Can a brief online intervention curb problematic alcohol use in the National Guard?
Brief interventions have been shown to help military personnel reduce or quit drinking but, reservists, who usually live off-base, need innovative ways of accessing these kinds of supports. This study tested a brief, online drinking intervention specifically tailored to US military reservists.
On average, US military service members consume significantly more alcohol than their civilian counterparts and experience more alcohol-related problems. This has led to efforts by the US military to address hazardous and binge drinking among military personnel. However, military reservists, such as those in the National Guard, often have difficulty accessing these kinds of services because they typically live in the community and are only on-base a few days a month.
Screening, Brief Intervention, Referral to Treatment (best known by the acronym “SBIRT” and pronounced “ess-bert”) has been shown to reduce problematic alcohol use in civilian populations. SBIRT, which was first developed by the US Substance Abuse and Mental Health Services Administration (SAMHSA) for deployment in primary care medical settings, is a protocol for, 1) identifying risky patterns of patient substance use, 2) engaging patients in a conversation about their substance use with the goal of increasing their motivation to reduce or stop using substances and seek treatment, and 3) providing referral to substance use related treatment for patients deemed to have, or be at risk for having a substance use disorder.
In this study, researchers adapted the SBIRT intervention, developing a 1-hour online course with booster sessions designed to address problematic alcohol use among US National Guard members endorsing hazardous alcohol use and/or recent binge drinking. Their intervention included a brief, 40-minute online session delivered by an avatar, and 3 subsequent booster sessions delivered online or by peers. Unlike traditional SBIRT, however, their intervention did not include referrals to treatment.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized controlled trial with 739 Michigan Army National Guard members who were assigned to one of three groups including, 1) a brief SBIRT-based intervention + three web-based booster sessions, 2) a brief SBIRT-based intervention + three peer-delivered booster sessions, or 3) usual care only in which participants received a standard pamphlet tailored to National Guard members including basic information on alcohol use and misuse of prescription drugs, as well as smoking and military-specific resources for help with these problems. The researchers compared the two brief intervention groups to usual care only, but not to one-another.
All Michigan National Guard members attending training camps between April 2015 and April 2017 were invited to participate in the study, however, to be eligible, volunteers had to have an Alcohol Use Disorders Identification Test (AUDIT-C) score of 5 or more for men, and 4 or more for women, indicating that they met criteria for at-risk drinking/hazardous alcohol use.
The study’s brief intervention consisted of a single, 30-40-minute, virtual session with a personally selected military or non-military avatar therapist who guided the participant through their ‘mission’ to navigate the program. The intervention was tailored for each participant by gender, deployment history, and baseline drinking pattern. Throughout the course of this mission, participants received personalized feedback regarding their substance use and risk factors, as well as their goals and strengths. Participants also completed a decisional balance exercise designed to increase motivation to change, which sought to develop discrepancy between their alcohol use and the ability to meet their goals. Participants’ readiness to change was also assessed and they were provided with strategies for change.
The brief intervention was also accompanied by three online or peer-led booster sessions:
The online booster sessions were also structured like a mission, with participants navigating points on a map, each of which required a task to be completed. Topics covered reasons for hazardous alcohol use, social factors, finances, mood, and physical fitness, and driving under the influence. In addition, calculators for determining the caloric count of drinking, approximate money spent on drinking, and estimated blood alcohol level associated with the amount of drinking were included. These booster sessions also included peer messages and testimonials that were tailored to the participant based on their misuse of alcohol and/or prescription opioids and on their deployment history.
The peer-delivered booster sessions were conducted in-person or over the phone based on participant choice (90% delivered by phone), with each lasting 15-20 minutes. During the first booster session, peers shared the purpose of the session and asked the participant to share about how they had experienced the brief intervention. Participant survey data was not shared with the peers, and peers did not directly ask participants about their alcohol use. Instead, the meetings included a discussion of how health-related behaviors can affect an individual, choices an individual can make, and potential next steps the participant could take to change their behaviors to align with their goals. Additional topics discussed at each peer-delivered booster session were the same as those included in the online booster sessions.
Participants were assessed at study baseline, and again at 4-, 8-, and 12-months following study enrollment. The main study outcome was number of binge drinking episodes in the past 30 days, measured at 12-month follow-up. Binge drinking was defined as consuming 5 or more drinks in a single occasion if male, and 4 or more drinks if female.
Secondary outcome measures at 12-month follow-up included amount of alcohol consumed in the past 30 days (quantity drinks × frequency of drinking), and the total Alcohol Use Disorders Identification and Short Inventory of Problems test scores.
The Alcohol Use Disorders Identification Test assesses quantity of alcohol use, as well as the frequency and binge drinking. It also assesses risk factors for hazardous alcohol use. The Short Inventory of Problems measures interpersonal, intrapersonal, physical, impulse control, and social consequences of alcohol use. Both measures asked participants to report on their experiences over the past three months.
On average, participants were 28 years old; 84% were male and 16% were female. Racially, 83% identified as White, 10% as Black, and 7% as Other/Multi-Racial. Ethnically, 12% of the sample identified as Hispanic. Over 92% of people enrolled in the study completed the initial brief intervention. Booster completion rates were higher in the brief intervention + peer booster sessions group, ranging from 69% to 58%, compared to a range of 57% to 49% for the brief intervention + online booster sessions group. Across groups and follow-up sessions, follow-up response rates for outcome measures ranged from 71% to 86%, with the usual care groups having better follow-up response rates overall.
WHAT DID THIS STUDY FIND?
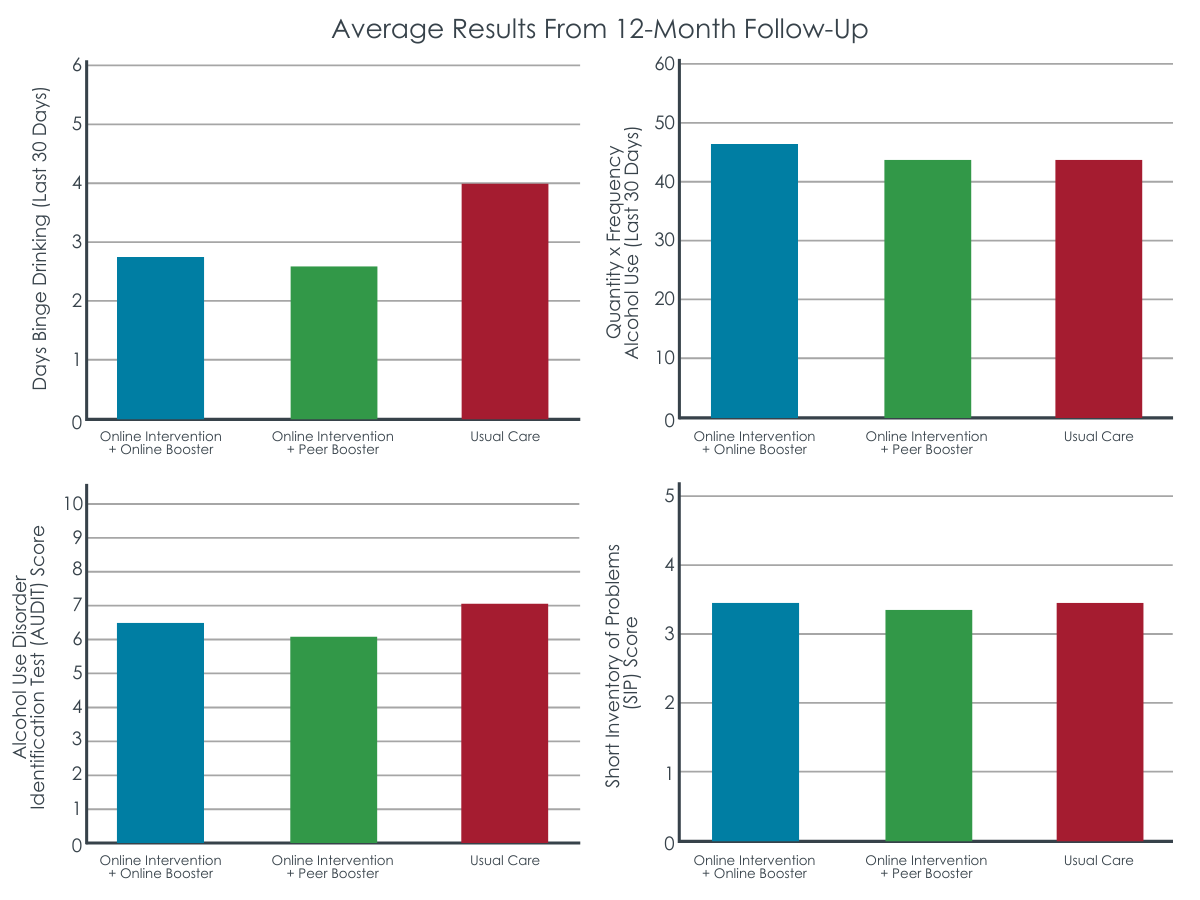
Brief intervention groups experienced reduced binge drinking, but not overall drinking at 12-month follow-up.
Both the brief intervention + online booster, and brief intervention + peer-delivered booster groups had fewer binge drinking days in the past 30 days at 12-month follow-up in comparison to the usual care group after statistically controlling for baseline binge drinking frequency and gender. Notably, similar advantages for the brief intervention groups on binge drinking were also observed at 4- and 8-month follow-up.
Though the researchers did not statistically test for differences between the brief intervention + online booster, and brief intervention + peer-delivered booster groups, based on the raw scores, there did not appear to be any meaningful differences between these groups in terms of binge drinking at any of the follow-up time-points.
Though participants in the brief online intervention groups had less binge drinking at 12-month follow-up, after controlling for baseline drinking and gender, groups were not found to be markedly different in terms of past- 30-day alcohol consumption (i.e., quantity × frequency) at this follow-up.
Peer connection may help reduce consequences.
At 12-month follow-up, after controlling for baseline scores and gender, both brief intervention groups had less alcohol problem severity as measured by the Alcohol Use Disorders Identification Test, compared to the usual care group. In terms of Short Inventory of Problems scores, however, at 12-month follow-up only the brief intervention + peer-delivered booster group had lower scores than the usual care group.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Interventions for hazardous and binge drinking are much needed in the US military and work is ongoing to develop tailored treatments for military service people and their families. Developing and implementing more accessible drinking interventions for military reservists involves additional challenges because reservists usually don’t live on or near military bases where services are typically offered.
Digital therapeutic support services like the brief intervention tested in this study are potentially useful because they increase access to resources that can support efforts to reduce or quit alcohol use. Additionally, such online interventions potentially surmount other major barriers to treatment engagement including stigma associated with seeking help, which is particularly prevalent in the military.
This study provides preliminary evidence supporting this brief, online intervention with booster sessions for problem drinking in military reservists. Notably, those receiving this intervention were doing better at 12-month follow-up relative to controls who received an online educational pamphlet in terms of number of past-month binge drinking days and alcohol use disorder related problems. And notably, those in the brief intervention + peer-delivered booster group had less alcohol problem severity at 12-month follow-up compared to controls, suggesting an additional benefit conferred by peer support.
At the same time, similar to findings for SBIRT in civilian populations, between group differences were not large in absolute terms. For instance, the active treatment and control groups only differed in number of past-30-day binge drinking days by a little over 1 day. Further, Alcohol Use Disorder Identification Test scores only differed by around 1 point; given scores on this measure can range from 0-40, this might not represent a clinically meaningful effect. Also, groups were not different in terms of overall amount alcohol consumed at 12-month follow-up. That said, reducing the more consequential higher intoxication levels associated with binge drinking by one day at a population level could substantially reduce alcohol related incidents and accidents which are more common at these more intensive alcohol exposure levels.
Furthermore, though the absolute observed between group differences were small, these findings are nevertheless promising given this kind of intervention could be delivered to many people who might otherwise not get help for problematic drinking, and at relatively low cost. Additionally, the benefits of brief drinking interventions are short-lived, but in this study, improvements in binge drinking were observed approximately nine months after participants in the online intervention groups received their final booster session. This sustained benefit may be in part explained by the booster sessions, which distinguished this brief intervention from others like it that typically don’t involve this kind of sustained support. With more research and additional modifications, it’s quite possible this intervention could have larger effects.
Though statistically significant differences were found between the experimental groups and the control group in this study at 12-month follow-up, in absolute terms these differences were not large. That said, reducing the more consequential higher intoxication levels associated with binge drinking by one day at a population level could substantially reduce alcohol related incidents and accidents which are more common at these more intensive alcohol exposure levels.
This preliminary study focused on testing differences between participants receiving a brief online drinking intervention with either web-based or peer-delivered booster sessions, and usual care. The researchers did not explore differences between the online intervention groups receiving online boosters and peer-delivered boosters. Future studies will ideally explore how online versus peer-delivered booster sessions might produce different outcomes.
Not necessarily a limitation per se, but the booster sessions in this study included a significant amount of new material. In this way, these additional sessions could be thought of as additional intervention sessions that complemented the brief online intervention, rather conventional booster sessions in which previously learnt material is reiterated and reinforced. It might be more accurate to reframe future iterations of this intervention accordingly.
Study participants received financial compensation for completing booster sessions. It is not clear whether booster session compliance would be the same under real-world conditions.
BOTTOM LINE
Brief, online interventions like the one tested in this study show promise for addressing problem alcohol use in the military. Although differences in overall drinking were not found, this intervention was notable for its sustained impact on binge drinking and alcohol related problems over the 12-month study period. Results further support the potential for brief, online interventions for military personnel, while also highlighting the possible importance of ongoing check-ins and skills training to address drinking problems in this population. It will be important for future studies to explore the unique benefits and costs conferred by these additional sessions, to see how they may boost the effects of such brief online interventions.
For individuals and families seeking recovery: Brief online interventions for hazardous and binge drinking have shown the potential to improve alcohol use outcomes in a variety of populations including members of the military and college students, among others. At the same time, individuals with more severe alcohol use problems, such as those with alcohol use disorder, will likely needadditional support beyond this kind of brief intervention.
For treatment professionals and treatment systems: Brief interventions like SBIRT, as well as online interventions for hazardous and binge drinking are increasingly being utilized in a range of settings and can be important early interventions that can increase the reach of these helpful services and alter drinking problem trajectories at low cost to individuals and systems.
For scientists: Brief online interventions for hazardous and binge drinking are increasingly being tested and utilized in a range of settings, and because of their accessibility, scalability, and cost effectiveness have tremendous potential to positively impact public health at the population level. At the same time, more work is needed to determine for whom and under what conditions these interventions are most helpful, and how they might be best delivered. Subsequent studies extending the present work reviewed here should compare active treatment groups and tease out how additional sessions or check-ups can potentially complement single-session interventions.
For policy makers: Brief online interventions for hazardous and binge drinking are increasingly being tested and utilized in a range of settings, and because of their accessibility, scalability, and cost effectiveness have tremendous potential to positively impact public health. Though such interventions cost money to develop, when effective, they ultimately represent good value for money because of the future cost savings they produce by changing problem drinking trajectories and helping engage people in treatment sooner.
On average, US military service members consume significantly more alcohol than their civilian counterparts and experience more alcohol-related problems. This has led to efforts by the US military to address hazardous and binge drinking among military personnel. However, military reservists, such as those in the National Guard, often have difficulty accessing these kinds of services because they typically live in the community and are only on-base a few days a month.
Screening, Brief Intervention, Referral to Treatment (best known by the acronym “SBIRT” and pronounced “ess-bert”) has been shown to reduce problematic alcohol use in civilian populations. SBIRT, which was first developed by the US Substance Abuse and Mental Health Services Administration (SAMHSA) for deployment in primary care medical settings, is a protocol for, 1) identifying risky patterns of patient substance use, 2) engaging patients in a conversation about their substance use with the goal of increasing their motivation to reduce or stop using substances and seek treatment, and 3) providing referral to substance use related treatment for patients deemed to have, or be at risk for having a substance use disorder.
In this study, researchers adapted the SBIRT intervention, developing a 1-hour online course with booster sessions designed to address problematic alcohol use among US National Guard members endorsing hazardous alcohol use and/or recent binge drinking. Their intervention included a brief, 40-minute online session delivered by an avatar, and 3 subsequent booster sessions delivered online or by peers. Unlike traditional SBIRT, however, their intervention did not include referrals to treatment.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized controlled trial with 739 Michigan Army National Guard members who were assigned to one of three groups including, 1) a brief SBIRT-based intervention + three web-based booster sessions, 2) a brief SBIRT-based intervention + three peer-delivered booster sessions, or 3) usual care only in which participants received a standard pamphlet tailored to National Guard members including basic information on alcohol use and misuse of prescription drugs, as well as smoking and military-specific resources for help with these problems. The researchers compared the two brief intervention groups to usual care only, but not to one-another.
All Michigan National Guard members attending training camps between April 2015 and April 2017 were invited to participate in the study, however, to be eligible, volunteers had to have an Alcohol Use Disorders Identification Test (AUDIT-C) score of 5 or more for men, and 4 or more for women, indicating that they met criteria for at-risk drinking/hazardous alcohol use.
The study’s brief intervention consisted of a single, 30-40-minute, virtual session with a personally selected military or non-military avatar therapist who guided the participant through their ‘mission’ to navigate the program. The intervention was tailored for each participant by gender, deployment history, and baseline drinking pattern. Throughout the course of this mission, participants received personalized feedback regarding their substance use and risk factors, as well as their goals and strengths. Participants also completed a decisional balance exercise designed to increase motivation to change, which sought to develop discrepancy between their alcohol use and the ability to meet their goals. Participants’ readiness to change was also assessed and they were provided with strategies for change.
The brief intervention was also accompanied by three online or peer-led booster sessions:
The online booster sessions were also structured like a mission, with participants navigating points on a map, each of which required a task to be completed. Topics covered reasons for hazardous alcohol use, social factors, finances, mood, and physical fitness, and driving under the influence. In addition, calculators for determining the caloric count of drinking, approximate money spent on drinking, and estimated blood alcohol level associated with the amount of drinking were included. These booster sessions also included peer messages and testimonials that were tailored to the participant based on their misuse of alcohol and/or prescription opioids and on their deployment history.
The peer-delivered booster sessions were conducted in-person or over the phone based on participant choice (90% delivered by phone), with each lasting 15-20 minutes. During the first booster session, peers shared the purpose of the session and asked the participant to share about how they had experienced the brief intervention. Participant survey data was not shared with the peers, and peers did not directly ask participants about their alcohol use. Instead, the meetings included a discussion of how health-related behaviors can affect an individual, choices an individual can make, and potential next steps the participant could take to change their behaviors to align with their goals. Additional topics discussed at each peer-delivered booster session were the same as those included in the online booster sessions.
Participants were assessed at study baseline, and again at 4-, 8-, and 12-months following study enrollment. The main study outcome was number of binge drinking episodes in the past 30 days, measured at 12-month follow-up. Binge drinking was defined as consuming 5 or more drinks in a single occasion if male, and 4 or more drinks if female.
Secondary outcome measures at 12-month follow-up included amount of alcohol consumed in the past 30 days (quantity drinks × frequency of drinking), and the total Alcohol Use Disorders Identification and Short Inventory of Problems test scores.
The Alcohol Use Disorders Identification Test assesses quantity of alcohol use, as well as the frequency and binge drinking. It also assesses risk factors for hazardous alcohol use. The Short Inventory of Problems measures interpersonal, intrapersonal, physical, impulse control, and social consequences of alcohol use. Both measures asked participants to report on their experiences over the past three months.
On average, participants were 28 years old; 84% were male and 16% were female. Racially, 83% identified as White, 10% as Black, and 7% as Other/Multi-Racial. Ethnically, 12% of the sample identified as Hispanic. Over 92% of people enrolled in the study completed the initial brief intervention. Booster completion rates were higher in the brief intervention + peer booster sessions group, ranging from 69% to 58%, compared to a range of 57% to 49% for the brief intervention + online booster sessions group. Across groups and follow-up sessions, follow-up response rates for outcome measures ranged from 71% to 86%, with the usual care groups having better follow-up response rates overall.
WHAT DID THIS STUDY FIND?
Brief intervention groups experienced reduced binge drinking, but not overall drinking at 12-month follow-up.
Both the brief intervention + online booster, and brief intervention + peer-delivered booster groups had fewer binge drinking days in the past 30 days at 12-month follow-up in comparison to the usual care group after statistically controlling for baseline binge drinking frequency and gender. Notably, similar advantages for the brief intervention groups on binge drinking were also observed at 4- and 8-month follow-up.
Though the researchers did not statistically test for differences between the brief intervention + online booster, and brief intervention + peer-delivered booster groups, based on the raw scores, there did not appear to be any meaningful differences between these groups in terms of binge drinking at any of the follow-up time-points.
Though participants in the brief online intervention groups had less binge drinking at 12-month follow-up, after controlling for baseline drinking and gender, groups were not found to be markedly different in terms of past- 30-day alcohol consumption (i.e., quantity × frequency) at this follow-up.
Peer connection may help reduce consequences.
At 12-month follow-up, after controlling for baseline scores and gender, both brief intervention groups had less alcohol problem severity as measured by the Alcohol Use Disorders Identification Test, compared to the usual care group. In terms of Short Inventory of Problems scores, however, at 12-month follow-up only the brief intervention + peer-delivered booster group had lower scores than the usual care group.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Interventions for hazardous and binge drinking are much needed in the US military and work is ongoing to develop tailored treatments for military service people and their families. Developing and implementing more accessible drinking interventions for military reservists involves additional challenges because reservists usually don’t live on or near military bases where services are typically offered.
Digital therapeutic support services like the brief intervention tested in this study are potentially useful because they increase access to resources that can support efforts to reduce or quit alcohol use. Additionally, such online interventions potentially surmount other major barriers to treatment engagement including stigma associated with seeking help, which is particularly prevalent in the military.
This study provides preliminary evidence supporting this brief, online intervention with booster sessions for problem drinking in military reservists. Notably, those receiving this intervention were doing better at 12-month follow-up relative to controls who received an online educational pamphlet in terms of number of past-month binge drinking days and alcohol use disorder related problems. And notably, those in the brief intervention + peer-delivered booster group had less alcohol problem severity at 12-month follow-up compared to controls, suggesting an additional benefit conferred by peer support.
At the same time, similar to findings for SBIRT in civilian populations, between group differences were not large in absolute terms. For instance, the active treatment and control groups only differed in number of past-30-day binge drinking days by a little over 1 day. Further, Alcohol Use Disorder Identification Test scores only differed by around 1 point; given scores on this measure can range from 0-40, this might not represent a clinically meaningful effect. Also, groups were not different in terms of overall amount alcohol consumed at 12-month follow-up. That said, reducing the more consequential higher intoxication levels associated with binge drinking by one day at a population level could substantially reduce alcohol related incidents and accidents which are more common at these more intensive alcohol exposure levels.
Furthermore, though the absolute observed between group differences were small, these findings are nevertheless promising given this kind of intervention could be delivered to many people who might otherwise not get help for problematic drinking, and at relatively low cost. Additionally, the benefits of brief drinking interventions are short-lived, but in this study, improvements in binge drinking were observed approximately nine months after participants in the online intervention groups received their final booster session. This sustained benefit may be in part explained by the booster sessions, which distinguished this brief intervention from others like it that typically don’t involve this kind of sustained support. With more research and additional modifications, it’s quite possible this intervention could have larger effects.
Though statistically significant differences were found between the experimental groups and the control group in this study at 12-month follow-up, in absolute terms these differences were not large. That said, reducing the more consequential higher intoxication levels associated with binge drinking by one day at a population level could substantially reduce alcohol related incidents and accidents which are more common at these more intensive alcohol exposure levels.
This preliminary study focused on testing differences between participants receiving a brief online drinking intervention with either web-based or peer-delivered booster sessions, and usual care. The researchers did not explore differences between the online intervention groups receiving online boosters and peer-delivered boosters. Future studies will ideally explore how online versus peer-delivered booster sessions might produce different outcomes.
Not necessarily a limitation per se, but the booster sessions in this study included a significant amount of new material. In this way, these additional sessions could be thought of as additional intervention sessions that complemented the brief online intervention, rather conventional booster sessions in which previously learnt material is reiterated and reinforced. It might be more accurate to reframe future iterations of this intervention accordingly.
Study participants received financial compensation for completing booster sessions. It is not clear whether booster session compliance would be the same under real-world conditions.
BOTTOM LINE
Brief, online interventions like the one tested in this study show promise for addressing problem alcohol use in the military. Although differences in overall drinking were not found, this intervention was notable for its sustained impact on binge drinking and alcohol related problems over the 12-month study period. Results further support the potential for brief, online interventions for military personnel, while also highlighting the possible importance of ongoing check-ins and skills training to address drinking problems in this population. It will be important for future studies to explore the unique benefits and costs conferred by these additional sessions, to see how they may boost the effects of such brief online interventions.
For individuals and families seeking recovery: Brief online interventions for hazardous and binge drinking have shown the potential to improve alcohol use outcomes in a variety of populations including members of the military and college students, among others. At the same time, individuals with more severe alcohol use problems, such as those with alcohol use disorder, will likely needadditional support beyond this kind of brief intervention.
For treatment professionals and treatment systems: Brief interventions like SBIRT, as well as online interventions for hazardous and binge drinking are increasingly being utilized in a range of settings and can be important early interventions that can increase the reach of these helpful services and alter drinking problem trajectories at low cost to individuals and systems.
For scientists: Brief online interventions for hazardous and binge drinking are increasingly being tested and utilized in a range of settings, and because of their accessibility, scalability, and cost effectiveness have tremendous potential to positively impact public health at the population level. At the same time, more work is needed to determine for whom and under what conditions these interventions are most helpful, and how they might be best delivered. Subsequent studies extending the present work reviewed here should compare active treatment groups and tease out how additional sessions or check-ups can potentially complement single-session interventions.
For policy makers: Brief online interventions for hazardous and binge drinking are increasingly being tested and utilized in a range of settings, and because of their accessibility, scalability, and cost effectiveness have tremendous potential to positively impact public health. Though such interventions cost money to develop, when effective, they ultimately represent good value for money because of the future cost savings they produce by changing problem drinking trajectories and helping engage people in treatment sooner.
On average, US military service members consume significantly more alcohol than their civilian counterparts and experience more alcohol-related problems. This has led to efforts by the US military to address hazardous and binge drinking among military personnel. However, military reservists, such as those in the National Guard, often have difficulty accessing these kinds of services because they typically live in the community and are only on-base a few days a month.
Screening, Brief Intervention, Referral to Treatment (best known by the acronym “SBIRT” and pronounced “ess-bert”) has been shown to reduce problematic alcohol use in civilian populations. SBIRT, which was first developed by the US Substance Abuse and Mental Health Services Administration (SAMHSA) for deployment in primary care medical settings, is a protocol for, 1) identifying risky patterns of patient substance use, 2) engaging patients in a conversation about their substance use with the goal of increasing their motivation to reduce or stop using substances and seek treatment, and 3) providing referral to substance use related treatment for patients deemed to have, or be at risk for having a substance use disorder.
In this study, researchers adapted the SBIRT intervention, developing a 1-hour online course with booster sessions designed to address problematic alcohol use among US National Guard members endorsing hazardous alcohol use and/or recent binge drinking. Their intervention included a brief, 40-minute online session delivered by an avatar, and 3 subsequent booster sessions delivered online or by peers. Unlike traditional SBIRT, however, their intervention did not include referrals to treatment.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized controlled trial with 739 Michigan Army National Guard members who were assigned to one of three groups including, 1) a brief SBIRT-based intervention + three web-based booster sessions, 2) a brief SBIRT-based intervention + three peer-delivered booster sessions, or 3) usual care only in which participants received a standard pamphlet tailored to National Guard members including basic information on alcohol use and misuse of prescription drugs, as well as smoking and military-specific resources for help with these problems. The researchers compared the two brief intervention groups to usual care only, but not to one-another.
All Michigan National Guard members attending training camps between April 2015 and April 2017 were invited to participate in the study, however, to be eligible, volunteers had to have an Alcohol Use Disorders Identification Test (AUDIT-C) score of 5 or more for men, and 4 or more for women, indicating that they met criteria for at-risk drinking/hazardous alcohol use.
The study’s brief intervention consisted of a single, 30-40-minute, virtual session with a personally selected military or non-military avatar therapist who guided the participant through their ‘mission’ to navigate the program. The intervention was tailored for each participant by gender, deployment history, and baseline drinking pattern. Throughout the course of this mission, participants received personalized feedback regarding their substance use and risk factors, as well as their goals and strengths. Participants also completed a decisional balance exercise designed to increase motivation to change, which sought to develop discrepancy between their alcohol use and the ability to meet their goals. Participants’ readiness to change was also assessed and they were provided with strategies for change.
The brief intervention was also accompanied by three online or peer-led booster sessions:
The online booster sessions were also structured like a mission, with participants navigating points on a map, each of which required a task to be completed. Topics covered reasons for hazardous alcohol use, social factors, finances, mood, and physical fitness, and driving under the influence. In addition, calculators for determining the caloric count of drinking, approximate money spent on drinking, and estimated blood alcohol level associated with the amount of drinking were included. These booster sessions also included peer messages and testimonials that were tailored to the participant based on their misuse of alcohol and/or prescription opioids and on their deployment history.
The peer-delivered booster sessions were conducted in-person or over the phone based on participant choice (90% delivered by phone), with each lasting 15-20 minutes. During the first booster session, peers shared the purpose of the session and asked the participant to share about how they had experienced the brief intervention. Participant survey data was not shared with the peers, and peers did not directly ask participants about their alcohol use. Instead, the meetings included a discussion of how health-related behaviors can affect an individual, choices an individual can make, and potential next steps the participant could take to change their behaviors to align with their goals. Additional topics discussed at each peer-delivered booster session were the same as those included in the online booster sessions.
Participants were assessed at study baseline, and again at 4-, 8-, and 12-months following study enrollment. The main study outcome was number of binge drinking episodes in the past 30 days, measured at 12-month follow-up. Binge drinking was defined as consuming 5 or more drinks in a single occasion if male, and 4 or more drinks if female.
Secondary outcome measures at 12-month follow-up included amount of alcohol consumed in the past 30 days (quantity drinks × frequency of drinking), and the total Alcohol Use Disorders Identification and Short Inventory of Problems test scores.
The Alcohol Use Disorders Identification Test assesses quantity of alcohol use, as well as the frequency and binge drinking. It also assesses risk factors for hazardous alcohol use. The Short Inventory of Problems measures interpersonal, intrapersonal, physical, impulse control, and social consequences of alcohol use. Both measures asked participants to report on their experiences over the past three months.
On average, participants were 28 years old; 84% were male and 16% were female. Racially, 83% identified as White, 10% as Black, and 7% as Other/Multi-Racial. Ethnically, 12% of the sample identified as Hispanic. Over 92% of people enrolled in the study completed the initial brief intervention. Booster completion rates were higher in the brief intervention + peer booster sessions group, ranging from 69% to 58%, compared to a range of 57% to 49% for the brief intervention + online booster sessions group. Across groups and follow-up sessions, follow-up response rates for outcome measures ranged from 71% to 86%, with the usual care groups having better follow-up response rates overall.
WHAT DID THIS STUDY FIND?
Brief intervention groups experienced reduced binge drinking, but not overall drinking at 12-month follow-up.
Both the brief intervention + online booster, and brief intervention + peer-delivered booster groups had fewer binge drinking days in the past 30 days at 12-month follow-up in comparison to the usual care group after statistically controlling for baseline binge drinking frequency and gender. Notably, similar advantages for the brief intervention groups on binge drinking were also observed at 4- and 8-month follow-up.
Though the researchers did not statistically test for differences between the brief intervention + online booster, and brief intervention + peer-delivered booster groups, based on the raw scores, there did not appear to be any meaningful differences between these groups in terms of binge drinking at any of the follow-up time-points.
Though participants in the brief online intervention groups had less binge drinking at 12-month follow-up, after controlling for baseline drinking and gender, groups were not found to be markedly different in terms of past- 30-day alcohol consumption (i.e., quantity × frequency) at this follow-up.
Peer connection may help reduce consequences.
At 12-month follow-up, after controlling for baseline scores and gender, both brief intervention groups had less alcohol problem severity as measured by the Alcohol Use Disorders Identification Test, compared to the usual care group. In terms of Short Inventory of Problems scores, however, at 12-month follow-up only the brief intervention + peer-delivered booster group had lower scores than the usual care group.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Interventions for hazardous and binge drinking are much needed in the US military and work is ongoing to develop tailored treatments for military service people and their families. Developing and implementing more accessible drinking interventions for military reservists involves additional challenges because reservists usually don’t live on or near military bases where services are typically offered.
Digital therapeutic support services like the brief intervention tested in this study are potentially useful because they increase access to resources that can support efforts to reduce or quit alcohol use. Additionally, such online interventions potentially surmount other major barriers to treatment engagement including stigma associated with seeking help, which is particularly prevalent in the military.
This study provides preliminary evidence supporting this brief, online intervention with booster sessions for problem drinking in military reservists. Notably, those receiving this intervention were doing better at 12-month follow-up relative to controls who received an online educational pamphlet in terms of number of past-month binge drinking days and alcohol use disorder related problems. And notably, those in the brief intervention + peer-delivered booster group had less alcohol problem severity at 12-month follow-up compared to controls, suggesting an additional benefit conferred by peer support.
At the same time, similar to findings for SBIRT in civilian populations, between group differences were not large in absolute terms. For instance, the active treatment and control groups only differed in number of past-30-day binge drinking days by a little over 1 day. Further, Alcohol Use Disorder Identification Test scores only differed by around 1 point; given scores on this measure can range from 0-40, this might not represent a clinically meaningful effect. Also, groups were not different in terms of overall amount alcohol consumed at 12-month follow-up. That said, reducing the more consequential higher intoxication levels associated with binge drinking by one day at a population level could substantially reduce alcohol related incidents and accidents which are more common at these more intensive alcohol exposure levels.
Furthermore, though the absolute observed between group differences were small, these findings are nevertheless promising given this kind of intervention could be delivered to many people who might otherwise not get help for problematic drinking, and at relatively low cost. Additionally, the benefits of brief drinking interventions are short-lived, but in this study, improvements in binge drinking were observed approximately nine months after participants in the online intervention groups received their final booster session. This sustained benefit may be in part explained by the booster sessions, which distinguished this brief intervention from others like it that typically don’t involve this kind of sustained support. With more research and additional modifications, it’s quite possible this intervention could have larger effects.
Though statistically significant differences were found between the experimental groups and the control group in this study at 12-month follow-up, in absolute terms these differences were not large. That said, reducing the more consequential higher intoxication levels associated with binge drinking by one day at a population level could substantially reduce alcohol related incidents and accidents which are more common at these more intensive alcohol exposure levels.
This preliminary study focused on testing differences between participants receiving a brief online drinking intervention with either web-based or peer-delivered booster sessions, and usual care. The researchers did not explore differences between the online intervention groups receiving online boosters and peer-delivered boosters. Future studies will ideally explore how online versus peer-delivered booster sessions might produce different outcomes.
Not necessarily a limitation per se, but the booster sessions in this study included a significant amount of new material. In this way, these additional sessions could be thought of as additional intervention sessions that complemented the brief online intervention, rather conventional booster sessions in which previously learnt material is reiterated and reinforced. It might be more accurate to reframe future iterations of this intervention accordingly.
Study participants received financial compensation for completing booster sessions. It is not clear whether booster session compliance would be the same under real-world conditions.
BOTTOM LINE
Brief, online interventions like the one tested in this study show promise for addressing problem alcohol use in the military. Although differences in overall drinking were not found, this intervention was notable for its sustained impact on binge drinking and alcohol related problems over the 12-month study period. Results further support the potential for brief, online interventions for military personnel, while also highlighting the possible importance of ongoing check-ins and skills training to address drinking problems in this population. It will be important for future studies to explore the unique benefits and costs conferred by these additional sessions, to see how they may boost the effects of such brief online interventions.
For individuals and families seeking recovery: Brief online interventions for hazardous and binge drinking have shown the potential to improve alcohol use outcomes in a variety of populations including members of the military and college students, among others. At the same time, individuals with more severe alcohol use problems, such as those with alcohol use disorder, will likely needadditional support beyond this kind of brief intervention.
For treatment professionals and treatment systems: Brief interventions like SBIRT, as well as online interventions for hazardous and binge drinking are increasingly being utilized in a range of settings and can be important early interventions that can increase the reach of these helpful services and alter drinking problem trajectories at low cost to individuals and systems.
For scientists: Brief online interventions for hazardous and binge drinking are increasingly being tested and utilized in a range of settings, and because of their accessibility, scalability, and cost effectiveness have tremendous potential to positively impact public health at the population level. At the same time, more work is needed to determine for whom and under what conditions these interventions are most helpful, and how they might be best delivered. Subsequent studies extending the present work reviewed here should compare active treatment groups and tease out how additional sessions or check-ups can potentially complement single-session interventions.
For policy makers: Brief online interventions for hazardous and binge drinking are increasingly being tested and utilized in a range of settings, and because of their accessibility, scalability, and cost effectiveness have tremendous potential to positively impact public health. Though such interventions cost money to develop, when effective, they ultimately represent good value for money because of the future cost savings they produce by changing problem drinking trajectories and helping engage people in treatment sooner.