Can supervised consumption site expansion reduce HIV and hepatitis C infections?
Supervised consumption sites can help reduce rates of infectious diseases that are commonly transmitted through injection drug use by providing sterile syringes and other resources that promote safer drug use. Researchers in this study examined the potential impact of scaling up these harm reduction services on rates of infectious disease.
People who inject drugs face increased risks of contracting the blood-borne infectious disease HIV and hepatitis C from sharing contaminated syringes and other equipment. Recent outbreaks of HIV and hepatitis C in the United States highlight the magnitude of this problem and that solutions are needed to help address it.
Supervised consumption sites, also called overdose prevention sites or safe injection sites, are a type of harm reduction strategy that have been established not only to address the opioid overdose crisis, but also to reduce transmission of infectious diseases. Transmission risks are reduced at these sites by providing people who inject drugs sterile syringes, guidance about safer drug use, education about infectious disease, and testing for infectious diseases which can help with early identification and prevent disease spread. They may also offer other services, such as linkage to healthcare, addiction treatment, and other social services, drug checking, and distribution of naloxone.
A recent systematic review of research conducted in Canada, Australia, and Europe suggests that supervised consumption sites are associated with public health benefits. However, they are still unsanctioned in the United States, which limits what is understood about their impact in the US. Researchers in this study examined the potential impact of scaling up the implementation of supervised consumption sites on rates of infectious disease. Such research can shed light on the extent to which supervised consumption sites can be an effective intervention for reducing infectious disease rates.
HOW WAS THIS STUDY CONDUCTED?
The research team used a modeling approach where they simulated the potential impact of scaling up the implementation of supervised consumption sites on rates of HIV and hepatitis C among people who inject drugs. This model used data from 3 counties in California.
Co-infection of both HIV and hepatitis C, disease stage, and treatment was accounted for in the simulation model.
Of note, stages of HIV include: susceptible, acute, latent, pre-AIDS, and AIDS. People who are susceptible, or at risk for contracting the disease, can become infected and enter the acute stage, which is of short duration with high viral load and transmissibility. After the acute stage, people progress to the latent stage, which is of longer duration with a lower viral load and transmissibility. Without treatment, people can then progress to the pre-AIDS and AIDS stages. However, people can begin treatment with antiretroviral therapy during the latent, pre-AIDS, and AIDS stages, which can slow the disease progression and decrease transmission due to lower viral loads. As such, researchers stratified the model by: HIV disease stage, which included susceptible, acute, latent, pre-AIDS, AIDS; stage of HIV/AIDS and antiretroviral therapy, which included latent HIV on therapy, pre-AIDS on therapy, and AIDS on therapy; chronic hepatitis C infection or uninfected; and predicted use of supervised consumption sites or not. Transmission of HIV through sex and injection drug use was incorporated into the simulation model, while transmission of hepatitis C through injection drug use only was incorporated. This is because HIV is commonly transmitted both ways, while hepatitis C is more commonly transmitted through injection equipment sharing.
The model was calibrated to epidemiological data for San Francisco, Los Angeles, and San Diego based on availability of data in these three areas. Data were pulled from the National HIV Behavioral Surveillance surveys and longitudinal cohorts of people who inject drugs. While exact years for the data pulls varied by county, the model included the following variables for each county: HIV prevalence among people who inject drugs, chronic hepatitis C prevalence among people who inject drugs, proportion of HIV infections from sexual transmission, and antiretroviral therapy coverage among people who inject drugs and living with HIV. For San Diego only, hepatitis C incidence among people who inject drugs was also included, where the researchers simulated a higher hepatitis C transmission rate from 2015 and thereafter of 4-fold, given recent research showing increasing risks of transmission in this area.
Based on 2022 data from the National HIV Behavioral Surveillance survey, the researchers estimated that HIV prevalence among people who inject drugs was 10.1% for San Francisco, 4.5% for Los Angeles, and 3.0% for San Diego. Estimates of the proportion of HIV infections due to sexual transmission ranged from 62% for San Francisco to 77% for Los Angeles and San Diego. Estimates of the proportion of people who inject drugs and living with HIV on antiretroviral therapy were 92% for San Francisco, 80% for Los Angeles, and 67% for San Diego.
Estimates of chronic hepatitis C prevalence were derived for 2 time points, given recent advances in curative therapies. For San Francisco, estimates were 42% in 2015 and 35% in 2018. For Los Angeles, estimates were 48% in 2015 and 41% in 2018. For San Diego, data was not available from the National HIV Behavioral Surveillance survey and the researchers used data from a cohort study instead for 1 time point. The prevalence in 2021 for San Diego was estimated to be 30%.
When programming the model, the researchers assumed that people can start and stop using supervised consumption sites. People enter the model when they hypothetically begin injection drug use, and it was assumed these individuals were at risk for both HIV and hepatitis C infection. People hypothetically leave the model when they stop injecting drugs or die, either due to HIV or otherwise. It was also assumed that access to sites reduced syringe sharing among people who inject drugs by 83% and attending a site reduced the risk of drug-related mortality by 54%.
The researchers modeled scenarios where site coverage was scaled up from 0% of people who inject drugs to 20% starting in 2024 and how this would impact rates of HIV and Hepatitis C over 10 years in each county. The main outcomes of interest were HIV and hepatitis C prevalence and incidence. Prevalence refers to the total number of cases (both old and new) at a given point in time and is measured as percentage, while incidence refers to the number of the new cases that occur over a period of time and is measured as a rate in person-years (i.e., the number of people multiplied by the number of years they are observed). New rates of HIV and hepatitis C that could have been prevented in each county were also assessed at 5 years and 10 years following the scale up.
WHAT DID THIS STUDY FIND?
Models projected that expansion of supervised consumption site coverage would reduce HIV infections
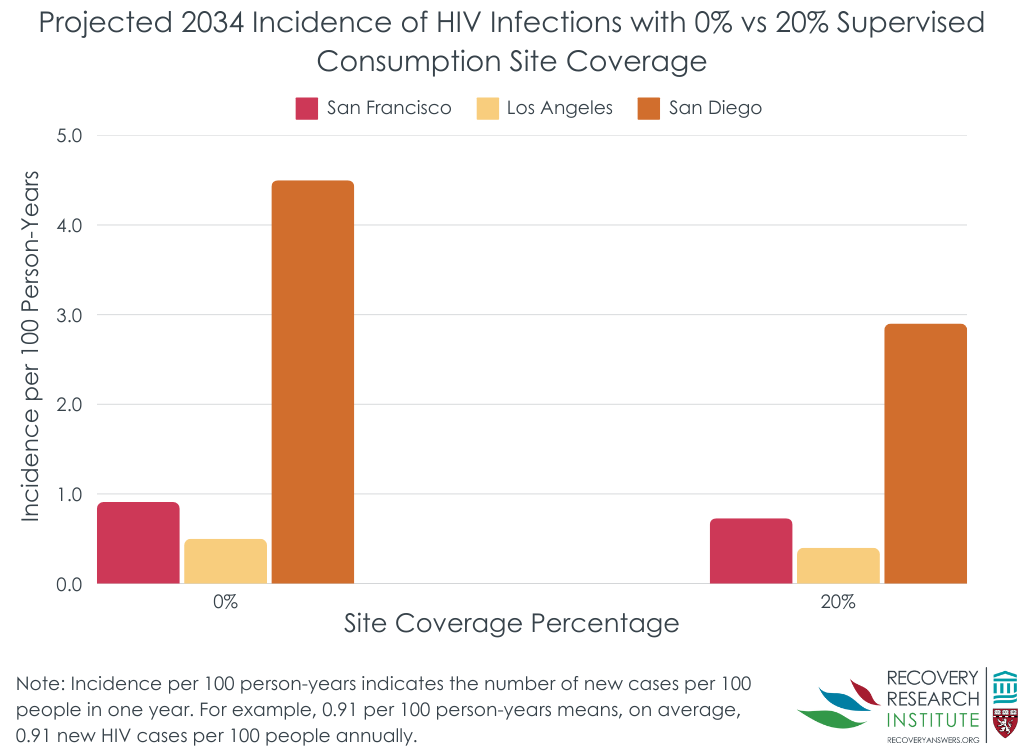
In San Francisco, at 0% site coverage, the prevalence of HIV in 2034 was estimated to be 9.6%. Increasing site coverage to 20% reduced the prevalence to 8.6% by 2034. The estimated incidence of HIV at 0% site coverage in 2034 was 0.91 per 100 person-years (i.e., 0.91 new HIV cases would occur for every 100 people observed for 1 year). Increasing coverage to 20% reduced the incidence to 0.73 by 2034, which equals a 20% reduction (see Figure below). The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 17.3% and 21.8% at 10 years.
In Los Angeles, at 0% site coverage, the prevalence of HIV in 2034 was estimated to be 4.1%. Increasing site coverage to 20% reduced the prevalence to 3.7% by 2034. The estimated incidence of HIV at 0% site coverage in 2034 was 0.48 per 100 person-years. Increasing coverage to 20% reduced the incidence to 0.40 by 2034, which equals a 17% reduction. The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 12.9% and 17.7% at 10 years.
In San Diego, rates of HIV were projected to increase due to increases in risk and lack of treatment advances, yet declines were still observed. At 0% site coverage, the prevalence of HIV in 2034 was estimated to be 20.6%. Increasing site coverage to 20% reduced the prevalence to 14.9% by 2034. The estimated incidence of HIV at 0% site coverage in 2034 was 4.5 per 100 person-years. Increasing coverage to 20% reduced the incidence to 2.9 by 2034, which equals a 35% reduction. The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 30.8% and 32.1% at 10 years.
Hypothetical expansion of supervised consumption sites reduced hepatitis C infections
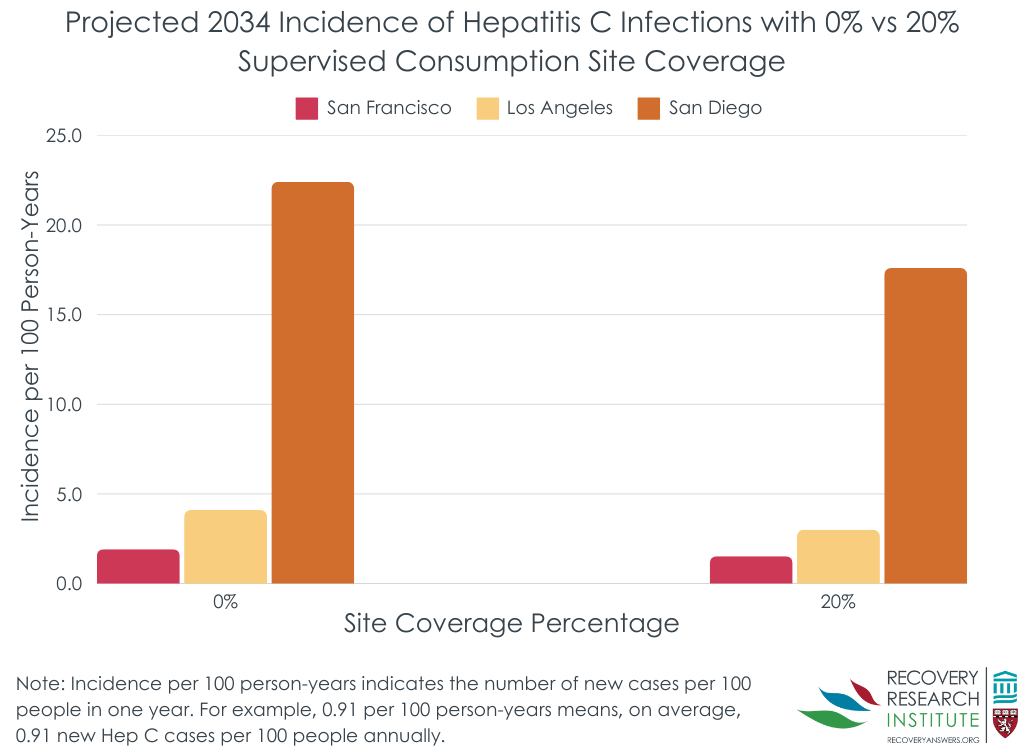
In San Francisco, at 0% site coverage, the prevalence of hepatitis C in 2034 was estimated to be 16.9%, which reflects a decline from 25.6% in 2024 due to treatment advances. Increasing site coverage to 20% resulted in even more of a decline, with a prevalence of 14.9% by 2034. The estimated incidence of hepatitis C at 0% site coverage in 2034 was 1.92 per 100 person-years. Increasing coverage to 20% reduced the incidence to 1.52 by 2034, which equals a 21% reduction (see Figure below). The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 22.6% and 28.3% at 10 years.
In Los Angeles, at 0% site coverage, the prevalence of hepatitis C in 2034 was estimated to be 24.2%, which reflects a decline from 2024 due to treatment advances. Increasing site coverage to 20% resulted in an even greater decline, with a prevalence of 20.8% by 2034. The estimated incidence of hepatitis C at 0% site coverage in 2034 was 4.08 per 100 person-years. Increasing coverage to 20% reduced the incidence to 3.00 by 2034, which equals a 26% reduction. The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 23.5% and 29.8% at 10 years.
In San Diego, at 0% site coverage, the prevalence of hepatitis C in 2034 was estimated to increase to 71.5%, given the high incidence in 2021. Increasing site coverage to 20% reduced the prevalence to 65.8% by 2034. The estimated incidence of hepatitis C at 0% site coverage in 2034 was 22.4 per 100 person-years. Increasing coverage to 20% reduced the incidence to 17.6 by 2034, which equals a 21% reduction. The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 23.3% and 24.3% at 10 years.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Scaling up supervised consumption site coverage resulted in reductions in the prevalence and incidence of both HIV and hepatitis C infections, as well as the percentage of new infections that could be prevented. These results suggest that supervised consumption sites may be an effective intervention for reducing infectious disease rates. Even in the context of treatment advances for hepatitis C, which would naturally result in a reduction of rates, these results demonstrated that scaling up supervised consumption sites may further reduce rates.
Of note, the statistical modeling used in the current study used estimates from existing epidemiological data to simulate what is statistically likely to happen over the next 10 years and is therefore considered hypothetical and demonstrates potential benefits, rather than a reflection of statistical associations found using data already collected. Nonetheless, the study has several strengths, including being one of the first to examine long-term public health benefits of supervised consumption sites in the US. The study was also able to compare counties with different rates of HIV and hepatitis C, which sheds light on the impact of the sites in counties that are experiencing different magnitudes of the problem.
One issue is cost-effectiveness of providing supervised consumption sites given that the main mechanism through which these positive effects are projected to occur is mostly by providing access to sterile syringes. While supervised consumption sites clearly provide other major benefits (i.e., preventing death form overdose), access to sterile syringes, specifically, might be possible much more cheaply and efficiently through other more ubiquitous venues, such as substance use disorder and infectious disease treatment venues or even primary care offices and pharmacies. Nevertheless, what is compelling here is that the potential increase of supervised consumption sites would not only likely decrease overdose deaths, but also additionally decrease infectious disease transmission that confer enormous long-term health and economic burdens.
The study was conducted based on epidemiological data from California, a progressive state that already has more favorable views towards harm reduction. Results may therefore not generalize to other US states with less favorable views or to other countries.
Due to a lack of data, the research team was not able to include demographic data in the modeling, such as age, sex, race/ethnicity, and sexual orientation. These variables could have affected the results since they can influence access to harm reduction strategies.
The study used statistical modeling to simulate what is statistically likely to happen over the next 10 years. Therefore, the results are based on a hypothetical scenario of scaling up supervised consumption sites and demonstrates potential benefits.
Estimates from the study have a wide range, which reflects uncertainty and the possibility of inaccurate results.
The researchers focused on the outcomes of HIV and hepatitis C only and did not consider other soft tissue infections that people who use drugs are at risk for. They also did not examine the costs vs. benefits to implement supervised consumption sites.
BOTTOM LINE
Hypothetical expansion of supervised consumption site coverage resulted in reductions in the prevalence and incidence of both HIV and hepatitis C infections, as well as the percentage of new infections that could be prevented. Statistical modeling in the current study employed estimates from existing epidemiological data to simulate what is statistically likely to happen over the next 10 years. Because studies of real-world outcomes in US supervised consumption sites are in the earliest stages while decisions around their criminal-legal status are at hand, computer simulation studies like these can help policy makers make critical decisions for their communities.
For individuals and families seeking recovery: This study found that expanding supervised consumption sites could result in fewer HIV and hepatitis C infections and prevent new infections. Accordingly, people who use drugs and have access to these sites may see similar benefits of using them. However, they are still unsanctioned or illegal in many US states. People without access to such programs who similarly try to engage in safer injection drug use practices and use sterile injection equipment could also reduce their risk of HIV and hepatitis C.
For treatment professionals and treatment systems: This study showed that hypothetically expanding supervised consumption sites resulted in fewer HIV and hepatitis C infections and prevented new infections by providing access to sterile syringes. Accordingly, treatment systems and professionals that similarly promote safer injection drug use practices and use of sterile injection equipment among people who inject drugs could see similar benefits of reductions in infectious diseases.
For scientists: Because the current study used simulation modeling to predict what is statistically likely to happen over the next 10 years, future research that examines the actual observed impact of supervised consumption sites as they become available in the US could corroborate the potential benefits demonstrated by hypothetical modeling studies such as the one summarize here. Additionally, future research that examines demographic differences would shed light on whether the outcomes generalize to different demographic groups. Finally, cost-benefit analyses would help us understand what the costs were to implement supervised consumption sites and what the savings could be in terms of the number of infections that were averted and the health care savings therein.
For policy makers: This study demonstrated that scaling up supervised consumption sites may potentially reduce rates of HIV and hepatitis C. However, supervised consumption sites are currently unsanctioned in the US. Because studies of real-world outcomes in US supervised consumption sites are in the earliest stages while decisions around their criminal-legal status are at hand, computer simulation studies like these can help policy makers make critical decisions for their communities. Additionally, policies that fund research to evaluate the impact of supervised consumption sites could further demonstrate the public health benefits of them, as well as the costs vs. benefits of implementation.
People who inject drugs face increased risks of contracting the blood-borne infectious disease HIV and hepatitis C from sharing contaminated syringes and other equipment. Recent outbreaks of HIV and hepatitis C in the United States highlight the magnitude of this problem and that solutions are needed to help address it.
Supervised consumption sites, also called overdose prevention sites or safe injection sites, are a type of harm reduction strategy that have been established not only to address the opioid overdose crisis, but also to reduce transmission of infectious diseases. Transmission risks are reduced at these sites by providing people who inject drugs sterile syringes, guidance about safer drug use, education about infectious disease, and testing for infectious diseases which can help with early identification and prevent disease spread. They may also offer other services, such as linkage to healthcare, addiction treatment, and other social services, drug checking, and distribution of naloxone.
A recent systematic review of research conducted in Canada, Australia, and Europe suggests that supervised consumption sites are associated with public health benefits. However, they are still unsanctioned in the United States, which limits what is understood about their impact in the US. Researchers in this study examined the potential impact of scaling up the implementation of supervised consumption sites on rates of infectious disease. Such research can shed light on the extent to which supervised consumption sites can be an effective intervention for reducing infectious disease rates.
HOW WAS THIS STUDY CONDUCTED?
The research team used a modeling approach where they simulated the potential impact of scaling up the implementation of supervised consumption sites on rates of HIV and hepatitis C among people who inject drugs. This model used data from 3 counties in California.
Co-infection of both HIV and hepatitis C, disease stage, and treatment was accounted for in the simulation model.
Of note, stages of HIV include: susceptible, acute, latent, pre-AIDS, and AIDS. People who are susceptible, or at risk for contracting the disease, can become infected and enter the acute stage, which is of short duration with high viral load and transmissibility. After the acute stage, people progress to the latent stage, which is of longer duration with a lower viral load and transmissibility. Without treatment, people can then progress to the pre-AIDS and AIDS stages. However, people can begin treatment with antiretroviral therapy during the latent, pre-AIDS, and AIDS stages, which can slow the disease progression and decrease transmission due to lower viral loads. As such, researchers stratified the model by: HIV disease stage, which included susceptible, acute, latent, pre-AIDS, AIDS; stage of HIV/AIDS and antiretroviral therapy, which included latent HIV on therapy, pre-AIDS on therapy, and AIDS on therapy; chronic hepatitis C infection or uninfected; and predicted use of supervised consumption sites or not. Transmission of HIV through sex and injection drug use was incorporated into the simulation model, while transmission of hepatitis C through injection drug use only was incorporated. This is because HIV is commonly transmitted both ways, while hepatitis C is more commonly transmitted through injection equipment sharing.
The model was calibrated to epidemiological data for San Francisco, Los Angeles, and San Diego based on availability of data in these three areas. Data were pulled from the National HIV Behavioral Surveillance surveys and longitudinal cohorts of people who inject drugs. While exact years for the data pulls varied by county, the model included the following variables for each county: HIV prevalence among people who inject drugs, chronic hepatitis C prevalence among people who inject drugs, proportion of HIV infections from sexual transmission, and antiretroviral therapy coverage among people who inject drugs and living with HIV. For San Diego only, hepatitis C incidence among people who inject drugs was also included, where the researchers simulated a higher hepatitis C transmission rate from 2015 and thereafter of 4-fold, given recent research showing increasing risks of transmission in this area.
Based on 2022 data from the National HIV Behavioral Surveillance survey, the researchers estimated that HIV prevalence among people who inject drugs was 10.1% for San Francisco, 4.5% for Los Angeles, and 3.0% for San Diego. Estimates of the proportion of HIV infections due to sexual transmission ranged from 62% for San Francisco to 77% for Los Angeles and San Diego. Estimates of the proportion of people who inject drugs and living with HIV on antiretroviral therapy were 92% for San Francisco, 80% for Los Angeles, and 67% for San Diego.
Estimates of chronic hepatitis C prevalence were derived for 2 time points, given recent advances in curative therapies. For San Francisco, estimates were 42% in 2015 and 35% in 2018. For Los Angeles, estimates were 48% in 2015 and 41% in 2018. For San Diego, data was not available from the National HIV Behavioral Surveillance survey and the researchers used data from a cohort study instead for 1 time point. The prevalence in 2021 for San Diego was estimated to be 30%.
When programming the model, the researchers assumed that people can start and stop using supervised consumption sites. People enter the model when they hypothetically begin injection drug use, and it was assumed these individuals were at risk for both HIV and hepatitis C infection. People hypothetically leave the model when they stop injecting drugs or die, either due to HIV or otherwise. It was also assumed that access to sites reduced syringe sharing among people who inject drugs by 83% and attending a site reduced the risk of drug-related mortality by 54%.
The researchers modeled scenarios where site coverage was scaled up from 0% of people who inject drugs to 20% starting in 2024 and how this would impact rates of HIV and Hepatitis C over 10 years in each county. The main outcomes of interest were HIV and hepatitis C prevalence and incidence. Prevalence refers to the total number of cases (both old and new) at a given point in time and is measured as percentage, while incidence refers to the number of the new cases that occur over a period of time and is measured as a rate in person-years (i.e., the number of people multiplied by the number of years they are observed). New rates of HIV and hepatitis C that could have been prevented in each county were also assessed at 5 years and 10 years following the scale up.
WHAT DID THIS STUDY FIND?
Models projected that expansion of supervised consumption site coverage would reduce HIV infections
In San Francisco, at 0% site coverage, the prevalence of HIV in 2034 was estimated to be 9.6%. Increasing site coverage to 20% reduced the prevalence to 8.6% by 2034. The estimated incidence of HIV at 0% site coverage in 2034 was 0.91 per 100 person-years (i.e., 0.91 new HIV cases would occur for every 100 people observed for 1 year). Increasing coverage to 20% reduced the incidence to 0.73 by 2034, which equals a 20% reduction (see Figure below). The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 17.3% and 21.8% at 10 years.
In Los Angeles, at 0% site coverage, the prevalence of HIV in 2034 was estimated to be 4.1%. Increasing site coverage to 20% reduced the prevalence to 3.7% by 2034. The estimated incidence of HIV at 0% site coverage in 2034 was 0.48 per 100 person-years. Increasing coverage to 20% reduced the incidence to 0.40 by 2034, which equals a 17% reduction. The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 12.9% and 17.7% at 10 years.
In San Diego, rates of HIV were projected to increase due to increases in risk and lack of treatment advances, yet declines were still observed. At 0% site coverage, the prevalence of HIV in 2034 was estimated to be 20.6%. Increasing site coverage to 20% reduced the prevalence to 14.9% by 2034. The estimated incidence of HIV at 0% site coverage in 2034 was 4.5 per 100 person-years. Increasing coverage to 20% reduced the incidence to 2.9 by 2034, which equals a 35% reduction. The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 30.8% and 32.1% at 10 years.
Hypothetical expansion of supervised consumption sites reduced hepatitis C infections
In San Francisco, at 0% site coverage, the prevalence of hepatitis C in 2034 was estimated to be 16.9%, which reflects a decline from 25.6% in 2024 due to treatment advances. Increasing site coverage to 20% resulted in even more of a decline, with a prevalence of 14.9% by 2034. The estimated incidence of hepatitis C at 0% site coverage in 2034 was 1.92 per 100 person-years. Increasing coverage to 20% reduced the incidence to 1.52 by 2034, which equals a 21% reduction (see Figure below). The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 22.6% and 28.3% at 10 years.
In Los Angeles, at 0% site coverage, the prevalence of hepatitis C in 2034 was estimated to be 24.2%, which reflects a decline from 2024 due to treatment advances. Increasing site coverage to 20% resulted in an even greater decline, with a prevalence of 20.8% by 2034. The estimated incidence of hepatitis C at 0% site coverage in 2034 was 4.08 per 100 person-years. Increasing coverage to 20% reduced the incidence to 3.00 by 2034, which equals a 26% reduction. The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 23.5% and 29.8% at 10 years.
In San Diego, at 0% site coverage, the prevalence of hepatitis C in 2034 was estimated to increase to 71.5%, given the high incidence in 2021. Increasing site coverage to 20% reduced the prevalence to 65.8% by 2034. The estimated incidence of hepatitis C at 0% site coverage in 2034 was 22.4 per 100 person-years. Increasing coverage to 20% reduced the incidence to 17.6 by 2034, which equals a 21% reduction. The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 23.3% and 24.3% at 10 years.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Scaling up supervised consumption site coverage resulted in reductions in the prevalence and incidence of both HIV and hepatitis C infections, as well as the percentage of new infections that could be prevented. These results suggest that supervised consumption sites may be an effective intervention for reducing infectious disease rates. Even in the context of treatment advances for hepatitis C, which would naturally result in a reduction of rates, these results demonstrated that scaling up supervised consumption sites may further reduce rates.
Of note, the statistical modeling used in the current study used estimates from existing epidemiological data to simulate what is statistically likely to happen over the next 10 years and is therefore considered hypothetical and demonstrates potential benefits, rather than a reflection of statistical associations found using data already collected. Nonetheless, the study has several strengths, including being one of the first to examine long-term public health benefits of supervised consumption sites in the US. The study was also able to compare counties with different rates of HIV and hepatitis C, which sheds light on the impact of the sites in counties that are experiencing different magnitudes of the problem.
One issue is cost-effectiveness of providing supervised consumption sites given that the main mechanism through which these positive effects are projected to occur is mostly by providing access to sterile syringes. While supervised consumption sites clearly provide other major benefits (i.e., preventing death form overdose), access to sterile syringes, specifically, might be possible much more cheaply and efficiently through other more ubiquitous venues, such as substance use disorder and infectious disease treatment venues or even primary care offices and pharmacies. Nevertheless, what is compelling here is that the potential increase of supervised consumption sites would not only likely decrease overdose deaths, but also additionally decrease infectious disease transmission that confer enormous long-term health and economic burdens.
The study was conducted based on epidemiological data from California, a progressive state that already has more favorable views towards harm reduction. Results may therefore not generalize to other US states with less favorable views or to other countries.
Due to a lack of data, the research team was not able to include demographic data in the modeling, such as age, sex, race/ethnicity, and sexual orientation. These variables could have affected the results since they can influence access to harm reduction strategies.
The study used statistical modeling to simulate what is statistically likely to happen over the next 10 years. Therefore, the results are based on a hypothetical scenario of scaling up supervised consumption sites and demonstrates potential benefits.
Estimates from the study have a wide range, which reflects uncertainty and the possibility of inaccurate results.
The researchers focused on the outcomes of HIV and hepatitis C only and did not consider other soft tissue infections that people who use drugs are at risk for. They also did not examine the costs vs. benefits to implement supervised consumption sites.
BOTTOM LINE
Hypothetical expansion of supervised consumption site coverage resulted in reductions in the prevalence and incidence of both HIV and hepatitis C infections, as well as the percentage of new infections that could be prevented. Statistical modeling in the current study employed estimates from existing epidemiological data to simulate what is statistically likely to happen over the next 10 years. Because studies of real-world outcomes in US supervised consumption sites are in the earliest stages while decisions around their criminal-legal status are at hand, computer simulation studies like these can help policy makers make critical decisions for their communities.
For individuals and families seeking recovery: This study found that expanding supervised consumption sites could result in fewer HIV and hepatitis C infections and prevent new infections. Accordingly, people who use drugs and have access to these sites may see similar benefits of using them. However, they are still unsanctioned or illegal in many US states. People without access to such programs who similarly try to engage in safer injection drug use practices and use sterile injection equipment could also reduce their risk of HIV and hepatitis C.
For treatment professionals and treatment systems: This study showed that hypothetically expanding supervised consumption sites resulted in fewer HIV and hepatitis C infections and prevented new infections by providing access to sterile syringes. Accordingly, treatment systems and professionals that similarly promote safer injection drug use practices and use of sterile injection equipment among people who inject drugs could see similar benefits of reductions in infectious diseases.
For scientists: Because the current study used simulation modeling to predict what is statistically likely to happen over the next 10 years, future research that examines the actual observed impact of supervised consumption sites as they become available in the US could corroborate the potential benefits demonstrated by hypothetical modeling studies such as the one summarize here. Additionally, future research that examines demographic differences would shed light on whether the outcomes generalize to different demographic groups. Finally, cost-benefit analyses would help us understand what the costs were to implement supervised consumption sites and what the savings could be in terms of the number of infections that were averted and the health care savings therein.
For policy makers: This study demonstrated that scaling up supervised consumption sites may potentially reduce rates of HIV and hepatitis C. However, supervised consumption sites are currently unsanctioned in the US. Because studies of real-world outcomes in US supervised consumption sites are in the earliest stages while decisions around their criminal-legal status are at hand, computer simulation studies like these can help policy makers make critical decisions for their communities. Additionally, policies that fund research to evaluate the impact of supervised consumption sites could further demonstrate the public health benefits of them, as well as the costs vs. benefits of implementation.
People who inject drugs face increased risks of contracting the blood-borne infectious disease HIV and hepatitis C from sharing contaminated syringes and other equipment. Recent outbreaks of HIV and hepatitis C in the United States highlight the magnitude of this problem and that solutions are needed to help address it.
Supervised consumption sites, also called overdose prevention sites or safe injection sites, are a type of harm reduction strategy that have been established not only to address the opioid overdose crisis, but also to reduce transmission of infectious diseases. Transmission risks are reduced at these sites by providing people who inject drugs sterile syringes, guidance about safer drug use, education about infectious disease, and testing for infectious diseases which can help with early identification and prevent disease spread. They may also offer other services, such as linkage to healthcare, addiction treatment, and other social services, drug checking, and distribution of naloxone.
A recent systematic review of research conducted in Canada, Australia, and Europe suggests that supervised consumption sites are associated with public health benefits. However, they are still unsanctioned in the United States, which limits what is understood about their impact in the US. Researchers in this study examined the potential impact of scaling up the implementation of supervised consumption sites on rates of infectious disease. Such research can shed light on the extent to which supervised consumption sites can be an effective intervention for reducing infectious disease rates.
HOW WAS THIS STUDY CONDUCTED?
The research team used a modeling approach where they simulated the potential impact of scaling up the implementation of supervised consumption sites on rates of HIV and hepatitis C among people who inject drugs. This model used data from 3 counties in California.
Co-infection of both HIV and hepatitis C, disease stage, and treatment was accounted for in the simulation model.
Of note, stages of HIV include: susceptible, acute, latent, pre-AIDS, and AIDS. People who are susceptible, or at risk for contracting the disease, can become infected and enter the acute stage, which is of short duration with high viral load and transmissibility. After the acute stage, people progress to the latent stage, which is of longer duration with a lower viral load and transmissibility. Without treatment, people can then progress to the pre-AIDS and AIDS stages. However, people can begin treatment with antiretroviral therapy during the latent, pre-AIDS, and AIDS stages, which can slow the disease progression and decrease transmission due to lower viral loads. As such, researchers stratified the model by: HIV disease stage, which included susceptible, acute, latent, pre-AIDS, AIDS; stage of HIV/AIDS and antiretroviral therapy, which included latent HIV on therapy, pre-AIDS on therapy, and AIDS on therapy; chronic hepatitis C infection or uninfected; and predicted use of supervised consumption sites or not. Transmission of HIV through sex and injection drug use was incorporated into the simulation model, while transmission of hepatitis C through injection drug use only was incorporated. This is because HIV is commonly transmitted both ways, while hepatitis C is more commonly transmitted through injection equipment sharing.
The model was calibrated to epidemiological data for San Francisco, Los Angeles, and San Diego based on availability of data in these three areas. Data were pulled from the National HIV Behavioral Surveillance surveys and longitudinal cohorts of people who inject drugs. While exact years for the data pulls varied by county, the model included the following variables for each county: HIV prevalence among people who inject drugs, chronic hepatitis C prevalence among people who inject drugs, proportion of HIV infections from sexual transmission, and antiretroviral therapy coverage among people who inject drugs and living with HIV. For San Diego only, hepatitis C incidence among people who inject drugs was also included, where the researchers simulated a higher hepatitis C transmission rate from 2015 and thereafter of 4-fold, given recent research showing increasing risks of transmission in this area.
Based on 2022 data from the National HIV Behavioral Surveillance survey, the researchers estimated that HIV prevalence among people who inject drugs was 10.1% for San Francisco, 4.5% for Los Angeles, and 3.0% for San Diego. Estimates of the proportion of HIV infections due to sexual transmission ranged from 62% for San Francisco to 77% for Los Angeles and San Diego. Estimates of the proportion of people who inject drugs and living with HIV on antiretroviral therapy were 92% for San Francisco, 80% for Los Angeles, and 67% for San Diego.
Estimates of chronic hepatitis C prevalence were derived for 2 time points, given recent advances in curative therapies. For San Francisco, estimates were 42% in 2015 and 35% in 2018. For Los Angeles, estimates were 48% in 2015 and 41% in 2018. For San Diego, data was not available from the National HIV Behavioral Surveillance survey and the researchers used data from a cohort study instead for 1 time point. The prevalence in 2021 for San Diego was estimated to be 30%.
When programming the model, the researchers assumed that people can start and stop using supervised consumption sites. People enter the model when they hypothetically begin injection drug use, and it was assumed these individuals were at risk for both HIV and hepatitis C infection. People hypothetically leave the model when they stop injecting drugs or die, either due to HIV or otherwise. It was also assumed that access to sites reduced syringe sharing among people who inject drugs by 83% and attending a site reduced the risk of drug-related mortality by 54%.
The researchers modeled scenarios where site coverage was scaled up from 0% of people who inject drugs to 20% starting in 2024 and how this would impact rates of HIV and Hepatitis C over 10 years in each county. The main outcomes of interest were HIV and hepatitis C prevalence and incidence. Prevalence refers to the total number of cases (both old and new) at a given point in time and is measured as percentage, while incidence refers to the number of the new cases that occur over a period of time and is measured as a rate in person-years (i.e., the number of people multiplied by the number of years they are observed). New rates of HIV and hepatitis C that could have been prevented in each county were also assessed at 5 years and 10 years following the scale up.
WHAT DID THIS STUDY FIND?
Models projected that expansion of supervised consumption site coverage would reduce HIV infections
In San Francisco, at 0% site coverage, the prevalence of HIV in 2034 was estimated to be 9.6%. Increasing site coverage to 20% reduced the prevalence to 8.6% by 2034. The estimated incidence of HIV at 0% site coverage in 2034 was 0.91 per 100 person-years (i.e., 0.91 new HIV cases would occur for every 100 people observed for 1 year). Increasing coverage to 20% reduced the incidence to 0.73 by 2034, which equals a 20% reduction (see Figure below). The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 17.3% and 21.8% at 10 years.
In Los Angeles, at 0% site coverage, the prevalence of HIV in 2034 was estimated to be 4.1%. Increasing site coverage to 20% reduced the prevalence to 3.7% by 2034. The estimated incidence of HIV at 0% site coverage in 2034 was 0.48 per 100 person-years. Increasing coverage to 20% reduced the incidence to 0.40 by 2034, which equals a 17% reduction. The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 12.9% and 17.7% at 10 years.
In San Diego, rates of HIV were projected to increase due to increases in risk and lack of treatment advances, yet declines were still observed. At 0% site coverage, the prevalence of HIV in 2034 was estimated to be 20.6%. Increasing site coverage to 20% reduced the prevalence to 14.9% by 2034. The estimated incidence of HIV at 0% site coverage in 2034 was 4.5 per 100 person-years. Increasing coverage to 20% reduced the incidence to 2.9 by 2034, which equals a 35% reduction. The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 30.8% and 32.1% at 10 years.
Hypothetical expansion of supervised consumption sites reduced hepatitis C infections
In San Francisco, at 0% site coverage, the prevalence of hepatitis C in 2034 was estimated to be 16.9%, which reflects a decline from 25.6% in 2024 due to treatment advances. Increasing site coverage to 20% resulted in even more of a decline, with a prevalence of 14.9% by 2034. The estimated incidence of hepatitis C at 0% site coverage in 2034 was 1.92 per 100 person-years. Increasing coverage to 20% reduced the incidence to 1.52 by 2034, which equals a 21% reduction (see Figure below). The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 22.6% and 28.3% at 10 years.
In Los Angeles, at 0% site coverage, the prevalence of hepatitis C in 2034 was estimated to be 24.2%, which reflects a decline from 2024 due to treatment advances. Increasing site coverage to 20% resulted in an even greater decline, with a prevalence of 20.8% by 2034. The estimated incidence of hepatitis C at 0% site coverage in 2034 was 4.08 per 100 person-years. Increasing coverage to 20% reduced the incidence to 3.00 by 2034, which equals a 26% reduction. The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 23.5% and 29.8% at 10 years.
In San Diego, at 0% site coverage, the prevalence of hepatitis C in 2034 was estimated to increase to 71.5%, given the high incidence in 2021. Increasing site coverage to 20% reduced the prevalence to 65.8% by 2034. The estimated incidence of hepatitis C at 0% site coverage in 2034 was 22.4 per 100 person-years. Increasing coverage to 20% reduced the incidence to 17.6 by 2034, which equals a 21% reduction. The percentage of new infections that could have been prevented with scaling up coverage to 20% at 5 years was 23.3% and 24.3% at 10 years.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Scaling up supervised consumption site coverage resulted in reductions in the prevalence and incidence of both HIV and hepatitis C infections, as well as the percentage of new infections that could be prevented. These results suggest that supervised consumption sites may be an effective intervention for reducing infectious disease rates. Even in the context of treatment advances for hepatitis C, which would naturally result in a reduction of rates, these results demonstrated that scaling up supervised consumption sites may further reduce rates.
Of note, the statistical modeling used in the current study used estimates from existing epidemiological data to simulate what is statistically likely to happen over the next 10 years and is therefore considered hypothetical and demonstrates potential benefits, rather than a reflection of statistical associations found using data already collected. Nonetheless, the study has several strengths, including being one of the first to examine long-term public health benefits of supervised consumption sites in the US. The study was also able to compare counties with different rates of HIV and hepatitis C, which sheds light on the impact of the sites in counties that are experiencing different magnitudes of the problem.
One issue is cost-effectiveness of providing supervised consumption sites given that the main mechanism through which these positive effects are projected to occur is mostly by providing access to sterile syringes. While supervised consumption sites clearly provide other major benefits (i.e., preventing death form overdose), access to sterile syringes, specifically, might be possible much more cheaply and efficiently through other more ubiquitous venues, such as substance use disorder and infectious disease treatment venues or even primary care offices and pharmacies. Nevertheless, what is compelling here is that the potential increase of supervised consumption sites would not only likely decrease overdose deaths, but also additionally decrease infectious disease transmission that confer enormous long-term health and economic burdens.
The study was conducted based on epidemiological data from California, a progressive state that already has more favorable views towards harm reduction. Results may therefore not generalize to other US states with less favorable views or to other countries.
Due to a lack of data, the research team was not able to include demographic data in the modeling, such as age, sex, race/ethnicity, and sexual orientation. These variables could have affected the results since they can influence access to harm reduction strategies.
The study used statistical modeling to simulate what is statistically likely to happen over the next 10 years. Therefore, the results are based on a hypothetical scenario of scaling up supervised consumption sites and demonstrates potential benefits.
Estimates from the study have a wide range, which reflects uncertainty and the possibility of inaccurate results.
The researchers focused on the outcomes of HIV and hepatitis C only and did not consider other soft tissue infections that people who use drugs are at risk for. They also did not examine the costs vs. benefits to implement supervised consumption sites.
BOTTOM LINE
Hypothetical expansion of supervised consumption site coverage resulted in reductions in the prevalence and incidence of both HIV and hepatitis C infections, as well as the percentage of new infections that could be prevented. Statistical modeling in the current study employed estimates from existing epidemiological data to simulate what is statistically likely to happen over the next 10 years. Because studies of real-world outcomes in US supervised consumption sites are in the earliest stages while decisions around their criminal-legal status are at hand, computer simulation studies like these can help policy makers make critical decisions for their communities.
For individuals and families seeking recovery: This study found that expanding supervised consumption sites could result in fewer HIV and hepatitis C infections and prevent new infections. Accordingly, people who use drugs and have access to these sites may see similar benefits of using them. However, they are still unsanctioned or illegal in many US states. People without access to such programs who similarly try to engage in safer injection drug use practices and use sterile injection equipment could also reduce their risk of HIV and hepatitis C.
For treatment professionals and treatment systems: This study showed that hypothetically expanding supervised consumption sites resulted in fewer HIV and hepatitis C infections and prevented new infections by providing access to sterile syringes. Accordingly, treatment systems and professionals that similarly promote safer injection drug use practices and use of sterile injection equipment among people who inject drugs could see similar benefits of reductions in infectious diseases.
For scientists: Because the current study used simulation modeling to predict what is statistically likely to happen over the next 10 years, future research that examines the actual observed impact of supervised consumption sites as they become available in the US could corroborate the potential benefits demonstrated by hypothetical modeling studies such as the one summarize here. Additionally, future research that examines demographic differences would shed light on whether the outcomes generalize to different demographic groups. Finally, cost-benefit analyses would help us understand what the costs were to implement supervised consumption sites and what the savings could be in terms of the number of infections that were averted and the health care savings therein.
For policy makers: This study demonstrated that scaling up supervised consumption sites may potentially reduce rates of HIV and hepatitis C. However, supervised consumption sites are currently unsanctioned in the US. Because studies of real-world outcomes in US supervised consumption sites are in the earliest stages while decisions around their criminal-legal status are at hand, computer simulation studies like these can help policy makers make critical decisions for their communities. Additionally, policies that fund research to evaluate the impact of supervised consumption sites could further demonstrate the public health benefits of them, as well as the costs vs. benefits of implementation.