Linking individuals with opioid use disorder medications more challenging for those living in rural areas and with mental health difficulties
Agonist medications for opioid use disorder, including buprenorphine and methadone, are life-saving treatments, yet there are large disparities in who engages in this treatment and who is retained. This study used Canadian health administrative data sets to examine predictors of engagement, which can ultimately help address gaps in the service continuum.
FDA-approved agonist medications for opioid use disorder — buprenorphine (often prescribed in formulation with naloxone known by the brand name Suboxone) and methadone — stimulate opioid receptors in controlled ways mitigating craving and facilitating functional stability. Taking these medications is associated with substantially lower likelihood of overdose and death and better recovery outcomes. Yet, despite evidence for their success, there are challenges to engaging and retaining individuals in treatment using these medications: only 20% of individuals with opioid use disorder in the United States receive any treatment. There are also large disparities in who engages in this treatment and who is retained. For example, among pregnant women, there are stark racial differences in the use of medications for opioid use disorder. Access can also be difficult due to financial barriers (e.g., being uninsured or homeless) or system capacity challenges (e.g., long waitlists).
There are a variety of factors at both the individual and the system level that seem to influence someone’s ability to be engaged in and retained in medication treatment for opioid use disorder. This study used Canadian health administrative data sets to explore characteristics of who is engaged and retained in opioid agonist therapy and who is not, to identify gaps in the service continuum.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of several linked health administrative data sets in Ontario, Canada. Ontario has a single-payer healthcare system with comprehensive administrative data systems. The analysis included individuals ages 16-100 years old who had sought medical care for opioid-related health problems and those who died from an opioid-related cause between 2005 and 2019 in Ontario, Canada. In Ontario, buprenorphine and methadone are typically prescribed in stand-alone clinics that have a focus on these medications and is separate from comprehensive primary care services. Prescribers are typically family physicians or general practitioners.
The outcomes of the study were an individual’s monthly treatment status for buprenorphine or methadone and their retention status between 2013-2019 (i.e., off medication treatment, retained on medication treatment less than 6 months, retained on medication treatment for 6 months or more). Medication treatment receipt was determined by whether a prescription was dispensed according to administrative data. The study included key factors related to both individual-level characteristics and the wider community setting: age, sex, urban/rural residence and which local health integration network an individual belonged to, neighborhood-based income, number of local opioid prescribers, type of medication received, and the type of provider responsible for the prescription. It also included history of mental health diagnoses which were determined from several databases using IDC-10, DSM-IV or Ontario Health Insurance Plan diagnostic data and included major mood disorders, psychotic disorders, anxiety disorders, and other non-substance use disorders such as personality disorders or dissociative disorders.
Of the 122,811 individuals in this study cohort, 60% were male and the median age was 36 years. During the study period, 79% of the study cohort received medication treatment at least once. The majority of the prescriptions were for methadone (78%) versus buprenorphine (22%) and nearly all came from high-volume prescribers.
WHAT DID THIS STUDY FIND?
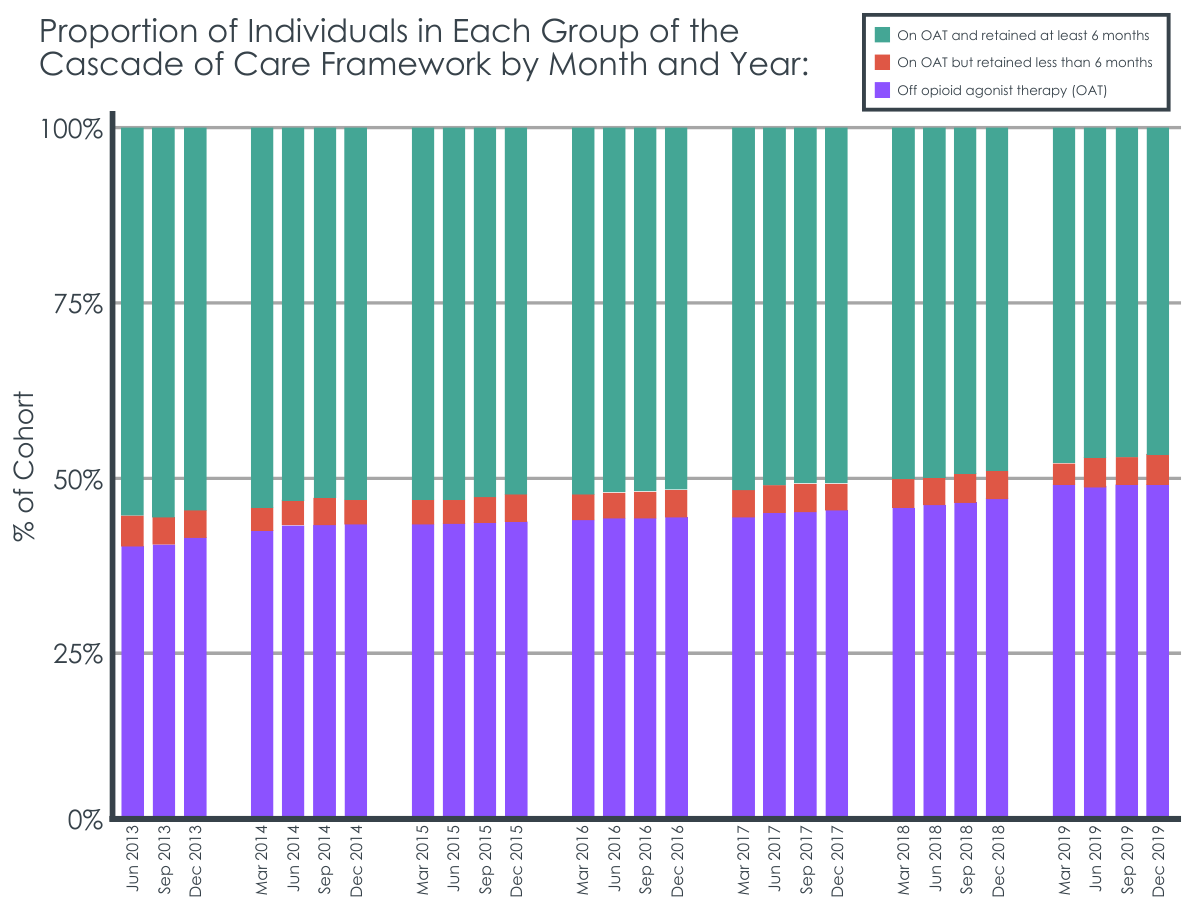
Majority of individuals received medication treatment but retention was poor.
Over a 6-year period, retention among those who received medication for at least 6-months declined from 55% to 48%. These rates indicate both that individuals who started medication in Ontario tended to stop it before guidelines suggested and that this decrease was happening overall, at a population level.
Medication initiation and retention have unique patterns of correlates.
There were unique patterns of indicators for receiving medication and for being retained on medication . That is, males were more likely to be taking medication , but once engaged, less likely to be retained for 6 or more months. Alternatively, both older individuals and individuals with higher neighborhood income were less likely to be receiving medication each month but were more likely to be retained for 6 or more months. The magnitude of these relationships, however, was small, indicating there are other important factors driving engagement and retention in buprenorphine and methadone for opioid use disorder.
Individuals living in rural areas and with a history of mental health diagnoses had lower overall engagement.
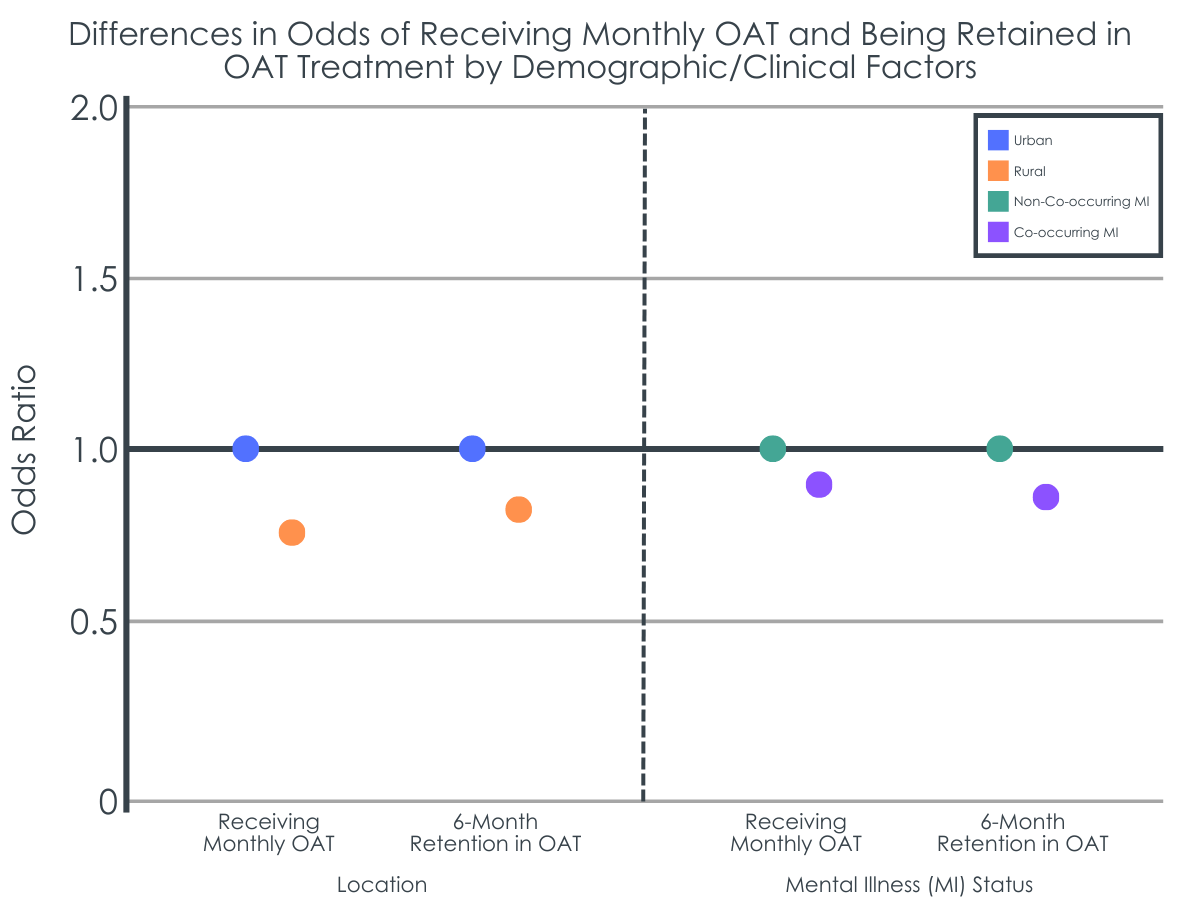
Individuals living in rural areas were less likely to receive medication each month and also to be retained for 6 or more months. Similarly, individuals with a history of mental health diagnoses (versus those without any co-occurring mental health diagnosis) were less likely to receive medication each month, to be retained for 6 or more months, and at higher risk for starting and discontinuing the medication. Individuals with a history of mental health diagnoses also had a higher risk of death, regardless of medication treatment status.
Figure 2. Odds ratios indicate the likelihood of an outcome, where 1 is the baseline the rest of the data are compared to. A data point being more than 1 indicates a higher likelihood, while less than 1 indicates a lower likelihood. In this instance, for example, rural participants were less likely to be receiving monthly OAT compared to urban participants.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Of those who sought treatment for opioid use disorder or died from an opioid-related cause in Ontario, Canada, this study found decreasing retention over time similar to a national US study of adults discharged from treatment, and participant characteristics seemed to drive potential gaps in retention. Interestingly, factors linked to receiving medication were not the same for factors linked to retention suggesting there may be different pathways to access and engagement with buprenorphine and methadone. For example, the finding that individuals living in high income neighborhoods were less likely to be engaged in medication treatment, but highly likely to be retained if they were engaged, suggests these individuals may be less likely overall to experience opioid related problems severe enough to warrant treatment, but when they do, they are also better able to access medication and continuing to receive it. This is in stark contrast to individuals living in rural areas and those with a history of mental health diagnoses. These individuals had poorer overall outcomes in terms of medication engagement, retention, and likelihood of dying during the study window suggesting they face elevated challenges and that there may be system-level gaps in their ability to access medication for opioid use disorder and other health resources. While these risks were relatively small in magnitude, they occurred in large population of individuals and would thus be likely to have important public health implications. Also, in line with previous research, younger participants were less likely to be retained in medication treatment for 6 months, suggesting multicomponent solutions may be needed to address known barriers to retention with this demographic (e.g., interventions that provide extended dosing options, home delivery, family involvement). Yet, the magnitude of all relationships examined were small, indicating there are still other important factors driving engagement and retention in medication treatment that were not measured or examined in this report.
Although the study provides a thorough summary of medication treatment rate of discharges and participant characteristics, several pieces of information were missing including substance use or mental health severity, dose of medication, and status of individuals when they stopped treatment (e.g., completed treatment versus dropped out.)
Additionally, while not directly examined, motivation to take medication, and views of medication treatment including potential stigma may play a substantial role in engagement with medications, and such measures should be considered in future studies.
Also, the majority of prescriptions were for methadone rather than buprenorphine and initiation and retention rates may differ if the opposite trend was true (majority buprenorphine). Also, methadone is typically reserved for more severe opioid use disorder and thus the estimates here may pertain more to patients at the more severe end of the disorder continuum.
It is unclear which particular mental health diagnoses may represent particular challenges for medication continuation, or whether any such diagnosis was associated with the same elevated levels of risks.
BOTTOM LINE
In this large-scale study of Canadian individuals with a history of opioid-related health problems, there was decreasing retention in medication treatment over time and participant characteristics seemed to partially account for potential gaps in both treatment and retention – those who lived in rural areas and who experienced mental health problems had slightly worse outcomes.
For individuals and families seeking recovery: Recovery from an opioid use disorder is a difficult process for many individuals. Medications such as methadone and buprenorphine for opioid use disorders can improve recovery outcomes, but only if individuals consistently receive it for a sustained period of time. Notably, there are many barriers to starting and staying on the medication, chief among these is the presence of a co-occurring mental health disorder. It is important to know that those barriers exist and to seek support in addressing them from providers and recovery supports in communities.
For treatment professionals and treatment systems: There is building evidence that medications for opioid use disorder are helpful approaches to reducing opioid use and decreasing overdose risk, yet patients face many barriers to starting medication and other barriers to continue with it.. Approaches that reach patients where they live, especially those in rural areas through telemedicine, may be one way to reduce barriers associated with treatment retention. Also, strategies that screen individuals seeking primary mental health treatment for opioid use disorder and actively link those with co-occurring disorders to buprenorphine and methadone providers may improve outcomes for these at-risk individuals. Providers and systems should be part of the bridge that connects patients to these needed services and helps them to reduce barriers.
For scientists: Scientists can play a valuable role in using innovative study designs, such as this one that links several comprehensive province-wide datasets, to better understand the reasons and barriers to treatment engagement and retention and assessing strategies to address these barriers. While this study identifies some significant relationships between individual, environmental, and systems-level factors associated with engagement and retention, the small magnitude of these relationships still suggests there are key factors not examined that may help further our understanding of engagement in medication for opioid use disorder. For example, although not examined in this study, stigma is a documented barrier to engaging in medication treatment for opioid use disorder and so future research in this area should examine the interrelated structural aspects of stigma and medication initiation and retention.
FDA-approved agonist medications for opioid use disorder — buprenorphine (often prescribed in formulation with naloxone known by the brand name Suboxone) and methadone — stimulate opioid receptors in controlled ways mitigating craving and facilitating functional stability. Taking these medications is associated with substantially lower likelihood of overdose and death and better recovery outcomes. Yet, despite evidence for their success, there are challenges to engaging and retaining individuals in treatment using these medications: only 20% of individuals with opioid use disorder in the United States receive any treatment. There are also large disparities in who engages in this treatment and who is retained. For example, among pregnant women, there are stark racial differences in the use of medications for opioid use disorder. Access can also be difficult due to financial barriers (e.g., being uninsured or homeless) or system capacity challenges (e.g., long waitlists).
There are a variety of factors at both the individual and the system level that seem to influence someone’s ability to be engaged in and retained in medication treatment for opioid use disorder. This study used Canadian health administrative data sets to explore characteristics of who is engaged and retained in opioid agonist therapy and who is not, to identify gaps in the service continuum.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of several linked health administrative data sets in Ontario, Canada. Ontario has a single-payer healthcare system with comprehensive administrative data systems. The analysis included individuals ages 16-100 years old who had sought medical care for opioid-related health problems and those who died from an opioid-related cause between 2005 and 2019 in Ontario, Canada. In Ontario, buprenorphine and methadone are typically prescribed in stand-alone clinics that have a focus on these medications and is separate from comprehensive primary care services. Prescribers are typically family physicians or general practitioners.
The outcomes of the study were an individual’s monthly treatment status for buprenorphine or methadone and their retention status between 2013-2019 (i.e., off medication treatment, retained on medication treatment less than 6 months, retained on medication treatment for 6 months or more). Medication treatment receipt was determined by whether a prescription was dispensed according to administrative data. The study included key factors related to both individual-level characteristics and the wider community setting: age, sex, urban/rural residence and which local health integration network an individual belonged to, neighborhood-based income, number of local opioid prescribers, type of medication received, and the type of provider responsible for the prescription. It also included history of mental health diagnoses which were determined from several databases using IDC-10, DSM-IV or Ontario Health Insurance Plan diagnostic data and included major mood disorders, psychotic disorders, anxiety disorders, and other non-substance use disorders such as personality disorders or dissociative disorders.
Of the 122,811 individuals in this study cohort, 60% were male and the median age was 36 years. During the study period, 79% of the study cohort received medication treatment at least once. The majority of the prescriptions were for methadone (78%) versus buprenorphine (22%) and nearly all came from high-volume prescribers.
WHAT DID THIS STUDY FIND?
Majority of individuals received medication treatment but retention was poor.
Over a 6-year period, retention among those who received medication for at least 6-months declined from 55% to 48%. These rates indicate both that individuals who started medication in Ontario tended to stop it before guidelines suggested and that this decrease was happening overall, at a population level.
Medication initiation and retention have unique patterns of correlates.
There were unique patterns of indicators for receiving medication and for being retained on medication . That is, males were more likely to be taking medication , but once engaged, less likely to be retained for 6 or more months. Alternatively, both older individuals and individuals with higher neighborhood income were less likely to be receiving medication each month but were more likely to be retained for 6 or more months. The magnitude of these relationships, however, was small, indicating there are other important factors driving engagement and retention in buprenorphine and methadone for opioid use disorder.
Individuals living in rural areas and with a history of mental health diagnoses had lower overall engagement.
Individuals living in rural areas were less likely to receive medication each month and also to be retained for 6 or more months. Similarly, individuals with a history of mental health diagnoses (versus those without any co-occurring mental health diagnosis) were less likely to receive medication each month, to be retained for 6 or more months, and at higher risk for starting and discontinuing the medication. Individuals with a history of mental health diagnoses also had a higher risk of death, regardless of medication treatment status.
Figure 2. Odds ratios indicate the likelihood of an outcome, where 1 is the baseline the rest of the data are compared to. A data point being more than 1 indicates a higher likelihood, while less than 1 indicates a lower likelihood. In this instance, for example, rural participants were less likely to be receiving monthly OAT compared to urban participants.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Of those who sought treatment for opioid use disorder or died from an opioid-related cause in Ontario, Canada, this study found decreasing retention over time similar to a national US study of adults discharged from treatment, and participant characteristics seemed to drive potential gaps in retention. Interestingly, factors linked to receiving medication were not the same for factors linked to retention suggesting there may be different pathways to access and engagement with buprenorphine and methadone. For example, the finding that individuals living in high income neighborhoods were less likely to be engaged in medication treatment, but highly likely to be retained if they were engaged, suggests these individuals may be less likely overall to experience opioid related problems severe enough to warrant treatment, but when they do, they are also better able to access medication and continuing to receive it. This is in stark contrast to individuals living in rural areas and those with a history of mental health diagnoses. These individuals had poorer overall outcomes in terms of medication engagement, retention, and likelihood of dying during the study window suggesting they face elevated challenges and that there may be system-level gaps in their ability to access medication for opioid use disorder and other health resources. While these risks were relatively small in magnitude, they occurred in large population of individuals and would thus be likely to have important public health implications. Also, in line with previous research, younger participants were less likely to be retained in medication treatment for 6 months, suggesting multicomponent solutions may be needed to address known barriers to retention with this demographic (e.g., interventions that provide extended dosing options, home delivery, family involvement). Yet, the magnitude of all relationships examined were small, indicating there are still other important factors driving engagement and retention in medication treatment that were not measured or examined in this report.
Although the study provides a thorough summary of medication treatment rate of discharges and participant characteristics, several pieces of information were missing including substance use or mental health severity, dose of medication, and status of individuals when they stopped treatment (e.g., completed treatment versus dropped out.)
Additionally, while not directly examined, motivation to take medication, and views of medication treatment including potential stigma may play a substantial role in engagement with medications, and such measures should be considered in future studies.
Also, the majority of prescriptions were for methadone rather than buprenorphine and initiation and retention rates may differ if the opposite trend was true (majority buprenorphine). Also, methadone is typically reserved for more severe opioid use disorder and thus the estimates here may pertain more to patients at the more severe end of the disorder continuum.
It is unclear which particular mental health diagnoses may represent particular challenges for medication continuation, or whether any such diagnosis was associated with the same elevated levels of risks.
BOTTOM LINE
In this large-scale study of Canadian individuals with a history of opioid-related health problems, there was decreasing retention in medication treatment over time and participant characteristics seemed to partially account for potential gaps in both treatment and retention – those who lived in rural areas and who experienced mental health problems had slightly worse outcomes.
For individuals and families seeking recovery: Recovery from an opioid use disorder is a difficult process for many individuals. Medications such as methadone and buprenorphine for opioid use disorders can improve recovery outcomes, but only if individuals consistently receive it for a sustained period of time. Notably, there are many barriers to starting and staying on the medication, chief among these is the presence of a co-occurring mental health disorder. It is important to know that those barriers exist and to seek support in addressing them from providers and recovery supports in communities.
For treatment professionals and treatment systems: There is building evidence that medications for opioid use disorder are helpful approaches to reducing opioid use and decreasing overdose risk, yet patients face many barriers to starting medication and other barriers to continue with it.. Approaches that reach patients where they live, especially those in rural areas through telemedicine, may be one way to reduce barriers associated with treatment retention. Also, strategies that screen individuals seeking primary mental health treatment for opioid use disorder and actively link those with co-occurring disorders to buprenorphine and methadone providers may improve outcomes for these at-risk individuals. Providers and systems should be part of the bridge that connects patients to these needed services and helps them to reduce barriers.
For scientists: Scientists can play a valuable role in using innovative study designs, such as this one that links several comprehensive province-wide datasets, to better understand the reasons and barriers to treatment engagement and retention and assessing strategies to address these barriers. While this study identifies some significant relationships between individual, environmental, and systems-level factors associated with engagement and retention, the small magnitude of these relationships still suggests there are key factors not examined that may help further our understanding of engagement in medication for opioid use disorder. For example, although not examined in this study, stigma is a documented barrier to engaging in medication treatment for opioid use disorder and so future research in this area should examine the interrelated structural aspects of stigma and medication initiation and retention.
FDA-approved agonist medications for opioid use disorder — buprenorphine (often prescribed in formulation with naloxone known by the brand name Suboxone) and methadone — stimulate opioid receptors in controlled ways mitigating craving and facilitating functional stability. Taking these medications is associated with substantially lower likelihood of overdose and death and better recovery outcomes. Yet, despite evidence for their success, there are challenges to engaging and retaining individuals in treatment using these medications: only 20% of individuals with opioid use disorder in the United States receive any treatment. There are also large disparities in who engages in this treatment and who is retained. For example, among pregnant women, there are stark racial differences in the use of medications for opioid use disorder. Access can also be difficult due to financial barriers (e.g., being uninsured or homeless) or system capacity challenges (e.g., long waitlists).
There are a variety of factors at both the individual and the system level that seem to influence someone’s ability to be engaged in and retained in medication treatment for opioid use disorder. This study used Canadian health administrative data sets to explore characteristics of who is engaged and retained in opioid agonist therapy and who is not, to identify gaps in the service continuum.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of several linked health administrative data sets in Ontario, Canada. Ontario has a single-payer healthcare system with comprehensive administrative data systems. The analysis included individuals ages 16-100 years old who had sought medical care for opioid-related health problems and those who died from an opioid-related cause between 2005 and 2019 in Ontario, Canada. In Ontario, buprenorphine and methadone are typically prescribed in stand-alone clinics that have a focus on these medications and is separate from comprehensive primary care services. Prescribers are typically family physicians or general practitioners.
The outcomes of the study were an individual’s monthly treatment status for buprenorphine or methadone and their retention status between 2013-2019 (i.e., off medication treatment, retained on medication treatment less than 6 months, retained on medication treatment for 6 months or more). Medication treatment receipt was determined by whether a prescription was dispensed according to administrative data. The study included key factors related to both individual-level characteristics and the wider community setting: age, sex, urban/rural residence and which local health integration network an individual belonged to, neighborhood-based income, number of local opioid prescribers, type of medication received, and the type of provider responsible for the prescription. It also included history of mental health diagnoses which were determined from several databases using IDC-10, DSM-IV or Ontario Health Insurance Plan diagnostic data and included major mood disorders, psychotic disorders, anxiety disorders, and other non-substance use disorders such as personality disorders or dissociative disorders.
Of the 122,811 individuals in this study cohort, 60% were male and the median age was 36 years. During the study period, 79% of the study cohort received medication treatment at least once. The majority of the prescriptions were for methadone (78%) versus buprenorphine (22%) and nearly all came from high-volume prescribers.
WHAT DID THIS STUDY FIND?
Majority of individuals received medication treatment but retention was poor.
Over a 6-year period, retention among those who received medication for at least 6-months declined from 55% to 48%. These rates indicate both that individuals who started medication in Ontario tended to stop it before guidelines suggested and that this decrease was happening overall, at a population level.
Medication initiation and retention have unique patterns of correlates.
There were unique patterns of indicators for receiving medication and for being retained on medication . That is, males were more likely to be taking medication , but once engaged, less likely to be retained for 6 or more months. Alternatively, both older individuals and individuals with higher neighborhood income were less likely to be receiving medication each month but were more likely to be retained for 6 or more months. The magnitude of these relationships, however, was small, indicating there are other important factors driving engagement and retention in buprenorphine and methadone for opioid use disorder.
Individuals living in rural areas and with a history of mental health diagnoses had lower overall engagement.
Individuals living in rural areas were less likely to receive medication each month and also to be retained for 6 or more months. Similarly, individuals with a history of mental health diagnoses (versus those without any co-occurring mental health diagnosis) were less likely to receive medication each month, to be retained for 6 or more months, and at higher risk for starting and discontinuing the medication. Individuals with a history of mental health diagnoses also had a higher risk of death, regardless of medication treatment status.
Figure 2. Odds ratios indicate the likelihood of an outcome, where 1 is the baseline the rest of the data are compared to. A data point being more than 1 indicates a higher likelihood, while less than 1 indicates a lower likelihood. In this instance, for example, rural participants were less likely to be receiving monthly OAT compared to urban participants.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Of those who sought treatment for opioid use disorder or died from an opioid-related cause in Ontario, Canada, this study found decreasing retention over time similar to a national US study of adults discharged from treatment, and participant characteristics seemed to drive potential gaps in retention. Interestingly, factors linked to receiving medication were not the same for factors linked to retention suggesting there may be different pathways to access and engagement with buprenorphine and methadone. For example, the finding that individuals living in high income neighborhoods were less likely to be engaged in medication treatment, but highly likely to be retained if they were engaged, suggests these individuals may be less likely overall to experience opioid related problems severe enough to warrant treatment, but when they do, they are also better able to access medication and continuing to receive it. This is in stark contrast to individuals living in rural areas and those with a history of mental health diagnoses. These individuals had poorer overall outcomes in terms of medication engagement, retention, and likelihood of dying during the study window suggesting they face elevated challenges and that there may be system-level gaps in their ability to access medication for opioid use disorder and other health resources. While these risks were relatively small in magnitude, they occurred in large population of individuals and would thus be likely to have important public health implications. Also, in line with previous research, younger participants were less likely to be retained in medication treatment for 6 months, suggesting multicomponent solutions may be needed to address known barriers to retention with this demographic (e.g., interventions that provide extended dosing options, home delivery, family involvement). Yet, the magnitude of all relationships examined were small, indicating there are still other important factors driving engagement and retention in medication treatment that were not measured or examined in this report.
Although the study provides a thorough summary of medication treatment rate of discharges and participant characteristics, several pieces of information were missing including substance use or mental health severity, dose of medication, and status of individuals when they stopped treatment (e.g., completed treatment versus dropped out.)
Additionally, while not directly examined, motivation to take medication, and views of medication treatment including potential stigma may play a substantial role in engagement with medications, and such measures should be considered in future studies.
Also, the majority of prescriptions were for methadone rather than buprenorphine and initiation and retention rates may differ if the opposite trend was true (majority buprenorphine). Also, methadone is typically reserved for more severe opioid use disorder and thus the estimates here may pertain more to patients at the more severe end of the disorder continuum.
It is unclear which particular mental health diagnoses may represent particular challenges for medication continuation, or whether any such diagnosis was associated with the same elevated levels of risks.
BOTTOM LINE
In this large-scale study of Canadian individuals with a history of opioid-related health problems, there was decreasing retention in medication treatment over time and participant characteristics seemed to partially account for potential gaps in both treatment and retention – those who lived in rural areas and who experienced mental health problems had slightly worse outcomes.
For individuals and families seeking recovery: Recovery from an opioid use disorder is a difficult process for many individuals. Medications such as methadone and buprenorphine for opioid use disorders can improve recovery outcomes, but only if individuals consistently receive it for a sustained period of time. Notably, there are many barriers to starting and staying on the medication, chief among these is the presence of a co-occurring mental health disorder. It is important to know that those barriers exist and to seek support in addressing them from providers and recovery supports in communities.
For treatment professionals and treatment systems: There is building evidence that medications for opioid use disorder are helpful approaches to reducing opioid use and decreasing overdose risk, yet patients face many barriers to starting medication and other barriers to continue with it.. Approaches that reach patients where they live, especially those in rural areas through telemedicine, may be one way to reduce barriers associated with treatment retention. Also, strategies that screen individuals seeking primary mental health treatment for opioid use disorder and actively link those with co-occurring disorders to buprenorphine and methadone providers may improve outcomes for these at-risk individuals. Providers and systems should be part of the bridge that connects patients to these needed services and helps them to reduce barriers.
For scientists: Scientists can play a valuable role in using innovative study designs, such as this one that links several comprehensive province-wide datasets, to better understand the reasons and barriers to treatment engagement and retention and assessing strategies to address these barriers. While this study identifies some significant relationships between individual, environmental, and systems-level factors associated with engagement and retention, the small magnitude of these relationships still suggests there are key factors not examined that may help further our understanding of engagement in medication for opioid use disorder. For example, although not examined in this study, stigma is a documented barrier to engaging in medication treatment for opioid use disorder and so future research in this area should examine the interrelated structural aspects of stigma and medication initiation and retention.