Can you just cut back rather than stop cocaine use and have good outcomes?
For some individuals with substance use disorder, reducing alcohol and other drug use may confer some of the psychological and functional benefits also associated with stopping completely. The researchers in this study examined the effects of different cocaine use outcomes over time on drug use consequences and other aspects of functioning.
Substance use disorder treatments have historically encouraged, or in some cases required, goals of abstinence from alcohol and other drugs. While complete cessation is typically the optimal goal and associated with the highest levels of functioning, reduced use can also lead to some improvement. While much research to date supporting this idea has focused on alcohol (for example), some work has also begun to explore how reductions in cocaine use among people with cocaine use disorder may also have benefits.
For instance, one study pooling data from 7 clinical trials found that less cocaine use frequency in the final month of cocaine use disorder treatment was associated with better overall functioning over follow-up, especially for individuals who stopped cocaine use completely or used only occasionally. Another study found that reducing from high-frequency to low-frequency cocaine use during treatment was associated with improvements similar to total abstinence in psychological and social functioning at 12-month follow-up for those able to achieve that lower level of use.
In this study, the researchers extended this work to better understand how different degrees of cocaine use reduction affect long-term outcomes in individuals receiving treatment and continuing care for cocaine use disorder.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of 2 randomized clinical trials of outpatient treatment for substance use disorder that included assessments of cocaine use, and addiction problem severity at baseline, and at 12- and 24-month follow-up, to examine associations between change in cocaine use frequency and related problems.
Both clinical trials were conducted in the early-to-mid 2000s and included substance use disorder outpatient care as well as continuing care in the form of relapse prevention, and/or telephone monitoring and ongoing support. The researchers’ combined study sample included 445 clinical trial participants with lifetime cocaine use disorder, and at least 1 day of cocaine use just prior to commencing treatment.
Cocaine use was assessed for the 30 days prior to beginning the index treatment episode (i.e., study baseline), and again at 12-, and 24-month follow-ups. At each time-point, participants’ cocaine use status was coded as, 1) abstinent, 2) low-frequency use (1–4 days of use in the past 30 days), or 3) high-frequency use (5+ days of use in the past 30 days).
Participants’ change in cocaine use from baseline to 12-month follow-up was then coded as, 1) no change in cocaine use frequency or an increase in cocaine use frequency, 2) a 1-level reduction in cocaine use frequency (i.e., high to low-frequency use or low-frequency use to abstinence), or 3) a 2-level reduction in cocaine use frequency (i.e., high-frequency use to abstinence).
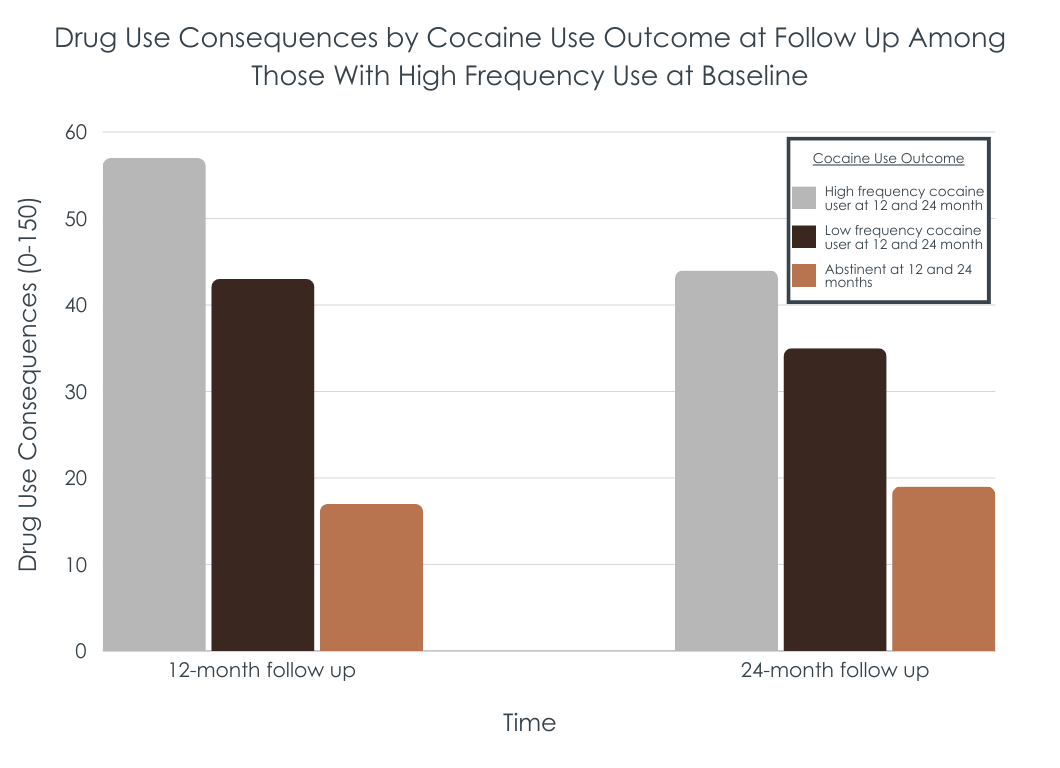
Study outcomes included alcohol and other drug problem severity across the following domains: 1) alcohol and other drug use, 2) drug use consequences measured with The Inventory of Drug Use Consequences, 3) medical, 4) employment, 5) legal, 6) family/social, and 7) psychological.
The study sample was 77% male and an average of 42 years of age, with 87% of participants identifying as Black, 11% as White, 1% as Puerto Rican, and less than 1% as Other Hispanic or Native American.
At baseline (i.e., before beginning treatment), 83% of participants reported high-frequency cocaine use (i.e., 5+ past-month days cocaine use) and 17% reported low-frequency use (i.e., 1-4 past-month days cocaine use).
WHAT DID THIS STUDY FIND?
Most participants reduced or stopped cocaine use
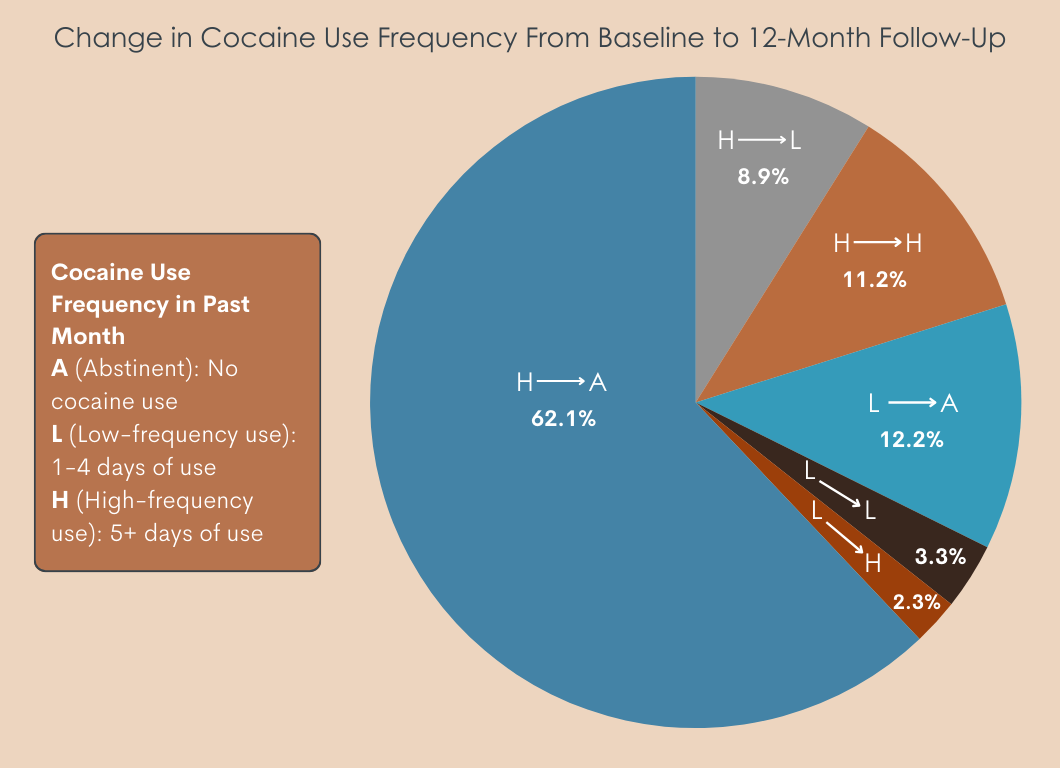
The majority of study participants began the study with high-frequency cocaine use (83%). Of the total study sample, 62% of participants endorsed high-frequency cocaine use at baseline and then cocaine abstinence at 12-month follow-up, reflecting a 2-level reduction in use. A smaller group endorsed a 1-level reduction from high- to low-frequency use (9%).
Approximately 18% of the study sample endorsed low-frequency use at baseline: by 12-month follow-up, 2% increased to high-frequency use, 3% remained at low-frequency use, while 12% were abstinent at 12-month follow-up.
Among participants who reported cocaine abstinence at 12-month follow-up, 84% were still abstinent at 24 months, 7% had transitioned to low-frequency use, and 9% had transitioned to high-frequency use.
Any reduction in cocaine use frequency was associated with benefits
At least a 1-level reduction in cocaine use from baseline to 12-month follow-up was associated with less alcohol and other drug use and fewer drug use consequences and legal problems, relative to no change or an increase in cocaine use frequency. With the exception of fewer legal problems, these benefits of reduced cocaine use were also present at 24-month follow-up.
Abstinence was associated with the greatest benefit
As expected, participants who reduced more, such as by 2 levels (i.e., from high-frequency use to abstinent) had less alcohol and other drug use, drug use consequences, and legal problems at 12-month follow-up, relative to those who reported no change or an increase in their cocaine use frequency. In addition, relative to those reducing 1 level (e.g., from high-frequency use to low-frequency use), abstinent individuals had less alcohol and other drug use, and drug use consequences, though these differences were no longer apparent at 24-month follow-up. However, at 24-month follow-up, compared to those with no change or increase, the participants endorsing abstinence had fewer drug use consequences while the low-frequency group did not.
Notably, there were no associations between reducing or quitting cocaine use and employment, medical, psychological, or social problem severity at 12- or 24-month follow-up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
For some individuals—especially those with less severe substance use disorder—significantly reducing substance use can confer many of the mental and physical health benefits typically associated with abstinence. Most studies on this topic to date, however, have focused on alcohol consumption in people with alcohol use disorder. This study builds on a smaller body of work suggesting that reductions in cocaine use frequency in individuals with cocaine use disorder is also associated with benefits. Based on these findings and previous studies (see here and here), it is likely that for some individuals with cocaine use disorder, tangible benefits can be reaped by reducing the frequency of use.
At the same time, the researchers in this study also found that stopping cocaine use altogether was associated with the greatest reductions in alcohol and other drug use and related consequences. These alcohol and other drug use consequences include, for example, failing to do what is expected and doing things impulsively that are later regretted. While any meaningful reduction in cocaine use may confer benefits, based on these findings, making large reductions or stopping altogether will likely confer the most benefits in terms of reducing substance use related problems. The fact alcohol use was lowest in cocaine abstainers suggests there also may be some cross-substance benefits.
It was notable, however, that regardless of whether participants changed their cocaine use, employment, medical, psychological, or social problem severity did not markedly change over follow-up. This was even true when comparing those with cocaine abstinence to those who maintained high levels of use. This suggests the study sample was experiencing significant psychosocial challenges that were perhaps countering potential benefits associated with reducing or stopping cocaine use. This may be linked to the fact that the study sample was predominantly Black. Previous work has shown that while all people in substance use disorder recovery struggle with employment and health inequities relative to the general population, people who identify as Black are especially disadvantaged (see examples here and here), suggesting resources including but not limited to treatment are needed to help this group build and sustain recovery capital over time.
Cocaine use was assessed for 30-day periods prior to baseline and 12- and 24-month follow-up. Though this is a common way to measure substance use over time, it is likely that many participants’ cocaine use patterns varied over the 1-year follow-up periods. For such participants, assessed cocaine use frequency would not fully characterize their use patterns over the study monitoring period.
This study focused on cocaine use in people with cocaine use disorder. While use of drugs other than cocaine was included as an outcome measure, it was not considered as a predictor of substance use problem severity and life satisfaction. For some participants, non-cocaine substance use (e.g., opioid use) could have contributed to the substance use related problems measured in this study but analyses did not account for this possibility.
The sample was majority Black individuals and generalizations of study findings to other racial/ethnic groups is unknown.
BOTTOM LINE
As might be expected, for people with cocaine use disorder, reduced cocaine use frequency was associated with reductions in substance use related problems. While any meaningful reduction in use frequency appeared to confer benefits, greater reductions and abstinence conferred the most benefit.
For individuals and families seeking recovery: For individuals with cocaine use disorder, reducing the frequency of cocaine use will likely lead to reductions in related problems, however, major reductions in use frequency or abstinence are likely to produce the most benefits. For many individuals, maintaining low-frequency use without returning to high-frequency use and its related problems can be very challenging. For such people, abstinence may be the best option.
For treatment professionals and treatment systems: For individuals with cocaine use disorder, reducing the frequency of cocaine use will likely lead to reductions in related problems, however, major reductions in use frequency or abstinence are likely to produce the most benefits. Programs that provide care for individuals with a reduced substance use goal (versus abstinence) have the potential to engage many individuals in treatment who otherwise would not seek care, while also helping such individuals achieve reductions in substance use related problems. Given that best practice recommendations may emphasize abstinence, programs need not require abstinence in order to encourage it.
For scientists: More research is needed to properly understand for whom and under what conditions reductions in substance use (versus abstinence) is likely to confer reductions in substance use problem severity. The role of race/ethnicity will be particularly important to explore. More work is also needed to understand how reductions in the use of one drug may lead to changes in the use of other drugs, and how this may affect quality of life and well-being.
For policy makers: Supporting non-abstinence-based substance use disorder treatment programs and organizations may improve the public health burden associated with substance use disorder by helping individuals with moderation substance use goals engage with treatment and reduce substance use related problems. Strategies that promote multiple pathways to recovery may strike the balance between recommended abstinence while engaging people with a range of substance use goals in treatment and recovery support settings.
Substance use disorder treatments have historically encouraged, or in some cases required, goals of abstinence from alcohol and other drugs. While complete cessation is typically the optimal goal and associated with the highest levels of functioning, reduced use can also lead to some improvement. While much research to date supporting this idea has focused on alcohol (for example), some work has also begun to explore how reductions in cocaine use among people with cocaine use disorder may also have benefits.
For instance, one study pooling data from 7 clinical trials found that less cocaine use frequency in the final month of cocaine use disorder treatment was associated with better overall functioning over follow-up, especially for individuals who stopped cocaine use completely or used only occasionally. Another study found that reducing from high-frequency to low-frequency cocaine use during treatment was associated with improvements similar to total abstinence in psychological and social functioning at 12-month follow-up for those able to achieve that lower level of use.
In this study, the researchers extended this work to better understand how different degrees of cocaine use reduction affect long-term outcomes in individuals receiving treatment and continuing care for cocaine use disorder.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of 2 randomized clinical trials of outpatient treatment for substance use disorder that included assessments of cocaine use, and addiction problem severity at baseline, and at 12- and 24-month follow-up, to examine associations between change in cocaine use frequency and related problems.
Both clinical trials were conducted in the early-to-mid 2000s and included substance use disorder outpatient care as well as continuing care in the form of relapse prevention, and/or telephone monitoring and ongoing support. The researchers’ combined study sample included 445 clinical trial participants with lifetime cocaine use disorder, and at least 1 day of cocaine use just prior to commencing treatment.
Cocaine use was assessed for the 30 days prior to beginning the index treatment episode (i.e., study baseline), and again at 12-, and 24-month follow-ups. At each time-point, participants’ cocaine use status was coded as, 1) abstinent, 2) low-frequency use (1–4 days of use in the past 30 days), or 3) high-frequency use (5+ days of use in the past 30 days).
Participants’ change in cocaine use from baseline to 12-month follow-up was then coded as, 1) no change in cocaine use frequency or an increase in cocaine use frequency, 2) a 1-level reduction in cocaine use frequency (i.e., high to low-frequency use or low-frequency use to abstinence), or 3) a 2-level reduction in cocaine use frequency (i.e., high-frequency use to abstinence).
Study outcomes included alcohol and other drug problem severity across the following domains: 1) alcohol and other drug use, 2) drug use consequences measured with The Inventory of Drug Use Consequences, 3) medical, 4) employment, 5) legal, 6) family/social, and 7) psychological.
The study sample was 77% male and an average of 42 years of age, with 87% of participants identifying as Black, 11% as White, 1% as Puerto Rican, and less than 1% as Other Hispanic or Native American.
At baseline (i.e., before beginning treatment), 83% of participants reported high-frequency cocaine use (i.e., 5+ past-month days cocaine use) and 17% reported low-frequency use (i.e., 1-4 past-month days cocaine use).
WHAT DID THIS STUDY FIND?
Most participants reduced or stopped cocaine use
The majority of study participants began the study with high-frequency cocaine use (83%). Of the total study sample, 62% of participants endorsed high-frequency cocaine use at baseline and then cocaine abstinence at 12-month follow-up, reflecting a 2-level reduction in use. A smaller group endorsed a 1-level reduction from high- to low-frequency use (9%).
Approximately 18% of the study sample endorsed low-frequency use at baseline: by 12-month follow-up, 2% increased to high-frequency use, 3% remained at low-frequency use, while 12% were abstinent at 12-month follow-up.
Among participants who reported cocaine abstinence at 12-month follow-up, 84% were still abstinent at 24 months, 7% had transitioned to low-frequency use, and 9% had transitioned to high-frequency use.
Any reduction in cocaine use frequency was associated with benefits
At least a 1-level reduction in cocaine use from baseline to 12-month follow-up was associated with less alcohol and other drug use and fewer drug use consequences and legal problems, relative to no change or an increase in cocaine use frequency. With the exception of fewer legal problems, these benefits of reduced cocaine use were also present at 24-month follow-up.
Abstinence was associated with the greatest benefit
As expected, participants who reduced more, such as by 2 levels (i.e., from high-frequency use to abstinent) had less alcohol and other drug use, drug use consequences, and legal problems at 12-month follow-up, relative to those who reported no change or an increase in their cocaine use frequency. In addition, relative to those reducing 1 level (e.g., from high-frequency use to low-frequency use), abstinent individuals had less alcohol and other drug use, and drug use consequences, though these differences were no longer apparent at 24-month follow-up. However, at 24-month follow-up, compared to those with no change or increase, the participants endorsing abstinence had fewer drug use consequences while the low-frequency group did not.
Notably, there were no associations between reducing or quitting cocaine use and employment, medical, psychological, or social problem severity at 12- or 24-month follow-up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
For some individuals—especially those with less severe substance use disorder—significantly reducing substance use can confer many of the mental and physical health benefits typically associated with abstinence. Most studies on this topic to date, however, have focused on alcohol consumption in people with alcohol use disorder. This study builds on a smaller body of work suggesting that reductions in cocaine use frequency in individuals with cocaine use disorder is also associated with benefits. Based on these findings and previous studies (see here and here), it is likely that for some individuals with cocaine use disorder, tangible benefits can be reaped by reducing the frequency of use.
At the same time, the researchers in this study also found that stopping cocaine use altogether was associated with the greatest reductions in alcohol and other drug use and related consequences. These alcohol and other drug use consequences include, for example, failing to do what is expected and doing things impulsively that are later regretted. While any meaningful reduction in cocaine use may confer benefits, based on these findings, making large reductions or stopping altogether will likely confer the most benefits in terms of reducing substance use related problems. The fact alcohol use was lowest in cocaine abstainers suggests there also may be some cross-substance benefits.
It was notable, however, that regardless of whether participants changed their cocaine use, employment, medical, psychological, or social problem severity did not markedly change over follow-up. This was even true when comparing those with cocaine abstinence to those who maintained high levels of use. This suggests the study sample was experiencing significant psychosocial challenges that were perhaps countering potential benefits associated with reducing or stopping cocaine use. This may be linked to the fact that the study sample was predominantly Black. Previous work has shown that while all people in substance use disorder recovery struggle with employment and health inequities relative to the general population, people who identify as Black are especially disadvantaged (see examples here and here), suggesting resources including but not limited to treatment are needed to help this group build and sustain recovery capital over time.
Cocaine use was assessed for 30-day periods prior to baseline and 12- and 24-month follow-up. Though this is a common way to measure substance use over time, it is likely that many participants’ cocaine use patterns varied over the 1-year follow-up periods. For such participants, assessed cocaine use frequency would not fully characterize their use patterns over the study monitoring period.
This study focused on cocaine use in people with cocaine use disorder. While use of drugs other than cocaine was included as an outcome measure, it was not considered as a predictor of substance use problem severity and life satisfaction. For some participants, non-cocaine substance use (e.g., opioid use) could have contributed to the substance use related problems measured in this study but analyses did not account for this possibility.
The sample was majority Black individuals and generalizations of study findings to other racial/ethnic groups is unknown.
BOTTOM LINE
As might be expected, for people with cocaine use disorder, reduced cocaine use frequency was associated with reductions in substance use related problems. While any meaningful reduction in use frequency appeared to confer benefits, greater reductions and abstinence conferred the most benefit.
For individuals and families seeking recovery: For individuals with cocaine use disorder, reducing the frequency of cocaine use will likely lead to reductions in related problems, however, major reductions in use frequency or abstinence are likely to produce the most benefits. For many individuals, maintaining low-frequency use without returning to high-frequency use and its related problems can be very challenging. For such people, abstinence may be the best option.
For treatment professionals and treatment systems: For individuals with cocaine use disorder, reducing the frequency of cocaine use will likely lead to reductions in related problems, however, major reductions in use frequency or abstinence are likely to produce the most benefits. Programs that provide care for individuals with a reduced substance use goal (versus abstinence) have the potential to engage many individuals in treatment who otherwise would not seek care, while also helping such individuals achieve reductions in substance use related problems. Given that best practice recommendations may emphasize abstinence, programs need not require abstinence in order to encourage it.
For scientists: More research is needed to properly understand for whom and under what conditions reductions in substance use (versus abstinence) is likely to confer reductions in substance use problem severity. The role of race/ethnicity will be particularly important to explore. More work is also needed to understand how reductions in the use of one drug may lead to changes in the use of other drugs, and how this may affect quality of life and well-being.
For policy makers: Supporting non-abstinence-based substance use disorder treatment programs and organizations may improve the public health burden associated with substance use disorder by helping individuals with moderation substance use goals engage with treatment and reduce substance use related problems. Strategies that promote multiple pathways to recovery may strike the balance between recommended abstinence while engaging people with a range of substance use goals in treatment and recovery support settings.
Substance use disorder treatments have historically encouraged, or in some cases required, goals of abstinence from alcohol and other drugs. While complete cessation is typically the optimal goal and associated with the highest levels of functioning, reduced use can also lead to some improvement. While much research to date supporting this idea has focused on alcohol (for example), some work has also begun to explore how reductions in cocaine use among people with cocaine use disorder may also have benefits.
For instance, one study pooling data from 7 clinical trials found that less cocaine use frequency in the final month of cocaine use disorder treatment was associated with better overall functioning over follow-up, especially for individuals who stopped cocaine use completely or used only occasionally. Another study found that reducing from high-frequency to low-frequency cocaine use during treatment was associated with improvements similar to total abstinence in psychological and social functioning at 12-month follow-up for those able to achieve that lower level of use.
In this study, the researchers extended this work to better understand how different degrees of cocaine use reduction affect long-term outcomes in individuals receiving treatment and continuing care for cocaine use disorder.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of 2 randomized clinical trials of outpatient treatment for substance use disorder that included assessments of cocaine use, and addiction problem severity at baseline, and at 12- and 24-month follow-up, to examine associations between change in cocaine use frequency and related problems.
Both clinical trials were conducted in the early-to-mid 2000s and included substance use disorder outpatient care as well as continuing care in the form of relapse prevention, and/or telephone monitoring and ongoing support. The researchers’ combined study sample included 445 clinical trial participants with lifetime cocaine use disorder, and at least 1 day of cocaine use just prior to commencing treatment.
Cocaine use was assessed for the 30 days prior to beginning the index treatment episode (i.e., study baseline), and again at 12-, and 24-month follow-ups. At each time-point, participants’ cocaine use status was coded as, 1) abstinent, 2) low-frequency use (1–4 days of use in the past 30 days), or 3) high-frequency use (5+ days of use in the past 30 days).
Participants’ change in cocaine use from baseline to 12-month follow-up was then coded as, 1) no change in cocaine use frequency or an increase in cocaine use frequency, 2) a 1-level reduction in cocaine use frequency (i.e., high to low-frequency use or low-frequency use to abstinence), or 3) a 2-level reduction in cocaine use frequency (i.e., high-frequency use to abstinence).
Study outcomes included alcohol and other drug problem severity across the following domains: 1) alcohol and other drug use, 2) drug use consequences measured with The Inventory of Drug Use Consequences, 3) medical, 4) employment, 5) legal, 6) family/social, and 7) psychological.
The study sample was 77% male and an average of 42 years of age, with 87% of participants identifying as Black, 11% as White, 1% as Puerto Rican, and less than 1% as Other Hispanic or Native American.
At baseline (i.e., before beginning treatment), 83% of participants reported high-frequency cocaine use (i.e., 5+ past-month days cocaine use) and 17% reported low-frequency use (i.e., 1-4 past-month days cocaine use).
WHAT DID THIS STUDY FIND?
Most participants reduced or stopped cocaine use
The majority of study participants began the study with high-frequency cocaine use (83%). Of the total study sample, 62% of participants endorsed high-frequency cocaine use at baseline and then cocaine abstinence at 12-month follow-up, reflecting a 2-level reduction in use. A smaller group endorsed a 1-level reduction from high- to low-frequency use (9%).
Approximately 18% of the study sample endorsed low-frequency use at baseline: by 12-month follow-up, 2% increased to high-frequency use, 3% remained at low-frequency use, while 12% were abstinent at 12-month follow-up.
Among participants who reported cocaine abstinence at 12-month follow-up, 84% were still abstinent at 24 months, 7% had transitioned to low-frequency use, and 9% had transitioned to high-frequency use.
Any reduction in cocaine use frequency was associated with benefits
At least a 1-level reduction in cocaine use from baseline to 12-month follow-up was associated with less alcohol and other drug use and fewer drug use consequences and legal problems, relative to no change or an increase in cocaine use frequency. With the exception of fewer legal problems, these benefits of reduced cocaine use were also present at 24-month follow-up.
Abstinence was associated with the greatest benefit
As expected, participants who reduced more, such as by 2 levels (i.e., from high-frequency use to abstinent) had less alcohol and other drug use, drug use consequences, and legal problems at 12-month follow-up, relative to those who reported no change or an increase in their cocaine use frequency. In addition, relative to those reducing 1 level (e.g., from high-frequency use to low-frequency use), abstinent individuals had less alcohol and other drug use, and drug use consequences, though these differences were no longer apparent at 24-month follow-up. However, at 24-month follow-up, compared to those with no change or increase, the participants endorsing abstinence had fewer drug use consequences while the low-frequency group did not.
Notably, there were no associations between reducing or quitting cocaine use and employment, medical, psychological, or social problem severity at 12- or 24-month follow-up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
For some individuals—especially those with less severe substance use disorder—significantly reducing substance use can confer many of the mental and physical health benefits typically associated with abstinence. Most studies on this topic to date, however, have focused on alcohol consumption in people with alcohol use disorder. This study builds on a smaller body of work suggesting that reductions in cocaine use frequency in individuals with cocaine use disorder is also associated with benefits. Based on these findings and previous studies (see here and here), it is likely that for some individuals with cocaine use disorder, tangible benefits can be reaped by reducing the frequency of use.
At the same time, the researchers in this study also found that stopping cocaine use altogether was associated with the greatest reductions in alcohol and other drug use and related consequences. These alcohol and other drug use consequences include, for example, failing to do what is expected and doing things impulsively that are later regretted. While any meaningful reduction in cocaine use may confer benefits, based on these findings, making large reductions or stopping altogether will likely confer the most benefits in terms of reducing substance use related problems. The fact alcohol use was lowest in cocaine abstainers suggests there also may be some cross-substance benefits.
It was notable, however, that regardless of whether participants changed their cocaine use, employment, medical, psychological, or social problem severity did not markedly change over follow-up. This was even true when comparing those with cocaine abstinence to those who maintained high levels of use. This suggests the study sample was experiencing significant psychosocial challenges that were perhaps countering potential benefits associated with reducing or stopping cocaine use. This may be linked to the fact that the study sample was predominantly Black. Previous work has shown that while all people in substance use disorder recovery struggle with employment and health inequities relative to the general population, people who identify as Black are especially disadvantaged (see examples here and here), suggesting resources including but not limited to treatment are needed to help this group build and sustain recovery capital over time.
Cocaine use was assessed for 30-day periods prior to baseline and 12- and 24-month follow-up. Though this is a common way to measure substance use over time, it is likely that many participants’ cocaine use patterns varied over the 1-year follow-up periods. For such participants, assessed cocaine use frequency would not fully characterize their use patterns over the study monitoring period.
This study focused on cocaine use in people with cocaine use disorder. While use of drugs other than cocaine was included as an outcome measure, it was not considered as a predictor of substance use problem severity and life satisfaction. For some participants, non-cocaine substance use (e.g., opioid use) could have contributed to the substance use related problems measured in this study but analyses did not account for this possibility.
The sample was majority Black individuals and generalizations of study findings to other racial/ethnic groups is unknown.
BOTTOM LINE
As might be expected, for people with cocaine use disorder, reduced cocaine use frequency was associated with reductions in substance use related problems. While any meaningful reduction in use frequency appeared to confer benefits, greater reductions and abstinence conferred the most benefit.
For individuals and families seeking recovery: For individuals with cocaine use disorder, reducing the frequency of cocaine use will likely lead to reductions in related problems, however, major reductions in use frequency or abstinence are likely to produce the most benefits. For many individuals, maintaining low-frequency use without returning to high-frequency use and its related problems can be very challenging. For such people, abstinence may be the best option.
For treatment professionals and treatment systems: For individuals with cocaine use disorder, reducing the frequency of cocaine use will likely lead to reductions in related problems, however, major reductions in use frequency or abstinence are likely to produce the most benefits. Programs that provide care for individuals with a reduced substance use goal (versus abstinence) have the potential to engage many individuals in treatment who otherwise would not seek care, while also helping such individuals achieve reductions in substance use related problems. Given that best practice recommendations may emphasize abstinence, programs need not require abstinence in order to encourage it.
For scientists: More research is needed to properly understand for whom and under what conditions reductions in substance use (versus abstinence) is likely to confer reductions in substance use problem severity. The role of race/ethnicity will be particularly important to explore. More work is also needed to understand how reductions in the use of one drug may lead to changes in the use of other drugs, and how this may affect quality of life and well-being.
For policy makers: Supporting non-abstinence-based substance use disorder treatment programs and organizations may improve the public health burden associated with substance use disorder by helping individuals with moderation substance use goals engage with treatment and reduce substance use related problems. Strategies that promote multiple pathways to recovery may strike the balance between recommended abstinence while engaging people with a range of substance use goals in treatment and recovery support settings.