks and mortality among a large group of Danish participants enrolled in residential substance use disorder treatment.
HOW WAS THIS STUDY CONDUCTED?
This longitudinal study analyzed data from the Danish Register of Individuals in Residential Substance Use Treatment, which tracked people undergoing residential treatment for substance use disorders in Denmark between 1998 and 2012. The final sample consisted of 4981 individuals. Study outcomes were disease or death fully attributable to alcohol, as classified by the International Classification of Diseases (ICD-10). These included alcohol use disorder, alcohol-related nerve damage, heart disease, liver disease, pancreatitis, alcohol poisoning, and alcohol-induced stomach inflammation.
At treatment intake, participants completed the European version of the Addiction Severity Index. Because the researchers were specifically concerned with whether self-reported alcohol consumption and difficulties in the 30 days before treatment predicted future alcohol-related hospitalizations and deaths, they narrowed their focus to a subcomponent of the Addiction Severity Index, the Alcohol Composite Score ranging from 0 (no alcohol use or problems) to 1 (severe alcohol use and problems). Participants were tracked from their date of treatment admission until either their death or the end of the study period on December 31, 2018, if they were still alive.
To understand how alcohol-related problems at the start of treatment were linked to the risk of dying from alcohol-related causes, researchers used a special statistical method that considers other possible causes of death. This approach ensured that if someone died from a non-alcohol-related cause, their death was accounted for because it meant they could no longer die from an alcohol-related condition. The analysis produced a risk estimate, showing how strongly a person’s level of alcohol-related difficulties at treatment entry was connected to their chance of dying from alcohol-related causes. Because many participants were hospitalized for alcohol-related conditions multiple times, researchers tracked all hospital visits over time, rather than just the first one. This approach provided a more complete picture of long-term health risks. If a participant died from any cause, their death was considered a final event, since it would prevent further hospitalizations.
To ensure accurate results, the analysis accounted for age, sex, employment status, and other key health and social factors, such as substance use, mental health, and legal issues. Researchers also investigated whether a person’s socioeconomic status influenced the link between alcohol use and health risks, specifically by examining whether being employed or unemployed changed the impact of alcohol-related difficulties on long-term health outcomes.
The final sample included 3810 men and 1171 women, with an average age of about 32 years at treatment enrollment. The majority (94%) were born in Denmark to Danish parents, and most were not living with a partner (81%) or children (87%). Only 14.2% were working or in school at the time of enrollment. In the 30 days before treatment, 43% reported drinking alcohol, and 9% engaged in daily heavy drinking, consuming five or more drinks per occasion. The most commonly used substances before treatment were cannabis, sedatives or hypnotics, and cocaine.
WHAT DID THIS STUDY FIND?
One in 20 died from alcohol-related deaths
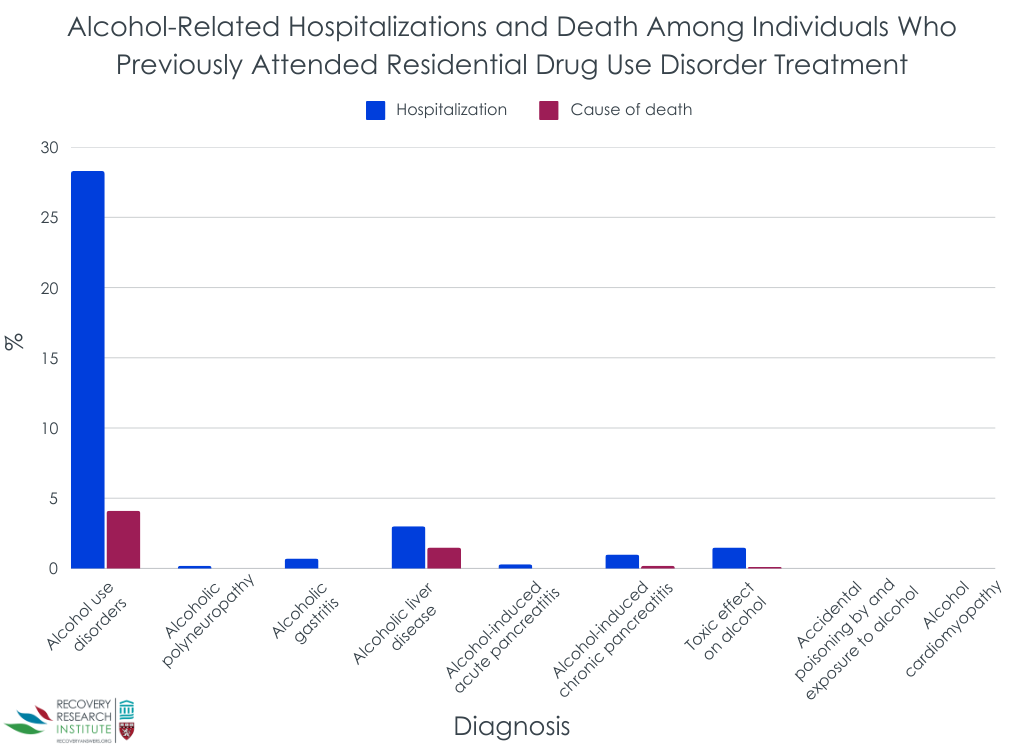
After entering treatment for another primary drug use disorder, 4% of participants died from alcohol use disorder, while 1.5% died from alcohol-related liver disease (see Figure below). Deaths from chronic pancreatitis (0.2%) and toxic effects of alcohol (0.1%) were much less frequent. Some conditions, such as accidental alcohol poisoning and alcohol-related heart disease, had too few cases to report.
One in 3 were hospitalized due to alcohol use
After entering treatment, 28% of participants were hospitalized at least once for alcohol use disorder (see Figure above), making it the most common alcohol-related hospital diagnosis. The second most frequent cause was alcohol-related liver disease, affecting 3% of participants. Other common alcohol-related hospitalizations included chronic pancreatitis (1%), toxic effects of alcohol (1.5%), gastritis (0.7%), acute pancreatitis (0.3%), and polyneuropathy (0.2%), though these conditions affected fewer individuals.
Higher alcohol composite scores at treatment admission significantly predicted risk of hospitalization and dying from alcohol-related causes
Individuals with higher alcohol composite scores at treatment admission had a substantially increased risk of alcohol-related death. Before adjusting for other factors, those with higher alcohol severity scores were 8.7 times more likely to die from alcohol-related causes compared to those with lower scores. Even after controlling for variables such as age, employment status, and other health conditions, the risk remained significantly elevated, with these individuals still being over 5 times more likely to die from alcohol-related causes. The analysis also revealed that older age further increased the risk, with each additional year raising the likelihood of alcohol-related death by 8%.
Similarly, those with higher alcohol composite scores at treatment admission were much more likely to be hospitalized for alcohol-related health issues. Even after considering other factors like age, employment, and overall health, those with higher alcohol-related difficulties were twice as likely to be hospitalized for alcohol-related conditions compared to those with lower severity scores. Other factors also played a role in hospitalization risk. Older individuals and those who were unemployed or not in school were more likely to be hospitalized for alcohol-related issues.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that individuals in treatment for a variety of different types of substance use disorder experience significantly higher rates of alcohol-related health problems and deaths compared to the general population and young people in Denmark. The researchers found that more alcohol use and problems upon admission to treatment for another primary drug problem substantially increased risk for alcohol-related deaths and hospitalizations up to 18 years later. The most common causes included alcohol use disorder and alcohol-related liver disease, with additional deaths from chronic pancreatitis and alcohol toxicity. These findings reinforce the well-established link between alcohol use and increased mortality risk. However, the fact that alcohol use disorder was the leading cause of alcohol-related deaths and hospitalizations highlights how this risk is further intensified by the co-occurrence of alcohol use and other drug use disorders.
The study found that individuals with higher alcohol composite scores at treatment admission faced a significantly greater risk of alcohol-related death, while those with more severe alcohol-related problems were far more likely to be hospitalized for alcohol-related health issues. As the research team notes, the study may even underestimate alcohol’s impact on health because 1) not everyone with alcohol-related issues seeks hospital care, 2) doctors may fail to diagnose alcohol-related conditions, and 3) hospital coding systems may not always accurately record diseases like liver cirrhosis. Interestingly, individuals with greater legal issues at treatment entry initially had a lower risk of alcohol-related death, though this protective effect weakened over time. Additionally, people with more severe drug use problems were less likely to be hospitalized for alcohol-related conditions, suggesting their substance use may have been more concentrated on this (non-alcohol) primary substance whereas those with lower severity drug use may have been using a mix of substances, including alcohol, making alcohol-related health consequences more likely.
These findings highlight an urgent need to better address alcohol use within drug use disorder treatment, as severe alcohol-related difficulties at admission strongly predict long-term health risks and mortality. Notably, the results also underscore the value of the Addiction Severity Index as a screening tool, which could help identify high-risk individuals early, enhance treatment strategies, and ultimately reduce alcohol-related harm in this population. The study reveals that many people in substance use disorder treatment also struggle with severe alcohol problems, but it does not determine whether substance use treatment programs are failing to address alcohol use. They may have been, but if they were, perhaps more assertive or different types of additional interventions are needed to offset long-term harms from alcohol in treated drug-addicted populations. Future research should examine how often these individuals are referred for alcohol treatment and whether such referrals help reduce long-term health risks.
The Addiction Severity Index was collected by clinicians for clinical use rather than research. Due to missing data, 28% of participants were excluded from the study, though it is unclear whether these individuals were systematically difference from those who were included.
As the research team notes, the study may underestimate alcohol’s impact on health because not everyone with alcohol-related issues seeks hospital care, doctors may fail to diagnose alcohol-related conditions, and hospital coding systems may not always accurately record diseases like liver cirrhosis.
The study’s long follow-up period is a strength, but it did not include individuals who started treatment more recently, so the findings may not fully reflect the experiences of people entering treatment today.
BOTTOM LINE
Individuals in treatment for drug use disorder face much higher rates of alcohol-related health issues and deaths compared to the general population. While past research shows that many people with a primary drug use disorder may drink in harmful and hazardous ways, this study confirms that they also suffer and die from from severe alcohol-related diseases, such as liver disease and pancreatitis, directly caused by alcohol use.
For individuals and families seeking recovery: These findings highlight an urgent need for integrated treatment that better addresses alcohol use for those with a primary drug use disorder, as individuals in substance use recovery face significantly higher risks of alcohol-related health issues and deaths. Many may not realize that even moderate drinking can lead to serious conditions like liver disease and pancreatitis, making early screening and intervention essential. Others may substitute alcohol for their primary drug leading to more alcohol-related harms over time. Families should advocate for comprehensive care that includes long-term health monitoring to prevent these risks. The study also underscores the danger of substituting alcohol for other substances, emphasizing the need for education on comorbidities and healthier coping strategies.
For treatment professionals and treatment systems: These findings underscore the urgent need for improved screening and better integrated treatment to address alcohol use within substance use disorder programs and reduce long-term health risks. Treatment programs that ensure that alcohol use is treated alongside other drug problems may help reduce the disease burden from excessive alcohol use. By acknowledging these risks, treatment providers and systems can collaborate to create more effective recovery plans that support long-term health and prevent avoidable harm.
For scientists: Future research should examine whether individuals with hazardous alcohol use in treatment for a primary drug problem are receiving integrated alcohol-drug treatment (as is typical in many programs in the US) or being systematically linked with alcohol-specific services, and whether these referrals lead to measurable reductions in long-term health risks. Researchers should focus on developing and evaluating tailored alcohol treatment approaches that consider the unique challenges of individuals with co-occurring alcohol and other drug use disorders, ensuring interventions are both clinically effective and feasible in real-world treatment settings.
For policy makers: Policymakers should integrate alcohol screening, assessment, and intervention into all drug use disorder treatment programs to address the high rates of alcohol-related illness and death in this population. Funding may support comprehensive recovery programs with long-term medical monitoring and harm reduction strategies to address the harms of alcohol use. Additionally, public health initiatives should educate providers on the risks of alcohol substitution and/or co-use in drug use disorder recovery. Strengthening coordination between addiction treatment, mental health, and primary care through evidence-based policies can improve outcomes and reduce healthcare burdens.
Despite these risks, alcohol use may be overlooked in substance use disorder treatment when another drug, like opioids or stimulants, are a patient’s primary substance, leaving many individuals vulnerable to preventable health complications and premature death. In addition to this critical gap in care, there has been a lack of research on alcohol-related health risks in drug use disorder treatment populations, limiting the development of targeted interventions.
Addressing this gap is essential for improving screening, treatment, and harm reduction strategies, as well as clinical and public health recommendations. In this study, researchers assessed the relationship between self-reported alcohol use at admission and future alcohol-related health risks and mortality among a large group of Danish participants enrolled in residential substance use disorder treatment.
HOW WAS THIS STUDY CONDUCTED?
This longitudinal study analyzed data from the Danish Register of Individuals in Residential Substance Use Treatment, which tracked people undergoing residential treatment for substance use disorders in Denmark between 1998 and 2012. The final sample consisted of 4981 individuals. Study outcomes were disease or death fully attributable to alcohol, as classified by the International Classification of Diseases (ICD-10). These included alcohol use disorder, alcohol-related nerve damage, heart disease, liver disease, pancreatitis, alcohol poisoning, and alcohol-induced stomach inflammation.
At treatment intake, participants completed the European version of the Addiction Severity Index. Because the researchers were specifically concerned with whether self-reported alcohol consumption and difficulties in the 30 days before treatment predicted future alcohol-related hospitalizations and deaths, they narrowed their focus to a subcomponent of the Addiction Severity Index, the Alcohol Composite Score ranging from 0 (no alcohol use or problems) to 1 (severe alcohol use and problems). Participants were tracked from their date of treatment admission until either their death or the end of the study period on December 31, 2018, if they were still alive.
To understand how alcohol-related problems at the start of treatment were linked to the risk of dying from alcohol-related causes, researchers used a special statistical method that considers other possible causes of death. This approach ensured that if someone died from a non-alcohol-related cause, their death was accounted for because it meant they could no longer die from an alcohol-related condition. The analysis produced a risk estimate, showing how strongly a person’s level of alcohol-related difficulties at treatment entry was connected to their chance of dying from alcohol-related causes. Because many participants were hospitalized for alcohol-related conditions multiple times, researchers tracked all hospital visits over time, rather than just the first one. This approach provided a more complete picture of long-term health risks. If a participant died from any cause, their death was considered a final event, since it would prevent further hospitalizations.
To ensure accurate results, the analysis accounted for age, sex, employment status, and other key health and social factors, such as substance use, mental health, and legal issues. Researchers also investigated whether a person’s socioeconomic status influenced the link between alcohol use and health risks, specifically by examining whether being employed or unemployed changed the impact of alcohol-related difficulties on long-term health outcomes.
The final sample included 3810 men and 1171 women, with an average age of about 32 years at treatment enrollment. The majority (94%) were born in Denmark to Danish parents, and most were not living with a partner (81%) or children (87%). Only 14.2% were working or in school at the time of enrollment. In the 30 days before treatment, 43% reported drinking alcohol, and 9% engaged in daily heavy drinking, consuming five or more drinks per occasion. The most commonly used substances before treatment were cannabis, sedatives or hypnotics, and cocaine.
WHAT DID THIS STUDY FIND?
One in 20 died from alcohol-related deaths
After entering treatment for another primary drug use disorder, 4% of participants died from alcohol use disorder, while 1.5% died from alcohol-related liver disease (see Figure below). Deaths from chronic pancreatitis (0.2%) and toxic effects of alcohol (0.1%) were much less frequent. Some conditions, such as accidental alcohol poisoning and alcohol-related heart disease, had too few cases to report.
One in 3 were hospitalized due to alcohol use
After entering treatment, 28% of participants were hospitalized at least once for alcohol use disorder (see Figure above), making it the most common alcohol-related hospital diagnosis. The second most frequent cause was alcohol-related liver disease, affecting 3% of participants. Other common alcohol-related hospitalizations included chronic pancreatitis (1%), toxic effects of alcohol (1.5%), gastritis (0.7%), acute pancreatitis (0.3%), and polyneuropathy (0.2%), though these conditions affected fewer individuals.
Higher alcohol composite scores at treatment admission significantly predicted risk of hospitalization and dying from alcohol-related causes
Individuals with higher alcohol composite scores at treatment admission had a substantially increased risk of alcohol-related death. Before adjusting for other factors, those with higher alcohol severity scores were 8.7 times more likely to die from alcohol-related causes compared to those with lower scores. Even after controlling for variables such as age, employment status, and other health conditions, the risk remained significantly elevated, with these individuals still being over 5 times more likely to die from alcohol-related causes. The analysis also revealed that older age further increased the risk, with each additional year raising the likelihood of alcohol-related death by 8%.
Similarly, those with higher alcohol composite scores at treatment admission were much more likely to be hospitalized for alcohol-related health issues. Even after considering other factors like age, employment, and overall health, those with higher alcohol-related difficulties were twice as likely to be hospitalized for alcohol-related conditions compared to those with lower severity scores. Other factors also played a role in hospitalization risk. Older individuals and those who were unemployed or not in school were more likely to be hospitalized for alcohol-related issues.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that individuals in treatment for a variety of different types of substance use disorder experience significantly higher rates of alcohol-related health problems and deaths compared to the general population and young people in Denmark. The researchers found that more alcohol use and problems upon admission to treatment for another primary drug problem substantially increased risk for alcohol-related deaths and hospitalizations up to 18 years later. The most common causes included alcohol use disorder and alcohol-related liver disease, with additional deaths from chronic pancreatitis and alcohol toxicity. These findings reinforce the well-established link between alcohol use and increased mortality risk. However, the fact that alcohol use disorder was the leading cause of alcohol-related deaths and hospitalizations highlights how this risk is further intensified by the co-occurrence of alcohol use and other drug use disorders.
The study found that individuals with higher alcohol composite scores at treatment admission faced a significantly greater risk of alcohol-related death, while those with more severe alcohol-related problems were far more likely to be hospitalized for alcohol-related health issues. As the research team notes, the study may even underestimate alcohol’s impact on health because 1) not everyone with alcohol-related issues seeks hospital care, 2) doctors may fail to diagnose alcohol-related conditions, and 3) hospital coding systems may not always accurately record diseases like liver cirrhosis. Interestingly, individuals with greater legal issues at treatment entry initially had a lower risk of alcohol-related death, though this protective effect weakened over time. Additionally, people with more severe drug use problems were less likely to be hospitalized for alcohol-related conditions, suggesting their substance use may have been more concentrated on this (non-alcohol) primary substance whereas those with lower severity drug use may have been using a mix of substances, including alcohol, making alcohol-related health consequences more likely.
These findings highlight an urgent need to better address alcohol use within drug use disorder treatment, as severe alcohol-related difficulties at admission strongly predict long-term health risks and mortality. Notably, the results also underscore the value of the Addiction Severity Index as a screening tool, which could help identify high-risk individuals early, enhance treatment strategies, and ultimately reduce alcohol-related harm in this population. The study reveals that many people in substance use disorder treatment also struggle with severe alcohol problems, but it does not determine whether substance use treatment programs are failing to address alcohol use. They may have been, but if they were, perhaps more assertive or different types of additional interventions are needed to offset long-term harms from alcohol in treated drug-addicted populations. Future research should examine how often these individuals are referred for alcohol treatment and whether such referrals help reduce long-term health risks.
The Addiction Severity Index was collected by clinicians for clinical use rather than research. Due to missing data, 28% of participants were excluded from the study, though it is unclear whether these individuals were systematically difference from those who were included.
As the research team notes, the study may underestimate alcohol’s impact on health because not everyone with alcohol-related issues seeks hospital care, doctors may fail to diagnose alcohol-related conditions, and hospital coding systems may not always accurately record diseases like liver cirrhosis.
The study’s long follow-up period is a strength, but it did not include individuals who started treatment more recently, so the findings may not fully reflect the experiences of people entering treatment today.
BOTTOM LINE
Individuals in treatment for drug use disorder face much higher rates of alcohol-related health issues and deaths compared to the general population. While past research shows that many people with a primary drug use disorder may drink in harmful and hazardous ways, this study confirms that they also suffer and die from from severe alcohol-related diseases, such as liver disease and pancreatitis, directly caused by alcohol use.
For individuals and families seeking recovery: These findings highlight an urgent need for integrated treatment that better addresses alcohol use for those with a primary drug use disorder, as individuals in substance use recovery face significantly higher risks of alcohol-related health issues and deaths. Many may not realize that even moderate drinking can lead to serious conditions like liver disease and pancreatitis, making early screening and intervention essential. Others may substitute alcohol for their primary drug leading to more alcohol-related harms over time. Families should advocate for comprehensive care that includes long-term health monitoring to prevent these risks. The study also underscores the danger of substituting alcohol for other substances, emphasizing the need for education on comorbidities and healthier coping strategies.
For treatment professionals and treatment systems: These findings underscore the urgent need for improved screening and better integrated treatment to address alcohol use within substance use disorder programs and reduce long-term health risks. Treatment programs that ensure that alcohol use is treated alongside other drug problems may help reduce the disease burden from excessive alcohol use. By acknowledging these risks, treatment providers and systems can collaborate to create more effective recovery plans that support long-term health and prevent avoidable harm.
For scientists: Future research should examine whether individuals with hazardous alcohol use in treatment for a primary drug problem are receiving integrated alcohol-drug treatment (as is typical in many programs in the US) or being systematically linked with alcohol-specific services, and whether these referrals lead to measurable reductions in long-term health risks. Researchers should focus on developing and evaluating tailored alcohol treatment approaches that consider the unique challenges of individuals with co-occurring alcohol and other drug use disorders, ensuring interventions are both clinically effective and feasible in real-world treatment settings.
For policy makers: Policymakers should integrate alcohol screening, assessment, and intervention into all drug use disorder treatment programs to address the high rates of alcohol-related illness and death in this population. Funding may support comprehensive recovery programs with long-term medical monitoring and harm reduction strategies to address the harms of alcohol use. Additionally, public health initiatives should educate providers on the risks of alcohol substitution and/or co-use in drug use disorder recovery. Strengthening coordination between addiction treatment, mental health, and primary care through evidence-based policies can improve outcomes and reduce healthcare burdens.
Despite these risks, alcohol use may be overlooked in substance use disorder treatment when another drug, like opioids or stimulants, are a patient’s primary substance, leaving many individuals vulnerable to preventable health complications and premature death. In addition to this critical gap in care, there has been a lack of research on alcohol-related health risks in drug use disorder treatment populations, limiting the development of targeted interventions.
Addressing this gap is essential for improving screening, treatment, and harm reduction strategies, as well as clinical and public health recommendations. In this study, researchers assessed the relationship between self-reported alcohol use at admission and future alcohol-related health risks and mortality among a large group of Danish participants enrolled in residential substance use disorder treatment.
HOW WAS THIS STUDY CONDUCTED?
This longitudinal study analyzed data from the Danish Register of Individuals in Residential Substance Use Treatment, which tracked people undergoing residential treatment for substance use disorders in Denmark between 1998 and 2012. The final sample consisted of 4981 individuals. Study outcomes were disease or death fully attributable to alcohol, as classified by the International Classification of Diseases (ICD-10). These included alcohol use disorder, alcohol-related nerve damage, heart disease, liver disease, pancreatitis, alcohol poisoning, and alcohol-induced stomach inflammation.
At treatment intake, participants completed the European version of the Addiction Severity Index. Because the researchers were specifically concerned with whether self-reported alcohol consumption and difficulties in the 30 days before treatment predicted future alcohol-related hospitalizations and deaths, they narrowed their focus to a subcomponent of the Addiction Severity Index, the Alcohol Composite Score ranging from 0 (no alcohol use or problems) to 1 (severe alcohol use and problems). Participants were tracked from their date of treatment admission until either their death or the end of the study period on December 31, 2018, if they were still alive.
To understand how alcohol-related problems at the start of treatment were linked to the risk of dying from alcohol-related causes, researchers used a special statistical method that considers other possible causes of death. This approach ensured that if someone died from a non-alcohol-related cause, their death was accounted for because it meant they could no longer die from an alcohol-related condition. The analysis produced a risk estimate, showing how strongly a person’s level of alcohol-related difficulties at treatment entry was connected to their chance of dying from alcohol-related causes. Because many participants were hospitalized for alcohol-related conditions multiple times, researchers tracked all hospital visits over time, rather than just the first one. This approach provided a more complete picture of long-term health risks. If a participant died from any cause, their death was considered a final event, since it would prevent further hospitalizations.
To ensure accurate results, the analysis accounted for age, sex, employment status, and other key health and social factors, such as substance use, mental health, and legal issues. Researchers also investigated whether a person’s socioeconomic status influenced the link between alcohol use and health risks, specifically by examining whether being employed or unemployed changed the impact of alcohol-related difficulties on long-term health outcomes.
The final sample included 3810 men and 1171 women, with an average age of about 32 years at treatment enrollment. The majority (94%) were born in Denmark to Danish parents, and most were not living with a partner (81%) or children (87%). Only 14.2% were working or in school at the time of enrollment. In the 30 days before treatment, 43% reported drinking alcohol, and 9% engaged in daily heavy drinking, consuming five or more drinks per occasion. The most commonly used substances before treatment were cannabis, sedatives or hypnotics, and cocaine.
WHAT DID THIS STUDY FIND?
One in 20 died from alcohol-related deaths
After entering treatment for another primary drug use disorder, 4% of participants died from alcohol use disorder, while 1.5% died from alcohol-related liver disease (see Figure below). Deaths from chronic pancreatitis (0.2%) and toxic effects of alcohol (0.1%) were much less frequent. Some conditions, such as accidental alcohol poisoning and alcohol-related heart disease, had too few cases to report.
One in 3 were hospitalized due to alcohol use
After entering treatment, 28% of participants were hospitalized at least once for alcohol use disorder (see Figure above), making it the most common alcohol-related hospital diagnosis. The second most frequent cause was alcohol-related liver disease, affecting 3% of participants. Other common alcohol-related hospitalizations included chronic pancreatitis (1%), toxic effects of alcohol (1.5%), gastritis (0.7%), acute pancreatitis (0.3%), and polyneuropathy (0.2%), though these conditions affected fewer individuals.
Higher alcohol composite scores at treatment admission significantly predicted risk of hospitalization and dying from alcohol-related causes
Individuals with higher alcohol composite scores at treatment admission had a substantially increased risk of alcohol-related death. Before adjusting for other factors, those with higher alcohol severity scores were 8.7 times more likely to die from alcohol-related causes compared to those with lower scores. Even after controlling for variables such as age, employment status, and other health conditions, the risk remained significantly elevated, with these individuals still being over 5 times more likely to die from alcohol-related causes. The analysis also revealed that older age further increased the risk, with each additional year raising the likelihood of alcohol-related death by 8%.
Similarly, those with higher alcohol composite scores at treatment admission were much more likely to be hospitalized for alcohol-related health issues. Even after considering other factors like age, employment, and overall health, those with higher alcohol-related difficulties were twice as likely to be hospitalized for alcohol-related conditions compared to those with lower severity scores. Other factors also played a role in hospitalization risk. Older individuals and those who were unemployed or not in school were more likely to be hospitalized for alcohol-related issues.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that individuals in treatment for a variety of different types of substance use disorder experience significantly higher rates of alcohol-related health problems and deaths compared to the general population and young people in Denmark. The researchers found that more alcohol use and problems upon admission to treatment for another primary drug problem substantially increased risk for alcohol-related deaths and hospitalizations up to 18 years later. The most common causes included alcohol use disorder and alcohol-related liver disease, with additional deaths from chronic pancreatitis and alcohol toxicity. These findings reinforce the well-established link between alcohol use and increased mortality risk. However, the fact that alcohol use disorder was the leading cause of alcohol-related deaths and hospitalizations highlights how this risk is further intensified by the co-occurrence of alcohol use and other drug use disorders.
The study found that individuals with higher alcohol composite scores at treatment admission faced a significantly greater risk of alcohol-related death, while those with more severe alcohol-related problems were far more likely to be hospitalized for alcohol-related health issues. As the research team notes, the study may even underestimate alcohol’s impact on health because 1) not everyone with alcohol-related issues seeks hospital care, 2) doctors may fail to diagnose alcohol-related conditions, and 3) hospital coding systems may not always accurately record diseases like liver cirrhosis. Interestingly, individuals with greater legal issues at treatment entry initially had a lower risk of alcohol-related death, though this protective effect weakened over time. Additionally, people with more severe drug use problems were less likely to be hospitalized for alcohol-related conditions, suggesting their substance use may have been more concentrated on this (non-alcohol) primary substance whereas those with lower severity drug use may have been using a mix of substances, including alcohol, making alcohol-related health consequences more likely.
These findings highlight an urgent need to better address alcohol use within drug use disorder treatment, as severe alcohol-related difficulties at admission strongly predict long-term health risks and mortality. Notably, the results also underscore the value of the Addiction Severity Index as a screening tool, which could help identify high-risk individuals early, enhance treatment strategies, and ultimately reduce alcohol-related harm in this population. The study reveals that many people in substance use disorder treatment also struggle with severe alcohol problems, but it does not determine whether substance use treatment programs are failing to address alcohol use. They may have been, but if they were, perhaps more assertive or different types of additional interventions are needed to offset long-term harms from alcohol in treated drug-addicted populations. Future research should examine how often these individuals are referred for alcohol treatment and whether such referrals help reduce long-term health risks.
The Addiction Severity Index was collected by clinicians for clinical use rather than research. Due to missing data, 28% of participants were excluded from the study, though it is unclear whether these individuals were systematically difference from those who were included.
As the research team notes, the study may underestimate alcohol’s impact on health because not everyone with alcohol-related issues seeks hospital care, doctors may fail to diagnose alcohol-related conditions, and hospital coding systems may not always accurately record diseases like liver cirrhosis.
The study’s long follow-up period is a strength, but it did not include individuals who started treatment more recently, so the findings may not fully reflect the experiences of people entering treatment today.
BOTTOM LINE
Individuals in treatment for drug use disorder face much higher rates of alcohol-related health issues and deaths compared to the general population. While past research shows that many people with a primary drug use disorder may drink in harmful and hazardous ways, this study confirms that they also suffer and die from from severe alcohol-related diseases, such as liver disease and pancreatitis, directly caused by alcohol use.
For individuals and families seeking recovery: These findings highlight an urgent need for integrated treatment that better addresses alcohol use for those with a primary drug use disorder, as individuals in substance use recovery face significantly higher risks of alcohol-related health issues and deaths. Many may not realize that even moderate drinking can lead to serious conditions like liver disease and pancreatitis, making early screening and intervention essential. Others may substitute alcohol for their primary drug leading to more alcohol-related harms over time. Families should advocate for comprehensive care that includes long-term health monitoring to prevent these risks. The study also underscores the danger of substituting alcohol for other substances, emphasizing the need for education on comorbidities and healthier coping strategies.
For treatment professionals and treatment systems: These findings underscore the urgent need for improved screening and better integrated treatment to address alcohol use within substance use disorder programs and reduce long-term health risks. Treatment programs that ensure that alcohol use is treated alongside other drug problems may help reduce the disease burden from excessive alcohol use. By acknowledging these risks, treatment providers and systems can collaborate to create more effective recovery plans that support long-term health and prevent avoidable harm.
For scientists: Future research should examine whether individuals with hazardous alcohol use in treatment for a primary drug problem are receiving integrated alcohol-drug treatment (as is typical in many programs in the US) or being systematically linked with alcohol-specific services, and whether these referrals lead to measurable reductions in long-term health risks. Researchers should focus on developing and evaluating tailored alcohol treatment approaches that consider the unique challenges of individuals with co-occurring alcohol and other drug use disorders, ensuring interventions are both clinically effective and feasible in real-world treatment settings.
For policy makers: Policymakers should integrate alcohol screening, assessment, and intervention into all drug use disorder treatment programs to address the high rates of alcohol-related illness and death in this population. Funding may support comprehensive recovery programs with long-term medical monitoring and harm reduction strategies to address the harms of alcohol use. Additionally, public health initiatives should educate providers on the risks of alcohol substitution and/or co-use in drug use disorder recovery. Strengthening coordination between addiction treatment, mental health, and primary care through evidence-based policies can improve outcomes and reduce healthcare burdens.