Brief interventions at primary care visits associated with reduced drinking for patients with hypertension but not diabetes
Alcohol use exacerbates chronic health conditions such as hypertension and type 2 diabetes. Brief interventions at primary care visits may help patients with these health conditions reduce their alcohol use and improve their overall health and well-being. This study examined the impact of a brief intervention on drinking and relevant health outcomes in patients with hypertension or type 2 diabetes.
Brief Interventions in primary care settings have been recommended to help address alcohol use among patients, but evidence for the efficacy of brief interventions at reducing unhealthy alcohol use and health outcomes has been mixed.
The current research examined associations between receiving a brief intervention designed to reduce alcohol use and 12-month drinking and 18-month health outcomes among adult patients with hypertension and type 2 diabetes who screened positive for unhealthy alcohol use during a primary care visit.
HOW WAS THIS STUDY CONDUCTED?
This study was a population-based observational study using electronic health records data of patients in the Kaiser Permanente Northern California healthcare system. Participants included in the analyses (N=92,621) were patients with hypertension or type 2 diabetes who had screened positive for unhealthy alcohol use at a primary care visit between 2014-2017.
Unhealthy alcohol use was defined as drinking that exceeded 7 drinks per week for women and men aged 66 and older, or >14 drinks per week for men aged 18–65. Patients were excluded from the analyses if they (1) did not have continuous Kaiser Permanente healthcare system membership in the year prior to baseline date; (2) were older than 85 years of age at baseline; or (3) did not have complete baseline alcohol screening data.
The intervention used in the current study was a physician administered brief intervention based on motivational interviewing principles. This included referrals to outpatient addiction medicine treatment. No other information about the brief intervention was provided by the authors.
The primary outcome was alcohol use behavior 12 months post-intervention. Alcohol use was measured in 4 ways: number of heavy drinking days over the past 3 months, number of drinking days per week, drinks per drinking day, and drinks per week from baseline to 12-month follow-up. These behaviors were measured via alcohol screening conducted at primary care visits. The study also examined health outcomes at 18 months post-intervention. These health measures were systolic and diastolic blood pressure and blood sugar (i.e., glycohemoglobin [HbA1c] level and ‘controlled HbA1c’ [HbA1c<8%]) at 18-month follow-up for patients with type 2 diabetes. The authors defined a clinically meaningful improvement in blood pressure to be ≥3 mm Hg reduction from baseline at 18 months. All outcomes were measured as part of routine care visits, and thus were derived from participants’ electronic health records. Because this was a naturalistic study using electronic health records only, follow-up time points were approximate (e.g., drinking measured at the 12-month follow-up was as close to 12 months post-intervention as possible).
The researchers used statistical modeling to compare drinking outcomes at 12 months and health outcomes at 18 months between patients who received the brief intervention and those who did not. The researchers used a statistical modeling technique to adjust for variables associated with receiving the brief intervention and the outcomes (drinking and health outcomes). This analytic method allowed the researchers to account for as many alternative explanations of a potential positive effect of brief intervention as possible, thereby increasing confidence that the intervention caused the positive effects on drinking and/or health outcomes.
Participants included individuals with hypertension (n=72,979) and type 2 diabetes (n=19,642). The majority were male (67.5% and 79.0% for the hypertension group and diabetes group respectively). On average, participants with hypertension were 62 years of age while the average age of participants with type 2 diabetes were60. Most participants were non-Hispanic White (70.5% and 52.8%). At baseline about 17% and 15% of participants reported drinking at levels exceeding daily and weekly limits, respectively. Approximately 5% of participants in both samples had an alcohol use disorder diagnosis. Roughly 17% and 15% of participants with hypertension and type 2 diabetes had co-occurring mental health conditions in the prior year, respectively.
WHAT DID THIS STUDY FIND?
Brief interventions reduced alcohol use only for certain subgroups.
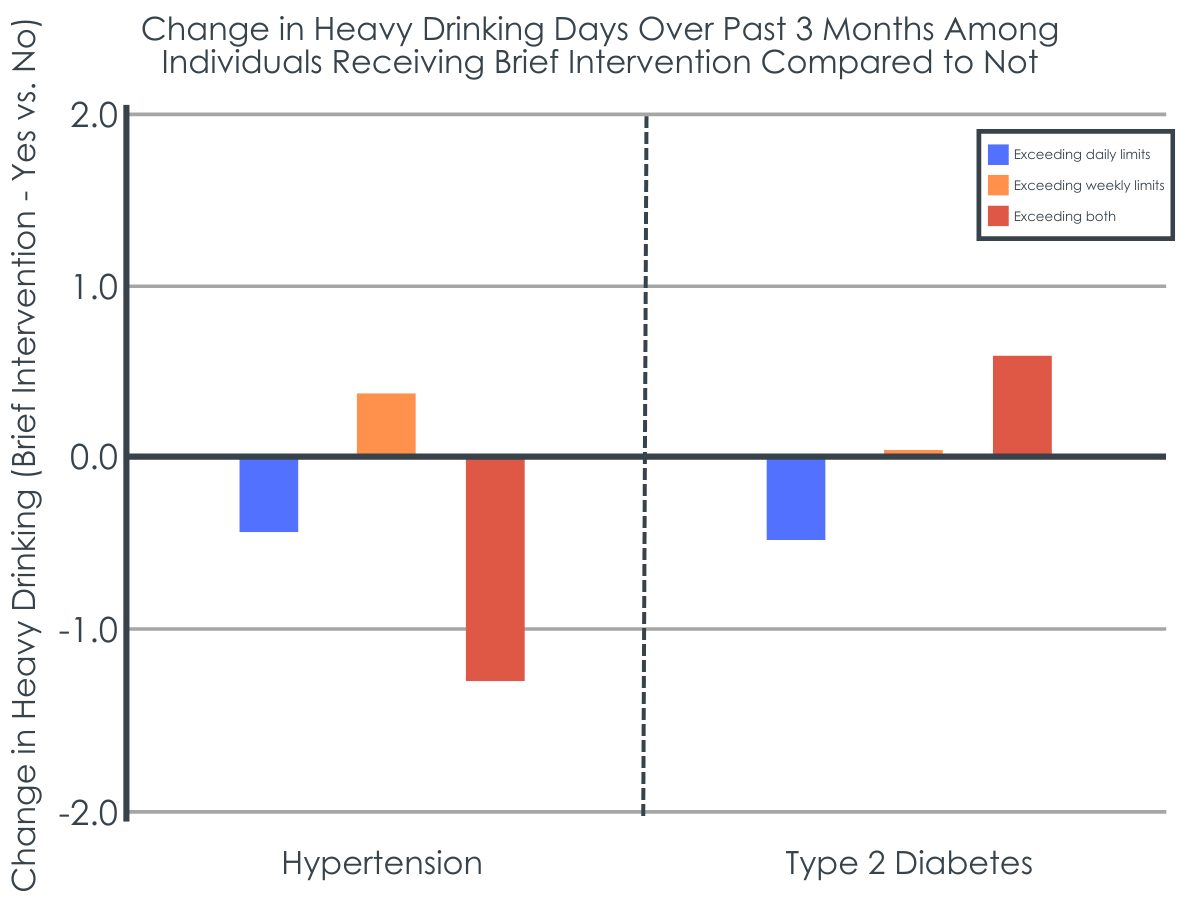
All participants drank less alcohol 12 months post-baseline visit regardless of whether they received the brief intervention. However, for those who exceeded only daily drinking limits at baseline, the brief intervention showed greater reduced alcohol use for all 4 outcomes at 12 months. Hypertension patients who exceeded only weekly alcohol limits or those exceeding both daily and weekly alcohol limits drank at similar levels did not benefit from the brief intervention.
Figure 1. All participants drank less compared to their baseline levels regardless of receiving the brief intervention, but differences were seen in changes in drinking levels between those who received the brief intervention and those who didn’t.
Only patients with type 2 diabetes aged 30-44 drank less after receiving the brief intervention.
All other participants with type 2 diabetes had similar alcohol use reductions whether they received the brief intervention or not.
Receiving the brief intervention was associated with reduced blood pressure only among hypertensive patients.
Among patients with hypertension, those who received a brief intervention had an additional decline in blood pressure at 18 months compared with those who did not. Receiving the brief intervention was associated with a 5% greater likelihood of clinically meaningful improvement. The researchers did not observe an association between getting the brief intervention and blood pressure among patients with type 2 diabetes. There was no impact on blood sugar levels for those with diabetes.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of the study suggest that an alcohol-focused brief intervention delivered in a primary care setting can impact alcohol use and chronic health conditions among specific types of patients with chronic health conditions.
The researchers found that all participants drank less alcohol 12 months post-baseline visit regardless of if they received the brief intervention or not. Participants with hypertension whose drinking exceeded daily drinking limits at baseline had greater reductions than other groups after receiving the intervention. Hypertension patients who exceeded only weekly limits or those exceeding both daily and weekly limits drank at similar levels as the rest of the sample post-intervention. Similarly, only patients with type 2 diabetes aged 30-44 showed more reductions in alcohol use 1-year post intervention. All other patients with type 2 diabetes showed similar reductions in drinking.
This pattern of results may suggest that the impact of brief interventions varies depending on patients’ characteristics. For example, the finding that only participants whose drinking exceeded daily drinking (but not weekly) limits at baseline drank less after receiving the intervention may suggest that regular heavier drinkers may be more open to the advice and feedback presented during brief interventions. Similarly, the fact that patients with type 2 diabetes saw no changes in alcohol use post intervention suggest that factors like type of chronic disease, disease severity, medication intensity and patient adherence to medications and lifestyle changes may play a role in brief interventions effectiveness. These findings suggest that different approaches, including tailoring to population subgroups or health conditions, may be needed to address unhealthy drinking and related health outcomes among patients with chronic conditions.
It is unclear based on the data presented if the sample included patients with both hypertension and type 2 diabetes. If the sample included patients with both conditions, it is possible that some participants were included in both groups and thus impacted the results. If the researchers only included patients with either hypertension or type 2 diabetes (but not those with both conditions) then the generalizability of the results was likely impacted. There is a high degree of comorbidity between these conditions, therefore excluding patients with both does not reflect how the real-world population may respond to the brief intervention. It is possible the management of these conditions simultaneously could impact the intervention’s effectiveness.
The nature of the brief intervention is unclear based on thedescription in text. The authors describe the brief intervention as being an intervention provided by physicians that was “based on motivational interviewing principles.”It is not apparent what the content of the intervention was, nor how well providers administered it. It is unknown what (if any) fidelity protocols were put in place to ensure providers were adequately administering this treatment. Poor adherence to intervention protocols has been associated with lackluster outcomes post-intervention. This makes it unclear how much the observed changes in behavior can be attributable to the brief intervention.
It is unclear if the changes in health outcomes observed at 18 months were the result of the brief intervention. The researchers did not present data on alcohol use at 18-months,so it is unknown if changes in drinking were maintained over time. Furthermore, the sample was entirely comprised of patients who were already in long term care which may have impacted the observed changes in health outcomes (e.g., being prescribed blood pressure medication). Additionally, while the analyses accounted for many clinical and medical factors at baseline that would impact health outcomes over time, it is unclear if the researchers adjusted for time-varying factors which also impact these outcomes (e.g., cigarette smoking cessation, weight loss, etc.).
BOTTOM LINE
Results of this research suggest that a physician administered brief intervention can impact alcohol use and health outcomes among certain types of patients with chronic health conditions. The benefits of the brief intervention to address unhealthy alcohol use for individuals with hypertension and type 2 diabetes varied depending upon individual patient characteristics. Patients with type 2 diabetes aged 30-44 drank less after receiving the brief intervention, whereas all other participants with type 2 diabetes did not drink less alcohol 12 months post–intervention. Participants with hypertension who reported exceeding only daily drinking limits at baseline who received the intervention showed greater reduction on all drinking outcomes 12 months post-intervention. Hypertension patients who exceeded only weekly drinking limits or those exceeding both daily and weekly limits drank at similar levels as the rest of the sample post-intervention. These results suggest that brief interventions targeting alcohol use among primary care patients may not work well for all patients. For example, patients with more severe alcohol use may benefit less from brief interventions.Providers should consider individual patients’ unique demographics/behaviors when deciding to implement a brief intervention or to refer to more intensive treatment. More research is needed to corroborate these findings and test potential interventions.
For individuals and families seeking recovery: Individuals and families seeking recovery may do well to discuss substance use with their medical providers. There are a plethora of treatment options available for substance use issues. Many treatment options are also covered by Medicaid, which further increases access to care. It may also be important for those seeking substance use care to be aware of the signs/symptoms of substance use disorder.
For treatment professionals and treatment systems: Despite the limitations of the present research described, this study suggests brief interventions can be one way to change alcohol use behavior among patients. As such, it is important for providers to adopt screening, brief intervention, and referral to treatment (SBIRT) practices. It can be challenging for physicians given time constraints of office visits and/or the challenges of managing health of patients with chronic conditions. Nevertheless, resources are available for providers to implement SBIRT some of which offer continuing education credit. In addition, new technologies may help automate some SBIRT procedures.
For scientists:Scientific study of the factors which impact the effectiveness of brief interventions may enhance their overall public health impact. Presently, it is unclear precisely how brief interventions impact behavior- that is the psychological/behavioral mechanisms through which brief interventions impact behavior are unclear. In addition, it is not completely clear how individual components of brief interventions impact behavior. For example, some research in motivational interviewing suggests that strict adherence to treatment protocols is less crucial at behavioral change than displaying empathy with participants. Research is needed to better understand what the “active ingredients” of brief interventions may be and how best to utilize them so that they may be scaled, thereby reducing the public health burden of alcohol use.
For policy makers: This study adds to the literature on the effectiveness of brief interventionsin primary care settings. It may be helpful for policymakers to incentivize adoption of SBIRT practices in clinical settings. For instance, by offering compensation to clinics/centers which follow SBIRT guidelines. This could include reimbursement for time spent training clinicians/staff in SBIRT. Another option could be offering training support for clinic staff. This could come in the form of developing automated screening tools for substance use and integrating them into existing electronic health record systems. Another option could be to advertise available free training on SBIRT practices and that these courses can count towardscontinuing education credit.
Brief Interventions in primary care settings have been recommended to help address alcohol use among patients, but evidence for the efficacy of brief interventions at reducing unhealthy alcohol use and health outcomes has been mixed.
The current research examined associations between receiving a brief intervention designed to reduce alcohol use and 12-month drinking and 18-month health outcomes among adult patients with hypertension and type 2 diabetes who screened positive for unhealthy alcohol use during a primary care visit.
HOW WAS THIS STUDY CONDUCTED?
This study was a population-based observational study using electronic health records data of patients in the Kaiser Permanente Northern California healthcare system. Participants included in the analyses (N=92,621) were patients with hypertension or type 2 diabetes who had screened positive for unhealthy alcohol use at a primary care visit between 2014-2017.
Unhealthy alcohol use was defined as drinking that exceeded 7 drinks per week for women and men aged 66 and older, or >14 drinks per week for men aged 18–65. Patients were excluded from the analyses if they (1) did not have continuous Kaiser Permanente healthcare system membership in the year prior to baseline date; (2) were older than 85 years of age at baseline; or (3) did not have complete baseline alcohol screening data.
The intervention used in the current study was a physician administered brief intervention based on motivational interviewing principles. This included referrals to outpatient addiction medicine treatment. No other information about the brief intervention was provided by the authors.
The primary outcome was alcohol use behavior 12 months post-intervention. Alcohol use was measured in 4 ways: number of heavy drinking days over the past 3 months, number of drinking days per week, drinks per drinking day, and drinks per week from baseline to 12-month follow-up. These behaviors were measured via alcohol screening conducted at primary care visits. The study also examined health outcomes at 18 months post-intervention. These health measures were systolic and diastolic blood pressure and blood sugar (i.e., glycohemoglobin [HbA1c] level and ‘controlled HbA1c’ [HbA1c<8%]) at 18-month follow-up for patients with type 2 diabetes. The authors defined a clinically meaningful improvement in blood pressure to be ≥3 mm Hg reduction from baseline at 18 months. All outcomes were measured as part of routine care visits, and thus were derived from participants’ electronic health records. Because this was a naturalistic study using electronic health records only, follow-up time points were approximate (e.g., drinking measured at the 12-month follow-up was as close to 12 months post-intervention as possible).
The researchers used statistical modeling to compare drinking outcomes at 12 months and health outcomes at 18 months between patients who received the brief intervention and those who did not. The researchers used a statistical modeling technique to adjust for variables associated with receiving the brief intervention and the outcomes (drinking and health outcomes). This analytic method allowed the researchers to account for as many alternative explanations of a potential positive effect of brief intervention as possible, thereby increasing confidence that the intervention caused the positive effects on drinking and/or health outcomes.
Participants included individuals with hypertension (n=72,979) and type 2 diabetes (n=19,642). The majority were male (67.5% and 79.0% for the hypertension group and diabetes group respectively). On average, participants with hypertension were 62 years of age while the average age of participants with type 2 diabetes were60. Most participants were non-Hispanic White (70.5% and 52.8%). At baseline about 17% and 15% of participants reported drinking at levels exceeding daily and weekly limits, respectively. Approximately 5% of participants in both samples had an alcohol use disorder diagnosis. Roughly 17% and 15% of participants with hypertension and type 2 diabetes had co-occurring mental health conditions in the prior year, respectively.
WHAT DID THIS STUDY FIND?
Brief interventions reduced alcohol use only for certain subgroups.
All participants drank less alcohol 12 months post-baseline visit regardless of whether they received the brief intervention. However, for those who exceeded only daily drinking limits at baseline, the brief intervention showed greater reduced alcohol use for all 4 outcomes at 12 months. Hypertension patients who exceeded only weekly alcohol limits or those exceeding both daily and weekly alcohol limits drank at similar levels did not benefit from the brief intervention.
Figure 1. All participants drank less compared to their baseline levels regardless of receiving the brief intervention, but differences were seen in changes in drinking levels between those who received the brief intervention and those who didn’t.
Only patients with type 2 diabetes aged 30-44 drank less after receiving the brief intervention.
All other participants with type 2 diabetes had similar alcohol use reductions whether they received the brief intervention or not.
Receiving the brief intervention was associated with reduced blood pressure only among hypertensive patients.
Among patients with hypertension, those who received a brief intervention had an additional decline in blood pressure at 18 months compared with those who did not. Receiving the brief intervention was associated with a 5% greater likelihood of clinically meaningful improvement. The researchers did not observe an association between getting the brief intervention and blood pressure among patients with type 2 diabetes. There was no impact on blood sugar levels for those with diabetes.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of the study suggest that an alcohol-focused brief intervention delivered in a primary care setting can impact alcohol use and chronic health conditions among specific types of patients with chronic health conditions.
The researchers found that all participants drank less alcohol 12 months post-baseline visit regardless of if they received the brief intervention or not. Participants with hypertension whose drinking exceeded daily drinking limits at baseline had greater reductions than other groups after receiving the intervention. Hypertension patients who exceeded only weekly limits or those exceeding both daily and weekly limits drank at similar levels as the rest of the sample post-intervention. Similarly, only patients with type 2 diabetes aged 30-44 showed more reductions in alcohol use 1-year post intervention. All other patients with type 2 diabetes showed similar reductions in drinking.
This pattern of results may suggest that the impact of brief interventions varies depending on patients’ characteristics. For example, the finding that only participants whose drinking exceeded daily drinking (but not weekly) limits at baseline drank less after receiving the intervention may suggest that regular heavier drinkers may be more open to the advice and feedback presented during brief interventions. Similarly, the fact that patients with type 2 diabetes saw no changes in alcohol use post intervention suggest that factors like type of chronic disease, disease severity, medication intensity and patient adherence to medications and lifestyle changes may play a role in brief interventions effectiveness. These findings suggest that different approaches, including tailoring to population subgroups or health conditions, may be needed to address unhealthy drinking and related health outcomes among patients with chronic conditions.
It is unclear based on the data presented if the sample included patients with both hypertension and type 2 diabetes. If the sample included patients with both conditions, it is possible that some participants were included in both groups and thus impacted the results. If the researchers only included patients with either hypertension or type 2 diabetes (but not those with both conditions) then the generalizability of the results was likely impacted. There is a high degree of comorbidity between these conditions, therefore excluding patients with both does not reflect how the real-world population may respond to the brief intervention. It is possible the management of these conditions simultaneously could impact the intervention’s effectiveness.
The nature of the brief intervention is unclear based on thedescription in text. The authors describe the brief intervention as being an intervention provided by physicians that was “based on motivational interviewing principles.”It is not apparent what the content of the intervention was, nor how well providers administered it. It is unknown what (if any) fidelity protocols were put in place to ensure providers were adequately administering this treatment. Poor adherence to intervention protocols has been associated with lackluster outcomes post-intervention. This makes it unclear how much the observed changes in behavior can be attributable to the brief intervention.
It is unclear if the changes in health outcomes observed at 18 months were the result of the brief intervention. The researchers did not present data on alcohol use at 18-months,so it is unknown if changes in drinking were maintained over time. Furthermore, the sample was entirely comprised of patients who were already in long term care which may have impacted the observed changes in health outcomes (e.g., being prescribed blood pressure medication). Additionally, while the analyses accounted for many clinical and medical factors at baseline that would impact health outcomes over time, it is unclear if the researchers adjusted for time-varying factors which also impact these outcomes (e.g., cigarette smoking cessation, weight loss, etc.).
BOTTOM LINE
Results of this research suggest that a physician administered brief intervention can impact alcohol use and health outcomes among certain types of patients with chronic health conditions. The benefits of the brief intervention to address unhealthy alcohol use for individuals with hypertension and type 2 diabetes varied depending upon individual patient characteristics. Patients with type 2 diabetes aged 30-44 drank less after receiving the brief intervention, whereas all other participants with type 2 diabetes did not drink less alcohol 12 months post–intervention. Participants with hypertension who reported exceeding only daily drinking limits at baseline who received the intervention showed greater reduction on all drinking outcomes 12 months post-intervention. Hypertension patients who exceeded only weekly drinking limits or those exceeding both daily and weekly limits drank at similar levels as the rest of the sample post-intervention. These results suggest that brief interventions targeting alcohol use among primary care patients may not work well for all patients. For example, patients with more severe alcohol use may benefit less from brief interventions.Providers should consider individual patients’ unique demographics/behaviors when deciding to implement a brief intervention or to refer to more intensive treatment. More research is needed to corroborate these findings and test potential interventions.
For individuals and families seeking recovery: Individuals and families seeking recovery may do well to discuss substance use with their medical providers. There are a plethora of treatment options available for substance use issues. Many treatment options are also covered by Medicaid, which further increases access to care. It may also be important for those seeking substance use care to be aware of the signs/symptoms of substance use disorder.
For treatment professionals and treatment systems: Despite the limitations of the present research described, this study suggests brief interventions can be one way to change alcohol use behavior among patients. As such, it is important for providers to adopt screening, brief intervention, and referral to treatment (SBIRT) practices. It can be challenging for physicians given time constraints of office visits and/or the challenges of managing health of patients with chronic conditions. Nevertheless, resources are available for providers to implement SBIRT some of which offer continuing education credit. In addition, new technologies may help automate some SBIRT procedures.
For scientists:Scientific study of the factors which impact the effectiveness of brief interventions may enhance their overall public health impact. Presently, it is unclear precisely how brief interventions impact behavior- that is the psychological/behavioral mechanisms through which brief interventions impact behavior are unclear. In addition, it is not completely clear how individual components of brief interventions impact behavior. For example, some research in motivational interviewing suggests that strict adherence to treatment protocols is less crucial at behavioral change than displaying empathy with participants. Research is needed to better understand what the “active ingredients” of brief interventions may be and how best to utilize them so that they may be scaled, thereby reducing the public health burden of alcohol use.
For policy makers: This study adds to the literature on the effectiveness of brief interventionsin primary care settings. It may be helpful for policymakers to incentivize adoption of SBIRT practices in clinical settings. For instance, by offering compensation to clinics/centers which follow SBIRT guidelines. This could include reimbursement for time spent training clinicians/staff in SBIRT. Another option could be offering training support for clinic staff. This could come in the form of developing automated screening tools for substance use and integrating them into existing electronic health record systems. Another option could be to advertise available free training on SBIRT practices and that these courses can count towardscontinuing education credit.
Brief Interventions in primary care settings have been recommended to help address alcohol use among patients, but evidence for the efficacy of brief interventions at reducing unhealthy alcohol use and health outcomes has been mixed.
The current research examined associations between receiving a brief intervention designed to reduce alcohol use and 12-month drinking and 18-month health outcomes among adult patients with hypertension and type 2 diabetes who screened positive for unhealthy alcohol use during a primary care visit.
HOW WAS THIS STUDY CONDUCTED?
This study was a population-based observational study using electronic health records data of patients in the Kaiser Permanente Northern California healthcare system. Participants included in the analyses (N=92,621) were patients with hypertension or type 2 diabetes who had screened positive for unhealthy alcohol use at a primary care visit between 2014-2017.
Unhealthy alcohol use was defined as drinking that exceeded 7 drinks per week for women and men aged 66 and older, or >14 drinks per week for men aged 18–65. Patients were excluded from the analyses if they (1) did not have continuous Kaiser Permanente healthcare system membership in the year prior to baseline date; (2) were older than 85 years of age at baseline; or (3) did not have complete baseline alcohol screening data.
The intervention used in the current study was a physician administered brief intervention based on motivational interviewing principles. This included referrals to outpatient addiction medicine treatment. No other information about the brief intervention was provided by the authors.
The primary outcome was alcohol use behavior 12 months post-intervention. Alcohol use was measured in 4 ways: number of heavy drinking days over the past 3 months, number of drinking days per week, drinks per drinking day, and drinks per week from baseline to 12-month follow-up. These behaviors were measured via alcohol screening conducted at primary care visits. The study also examined health outcomes at 18 months post-intervention. These health measures were systolic and diastolic blood pressure and blood sugar (i.e., glycohemoglobin [HbA1c] level and ‘controlled HbA1c’ [HbA1c<8%]) at 18-month follow-up for patients with type 2 diabetes. The authors defined a clinically meaningful improvement in blood pressure to be ≥3 mm Hg reduction from baseline at 18 months. All outcomes were measured as part of routine care visits, and thus were derived from participants’ electronic health records. Because this was a naturalistic study using electronic health records only, follow-up time points were approximate (e.g., drinking measured at the 12-month follow-up was as close to 12 months post-intervention as possible).
The researchers used statistical modeling to compare drinking outcomes at 12 months and health outcomes at 18 months between patients who received the brief intervention and those who did not. The researchers used a statistical modeling technique to adjust for variables associated with receiving the brief intervention and the outcomes (drinking and health outcomes). This analytic method allowed the researchers to account for as many alternative explanations of a potential positive effect of brief intervention as possible, thereby increasing confidence that the intervention caused the positive effects on drinking and/or health outcomes.
Participants included individuals with hypertension (n=72,979) and type 2 diabetes (n=19,642). The majority were male (67.5% and 79.0% for the hypertension group and diabetes group respectively). On average, participants with hypertension were 62 years of age while the average age of participants with type 2 diabetes were60. Most participants were non-Hispanic White (70.5% and 52.8%). At baseline about 17% and 15% of participants reported drinking at levels exceeding daily and weekly limits, respectively. Approximately 5% of participants in both samples had an alcohol use disorder diagnosis. Roughly 17% and 15% of participants with hypertension and type 2 diabetes had co-occurring mental health conditions in the prior year, respectively.
WHAT DID THIS STUDY FIND?
Brief interventions reduced alcohol use only for certain subgroups.
All participants drank less alcohol 12 months post-baseline visit regardless of whether they received the brief intervention. However, for those who exceeded only daily drinking limits at baseline, the brief intervention showed greater reduced alcohol use for all 4 outcomes at 12 months. Hypertension patients who exceeded only weekly alcohol limits or those exceeding both daily and weekly alcohol limits drank at similar levels did not benefit from the brief intervention.
Figure 1. All participants drank less compared to their baseline levels regardless of receiving the brief intervention, but differences were seen in changes in drinking levels between those who received the brief intervention and those who didn’t.
Only patients with type 2 diabetes aged 30-44 drank less after receiving the brief intervention.
All other participants with type 2 diabetes had similar alcohol use reductions whether they received the brief intervention or not.
Receiving the brief intervention was associated with reduced blood pressure only among hypertensive patients.
Among patients with hypertension, those who received a brief intervention had an additional decline in blood pressure at 18 months compared with those who did not. Receiving the brief intervention was associated with a 5% greater likelihood of clinically meaningful improvement. The researchers did not observe an association between getting the brief intervention and blood pressure among patients with type 2 diabetes. There was no impact on blood sugar levels for those with diabetes.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of the study suggest that an alcohol-focused brief intervention delivered in a primary care setting can impact alcohol use and chronic health conditions among specific types of patients with chronic health conditions.
The researchers found that all participants drank less alcohol 12 months post-baseline visit regardless of if they received the brief intervention or not. Participants with hypertension whose drinking exceeded daily drinking limits at baseline had greater reductions than other groups after receiving the intervention. Hypertension patients who exceeded only weekly limits or those exceeding both daily and weekly limits drank at similar levels as the rest of the sample post-intervention. Similarly, only patients with type 2 diabetes aged 30-44 showed more reductions in alcohol use 1-year post intervention. All other patients with type 2 diabetes showed similar reductions in drinking.
This pattern of results may suggest that the impact of brief interventions varies depending on patients’ characteristics. For example, the finding that only participants whose drinking exceeded daily drinking (but not weekly) limits at baseline drank less after receiving the intervention may suggest that regular heavier drinkers may be more open to the advice and feedback presented during brief interventions. Similarly, the fact that patients with type 2 diabetes saw no changes in alcohol use post intervention suggest that factors like type of chronic disease, disease severity, medication intensity and patient adherence to medications and lifestyle changes may play a role in brief interventions effectiveness. These findings suggest that different approaches, including tailoring to population subgroups or health conditions, may be needed to address unhealthy drinking and related health outcomes among patients with chronic conditions.
It is unclear based on the data presented if the sample included patients with both hypertension and type 2 diabetes. If the sample included patients with both conditions, it is possible that some participants were included in both groups and thus impacted the results. If the researchers only included patients with either hypertension or type 2 diabetes (but not those with both conditions) then the generalizability of the results was likely impacted. There is a high degree of comorbidity between these conditions, therefore excluding patients with both does not reflect how the real-world population may respond to the brief intervention. It is possible the management of these conditions simultaneously could impact the intervention’s effectiveness.
The nature of the brief intervention is unclear based on thedescription in text. The authors describe the brief intervention as being an intervention provided by physicians that was “based on motivational interviewing principles.”It is not apparent what the content of the intervention was, nor how well providers administered it. It is unknown what (if any) fidelity protocols were put in place to ensure providers were adequately administering this treatment. Poor adherence to intervention protocols has been associated with lackluster outcomes post-intervention. This makes it unclear how much the observed changes in behavior can be attributable to the brief intervention.
It is unclear if the changes in health outcomes observed at 18 months were the result of the brief intervention. The researchers did not present data on alcohol use at 18-months,so it is unknown if changes in drinking were maintained over time. Furthermore, the sample was entirely comprised of patients who were already in long term care which may have impacted the observed changes in health outcomes (e.g., being prescribed blood pressure medication). Additionally, while the analyses accounted for many clinical and medical factors at baseline that would impact health outcomes over time, it is unclear if the researchers adjusted for time-varying factors which also impact these outcomes (e.g., cigarette smoking cessation, weight loss, etc.).
BOTTOM LINE
Results of this research suggest that a physician administered brief intervention can impact alcohol use and health outcomes among certain types of patients with chronic health conditions. The benefits of the brief intervention to address unhealthy alcohol use for individuals with hypertension and type 2 diabetes varied depending upon individual patient characteristics. Patients with type 2 diabetes aged 30-44 drank less after receiving the brief intervention, whereas all other participants with type 2 diabetes did not drink less alcohol 12 months post–intervention. Participants with hypertension who reported exceeding only daily drinking limits at baseline who received the intervention showed greater reduction on all drinking outcomes 12 months post-intervention. Hypertension patients who exceeded only weekly drinking limits or those exceeding both daily and weekly limits drank at similar levels as the rest of the sample post-intervention. These results suggest that brief interventions targeting alcohol use among primary care patients may not work well for all patients. For example, patients with more severe alcohol use may benefit less from brief interventions.Providers should consider individual patients’ unique demographics/behaviors when deciding to implement a brief intervention or to refer to more intensive treatment. More research is needed to corroborate these findings and test potential interventions.
For individuals and families seeking recovery: Individuals and families seeking recovery may do well to discuss substance use with their medical providers. There are a plethora of treatment options available for substance use issues. Many treatment options are also covered by Medicaid, which further increases access to care. It may also be important for those seeking substance use care to be aware of the signs/symptoms of substance use disorder.
For treatment professionals and treatment systems: Despite the limitations of the present research described, this study suggests brief interventions can be one way to change alcohol use behavior among patients. As such, it is important for providers to adopt screening, brief intervention, and referral to treatment (SBIRT) practices. It can be challenging for physicians given time constraints of office visits and/or the challenges of managing health of patients with chronic conditions. Nevertheless, resources are available for providers to implement SBIRT some of which offer continuing education credit. In addition, new technologies may help automate some SBIRT procedures.
For scientists:Scientific study of the factors which impact the effectiveness of brief interventions may enhance their overall public health impact. Presently, it is unclear precisely how brief interventions impact behavior- that is the psychological/behavioral mechanisms through which brief interventions impact behavior are unclear. In addition, it is not completely clear how individual components of brief interventions impact behavior. For example, some research in motivational interviewing suggests that strict adherence to treatment protocols is less crucial at behavioral change than displaying empathy with participants. Research is needed to better understand what the “active ingredients” of brief interventions may be and how best to utilize them so that they may be scaled, thereby reducing the public health burden of alcohol use.
For policy makers: This study adds to the literature on the effectiveness of brief interventionsin primary care settings. It may be helpful for policymakers to incentivize adoption of SBIRT practices in clinical settings. For instance, by offering compensation to clinics/centers which follow SBIRT guidelines. This could include reimbursement for time spent training clinicians/staff in SBIRT. Another option could be offering training support for clinic staff. This could come in the form of developing automated screening tools for substance use and integrating them into existing electronic health record systems. Another option could be to advertise available free training on SBIRT practices and that these courses can count towardscontinuing education credit.