Are some substance use disorders associated with more recovery barriers than others?
Sociodemographic and economic characteristics mark potential barriers to recovery, and can help inform the development of treatment plans, healthcare system models, and policies. This study used Norwegian public health data to identify some of these factors that help uncover disadvantages for people with substance use disorder.
Demographic, social, and economic factors associated with substance use disorders are important for developing individualized treatment plans and offering services that meet the needs of specific sub-populations. Characterizing sociodemographic factors in drug-specific populations can also inform new policies to help address inequalities in healthcare systems that hinder recovery among individuals with certain substance use disorders and sociodemographic backgrounds.
Though previous studies have evaluated the sociodemographics associated with substance use disorders in treatment settings or in the broader population, there are several limitations to this research. Data that concern the entire population are often restricted to the evaluation of the most prevalent types of substance use disorders (e.g., alcohol, cannabis), which limit important comparisons between less prevalent drug use disorders with significant societal impact (e.g., opioids, sedatives). Moreover, few largescale (e.g., national) investigations of treatment-seeking populations have compared sociodemographic factors across multiple different drug classes, restricting our ability to make drug-specific conclusions and recommendations.
Additional large-scale population level research looking at the sociodemographic and economic characteristics associated with specific substance use disorders among individuals in addiction treatment is needed to further inform our understanding of addiction and enhance individualized treatment approaches. International research is also needed to speak to cultural (e.g., drug trends) and healthcare differences (e.g., publicly vs. privately funded addiction healthcare systems) that might influence different findings in different countries. In this study, the researchers used national Norwegian public health data to evaluate sociodemographic differences between individuals receiving publicly funded substance use disorder treatment and the general population, and between individuals with different types of substance use disorders.
HOW WAS THIS STUDY CONDUCTED?
The research team conducted a national retrospective case-control study of 31,245 individuals with substance use disorders who were enrolled in treatment in Norway, and 31,275 individuals from the general population in Norway (i.e., control group).
Two primary datasets were used to extract sociodemographic data, including the Norwegian Patient Registry and the Norwegian National Population Register. The Norwegian Patient Registry, consisting of the entire population of patients in Norway’s public specialized healthcare system, was used to extract a sample of individuals with a primary diagnosis of substance use disorder who were admitted to specialized substance use disorder treatment or a psychiatric hospital between 2009 and 2010. The Norwegian National Population Register was used to obtain a random sample of age and gender matched individuals from the general population who were surveyed in 2010.
Substance use disorders assessed in this study included a primary diagnosis of: 1) alcohol use disorder (40%), 2) opioid use disorder (19%), 3) cannabis use disorder (11%), 4) sedative/hypnotic use disorder (5%; e.g., benzodiazepines), 5) cocaine use disorder (1%), 6) other stimulants (7%; e.g., amphetamines), and 7) other substance use disorders or several substance use disorders (17%), which may have included alcohol and/or sedatives/hypnotics. These disorders were also grouped into licit and illicit substance use disorders. Licit substance use disorder (45%) included alcohol use disorder and sedative/hypnotic use disorder. Illicit substance use disorder (55%) included all other categories.
Sociodemographic variables of interest included:
Low education level (i.e., % who did not complete mandatory education of at least ~7-10 years)
Employed (i.e., % of those aged 18 – 66 years receiving income from work or business)
Average annual income (in Norwegian Krone currency)
Average annual wealth (i.e., capital income, bank deposits, equity, bond and money market funds, shares, & assets; in Norwegian Krone currency)
Receiving financial assistance (i.e., % receiving temporary government benefits to cover basic needs)
Receiving a disability pension (i.e., % aged 18 – 66 receiving permanent government benefits for permanently reduced work capacity (≥ 50%) due to illness/injury, including substance use disorder)
Living alone (% living alone)
Living with young children (i.e., % living with a child under six years of age)
Urban dwelling (i.e., % living in cities with > 50,000 residents)
Sociodemographic factors (percentages and averages) were compared between patient vs. control populations and between patients with illicit vs. licit substance use disorders. Means and percentages among specific substance groups were also compared by examining differences between patients with different types of substance use disorder.
WHAT DID THIS STUDY FIND?
Individuals with substance use disorders were more disadvantaged in all sociodemographic and economic categories.
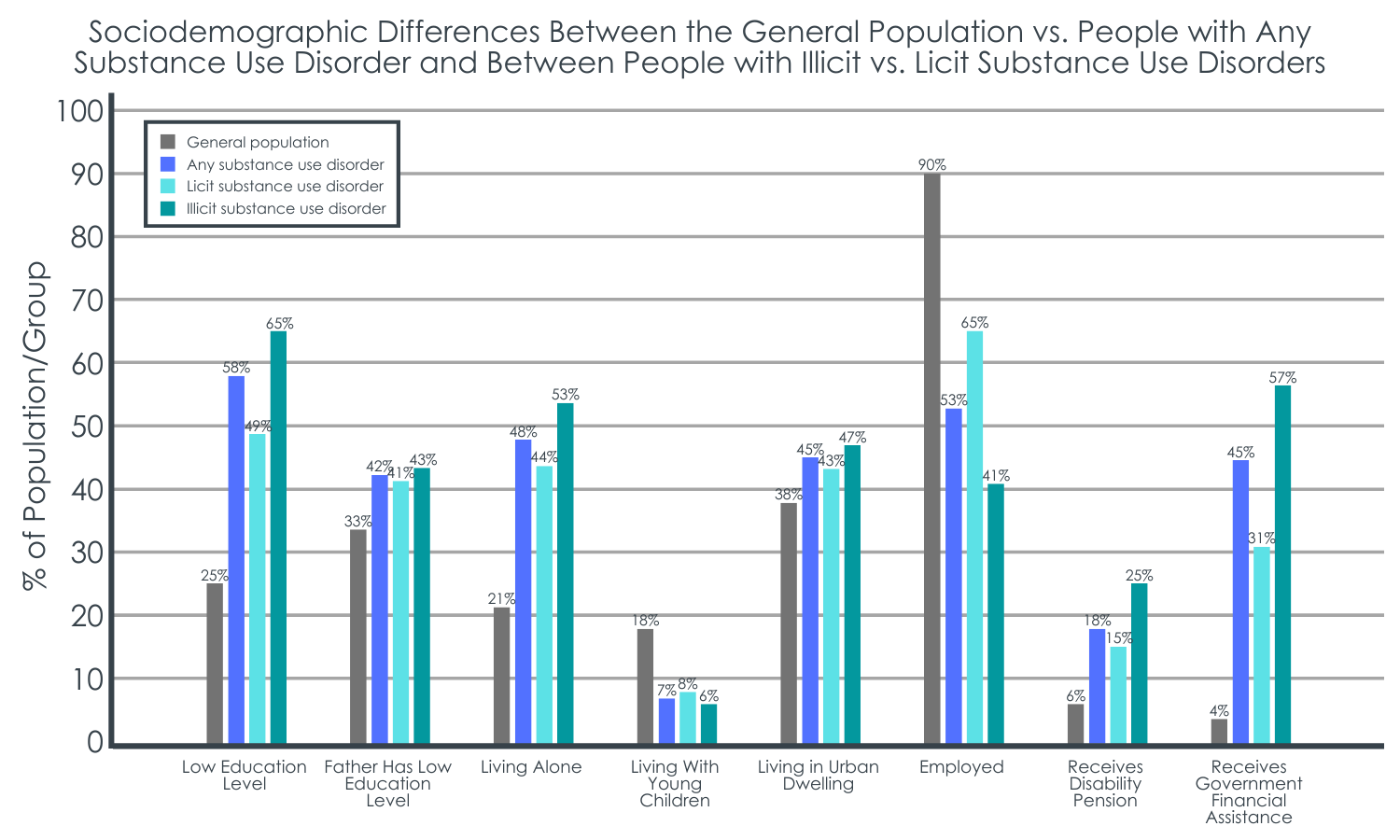
Compared to the general population, individuals admitted to substance use disorder treatment were more likely to have a low level of education, to have a father with a low level of education, to live alone in an urban dwelling, and to receive disability pensions and government financial assistance.
The general population had a greater percentage of people who lived with young children and were employed, with a higher average annual income and higher annual wealth.
Individuals with an illicit substance use disorder were more disadvantaged in all sociodemographic and economic categories.
Compared to individuals with licit substance use disorders and controlling for age and gender, those with illicit substance use disorders were more likely to have a low level of education, to have a father with a low level of education, to live alone in an urban dwelling, and to receive disability pensions and government financial assistance.
A greater percentage of people with a licit substance use disorder lived with young children and were employed, with a higher average annual income and higher average annual wealth.
Figure 1. This figure shows sociodemographic differences between the general Norwegian population and individuals in Norway who were admitted to treatment for a substance use disorder, as well as differences between those with a primary diagnosis of a licit versus illicit substance use disorder. Those with any substance use disorder had disadvantaged sociodemographic and economic characteristics across all categories, relative to the general population. Compared to individuals with licit substance use disorders, those with illicit disorders had disadvantaged sociodemographic and economic characteristics across all categories. In this study, licit substance use disorders included 1) alcohol use disorder and 2) sedative/hypnotic use disorder, whereas illicit substance use disorders included 1) opioid use disorder, 2) cannabis use disorder, 3) cocaine use disorder, 4) other stimulant use disorders, and 5) ‘other substance use disorders or multiple primary substance use disorders.
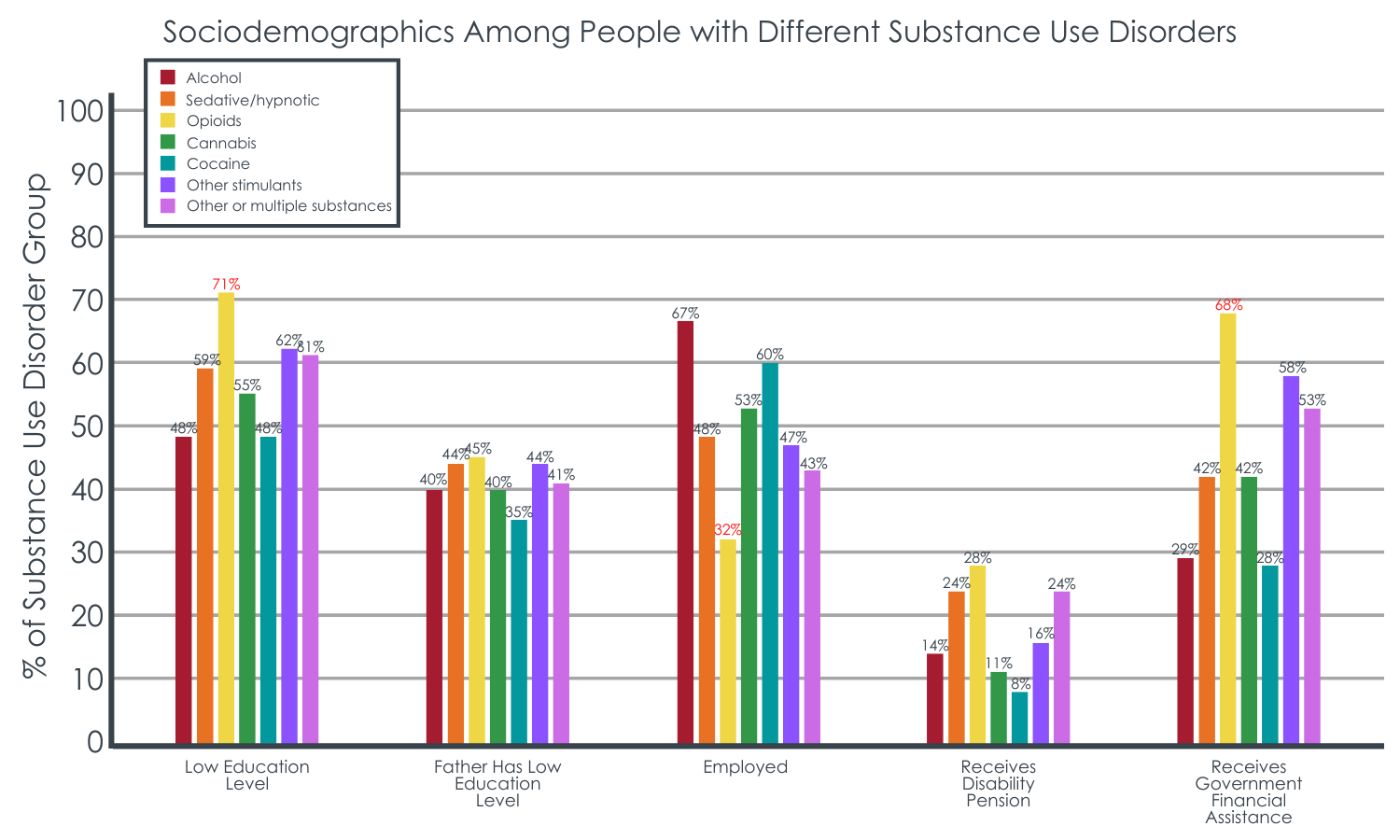
The opioid group was particularly disadvantaged.
Individuals with opioid use disorder had the highest percentage of individuals with low educational achievement, who were living alone, receiving government financial assistance and disability pensions. They also had the lowest likelihood of being employed, the lowest average annual income, and the lowest average annual wealth.
Individuals with alcohol use disorder and those with cocaine use disorder were most likely to be employed, had the highest average annual income, and were the least likely to have low educational attainment, to receive disability pensions and government financial assistance. In addition, individuals with cocaine use disorder less commonly lived alone and were most likely to live in an urban dwelling.
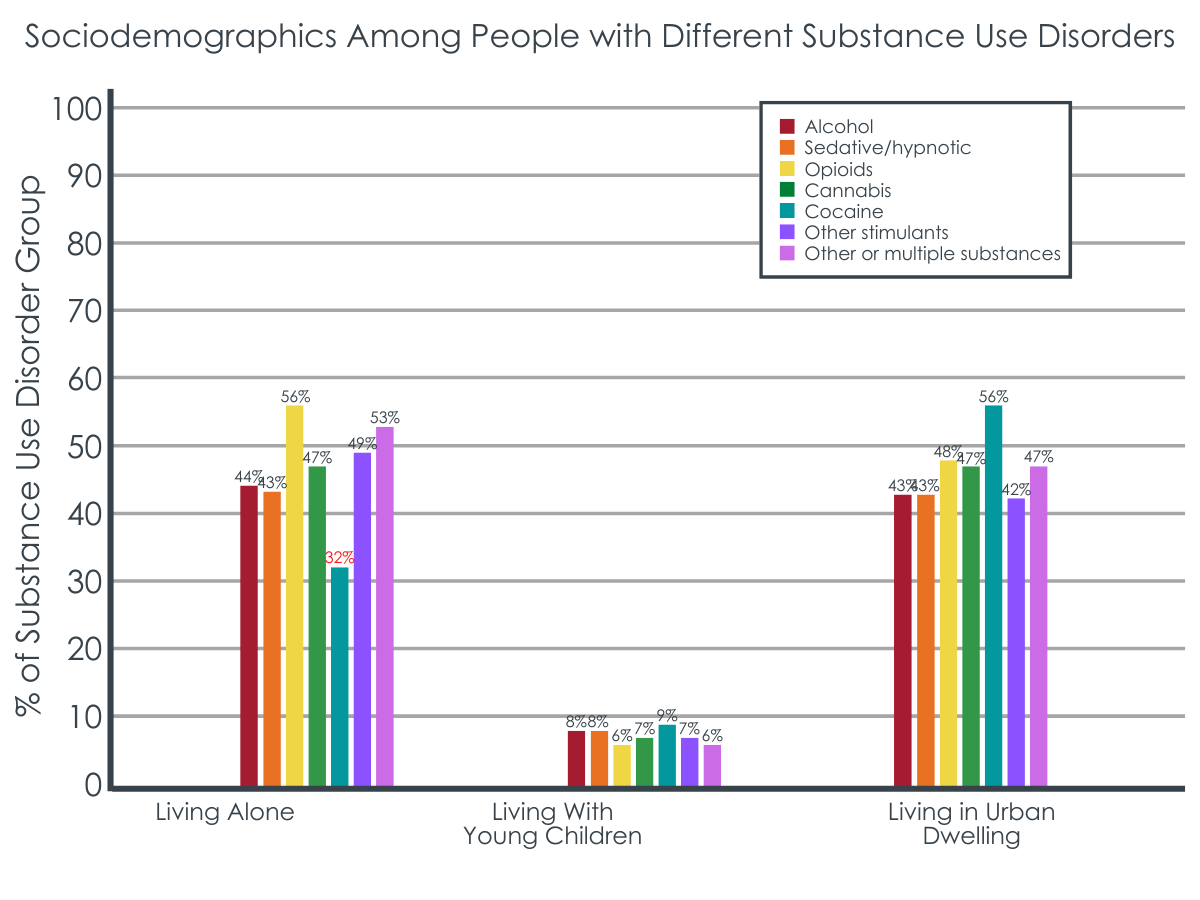
Figures 2 and 3. The highest and lowest percentages within each sociodemographic category that differed from all other substance use disorders are shown in bold red ink. Individuals with opioid use disorder were more likely than those with all other substance use disorders to have a low level of education and to receive government financial assistance and were the least likely to be employed. Individuals with cocaine use disorder were significantly less likely to be living alone relative to those with all other substance use disorders.
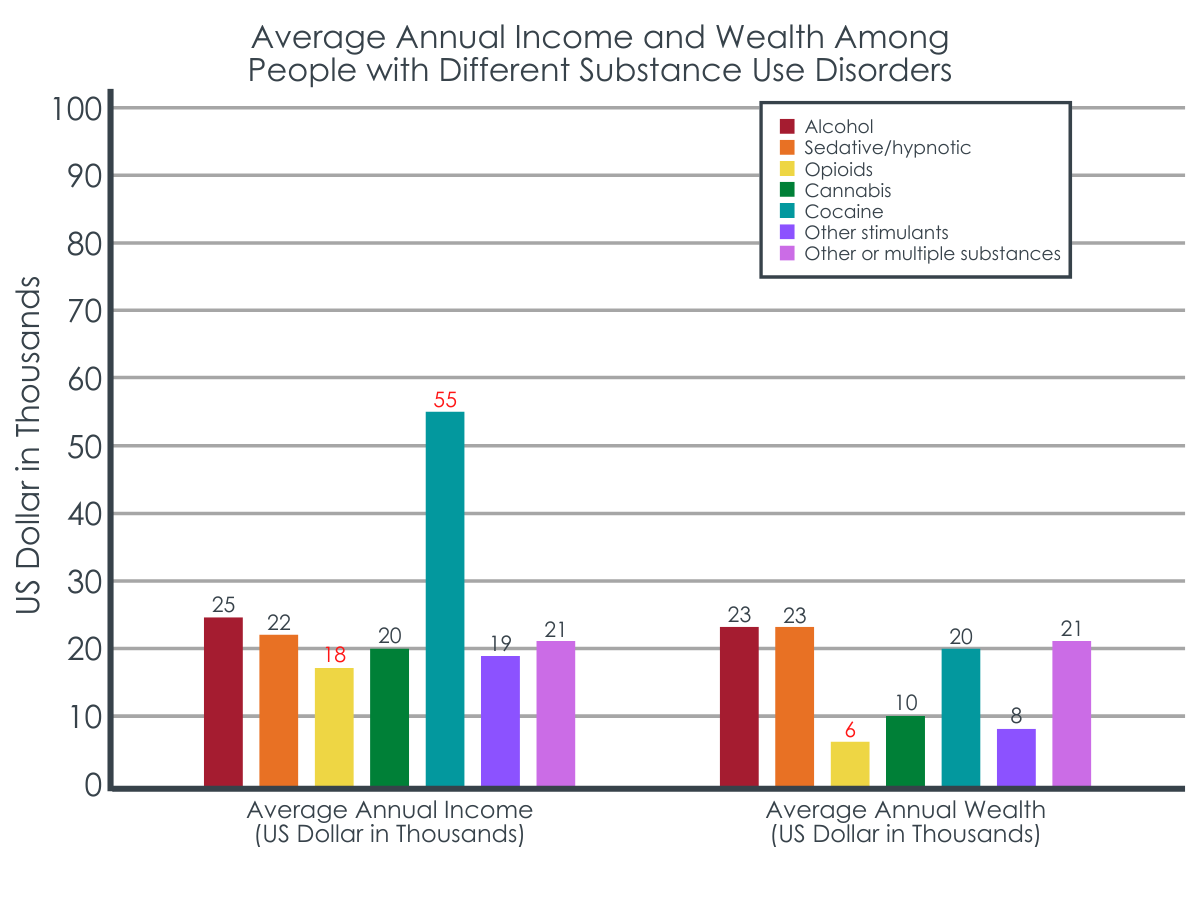
Figure 4. The highest and lowest values within each sociodemographic category that differed from all other substance use disorders are shown in bold red ink. Individuals with opioid use disorder had significantly lower average annual income and lower average annual wealth compared to all other substance use disorders. Individuals with cocaine use disorder had a significantly higher average annual income relative to all other substance use disorder groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand the characteristics of individuals who have substance use disorders, and how these characteristics differ by substance type. Studies like this can ultimately help us better understand the barriers to long-term recovery that patients might be facing which can inform individualized treatment plans and programs geared toward addressing disparities in certain substance use disorder populations.
The outcomes of this study are consistent with prior research conducted in other countries (e.g., United States, Finland, etc.), showing that individuals with substance use disorders have demographic and socioeconomic characteristics that put them at a disadvantage relative to the general population, including financial and educational disadvantages. Prior studies have found that living with a partner or being married may be a protective factor against developing a substance use disorder, and this study further suggests that living with young children may also be a protective factor. Whether these sociodemographic factors came before or after the substance use disorder developed is unclear, but these disadvantages have important implications for how healthcare systems can help support individuals in treatment and recovery. Understanding the differences between various types of substance use disorders can further inform individualized treatment approaches that help create an equal playing field for successful recovery outcomes.
In this study, individuals with opioid use disorders were most likely to have disadvantages, a finding demonstrated in previous research. For example, individuals with a history of opioid use disorder in the United States are shown to have lower employment rates and quality of life relative to individuals without a history of opioid problems. Even among people in recovery, those recovering from opioid problems show larger disadvantages, including lower recovery capital (resources that are needed to support recovery, such as basic needs, employment, social support, etc.) compared to individuals recovering from other substance use problems like alcohol and cannabis. These disadvantages may place individuals with opioid use disorder at increased risk for recurrence of substance use and disorder symptoms after treatment and work against their long-term recovery. Indeed studies show that being employed is associated with higher quality of life, self-esteem, and happiness. Therefore, it appears that healthcare and government systems might benefit from implementing employment training and access programs that help individuals who are seeking recovery from opioid use disorder. Doing so could help individuals acquire the skills and resources they need to build a stronger foundation from which they can launch a successful recovery journey, including adequate education and job skills/opportunities that can promote financial stability and long-term wellbeing to support recovery. Though licit substance use disorders like alcohol use disorder are associated with fewer disadvantages than the other substances, this group was still less well-off than the general population and, therefore, also require assistance to improve their social and economic wellbeing.
It is worth noting that addiction treatment is a public health service that is offered virtually free of charge in Norway, limiting the influence of financial barriers to treatment entry and completion on this study’s outcomes. Though treatment is more financially accessible in Norway, economic-related disparities nonetheless emerged for individuals with substance use disorders which could hinder successful recovery after treatment completion. For example, reduced income and wealth relative to the general population might limit one’s ability to flourish beyond treatment if opportunities do not arise to grow financial resources that help one afford basic needs and build recovery capital. Individuals with illicit substance use disorders, opioid use disorder in particular, appear to be more greatly disadvantaged financially and might require enhanced support to boost their economic status during/after treatment. Programs that help one obtain vocational skills and employment, or that help individuals plan for investment and retirement, might help promote financial stability in addition to long-term well-being.
This study was conducted in Norway among individuals in addiction treatment. Individual differences in addiction treatment across healthcare systems and drug policies in different countries demand additional research.
This data was collected as part of the government’s healthcare data system and missing data has the potential to influence outcomes. Prospective studies are needed to enhance this area of research and to determine whether certain sociodemographic characteristics precede substance use disorders and constitute risk factors, or if they emerge after the disorder has developed.
The population-level data that was intended to represent the healthy control group happened to include 353 patients who were also included in the treatment patient sample and additional research without overlapping samples is needed. This study did not define the type of opioids considered in the opioid use disorder group (e.g., heroin, fentanyl, prescription) and did not compare each substance group to the general population, calling for additional research.
BOTTOM LINE
Individuals with substance use disorder were more socially and economically disadvantaged relative to the general population, such that they had a lower average annual income and lower annual wealth, were more likely to have a low level of education, to be unemployed, and to receive disability pensions and government financial assistance. Those who had illicit substance use disorders faced more pronounced socioeconomic obstacles than individuals with licit substance use disorders. Specifically, those with opioid use disorder faced the greatest degree of disadvantage relative to the other substance groups, whereas those with alcohol use disorder and cocaine use disorder fared somewhat better.
For individuals and families seeking recovery: Every patient enters treatment with a unique set of needs and challenges but knowing someone’s primary substance on treatment entry (e.g., opioids) may help alert clinicians and programs to assess for and more aggressively address potential socio-economic deficits that lie outside their typical clinical purview (e.g., employment). Individualized treatment and recovery plans that cater to a person’s unique situation and help to enhance areas of their life that need improving may ultimately support their recovery.
For treatment professionals and treatment systems: Healthcare systems might benefit from developing individualized treatment plans that cater much more specifically to each patient’s particular set of non-clinical (e.g., employment) as well as clinical challenges. Doing so may ultimately help patients build more recovery capital, which can promote long-term successful recovery. Partnering with community-based programs that address these disadvantages (e.g., vocational and educational programs, employment programs) might help support patients’ treatment and recovery. In the US, Recovery Community Centers are designed to do exactly this.
For scientists:Prospective research is needed to better identify which sociodemographic and economic factors are risk factors for developing substance use disorders or if they develop as a consequence of the disorder. Studies directly comparing the general population to various sub populations of individuals with different substance use disorders are also needed to better understand the magnitude of disadvantage in each subgroup and inform the development of novel policies and programs that address them. The studies of additional social and economic factors, their interactions, and the role of national/local drug policies would also help to advance treatment and recovery approaches.
For policy makers: Socioeconomic disadvantages (e.g., lower education, lower income, etc.) faced by individuals seeking treatment for substance use disorder can hinder treatment effectiveness and recovery. Providing opportunities that allow individuals to flourish during and after treatment can ensure individuals build the recovery capital (resources) they need to become an active member of society and sustain their recovery. Programs that help one obtain vocational skills and employment, and that help individuals plan for investment and retirement, might help offset socioeconomic barriers to recovery faced by many with substance use disorder. Providing tools for socioeconomic stability also has the potential to boost a region’s workforce and reduce the number of individuals needing government financial assistance.
Demographic, social, and economic factors associated with substance use disorders are important for developing individualized treatment plans and offering services that meet the needs of specific sub-populations. Characterizing sociodemographic factors in drug-specific populations can also inform new policies to help address inequalities in healthcare systems that hinder recovery among individuals with certain substance use disorders and sociodemographic backgrounds.
Though previous studies have evaluated the sociodemographics associated with substance use disorders in treatment settings or in the broader population, there are several limitations to this research. Data that concern the entire population are often restricted to the evaluation of the most prevalent types of substance use disorders (e.g., alcohol, cannabis), which limit important comparisons between less prevalent drug use disorders with significant societal impact (e.g., opioids, sedatives). Moreover, few largescale (e.g., national) investigations of treatment-seeking populations have compared sociodemographic factors across multiple different drug classes, restricting our ability to make drug-specific conclusions and recommendations.
Additional large-scale population level research looking at the sociodemographic and economic characteristics associated with specific substance use disorders among individuals in addiction treatment is needed to further inform our understanding of addiction and enhance individualized treatment approaches. International research is also needed to speak to cultural (e.g., drug trends) and healthcare differences (e.g., publicly vs. privately funded addiction healthcare systems) that might influence different findings in different countries. In this study, the researchers used national Norwegian public health data to evaluate sociodemographic differences between individuals receiving publicly funded substance use disorder treatment and the general population, and between individuals with different types of substance use disorders.
HOW WAS THIS STUDY CONDUCTED?
The research team conducted a national retrospective case-control study of 31,245 individuals with substance use disorders who were enrolled in treatment in Norway, and 31,275 individuals from the general population in Norway (i.e., control group).
Two primary datasets were used to extract sociodemographic data, including the Norwegian Patient Registry and the Norwegian National Population Register. The Norwegian Patient Registry, consisting of the entire population of patients in Norway’s public specialized healthcare system, was used to extract a sample of individuals with a primary diagnosis of substance use disorder who were admitted to specialized substance use disorder treatment or a psychiatric hospital between 2009 and 2010. The Norwegian National Population Register was used to obtain a random sample of age and gender matched individuals from the general population who were surveyed in 2010.
Substance use disorders assessed in this study included a primary diagnosis of: 1) alcohol use disorder (40%), 2) opioid use disorder (19%), 3) cannabis use disorder (11%), 4) sedative/hypnotic use disorder (5%; e.g., benzodiazepines), 5) cocaine use disorder (1%), 6) other stimulants (7%; e.g., amphetamines), and 7) other substance use disorders or several substance use disorders (17%), which may have included alcohol and/or sedatives/hypnotics. These disorders were also grouped into licit and illicit substance use disorders. Licit substance use disorder (45%) included alcohol use disorder and sedative/hypnotic use disorder. Illicit substance use disorder (55%) included all other categories.
Sociodemographic variables of interest included:
Low education level (i.e., % who did not complete mandatory education of at least ~7-10 years)
Employed (i.e., % of those aged 18 – 66 years receiving income from work or business)
Average annual income (in Norwegian Krone currency)
Average annual wealth (i.e., capital income, bank deposits, equity, bond and money market funds, shares, & assets; in Norwegian Krone currency)
Receiving financial assistance (i.e., % receiving temporary government benefits to cover basic needs)
Receiving a disability pension (i.e., % aged 18 – 66 receiving permanent government benefits for permanently reduced work capacity (≥ 50%) due to illness/injury, including substance use disorder)
Living alone (% living alone)
Living with young children (i.e., % living with a child under six years of age)
Urban dwelling (i.e., % living in cities with > 50,000 residents)
Sociodemographic factors (percentages and averages) were compared between patient vs. control populations and between patients with illicit vs. licit substance use disorders. Means and percentages among specific substance groups were also compared by examining differences between patients with different types of substance use disorder.
WHAT DID THIS STUDY FIND?
Individuals with substance use disorders were more disadvantaged in all sociodemographic and economic categories.
Compared to the general population, individuals admitted to substance use disorder treatment were more likely to have a low level of education, to have a father with a low level of education, to live alone in an urban dwelling, and to receive disability pensions and government financial assistance.
The general population had a greater percentage of people who lived with young children and were employed, with a higher average annual income and higher annual wealth.
Individuals with an illicit substance use disorder were more disadvantaged in all sociodemographic and economic categories.
Compared to individuals with licit substance use disorders and controlling for age and gender, those with illicit substance use disorders were more likely to have a low level of education, to have a father with a low level of education, to live alone in an urban dwelling, and to receive disability pensions and government financial assistance.
A greater percentage of people with a licit substance use disorder lived with young children and were employed, with a higher average annual income and higher average annual wealth.
Figure 1. This figure shows sociodemographic differences between the general Norwegian population and individuals in Norway who were admitted to treatment for a substance use disorder, as well as differences between those with a primary diagnosis of a licit versus illicit substance use disorder. Those with any substance use disorder had disadvantaged sociodemographic and economic characteristics across all categories, relative to the general population. Compared to individuals with licit substance use disorders, those with illicit disorders had disadvantaged sociodemographic and economic characteristics across all categories. In this study, licit substance use disorders included 1) alcohol use disorder and 2) sedative/hypnotic use disorder, whereas illicit substance use disorders included 1) opioid use disorder, 2) cannabis use disorder, 3) cocaine use disorder, 4) other stimulant use disorders, and 5) ‘other substance use disorders or multiple primary substance use disorders.
The opioid group was particularly disadvantaged.
Individuals with opioid use disorder had the highest percentage of individuals with low educational achievement, who were living alone, receiving government financial assistance and disability pensions. They also had the lowest likelihood of being employed, the lowest average annual income, and the lowest average annual wealth.
Individuals with alcohol use disorder and those with cocaine use disorder were most likely to be employed, had the highest average annual income, and were the least likely to have low educational attainment, to receive disability pensions and government financial assistance. In addition, individuals with cocaine use disorder less commonly lived alone and were most likely to live in an urban dwelling.
Figures 2 and 3. The highest and lowest percentages within each sociodemographic category that differed from all other substance use disorders are shown in bold red ink. Individuals with opioid use disorder were more likely than those with all other substance use disorders to have a low level of education and to receive government financial assistance and were the least likely to be employed. Individuals with cocaine use disorder were significantly less likely to be living alone relative to those with all other substance use disorders.
Figure 4. The highest and lowest values within each sociodemographic category that differed from all other substance use disorders are shown in bold red ink. Individuals with opioid use disorder had significantly lower average annual income and lower average annual wealth compared to all other substance use disorders. Individuals with cocaine use disorder had a significantly higher average annual income relative to all other substance use disorder groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand the characteristics of individuals who have substance use disorders, and how these characteristics differ by substance type. Studies like this can ultimately help us better understand the barriers to long-term recovery that patients might be facing which can inform individualized treatment plans and programs geared toward addressing disparities in certain substance use disorder populations.
The outcomes of this study are consistent with prior research conducted in other countries (e.g., United States, Finland, etc.), showing that individuals with substance use disorders have demographic and socioeconomic characteristics that put them at a disadvantage relative to the general population, including financial and educational disadvantages. Prior studies have found that living with a partner or being married may be a protective factor against developing a substance use disorder, and this study further suggests that living with young children may also be a protective factor. Whether these sociodemographic factors came before or after the substance use disorder developed is unclear, but these disadvantages have important implications for how healthcare systems can help support individuals in treatment and recovery. Understanding the differences between various types of substance use disorders can further inform individualized treatment approaches that help create an equal playing field for successful recovery outcomes.
In this study, individuals with opioid use disorders were most likely to have disadvantages, a finding demonstrated in previous research. For example, individuals with a history of opioid use disorder in the United States are shown to have lower employment rates and quality of life relative to individuals without a history of opioid problems. Even among people in recovery, those recovering from opioid problems show larger disadvantages, including lower recovery capital (resources that are needed to support recovery, such as basic needs, employment, social support, etc.) compared to individuals recovering from other substance use problems like alcohol and cannabis. These disadvantages may place individuals with opioid use disorder at increased risk for recurrence of substance use and disorder symptoms after treatment and work against their long-term recovery. Indeed studies show that being employed is associated with higher quality of life, self-esteem, and happiness. Therefore, it appears that healthcare and government systems might benefit from implementing employment training and access programs that help individuals who are seeking recovery from opioid use disorder. Doing so could help individuals acquire the skills and resources they need to build a stronger foundation from which they can launch a successful recovery journey, including adequate education and job skills/opportunities that can promote financial stability and long-term wellbeing to support recovery. Though licit substance use disorders like alcohol use disorder are associated with fewer disadvantages than the other substances, this group was still less well-off than the general population and, therefore, also require assistance to improve their social and economic wellbeing.
It is worth noting that addiction treatment is a public health service that is offered virtually free of charge in Norway, limiting the influence of financial barriers to treatment entry and completion on this study’s outcomes. Though treatment is more financially accessible in Norway, economic-related disparities nonetheless emerged for individuals with substance use disorders which could hinder successful recovery after treatment completion. For example, reduced income and wealth relative to the general population might limit one’s ability to flourish beyond treatment if opportunities do not arise to grow financial resources that help one afford basic needs and build recovery capital. Individuals with illicit substance use disorders, opioid use disorder in particular, appear to be more greatly disadvantaged financially and might require enhanced support to boost their economic status during/after treatment. Programs that help one obtain vocational skills and employment, or that help individuals plan for investment and retirement, might help promote financial stability in addition to long-term well-being.
This study was conducted in Norway among individuals in addiction treatment. Individual differences in addiction treatment across healthcare systems and drug policies in different countries demand additional research.
This data was collected as part of the government’s healthcare data system and missing data has the potential to influence outcomes. Prospective studies are needed to enhance this area of research and to determine whether certain sociodemographic characteristics precede substance use disorders and constitute risk factors, or if they emerge after the disorder has developed.
The population-level data that was intended to represent the healthy control group happened to include 353 patients who were also included in the treatment patient sample and additional research without overlapping samples is needed. This study did not define the type of opioids considered in the opioid use disorder group (e.g., heroin, fentanyl, prescription) and did not compare each substance group to the general population, calling for additional research.
BOTTOM LINE
Individuals with substance use disorder were more socially and economically disadvantaged relative to the general population, such that they had a lower average annual income and lower annual wealth, were more likely to have a low level of education, to be unemployed, and to receive disability pensions and government financial assistance. Those who had illicit substance use disorders faced more pronounced socioeconomic obstacles than individuals with licit substance use disorders. Specifically, those with opioid use disorder faced the greatest degree of disadvantage relative to the other substance groups, whereas those with alcohol use disorder and cocaine use disorder fared somewhat better.
For individuals and families seeking recovery: Every patient enters treatment with a unique set of needs and challenges but knowing someone’s primary substance on treatment entry (e.g., opioids) may help alert clinicians and programs to assess for and more aggressively address potential socio-economic deficits that lie outside their typical clinical purview (e.g., employment). Individualized treatment and recovery plans that cater to a person’s unique situation and help to enhance areas of their life that need improving may ultimately support their recovery.
For treatment professionals and treatment systems: Healthcare systems might benefit from developing individualized treatment plans that cater much more specifically to each patient’s particular set of non-clinical (e.g., employment) as well as clinical challenges. Doing so may ultimately help patients build more recovery capital, which can promote long-term successful recovery. Partnering with community-based programs that address these disadvantages (e.g., vocational and educational programs, employment programs) might help support patients’ treatment and recovery. In the US, Recovery Community Centers are designed to do exactly this.
For scientists:Prospective research is needed to better identify which sociodemographic and economic factors are risk factors for developing substance use disorders or if they develop as a consequence of the disorder. Studies directly comparing the general population to various sub populations of individuals with different substance use disorders are also needed to better understand the magnitude of disadvantage in each subgroup and inform the development of novel policies and programs that address them. The studies of additional social and economic factors, their interactions, and the role of national/local drug policies would also help to advance treatment and recovery approaches.
For policy makers: Socioeconomic disadvantages (e.g., lower education, lower income, etc.) faced by individuals seeking treatment for substance use disorder can hinder treatment effectiveness and recovery. Providing opportunities that allow individuals to flourish during and after treatment can ensure individuals build the recovery capital (resources) they need to become an active member of society and sustain their recovery. Programs that help one obtain vocational skills and employment, and that help individuals plan for investment and retirement, might help offset socioeconomic barriers to recovery faced by many with substance use disorder. Providing tools for socioeconomic stability also has the potential to boost a region’s workforce and reduce the number of individuals needing government financial assistance.
Demographic, social, and economic factors associated with substance use disorders are important for developing individualized treatment plans and offering services that meet the needs of specific sub-populations. Characterizing sociodemographic factors in drug-specific populations can also inform new policies to help address inequalities in healthcare systems that hinder recovery among individuals with certain substance use disorders and sociodemographic backgrounds.
Though previous studies have evaluated the sociodemographics associated with substance use disorders in treatment settings or in the broader population, there are several limitations to this research. Data that concern the entire population are often restricted to the evaluation of the most prevalent types of substance use disorders (e.g., alcohol, cannabis), which limit important comparisons between less prevalent drug use disorders with significant societal impact (e.g., opioids, sedatives). Moreover, few largescale (e.g., national) investigations of treatment-seeking populations have compared sociodemographic factors across multiple different drug classes, restricting our ability to make drug-specific conclusions and recommendations.
Additional large-scale population level research looking at the sociodemographic and economic characteristics associated with specific substance use disorders among individuals in addiction treatment is needed to further inform our understanding of addiction and enhance individualized treatment approaches. International research is also needed to speak to cultural (e.g., drug trends) and healthcare differences (e.g., publicly vs. privately funded addiction healthcare systems) that might influence different findings in different countries. In this study, the researchers used national Norwegian public health data to evaluate sociodemographic differences between individuals receiving publicly funded substance use disorder treatment and the general population, and between individuals with different types of substance use disorders.
HOW WAS THIS STUDY CONDUCTED?
The research team conducted a national retrospective case-control study of 31,245 individuals with substance use disorders who were enrolled in treatment in Norway, and 31,275 individuals from the general population in Norway (i.e., control group).
Two primary datasets were used to extract sociodemographic data, including the Norwegian Patient Registry and the Norwegian National Population Register. The Norwegian Patient Registry, consisting of the entire population of patients in Norway’s public specialized healthcare system, was used to extract a sample of individuals with a primary diagnosis of substance use disorder who were admitted to specialized substance use disorder treatment or a psychiatric hospital between 2009 and 2010. The Norwegian National Population Register was used to obtain a random sample of age and gender matched individuals from the general population who were surveyed in 2010.
Substance use disorders assessed in this study included a primary diagnosis of: 1) alcohol use disorder (40%), 2) opioid use disorder (19%), 3) cannabis use disorder (11%), 4) sedative/hypnotic use disorder (5%; e.g., benzodiazepines), 5) cocaine use disorder (1%), 6) other stimulants (7%; e.g., amphetamines), and 7) other substance use disorders or several substance use disorders (17%), which may have included alcohol and/or sedatives/hypnotics. These disorders were also grouped into licit and illicit substance use disorders. Licit substance use disorder (45%) included alcohol use disorder and sedative/hypnotic use disorder. Illicit substance use disorder (55%) included all other categories.
Sociodemographic variables of interest included:
Low education level (i.e., % who did not complete mandatory education of at least ~7-10 years)
Employed (i.e., % of those aged 18 – 66 years receiving income from work or business)
Average annual income (in Norwegian Krone currency)
Average annual wealth (i.e., capital income, bank deposits, equity, bond and money market funds, shares, & assets; in Norwegian Krone currency)
Receiving financial assistance (i.e., % receiving temporary government benefits to cover basic needs)
Receiving a disability pension (i.e., % aged 18 – 66 receiving permanent government benefits for permanently reduced work capacity (≥ 50%) due to illness/injury, including substance use disorder)
Living alone (% living alone)
Living with young children (i.e., % living with a child under six years of age)
Urban dwelling (i.e., % living in cities with > 50,000 residents)
Sociodemographic factors (percentages and averages) were compared between patient vs. control populations and between patients with illicit vs. licit substance use disorders. Means and percentages among specific substance groups were also compared by examining differences between patients with different types of substance use disorder.
WHAT DID THIS STUDY FIND?
Individuals with substance use disorders were more disadvantaged in all sociodemographic and economic categories.
Compared to the general population, individuals admitted to substance use disorder treatment were more likely to have a low level of education, to have a father with a low level of education, to live alone in an urban dwelling, and to receive disability pensions and government financial assistance.
The general population had a greater percentage of people who lived with young children and were employed, with a higher average annual income and higher annual wealth.
Individuals with an illicit substance use disorder were more disadvantaged in all sociodemographic and economic categories.
Compared to individuals with licit substance use disorders and controlling for age and gender, those with illicit substance use disorders were more likely to have a low level of education, to have a father with a low level of education, to live alone in an urban dwelling, and to receive disability pensions and government financial assistance.
A greater percentage of people with a licit substance use disorder lived with young children and were employed, with a higher average annual income and higher average annual wealth.
Figure 1. This figure shows sociodemographic differences between the general Norwegian population and individuals in Norway who were admitted to treatment for a substance use disorder, as well as differences between those with a primary diagnosis of a licit versus illicit substance use disorder. Those with any substance use disorder had disadvantaged sociodemographic and economic characteristics across all categories, relative to the general population. Compared to individuals with licit substance use disorders, those with illicit disorders had disadvantaged sociodemographic and economic characteristics across all categories. In this study, licit substance use disorders included 1) alcohol use disorder and 2) sedative/hypnotic use disorder, whereas illicit substance use disorders included 1) opioid use disorder, 2) cannabis use disorder, 3) cocaine use disorder, 4) other stimulant use disorders, and 5) ‘other substance use disorders or multiple primary substance use disorders.
The opioid group was particularly disadvantaged.
Individuals with opioid use disorder had the highest percentage of individuals with low educational achievement, who were living alone, receiving government financial assistance and disability pensions. They also had the lowest likelihood of being employed, the lowest average annual income, and the lowest average annual wealth.
Individuals with alcohol use disorder and those with cocaine use disorder were most likely to be employed, had the highest average annual income, and were the least likely to have low educational attainment, to receive disability pensions and government financial assistance. In addition, individuals with cocaine use disorder less commonly lived alone and were most likely to live in an urban dwelling.
Figures 2 and 3. The highest and lowest percentages within each sociodemographic category that differed from all other substance use disorders are shown in bold red ink. Individuals with opioid use disorder were more likely than those with all other substance use disorders to have a low level of education and to receive government financial assistance and were the least likely to be employed. Individuals with cocaine use disorder were significantly less likely to be living alone relative to those with all other substance use disorders.
Figure 4. The highest and lowest values within each sociodemographic category that differed from all other substance use disorders are shown in bold red ink. Individuals with opioid use disorder had significantly lower average annual income and lower average annual wealth compared to all other substance use disorders. Individuals with cocaine use disorder had a significantly higher average annual income relative to all other substance use disorder groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand the characteristics of individuals who have substance use disorders, and how these characteristics differ by substance type. Studies like this can ultimately help us better understand the barriers to long-term recovery that patients might be facing which can inform individualized treatment plans and programs geared toward addressing disparities in certain substance use disorder populations.
The outcomes of this study are consistent with prior research conducted in other countries (e.g., United States, Finland, etc.), showing that individuals with substance use disorders have demographic and socioeconomic characteristics that put them at a disadvantage relative to the general population, including financial and educational disadvantages. Prior studies have found that living with a partner or being married may be a protective factor against developing a substance use disorder, and this study further suggests that living with young children may also be a protective factor. Whether these sociodemographic factors came before or after the substance use disorder developed is unclear, but these disadvantages have important implications for how healthcare systems can help support individuals in treatment and recovery. Understanding the differences between various types of substance use disorders can further inform individualized treatment approaches that help create an equal playing field for successful recovery outcomes.
In this study, individuals with opioid use disorders were most likely to have disadvantages, a finding demonstrated in previous research. For example, individuals with a history of opioid use disorder in the United States are shown to have lower employment rates and quality of life relative to individuals without a history of opioid problems. Even among people in recovery, those recovering from opioid problems show larger disadvantages, including lower recovery capital (resources that are needed to support recovery, such as basic needs, employment, social support, etc.) compared to individuals recovering from other substance use problems like alcohol and cannabis. These disadvantages may place individuals with opioid use disorder at increased risk for recurrence of substance use and disorder symptoms after treatment and work against their long-term recovery. Indeed studies show that being employed is associated with higher quality of life, self-esteem, and happiness. Therefore, it appears that healthcare and government systems might benefit from implementing employment training and access programs that help individuals who are seeking recovery from opioid use disorder. Doing so could help individuals acquire the skills and resources they need to build a stronger foundation from which they can launch a successful recovery journey, including adequate education and job skills/opportunities that can promote financial stability and long-term wellbeing to support recovery. Though licit substance use disorders like alcohol use disorder are associated with fewer disadvantages than the other substances, this group was still less well-off than the general population and, therefore, also require assistance to improve their social and economic wellbeing.
It is worth noting that addiction treatment is a public health service that is offered virtually free of charge in Norway, limiting the influence of financial barriers to treatment entry and completion on this study’s outcomes. Though treatment is more financially accessible in Norway, economic-related disparities nonetheless emerged for individuals with substance use disorders which could hinder successful recovery after treatment completion. For example, reduced income and wealth relative to the general population might limit one’s ability to flourish beyond treatment if opportunities do not arise to grow financial resources that help one afford basic needs and build recovery capital. Individuals with illicit substance use disorders, opioid use disorder in particular, appear to be more greatly disadvantaged financially and might require enhanced support to boost their economic status during/after treatment. Programs that help one obtain vocational skills and employment, or that help individuals plan for investment and retirement, might help promote financial stability in addition to long-term well-being.
This study was conducted in Norway among individuals in addiction treatment. Individual differences in addiction treatment across healthcare systems and drug policies in different countries demand additional research.
This data was collected as part of the government’s healthcare data system and missing data has the potential to influence outcomes. Prospective studies are needed to enhance this area of research and to determine whether certain sociodemographic characteristics precede substance use disorders and constitute risk factors, or if they emerge after the disorder has developed.
The population-level data that was intended to represent the healthy control group happened to include 353 patients who were also included in the treatment patient sample and additional research without overlapping samples is needed. This study did not define the type of opioids considered in the opioid use disorder group (e.g., heroin, fentanyl, prescription) and did not compare each substance group to the general population, calling for additional research.
BOTTOM LINE
Individuals with substance use disorder were more socially and economically disadvantaged relative to the general population, such that they had a lower average annual income and lower annual wealth, were more likely to have a low level of education, to be unemployed, and to receive disability pensions and government financial assistance. Those who had illicit substance use disorders faced more pronounced socioeconomic obstacles than individuals with licit substance use disorders. Specifically, those with opioid use disorder faced the greatest degree of disadvantage relative to the other substance groups, whereas those with alcohol use disorder and cocaine use disorder fared somewhat better.
For individuals and families seeking recovery: Every patient enters treatment with a unique set of needs and challenges but knowing someone’s primary substance on treatment entry (e.g., opioids) may help alert clinicians and programs to assess for and more aggressively address potential socio-economic deficits that lie outside their typical clinical purview (e.g., employment). Individualized treatment and recovery plans that cater to a person’s unique situation and help to enhance areas of their life that need improving may ultimately support their recovery.
For treatment professionals and treatment systems: Healthcare systems might benefit from developing individualized treatment plans that cater much more specifically to each patient’s particular set of non-clinical (e.g., employment) as well as clinical challenges. Doing so may ultimately help patients build more recovery capital, which can promote long-term successful recovery. Partnering with community-based programs that address these disadvantages (e.g., vocational and educational programs, employment programs) might help support patients’ treatment and recovery. In the US, Recovery Community Centers are designed to do exactly this.
For scientists:Prospective research is needed to better identify which sociodemographic and economic factors are risk factors for developing substance use disorders or if they develop as a consequence of the disorder. Studies directly comparing the general population to various sub populations of individuals with different substance use disorders are also needed to better understand the magnitude of disadvantage in each subgroup and inform the development of novel policies and programs that address them. The studies of additional social and economic factors, their interactions, and the role of national/local drug policies would also help to advance treatment and recovery approaches.
For policy makers: Socioeconomic disadvantages (e.g., lower education, lower income, etc.) faced by individuals seeking treatment for substance use disorder can hinder treatment effectiveness and recovery. Providing opportunities that allow individuals to flourish during and after treatment can ensure individuals build the recovery capital (resources) they need to become an active member of society and sustain their recovery. Programs that help one obtain vocational skills and employment, and that help individuals plan for investment and retirement, might help offset socioeconomic barriers to recovery faced by many with substance use disorder. Providing tools for socioeconomic stability also has the potential to boost a region’s workforce and reduce the number of individuals needing government financial assistance.