Belief in disease model associated with support for harm reduction
Public opinion towards harm reduction services has been mixed, which can prevent their adoption or limit the funding needed to continue providing these services over time. Understanding factors that can be influenced to increase support for harm reduction services may ultimately lead to greater implementation of these public health resources. This study aimed to identify the demographic factors and the knowledge, beliefs, and attitudes that are associated with support for harm reduction services.
Harm reduction services (e.g., syringe service programs, naloxone to reverse overdose) are often community-based resources designed to address opioid use disorder and help end the ongoing opioid crisis. Yet, public opinion towards them has generally been negative and unsupportive, also corresponding with limited, albeit increasing, support from elected public officials. This resistance to community-based substance use disorder services is heightened when services are offered in one’s own neighborhood and in communities with low “social capital.”
Certain knowledge, beliefs, and attitudes regarding opioid use disorder may in part reflect a community’s level of social capital and, in turn, support for resources that can help people with opioid use disorder. Understanding and improving these factors may lead to increased public support for community resources, which can lead to greater implementation of services.
The researchers in this study aimed to identify the factors that are associated with support for harm reduction services. Such research can help shed light on potential gaps in knowledge about opioid use disorder and beliefs and attitudes that may be strengthened if positive, or mitigated if negative, to increase support for critical services that address the opioid crisis.
HOW WAS THIS STUDY CONDUCTED?
The research team surveyed residents of a rural county in South Carolina to identify demographic factors and the knowledge, beliefs, and attitudes that are associated with support for harm reduction services. This survey included items that assessed respondents’ demographic information, beliefs, and attitudes about individuals with opioid use disorder and medications for opioid use disorder, and knowledge about substance use disorders.
Respondents completed the survey online or on paper between May and June 2022. If on paper, responses were then entered into the survey platform by research assistants. Solicitations to complete the survey were distributed through social media (e.g., Facebook), email, and in 4 primary care offices throughout the county.
The main outcome of interest was support for harm reduction services, as measured by the number of statements that respondents indicated that they agreed with. These 9 statements included items such as, “I would support having a syringe service program in my neighborhood” and “Emergency naloxone boxes should be placed in public places for emergency response to overdose.” The researchers calculated a harm reduction support score, which ranged from 0 to 9.
The researchers included 22 of the other survey items that they considered to be related to the knowledge, beliefs, and attitudes they were most interested in. These 22 items were included in the statistical analyses examining associations with the support score and differences between groups.
In total, 338 residents responded to the survey. Of these, the majority were White (88.6%), not Hispanic or Latino/a (96.9%), and female (68.1%). Approximately half were between 12 and 54 years old (47.8%) and the other approximate half were 55 years old and older (52.2%). A little more than half were married (62.4%), employed part- or full-time (56.1%), and had a household income of $50,000 or more (61.1%).
WHAT DID THIS STUDY FIND?
Younger and employed respondents indicated more harm reduction support.
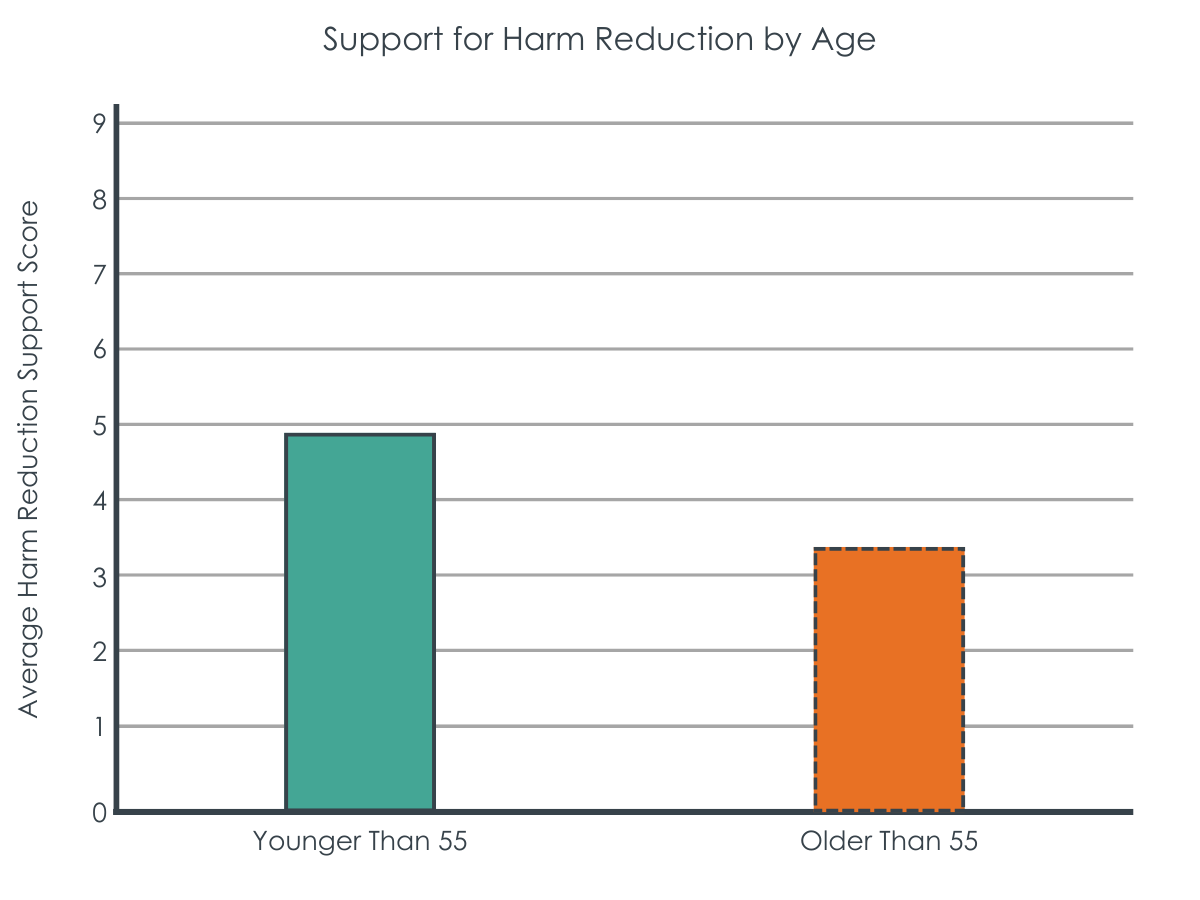
Age and employment status were associated with differences in support for harm reduction services. Respondents who were younger than 55 years old had an average support score of 4.9 (out of a possible 9), while those older than 55 had an average support score of 3.4. This is considered a fairly large difference between the 2 groups.
Respondents who were employed part- or full-time had an average support score of 4.6, while those with other employment statuses, such as unemployed or retired, had an average support score of 3.5. This is considered a medium-sized difference between the 2 groups.
There were no differences between the support scores for the demographic factors of gender, ethnicity, race, marital status, or income level.
Belief in disease model and effectiveness of medications associated with more harm reduction support.
Agreeing that opioid use disorder is a disease showed the strongest association with support for harm reduction services. Respondents who agreed with the statement, “An opioid use disorder is a real illness like diabetes and heart disease,” had an average support score of 4.46, while those who disagreed with the statement had an average support score of 3.13. This is a medium-sized difference.
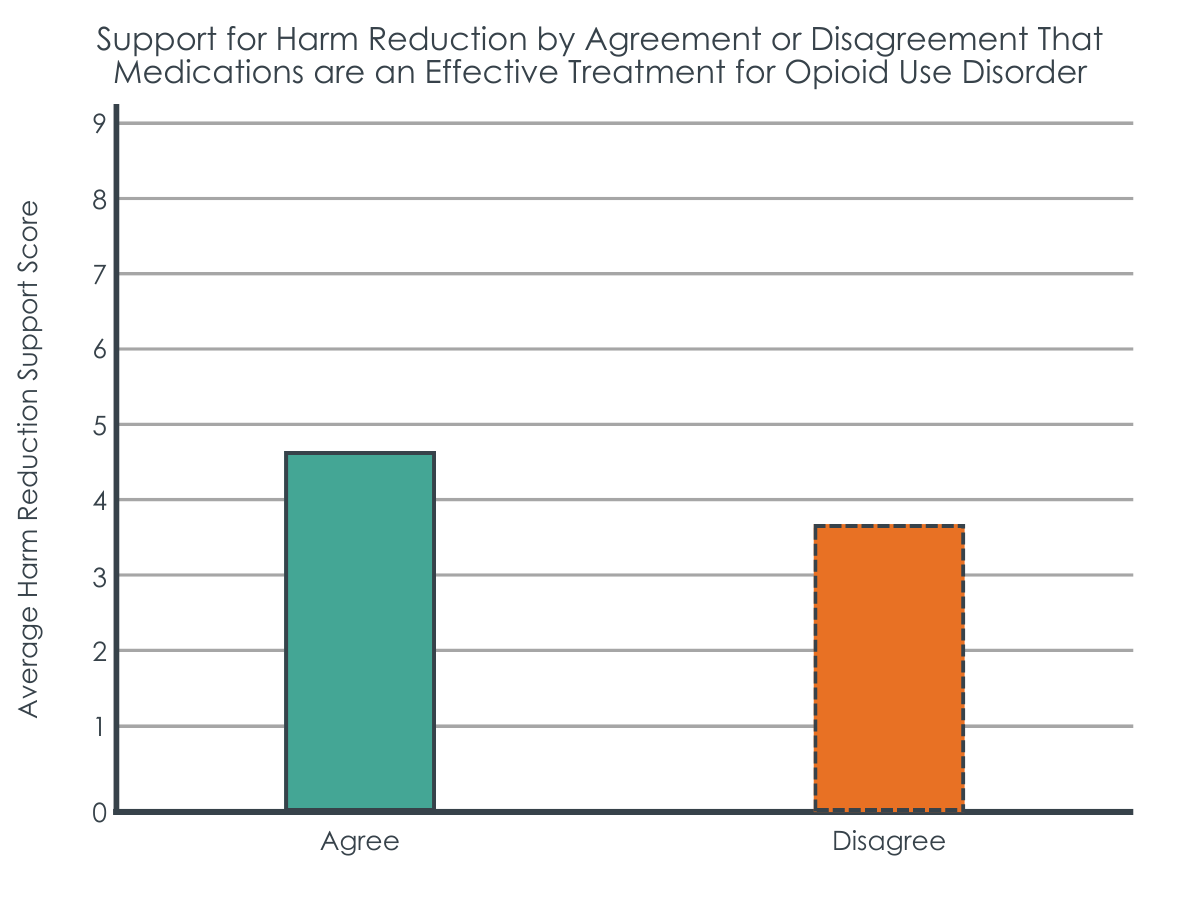
Agreeing that medications were effective was also strongly associated with higher levels of support. Respondents who agreed with the statement, “Medications for opioid use disorder, specifically buprenorphine, methadone, and naltrexone, is an effective treatment for opioid use disorder,” had an average support score of 4.73, while those who disagreed had an average score of 3.79. This is a medium-sized difference.
Less stigmatizing attitudes associated with higher support scores.
Agreeing with the following statements were associated with higher support scores than disagreeing: being willing to live in the same neighborhood as someone with an opioid use disorder (4.81 vs. 3.83); an individual with an opioid use disorder having the same right to a job as anyone else (4.79 vs. 3.61); the importance of being part of a supportive community for individuals with opioid use disorder (4.33 vs. 3.00); and being willing to administer naloxone to a stranger in an overdose situation (4.55 vs. 3.67). The differences between those who agreed and disagreed were generally medium-sized.
Disagreeing with the following statements were associated with higher support scores than agreeing: a person who is addicted to drugs being able to stop using drugs if they really wanted to (4.51 vs. 3.80); abstinence-based therapy being the only successful form of treatment for substance use disorders (4.67 vs. 3.63); and individuals with opioid use disorder being likely to be dangerous (4.78 vs. 3.62). The differences between those who disagreed and agreed were in the small to medium range.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study assessed the demographic factors and the knowledge, beliefs, and attitudes that are associated with support for harm reduction among residents of a rural county in South Carolina. Results showed that support was higher among younger respondents, those who were employed at least part time, those who agreed that opioid use disorder is a disease and that medications are effective, and those who held less stigmatizing attitudes.
These results suggest that increasing community awareness of the disease model of opioid use disorder and the effectiveness of medications for opioid use disorder, especially among older and unemployed or retired populations, could be a step toward increasing support for harm reduction service resources in the community. This is somewhat of a surprise, given that, anecdotally, understanding opioid use disorder as a disease has been thought to be associated with being against harm reduction services. Given the high level of pushback for implementing harm reduction services, better understanding of the factors that can be addressed may help increase social capital and public support for community resources.
While support was higher among younger respondents, those who were employed at least part time, those who agreed that opioid use disorder is a disease and that medications are effective, and those who held less stigmatizing attitudes, the average support scores were still quite low. Indeed, none of the scores were higher than 5, out of the highest possible score of 9. This reflects that negative and unsupportive attitudes are persisting, despite recent shifts towards more positive attitudes.
Further, support for certain harm reduction services was higher than others, particularly when it may directly affect the person or have financial implications. For instance, 90.7% of participants agreed that they would support HIV and Hepatitis C screening in the county and 82.9% agreed that they would support condom distribution in the county. However, support for syringe-related services was considerably lower, with 42.3% of participants agreeing that they would support the concept of syringe service programs in the community and 45.1% agreeing that they would support safe consumption sites. Support was further reduced when the syringe service program would be in their neighborhood, with only 21.0% of participants agreeing to support it, and when financial support was involved, with only 11.5% of participants agreeing that they would provide financial support for a syringe service program. These results reflect general support for harm reduction services, but not a willingness to allow them in close proximity or financially support them.
Recovery capital, a theory related to the concept of social capital, suggests having more recovery-supportive people in one’s network, and having stronger connections with them, promotes improved substance use and other recovery outcomes. These include influences such as bonding with others in the community and having access to sobriety-based fellowship. In this context, the results of the current study could extend to also improving recovery capital, providing another avenue for addressing the opioid crisis.
Of note, there may be particular characteristics of the people who chose to respond to the survey that differentiate them from people who chose to not to respond (i.e., selection effects). For example, it may be that the people who responded had stronger feelings about opioids that increased their willingness to respond, while those who did not respond may have had more neutral or indifferent feelings about such services. This could have biased the results by making them stronger one way or another than they may have been otherwise.
Despite this, this study helps shed light on gaps in knowledge about opioid use disorder and beliefs and attitudes that can be improved to increase community support for critical services that address the opioid crisis. Community support is vital to gaining support from elected public officials and implementing more harm reduction services.
The survey was conducted with residents of a rural county in South Carolina. The results may not generalize to other populations, such as other rural areas in the US, suburban areas, or other countries.
Respondents could only respond to the survey items with 2 options – “agree” or “disagree.” This limits the amount of nuance that is obtained from the results. For instance, including additional options that capture a range of agreement (e.g., strongly disagree, disagree, neutral, agree, strongly agree) would be more informative about the respondents’ beliefs and attitudes.
The harm reduction support score that the researchers developed had an internal consistency that was acceptable, but on the low side. Internal consistency, or how reliable an instrument is, is typically estimated by Cronbach’s alpha, with an estimate of .70 and above indicating good consistency. However, an estimate of .90 and above would indicate the best consistency. The support score used in this study had a Cronbach’s alpha of .72, suggesting that the 9 items may not all be measuring the same thing (the harm reduction domain) reliably and there may be some of the items in the 9-item scale that could be removed, improved, or exchanged for other items to improve reliability of the scale.
BOTTOM LINE
Support for harm reduction services was higher among younger respondents, those who were employed at least part time, those who agreed that opioid use disorder is a disease and that medications are effective, and those who held less stigmatizing attitudes. Holding public health campaigns and having discussions with peers about these issues may increase awareness and public support, thereby gaining support from elected public officials, which can lead to greater implementation of harm reduction services.
For individuals and families seeking recovery: The study’s results suggest that conceptualizing and framing opioid use disorder as a disease, improving knowledge about the effectiveness of medications for opioid use disorder, and promoting destigmatizing and supportive beliefs and attitudes, may lead to increased community support for harm reduction services. Therefore, if individuals discuss these concepts with their peers and help destigmatize opioid use disorder, social capital and support for services may be improved.
For treatment professionals and treatment systems: The study’s results suggest that treatment professionals and systems who conceptualize and frame opioid use disorder as a medical disease and improve knowledge about the effectiveness of medications for opioid use disorder though public health campaigns, may increase community support for harm reduction services. In addition, professionals and systems who facilitate and campaign for destigmatizing beliefs and attitudes may also increase community support. As (typically) trusted resources of the medical community, treatment professionals and systems are in a unique and particularly advantageous position to raise awareness and destigmatize opioid use disorder.
For scientists: Given that the response options in the current study’s survey were only “agree” and “disagree,” future research that includes a range of agreement options would provide more nuance and information regarding the extent to which the items are associated with support for harm reduction services. Further, additional research that assesses support for services with a more comprehensive, reliable, and valid measure would increase confidence in the results.
For policy makers: Results from this study suggest that community support for harm reduction services is higher when people believe more that opioid use disorder is a disease and understand the effectiveness of medications used to treat it, especially among older and unemployed or retired populations. Accordingly, policy makers may help increase support by implementing public health campaigns to raise awareness of the disease model and effectiveness of medications, particularly if they were targeted towards older and unemployed or retired populations.
Harm reduction services (e.g., syringe service programs, naloxone to reverse overdose) are often community-based resources designed to address opioid use disorder and help end the ongoing opioid crisis. Yet, public opinion towards them has generally been negative and unsupportive, also corresponding with limited, albeit increasing, support from elected public officials. This resistance to community-based substance use disorder services is heightened when services are offered in one’s own neighborhood and in communities with low “social capital.”
Certain knowledge, beliefs, and attitudes regarding opioid use disorder may in part reflect a community’s level of social capital and, in turn, support for resources that can help people with opioid use disorder. Understanding and improving these factors may lead to increased public support for community resources, which can lead to greater implementation of services.
The researchers in this study aimed to identify the factors that are associated with support for harm reduction services. Such research can help shed light on potential gaps in knowledge about opioid use disorder and beliefs and attitudes that may be strengthened if positive, or mitigated if negative, to increase support for critical services that address the opioid crisis.
HOW WAS THIS STUDY CONDUCTED?
The research team surveyed residents of a rural county in South Carolina to identify demographic factors and the knowledge, beliefs, and attitudes that are associated with support for harm reduction services. This survey included items that assessed respondents’ demographic information, beliefs, and attitudes about individuals with opioid use disorder and medications for opioid use disorder, and knowledge about substance use disorders.
Respondents completed the survey online or on paper between May and June 2022. If on paper, responses were then entered into the survey platform by research assistants. Solicitations to complete the survey were distributed through social media (e.g., Facebook), email, and in 4 primary care offices throughout the county.
The main outcome of interest was support for harm reduction services, as measured by the number of statements that respondents indicated that they agreed with. These 9 statements included items such as, “I would support having a syringe service program in my neighborhood” and “Emergency naloxone boxes should be placed in public places for emergency response to overdose.” The researchers calculated a harm reduction support score, which ranged from 0 to 9.
The researchers included 22 of the other survey items that they considered to be related to the knowledge, beliefs, and attitudes they were most interested in. These 22 items were included in the statistical analyses examining associations with the support score and differences between groups.
In total, 338 residents responded to the survey. Of these, the majority were White (88.6%), not Hispanic or Latino/a (96.9%), and female (68.1%). Approximately half were between 12 and 54 years old (47.8%) and the other approximate half were 55 years old and older (52.2%). A little more than half were married (62.4%), employed part- or full-time (56.1%), and had a household income of $50,000 or more (61.1%).
WHAT DID THIS STUDY FIND?
Younger and employed respondents indicated more harm reduction support.
Age and employment status were associated with differences in support for harm reduction services. Respondents who were younger than 55 years old had an average support score of 4.9 (out of a possible 9), while those older than 55 had an average support score of 3.4. This is considered a fairly large difference between the 2 groups.
Respondents who were employed part- or full-time had an average support score of 4.6, while those with other employment statuses, such as unemployed or retired, had an average support score of 3.5. This is considered a medium-sized difference between the 2 groups.
There were no differences between the support scores for the demographic factors of gender, ethnicity, race, marital status, or income level.
Belief in disease model and effectiveness of medications associated with more harm reduction support.
Agreeing that opioid use disorder is a disease showed the strongest association with support for harm reduction services. Respondents who agreed with the statement, “An opioid use disorder is a real illness like diabetes and heart disease,” had an average support score of 4.46, while those who disagreed with the statement had an average support score of 3.13. This is a medium-sized difference.
Agreeing that medications were effective was also strongly associated with higher levels of support. Respondents who agreed with the statement, “Medications for opioid use disorder, specifically buprenorphine, methadone, and naltrexone, is an effective treatment for opioid use disorder,” had an average support score of 4.73, while those who disagreed had an average score of 3.79. This is a medium-sized difference.
Less stigmatizing attitudes associated with higher support scores.
Agreeing with the following statements were associated with higher support scores than disagreeing: being willing to live in the same neighborhood as someone with an opioid use disorder (4.81 vs. 3.83); an individual with an opioid use disorder having the same right to a job as anyone else (4.79 vs. 3.61); the importance of being part of a supportive community for individuals with opioid use disorder (4.33 vs. 3.00); and being willing to administer naloxone to a stranger in an overdose situation (4.55 vs. 3.67). The differences between those who agreed and disagreed were generally medium-sized.
Disagreeing with the following statements were associated with higher support scores than agreeing: a person who is addicted to drugs being able to stop using drugs if they really wanted to (4.51 vs. 3.80); abstinence-based therapy being the only successful form of treatment for substance use disorders (4.67 vs. 3.63); and individuals with opioid use disorder being likely to be dangerous (4.78 vs. 3.62). The differences between those who disagreed and agreed were in the small to medium range.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study assessed the demographic factors and the knowledge, beliefs, and attitudes that are associated with support for harm reduction among residents of a rural county in South Carolina. Results showed that support was higher among younger respondents, those who were employed at least part time, those who agreed that opioid use disorder is a disease and that medications are effective, and those who held less stigmatizing attitudes.
These results suggest that increasing community awareness of the disease model of opioid use disorder and the effectiveness of medications for opioid use disorder, especially among older and unemployed or retired populations, could be a step toward increasing support for harm reduction service resources in the community. This is somewhat of a surprise, given that, anecdotally, understanding opioid use disorder as a disease has been thought to be associated with being against harm reduction services. Given the high level of pushback for implementing harm reduction services, better understanding of the factors that can be addressed may help increase social capital and public support for community resources.
While support was higher among younger respondents, those who were employed at least part time, those who agreed that opioid use disorder is a disease and that medications are effective, and those who held less stigmatizing attitudes, the average support scores were still quite low. Indeed, none of the scores were higher than 5, out of the highest possible score of 9. This reflects that negative and unsupportive attitudes are persisting, despite recent shifts towards more positive attitudes.
Further, support for certain harm reduction services was higher than others, particularly when it may directly affect the person or have financial implications. For instance, 90.7% of participants agreed that they would support HIV and Hepatitis C screening in the county and 82.9% agreed that they would support condom distribution in the county. However, support for syringe-related services was considerably lower, with 42.3% of participants agreeing that they would support the concept of syringe service programs in the community and 45.1% agreeing that they would support safe consumption sites. Support was further reduced when the syringe service program would be in their neighborhood, with only 21.0% of participants agreeing to support it, and when financial support was involved, with only 11.5% of participants agreeing that they would provide financial support for a syringe service program. These results reflect general support for harm reduction services, but not a willingness to allow them in close proximity or financially support them.
Recovery capital, a theory related to the concept of social capital, suggests having more recovery-supportive people in one’s network, and having stronger connections with them, promotes improved substance use and other recovery outcomes. These include influences such as bonding with others in the community and having access to sobriety-based fellowship. In this context, the results of the current study could extend to also improving recovery capital, providing another avenue for addressing the opioid crisis.
Of note, there may be particular characteristics of the people who chose to respond to the survey that differentiate them from people who chose to not to respond (i.e., selection effects). For example, it may be that the people who responded had stronger feelings about opioids that increased their willingness to respond, while those who did not respond may have had more neutral or indifferent feelings about such services. This could have biased the results by making them stronger one way or another than they may have been otherwise.
Despite this, this study helps shed light on gaps in knowledge about opioid use disorder and beliefs and attitudes that can be improved to increase community support for critical services that address the opioid crisis. Community support is vital to gaining support from elected public officials and implementing more harm reduction services.
The survey was conducted with residents of a rural county in South Carolina. The results may not generalize to other populations, such as other rural areas in the US, suburban areas, or other countries.
Respondents could only respond to the survey items with 2 options – “agree” or “disagree.” This limits the amount of nuance that is obtained from the results. For instance, including additional options that capture a range of agreement (e.g., strongly disagree, disagree, neutral, agree, strongly agree) would be more informative about the respondents’ beliefs and attitudes.
The harm reduction support score that the researchers developed had an internal consistency that was acceptable, but on the low side. Internal consistency, or how reliable an instrument is, is typically estimated by Cronbach’s alpha, with an estimate of .70 and above indicating good consistency. However, an estimate of .90 and above would indicate the best consistency. The support score used in this study had a Cronbach’s alpha of .72, suggesting that the 9 items may not all be measuring the same thing (the harm reduction domain) reliably and there may be some of the items in the 9-item scale that could be removed, improved, or exchanged for other items to improve reliability of the scale.
BOTTOM LINE
Support for harm reduction services was higher among younger respondents, those who were employed at least part time, those who agreed that opioid use disorder is a disease and that medications are effective, and those who held less stigmatizing attitudes. Holding public health campaigns and having discussions with peers about these issues may increase awareness and public support, thereby gaining support from elected public officials, which can lead to greater implementation of harm reduction services.
For individuals and families seeking recovery: The study’s results suggest that conceptualizing and framing opioid use disorder as a disease, improving knowledge about the effectiveness of medications for opioid use disorder, and promoting destigmatizing and supportive beliefs and attitudes, may lead to increased community support for harm reduction services. Therefore, if individuals discuss these concepts with their peers and help destigmatize opioid use disorder, social capital and support for services may be improved.
For treatment professionals and treatment systems: The study’s results suggest that treatment professionals and systems who conceptualize and frame opioid use disorder as a medical disease and improve knowledge about the effectiveness of medications for opioid use disorder though public health campaigns, may increase community support for harm reduction services. In addition, professionals and systems who facilitate and campaign for destigmatizing beliefs and attitudes may also increase community support. As (typically) trusted resources of the medical community, treatment professionals and systems are in a unique and particularly advantageous position to raise awareness and destigmatize opioid use disorder.
For scientists: Given that the response options in the current study’s survey were only “agree” and “disagree,” future research that includes a range of agreement options would provide more nuance and information regarding the extent to which the items are associated with support for harm reduction services. Further, additional research that assesses support for services with a more comprehensive, reliable, and valid measure would increase confidence in the results.
For policy makers: Results from this study suggest that community support for harm reduction services is higher when people believe more that opioid use disorder is a disease and understand the effectiveness of medications used to treat it, especially among older and unemployed or retired populations. Accordingly, policy makers may help increase support by implementing public health campaigns to raise awareness of the disease model and effectiveness of medications, particularly if they were targeted towards older and unemployed or retired populations.
Harm reduction services (e.g., syringe service programs, naloxone to reverse overdose) are often community-based resources designed to address opioid use disorder and help end the ongoing opioid crisis. Yet, public opinion towards them has generally been negative and unsupportive, also corresponding with limited, albeit increasing, support from elected public officials. This resistance to community-based substance use disorder services is heightened when services are offered in one’s own neighborhood and in communities with low “social capital.”
Certain knowledge, beliefs, and attitudes regarding opioid use disorder may in part reflect a community’s level of social capital and, in turn, support for resources that can help people with opioid use disorder. Understanding and improving these factors may lead to increased public support for community resources, which can lead to greater implementation of services.
The researchers in this study aimed to identify the factors that are associated with support for harm reduction services. Such research can help shed light on potential gaps in knowledge about opioid use disorder and beliefs and attitudes that may be strengthened if positive, or mitigated if negative, to increase support for critical services that address the opioid crisis.
HOW WAS THIS STUDY CONDUCTED?
The research team surveyed residents of a rural county in South Carolina to identify demographic factors and the knowledge, beliefs, and attitudes that are associated with support for harm reduction services. This survey included items that assessed respondents’ demographic information, beliefs, and attitudes about individuals with opioid use disorder and medications for opioid use disorder, and knowledge about substance use disorders.
Respondents completed the survey online or on paper between May and June 2022. If on paper, responses were then entered into the survey platform by research assistants. Solicitations to complete the survey were distributed through social media (e.g., Facebook), email, and in 4 primary care offices throughout the county.
The main outcome of interest was support for harm reduction services, as measured by the number of statements that respondents indicated that they agreed with. These 9 statements included items such as, “I would support having a syringe service program in my neighborhood” and “Emergency naloxone boxes should be placed in public places for emergency response to overdose.” The researchers calculated a harm reduction support score, which ranged from 0 to 9.
The researchers included 22 of the other survey items that they considered to be related to the knowledge, beliefs, and attitudes they were most interested in. These 22 items were included in the statistical analyses examining associations with the support score and differences between groups.
In total, 338 residents responded to the survey. Of these, the majority were White (88.6%), not Hispanic or Latino/a (96.9%), and female (68.1%). Approximately half were between 12 and 54 years old (47.8%) and the other approximate half were 55 years old and older (52.2%). A little more than half were married (62.4%), employed part- or full-time (56.1%), and had a household income of $50,000 or more (61.1%).
WHAT DID THIS STUDY FIND?
Younger and employed respondents indicated more harm reduction support.
Age and employment status were associated with differences in support for harm reduction services. Respondents who were younger than 55 years old had an average support score of 4.9 (out of a possible 9), while those older than 55 had an average support score of 3.4. This is considered a fairly large difference between the 2 groups.
Respondents who were employed part- or full-time had an average support score of 4.6, while those with other employment statuses, such as unemployed or retired, had an average support score of 3.5. This is considered a medium-sized difference between the 2 groups.
There were no differences between the support scores for the demographic factors of gender, ethnicity, race, marital status, or income level.
Belief in disease model and effectiveness of medications associated with more harm reduction support.
Agreeing that opioid use disorder is a disease showed the strongest association with support for harm reduction services. Respondents who agreed with the statement, “An opioid use disorder is a real illness like diabetes and heart disease,” had an average support score of 4.46, while those who disagreed with the statement had an average support score of 3.13. This is a medium-sized difference.
Agreeing that medications were effective was also strongly associated with higher levels of support. Respondents who agreed with the statement, “Medications for opioid use disorder, specifically buprenorphine, methadone, and naltrexone, is an effective treatment for opioid use disorder,” had an average support score of 4.73, while those who disagreed had an average score of 3.79. This is a medium-sized difference.
Less stigmatizing attitudes associated with higher support scores.
Agreeing with the following statements were associated with higher support scores than disagreeing: being willing to live in the same neighborhood as someone with an opioid use disorder (4.81 vs. 3.83); an individual with an opioid use disorder having the same right to a job as anyone else (4.79 vs. 3.61); the importance of being part of a supportive community for individuals with opioid use disorder (4.33 vs. 3.00); and being willing to administer naloxone to a stranger in an overdose situation (4.55 vs. 3.67). The differences between those who agreed and disagreed were generally medium-sized.
Disagreeing with the following statements were associated with higher support scores than agreeing: a person who is addicted to drugs being able to stop using drugs if they really wanted to (4.51 vs. 3.80); abstinence-based therapy being the only successful form of treatment for substance use disorders (4.67 vs. 3.63); and individuals with opioid use disorder being likely to be dangerous (4.78 vs. 3.62). The differences between those who disagreed and agreed were in the small to medium range.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study assessed the demographic factors and the knowledge, beliefs, and attitudes that are associated with support for harm reduction among residents of a rural county in South Carolina. Results showed that support was higher among younger respondents, those who were employed at least part time, those who agreed that opioid use disorder is a disease and that medications are effective, and those who held less stigmatizing attitudes.
These results suggest that increasing community awareness of the disease model of opioid use disorder and the effectiveness of medications for opioid use disorder, especially among older and unemployed or retired populations, could be a step toward increasing support for harm reduction service resources in the community. This is somewhat of a surprise, given that, anecdotally, understanding opioid use disorder as a disease has been thought to be associated with being against harm reduction services. Given the high level of pushback for implementing harm reduction services, better understanding of the factors that can be addressed may help increase social capital and public support for community resources.
While support was higher among younger respondents, those who were employed at least part time, those who agreed that opioid use disorder is a disease and that medications are effective, and those who held less stigmatizing attitudes, the average support scores were still quite low. Indeed, none of the scores were higher than 5, out of the highest possible score of 9. This reflects that negative and unsupportive attitudes are persisting, despite recent shifts towards more positive attitudes.
Further, support for certain harm reduction services was higher than others, particularly when it may directly affect the person or have financial implications. For instance, 90.7% of participants agreed that they would support HIV and Hepatitis C screening in the county and 82.9% agreed that they would support condom distribution in the county. However, support for syringe-related services was considerably lower, with 42.3% of participants agreeing that they would support the concept of syringe service programs in the community and 45.1% agreeing that they would support safe consumption sites. Support was further reduced when the syringe service program would be in their neighborhood, with only 21.0% of participants agreeing to support it, and when financial support was involved, with only 11.5% of participants agreeing that they would provide financial support for a syringe service program. These results reflect general support for harm reduction services, but not a willingness to allow them in close proximity or financially support them.
Recovery capital, a theory related to the concept of social capital, suggests having more recovery-supportive people in one’s network, and having stronger connections with them, promotes improved substance use and other recovery outcomes. These include influences such as bonding with others in the community and having access to sobriety-based fellowship. In this context, the results of the current study could extend to also improving recovery capital, providing another avenue for addressing the opioid crisis.
Of note, there may be particular characteristics of the people who chose to respond to the survey that differentiate them from people who chose to not to respond (i.e., selection effects). For example, it may be that the people who responded had stronger feelings about opioids that increased their willingness to respond, while those who did not respond may have had more neutral or indifferent feelings about such services. This could have biased the results by making them stronger one way or another than they may have been otherwise.
Despite this, this study helps shed light on gaps in knowledge about opioid use disorder and beliefs and attitudes that can be improved to increase community support for critical services that address the opioid crisis. Community support is vital to gaining support from elected public officials and implementing more harm reduction services.
The survey was conducted with residents of a rural county in South Carolina. The results may not generalize to other populations, such as other rural areas in the US, suburban areas, or other countries.
Respondents could only respond to the survey items with 2 options – “agree” or “disagree.” This limits the amount of nuance that is obtained from the results. For instance, including additional options that capture a range of agreement (e.g., strongly disagree, disagree, neutral, agree, strongly agree) would be more informative about the respondents’ beliefs and attitudes.
The harm reduction support score that the researchers developed had an internal consistency that was acceptable, but on the low side. Internal consistency, or how reliable an instrument is, is typically estimated by Cronbach’s alpha, with an estimate of .70 and above indicating good consistency. However, an estimate of .90 and above would indicate the best consistency. The support score used in this study had a Cronbach’s alpha of .72, suggesting that the 9 items may not all be measuring the same thing (the harm reduction domain) reliably and there may be some of the items in the 9-item scale that could be removed, improved, or exchanged for other items to improve reliability of the scale.
BOTTOM LINE
Support for harm reduction services was higher among younger respondents, those who were employed at least part time, those who agreed that opioid use disorder is a disease and that medications are effective, and those who held less stigmatizing attitudes. Holding public health campaigns and having discussions with peers about these issues may increase awareness and public support, thereby gaining support from elected public officials, which can lead to greater implementation of harm reduction services.
For individuals and families seeking recovery: The study’s results suggest that conceptualizing and framing opioid use disorder as a disease, improving knowledge about the effectiveness of medications for opioid use disorder, and promoting destigmatizing and supportive beliefs and attitudes, may lead to increased community support for harm reduction services. Therefore, if individuals discuss these concepts with their peers and help destigmatize opioid use disorder, social capital and support for services may be improved.
For treatment professionals and treatment systems: The study’s results suggest that treatment professionals and systems who conceptualize and frame opioid use disorder as a medical disease and improve knowledge about the effectiveness of medications for opioid use disorder though public health campaigns, may increase community support for harm reduction services. In addition, professionals and systems who facilitate and campaign for destigmatizing beliefs and attitudes may also increase community support. As (typically) trusted resources of the medical community, treatment professionals and systems are in a unique and particularly advantageous position to raise awareness and destigmatize opioid use disorder.
For scientists: Given that the response options in the current study’s survey were only “agree” and “disagree,” future research that includes a range of agreement options would provide more nuance and information regarding the extent to which the items are associated with support for harm reduction services. Further, additional research that assesses support for services with a more comprehensive, reliable, and valid measure would increase confidence in the results.
For policy makers: Results from this study suggest that community support for harm reduction services is higher when people believe more that opioid use disorder is a disease and understand the effectiveness of medications used to treat it, especially among older and unemployed or retired populations. Accordingly, policy makers may help increase support by implementing public health campaigns to raise awareness of the disease model and effectiveness of medications, particularly if they were targeted towards older and unemployed or retired populations.