Civil commitment to treatment associated with reduced healthcare utilization that is on par with more voluntary treatment
Civil commitment to substance use disorder treatment is a contentious issue and the evidence for this intervention is mixed. In this study, researchers examined the effect of involuntary treatment for individuals with severe alcohol use disorder on subsequent healthcare utilization.
Involuntary treatment, also known as civil commitment, is a legal mechanism that allows family members, healthcare professionals, and others to seek court-mandated treatment for an individual who poses a significant threat of harming themselves or others, but is unwilling to attend treatment. Involuntary treatment is sometimes used for those with substance use disorders, for example if a person is at considerable risk for overdose. This form of treatment is different than coercive treatment, such as drug courts, where individuals have a choice, albeit sometimes a very narrow one between treatment and incarceration. The role of involuntary treatment in substance use disorder is a contentious issue. In addition to potentially violating an individual’s rights through infringement of autonomy and privacy, evidence for involuntary commitments is mixed with some studies suggesting potential harms. On the other hand, it may save someone’s life and the lives of others, especially for those at the most severe levels of impairment. There is stronger empirical evidence that certain types of involuntary treatment can benefit health and safety for individuals with other forms of severe mental illness.
Given the dearth of empirical evidence on whether involuntary treatment actual helps individuals with substance use disorders, more research is needed, especially in settings outside of the criminal justice system. A statute in New South Wales, Australia allows for involuntary treatment in special circumstances as an approach of last resort for substance use disorder. In a previous evaluation study of this statute, researchers found that, although this form of treatment improved measured outcomes up to 1 year after treatment completion, this improvement did not differ from a comparison group suggesting similar outcomes relative to treatment as usual. In the current study, researchers examined the differences between involuntary and voluntary treatment for alcohol use disorder on subsequent healthcare utilization measures.
HOW WAS THIS STUDY CONDUCTED?
This a retrospective cohort study using linked administrative databases to measure the change in healthcare utilization measures before and after involuntary treatment for alcohol use disorder compared with a matched control group that underwent voluntary treatment.
The study took place in New South Wales, Australia from 2012 to 2018. The Involuntary Drug and Alcohol Program began in 2012 under a statute that allowed for involuntary treatment of substance use disorders as a last resort when certain conditions were met. There had to be robust evidence of:
Severe substance use disorder
Care or treatment necessary to protect from serious harm
Likely to benefit from treatment for substance use disorder and has previously refused treatment
No other appropriate and less restrictive means was available
Involuntary treatment consisted of medically supervised alcohol detoxification, comprehensive assessment, rehabilitation, and support for up to 28 days with voluntary aftercare for up to 6 months. Treatment took place in a locked ward of 1 of 2 hospitals in New South Wales.
Researchers limited the sample to individuals who identified alcohol as the principal drug of concern resulting in 231 eligible individuals between 2012 and 2018. These individuals were identified through the New South Wales Minimum Data Set for Drug and Alcohol Treatment Services. Since some individuals had more than 1 episode of involuntary treatment in the data set, the first episode of care was used for this study, called the index treatment episode.
The variables of interest were changes in 2 healthcare utilization measures: the change in the number of emergency department visits recorded in the 12 months prior to the index treatment episode and in the 12 months after the index treatment was completed, which was identified from the New South Wales Emergency Department Data Collection, and the change in the number of unplanned hospital admissions recorded in the 12 months prior to the index treatment episode and in the 12 months after the index treatment was completed, which was identified from the New South Wales Admitted Patient Data Collection.
A comparison group of individuals receiving voluntary treatment was constructed to compare the outcomes with involuntarily committed and treated individuals. Nearly 5000 individuals were identified as having a medical condition that resulted from harmful use of alcohol and received at least 1 of 3 forms of voluntary treatment consisting of medically supervised detoxification, rehabilitation, and/or pharmacotherapies for alcohol use disorder. Then, researchers used a statistical technique to identify 231 individuals in the control group that were most similar to the 231 individuals in the involuntary treatment group based on the pre-treatment variables of interest (emergency department visits and unplanned hospital admissions). Analyses also controlled for demographic characteristics as well as a summary variable capturing clinical complexity based on number of medical comorbidities, co-occurring psychiatric disorder, and social comorbidity (e.g., employment status) to try and equate the groups as closely as possible.
There were minimal demographic and clinical differences between the treatment and the comparison group. The only statistical differences were that there was a higher proportion of males in the voluntarily treated (control) group, and there were a higher proportion of individuals with no previous alcohol treatment episodes and more than 5 previous alcohol episodes in the involuntarily committed treatment group.
WHAT DID THIS STUDY FIND?
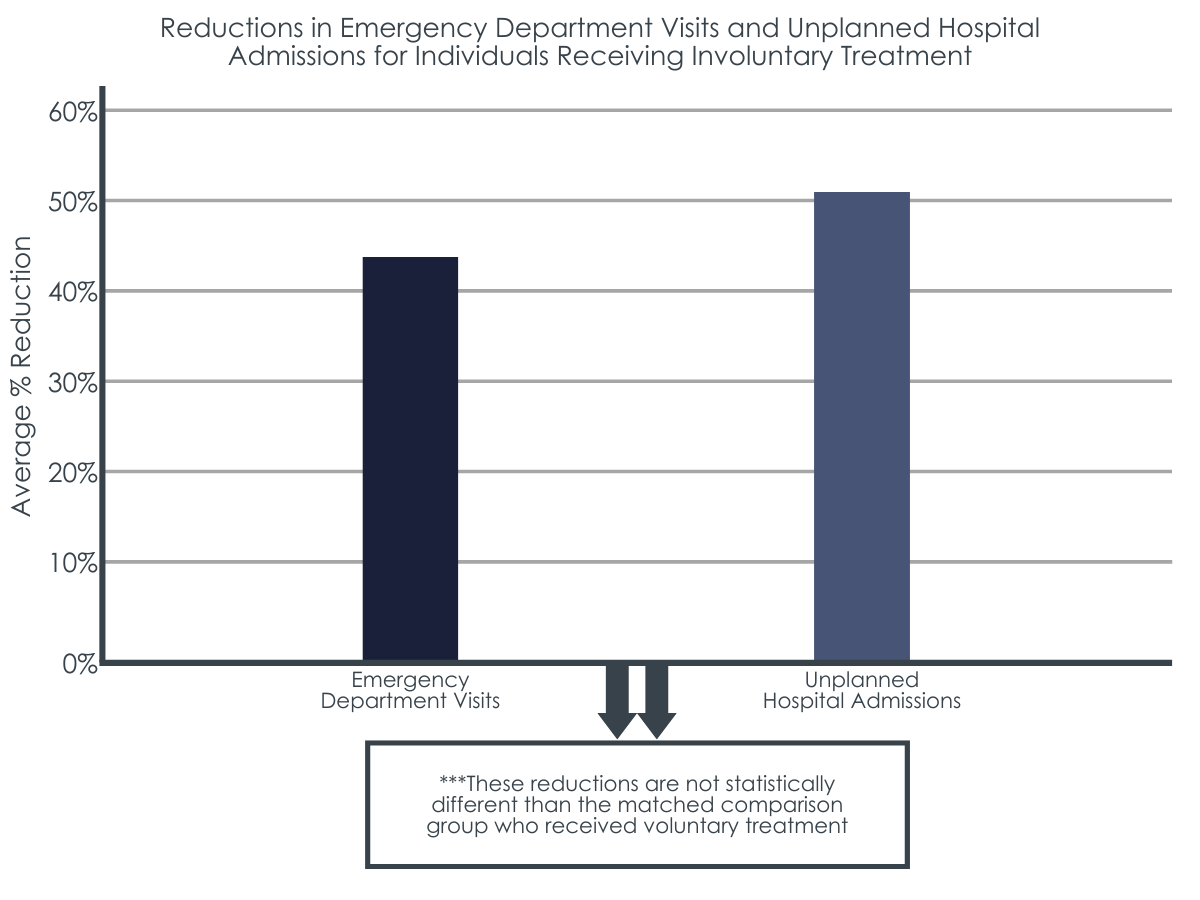
There was a reduction in healthcare utilization measures after involuntary treatment.
After the index treatment, emergency department visits were reduced by 44% on average and unplanned hospital admissions were reduced by 51% on average for people that received involuntary treatment.
This reduction was statistically similar to the comparison group.
The intervention effect, which measures the difference in emergency department visits and unplanned hospital admissions between those that received involuntary treatment and those that received voluntary treatment, was statistically similar, meaning that there was no difference between the 2 groups.
Sensitivity analyses showed that voluntary treatment might have been better at reducing healthcare utilization than involuntary treatment.
Even though the difference in outcomes was statistically similar between the 2 groups, the effect size favored the group that received voluntary treatment. When the researchers modified their assumptions in the model as a sensitivity analysis to test the robustness of their results, the effect size mostly favored the group that received voluntary treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers found that emergency department visits were reduced by 44% on average and unplanned hospital admissions were reduced by 51% on average for people that received involuntary treatment, although this reduction was similar for the control group that received voluntary treatment, suggesting that involuntary treatment was just as effective, but not more effective, in reducing these healthcare utilization measures than voluntary treatment.
A major limitation of this study is that individuals who are civilly committed are an especially high-risk group, and this high-risk group was compared to a group that underwent voluntary treatment without controlling for the severity of alcohol use disorder. In addition, motivation for change, an important factor in treatment outcomes, was likely higher in those who voluntary sought treatment for their alcohol use disorder compared with those who underwent involuntary treatment, which the study could not control for. However, some research suggests that motivation to change is unexpectedly high for patients undergoing involuntary treatment, although lower than patients undergoing voluntary treatment.
In light of these limitations, the study findings show that involuntary treatment was successful in reducing the measured healthcare utilization outcomes of subsequent emergency department visits and unplanned hospital admissions up to 1 year after the index treatment. This is an important finding given that it usually takes multiple serious attempts to resolve an alcohol problem and the vast majority of people with an alcohol use disorder do not perceive a need for treatment. Stated differently, involuntary treatment might provide an opportunity for individuals with severe alcohol use disorders who are especially at risk for adverse events to access needed treatment that they would have otherwise not received, beginning, or reinitiating the recovery process. However, these potential benefits should be balanced against any potential harms. For example, a civil commitment for someone with a similarly severe opioid use disorder that does not include medication could put that person at increased risk for overdose upon treatment completion (e.g., due to a lowered physiological tolerance to opioids acquired with total abstinence during an extended treatment residential phase). At the very least, involuntary treatment should be properly evidence-based, adhere to the “best practice” standards of clinical care, be delivered in an appropriate treatment facility, and be consistent with patients’ diverse treatment needs and preferences. The degree to which involuntary treatment programs use such approaches in cases of involuntary commitment is very much in question.
Although involuntary treatment was found to be no better or worse than voluntary treatment on the measured outcomes and timepoints, it is more ideal if an individual can decide for themselves whether they want to enter treatment or not for a number of reasons. In addition to violating someone’s autonomy and privacy, involuntary treatment is very resource intensive and thus more expensive also. Although involuntary treatment may serve as a last option for individuals with severe alcohol use disorder who have refused voluntary treatment and are at immediate risk of harm to themselves or others, all possible efforts should be made to encourage and enhance access to voluntary treatment. This might be done by increasing the flexibility, accessibility, and attractiveness of treatment, such as providing same-day treatment options and diversifying treatments to align with a variety of patient preferences.
This study compared involuntary treatment to voluntary treatment. However, the real-world counterfactual to involuntary treatment would be receiving no treatment. In other words, a critical question that this study does not address is whether there is benefit and/or harm from placing an individual in involuntary treatment compared to that person not receiving any treatment at all. However, identifying and measuring outcomes in a group receiving no treatment may be unrealistic given difficulty in monitoring and observing an untreated group with severe alcohol use disorder and the fact that the stakes are high for these individuals in terms of harm to themselves and others. Also, this study examined individuals with alcohol use disorder. Much of the recent criticism towards involuntary treatment pertains to individuals with opioid use disorder in light of current opioid overdose crisis, who are at increased risk for premature mortality particularly with fentanyl infusions into the drug supply. Generalizing the results of this study to individuals with other types of substance use disorders, including opioid use disorder, should be done with caution.
Civil commitments are common in other countries. In the United States, 36 states and the District of Columbia have some form of civil commitment for substance use disorder. Civil commitment statutes show wide variability in the law itself and utilization of the law, with some states with civil commitment statutes rarely using this form of involuntary treatment while others use it much more frequently. More research is needed to better understand the benefits and risks of civil commitments.
Even though the researchers used propensity score matching to reduce confounding, this was not a randomized controlled trial and other variables could have biased the results. For example, there was no measure for severity of addiction, which may have been very different between the 2 groups.
There were around 100 patients who underwent involuntary treatment that were excluded from the study because of missing data. If these individuals were different from individuals included in the study, it would bias the results.
This is a data-linkage study that relies on several linked administrative databases. Some of the data entered by clinicians or administrators could be miscoded or incorrect.
Generalizing these study findings should be done with caution given differences in addiction treatment systems and heterogeneity of civil commitments across countries and states.
Only 2 outcome measures were used, which were healthcare utilization measures. It is unclear if 1 or both groups also reduced drinking or achieved alcohol use disorder remission.
BOTTOM LINE
This study examined healthcare utilization before and after involuntary treatment for severe alcohol use disorder compared with a matched group of patients who underwent voluntary treatment. Researchers found that emergency department visits and unplanned hospital admissions were reduced 1 year after people received involuntary treatment as much as those who received voluntary treatment, suggesting that involuntary treatment may produce similar benefits in reducing healthcare utilization compared with voluntary treatment for severely alcohol addicted individuals who are at high risk of adverse events.
For individuals and families seeking recovery: Involuntary treatment might provide an opportunity for individuals with severe alcohol use disorders to access needed treatment that they would have otherwise not receive. However, these potential benefits should be weighed with any potential harms. Voluntary treatment is more ideal and preferred and should be pursued first, though involuntary treatment might serve as a last option in special circumstances.
For treatment professionals and treatment systems: Involuntary treatment might provide an opportunity for individuals with severe alcohol use disorders to access needed treatment that they would have otherwise not received. However, these potential benefits should be weighed with any potential harms. Given the loss of freedom and privacy as well as the fact that involuntary treatment is resource intensive and more expensive, voluntary treatment is preferred and should be pursued first, though involuntary treatment might serve as a last option in special circumstances. Involuntary treatment should be evidence-based, comprised of “best practice” standards of clinical care, delivered in an appropriate treatment environment, and consistent with patients’ diverse treatment needs and preferences. Making voluntary treatment more flexible, accessible, and attractive, such as providing same-day treatment and diversifying treatment options to align with a variety of patient preferences, might increase uptake of this form of treatment and circumvent the need for involuntary treatment in many cases.
For scientists: This a retrospective cohort study using linked administrative databases to measure the change in healthcare utilization measures before and after involuntary treatment for alcohol use disorder compared with a matched control group that underwent voluntary treatment. The comparison group was matched using propensity score matching but did not include a measure for severity in the propensity scores that certainly introduced residual confounding. The researchers also used a Bayesian approach since they found null findings in a similar study with a broader sample size of all types of substance use disorders. Evidence for involuntary commitments is mixed and sparse, calling for more rigorous research to better understand the benefits and risks of civil commitments. Also, the real-world counterfactual to involuntary treatment is no treatment, so a more rigorous study design for future studies would be comparing involuntary treatment to no treatment or harm reduction services only, although this ideal study design is likely unrealistic and infeasible due to the nature of severe alcohol use disorder.
For policy makers: Although more research is needed, the findings of this study add support to the notion of involuntary treatment as a last option under the special circumstances described above. Involuntary treatment might provide an opportunity for individuals with severe alcohol use disorders who are deemed at particularly high risk for adverse events or harm to others to access needed treatment that they would have otherwise not receive. However, these potential benefits should be weighed with any potential harms. If civil commitment laws are in place, policymakers should provide funding to better understand if the benefits outweigh the risks and for which specific cases in particular. Involuntary treatment should consist of “best practice” standards of clinical care, delivered in an appropriate treatment facility, and be consistent with patients’ diverse treatment needs and preferences. Efforts to increase treatment access and provide diversified treatment options may make voluntary treatment more attractive and possible circumvent the need for involuntary treatment in many cases. This is important given that involuntary commitment can be a much costlier option.
Involuntary treatment, also known as civil commitment, is a legal mechanism that allows family members, healthcare professionals, and others to seek court-mandated treatment for an individual who poses a significant threat of harming themselves or others, but is unwilling to attend treatment. Involuntary treatment is sometimes used for those with substance use disorders, for example if a person is at considerable risk for overdose. This form of treatment is different than coercive treatment, such as drug courts, where individuals have a choice, albeit sometimes a very narrow one between treatment and incarceration. The role of involuntary treatment in substance use disorder is a contentious issue. In addition to potentially violating an individual’s rights through infringement of autonomy and privacy, evidence for involuntary commitments is mixed with some studies suggesting potential harms. On the other hand, it may save someone’s life and the lives of others, especially for those at the most severe levels of impairment. There is stronger empirical evidence that certain types of involuntary treatment can benefit health and safety for individuals with other forms of severe mental illness.
Given the dearth of empirical evidence on whether involuntary treatment actual helps individuals with substance use disorders, more research is needed, especially in settings outside of the criminal justice system. A statute in New South Wales, Australia allows for involuntary treatment in special circumstances as an approach of last resort for substance use disorder. In a previous evaluation study of this statute, researchers found that, although this form of treatment improved measured outcomes up to 1 year after treatment completion, this improvement did not differ from a comparison group suggesting similar outcomes relative to treatment as usual. In the current study, researchers examined the differences between involuntary and voluntary treatment for alcohol use disorder on subsequent healthcare utilization measures.
HOW WAS THIS STUDY CONDUCTED?
This a retrospective cohort study using linked administrative databases to measure the change in healthcare utilization measures before and after involuntary treatment for alcohol use disorder compared with a matched control group that underwent voluntary treatment.
The study took place in New South Wales, Australia from 2012 to 2018. The Involuntary Drug and Alcohol Program began in 2012 under a statute that allowed for involuntary treatment of substance use disorders as a last resort when certain conditions were met. There had to be robust evidence of:
Severe substance use disorder
Care or treatment necessary to protect from serious harm
Likely to benefit from treatment for substance use disorder and has previously refused treatment
No other appropriate and less restrictive means was available
Involuntary treatment consisted of medically supervised alcohol detoxification, comprehensive assessment, rehabilitation, and support for up to 28 days with voluntary aftercare for up to 6 months. Treatment took place in a locked ward of 1 of 2 hospitals in New South Wales.
Researchers limited the sample to individuals who identified alcohol as the principal drug of concern resulting in 231 eligible individuals between 2012 and 2018. These individuals were identified through the New South Wales Minimum Data Set for Drug and Alcohol Treatment Services. Since some individuals had more than 1 episode of involuntary treatment in the data set, the first episode of care was used for this study, called the index treatment episode.
The variables of interest were changes in 2 healthcare utilization measures: the change in the number of emergency department visits recorded in the 12 months prior to the index treatment episode and in the 12 months after the index treatment was completed, which was identified from the New South Wales Emergency Department Data Collection, and the change in the number of unplanned hospital admissions recorded in the 12 months prior to the index treatment episode and in the 12 months after the index treatment was completed, which was identified from the New South Wales Admitted Patient Data Collection.
A comparison group of individuals receiving voluntary treatment was constructed to compare the outcomes with involuntarily committed and treated individuals. Nearly 5000 individuals were identified as having a medical condition that resulted from harmful use of alcohol and received at least 1 of 3 forms of voluntary treatment consisting of medically supervised detoxification, rehabilitation, and/or pharmacotherapies for alcohol use disorder. Then, researchers used a statistical technique to identify 231 individuals in the control group that were most similar to the 231 individuals in the involuntary treatment group based on the pre-treatment variables of interest (emergency department visits and unplanned hospital admissions). Analyses also controlled for demographic characteristics as well as a summary variable capturing clinical complexity based on number of medical comorbidities, co-occurring psychiatric disorder, and social comorbidity (e.g., employment status) to try and equate the groups as closely as possible.
There were minimal demographic and clinical differences between the treatment and the comparison group. The only statistical differences were that there was a higher proportion of males in the voluntarily treated (control) group, and there were a higher proportion of individuals with no previous alcohol treatment episodes and more than 5 previous alcohol episodes in the involuntarily committed treatment group.
WHAT DID THIS STUDY FIND?
There was a reduction in healthcare utilization measures after involuntary treatment.
After the index treatment, emergency department visits were reduced by 44% on average and unplanned hospital admissions were reduced by 51% on average for people that received involuntary treatment.
This reduction was statistically similar to the comparison group.
The intervention effect, which measures the difference in emergency department visits and unplanned hospital admissions between those that received involuntary treatment and those that received voluntary treatment, was statistically similar, meaning that there was no difference between the 2 groups.
Sensitivity analyses showed that voluntary treatment might have been better at reducing healthcare utilization than involuntary treatment.
Even though the difference in outcomes was statistically similar between the 2 groups, the effect size favored the group that received voluntary treatment. When the researchers modified their assumptions in the model as a sensitivity analysis to test the robustness of their results, the effect size mostly favored the group that received voluntary treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers found that emergency department visits were reduced by 44% on average and unplanned hospital admissions were reduced by 51% on average for people that received involuntary treatment, although this reduction was similar for the control group that received voluntary treatment, suggesting that involuntary treatment was just as effective, but not more effective, in reducing these healthcare utilization measures than voluntary treatment.
A major limitation of this study is that individuals who are civilly committed are an especially high-risk group, and this high-risk group was compared to a group that underwent voluntary treatment without controlling for the severity of alcohol use disorder. In addition, motivation for change, an important factor in treatment outcomes, was likely higher in those who voluntary sought treatment for their alcohol use disorder compared with those who underwent involuntary treatment, which the study could not control for. However, some research suggests that motivation to change is unexpectedly high for patients undergoing involuntary treatment, although lower than patients undergoing voluntary treatment.
In light of these limitations, the study findings show that involuntary treatment was successful in reducing the measured healthcare utilization outcomes of subsequent emergency department visits and unplanned hospital admissions up to 1 year after the index treatment. This is an important finding given that it usually takes multiple serious attempts to resolve an alcohol problem and the vast majority of people with an alcohol use disorder do not perceive a need for treatment. Stated differently, involuntary treatment might provide an opportunity for individuals with severe alcohol use disorders who are especially at risk for adverse events to access needed treatment that they would have otherwise not received, beginning, or reinitiating the recovery process. However, these potential benefits should be balanced against any potential harms. For example, a civil commitment for someone with a similarly severe opioid use disorder that does not include medication could put that person at increased risk for overdose upon treatment completion (e.g., due to a lowered physiological tolerance to opioids acquired with total abstinence during an extended treatment residential phase). At the very least, involuntary treatment should be properly evidence-based, adhere to the “best practice” standards of clinical care, be delivered in an appropriate treatment facility, and be consistent with patients’ diverse treatment needs and preferences. The degree to which involuntary treatment programs use such approaches in cases of involuntary commitment is very much in question.
Although involuntary treatment was found to be no better or worse than voluntary treatment on the measured outcomes and timepoints, it is more ideal if an individual can decide for themselves whether they want to enter treatment or not for a number of reasons. In addition to violating someone’s autonomy and privacy, involuntary treatment is very resource intensive and thus more expensive also. Although involuntary treatment may serve as a last option for individuals with severe alcohol use disorder who have refused voluntary treatment and are at immediate risk of harm to themselves or others, all possible efforts should be made to encourage and enhance access to voluntary treatment. This might be done by increasing the flexibility, accessibility, and attractiveness of treatment, such as providing same-day treatment options and diversifying treatments to align with a variety of patient preferences.
This study compared involuntary treatment to voluntary treatment. However, the real-world counterfactual to involuntary treatment would be receiving no treatment. In other words, a critical question that this study does not address is whether there is benefit and/or harm from placing an individual in involuntary treatment compared to that person not receiving any treatment at all. However, identifying and measuring outcomes in a group receiving no treatment may be unrealistic given difficulty in monitoring and observing an untreated group with severe alcohol use disorder and the fact that the stakes are high for these individuals in terms of harm to themselves and others. Also, this study examined individuals with alcohol use disorder. Much of the recent criticism towards involuntary treatment pertains to individuals with opioid use disorder in light of current opioid overdose crisis, who are at increased risk for premature mortality particularly with fentanyl infusions into the drug supply. Generalizing the results of this study to individuals with other types of substance use disorders, including opioid use disorder, should be done with caution.
Civil commitments are common in other countries. In the United States, 36 states and the District of Columbia have some form of civil commitment for substance use disorder. Civil commitment statutes show wide variability in the law itself and utilization of the law, with some states with civil commitment statutes rarely using this form of involuntary treatment while others use it much more frequently. More research is needed to better understand the benefits and risks of civil commitments.
Even though the researchers used propensity score matching to reduce confounding, this was not a randomized controlled trial and other variables could have biased the results. For example, there was no measure for severity of addiction, which may have been very different between the 2 groups.
There were around 100 patients who underwent involuntary treatment that were excluded from the study because of missing data. If these individuals were different from individuals included in the study, it would bias the results.
This is a data-linkage study that relies on several linked administrative databases. Some of the data entered by clinicians or administrators could be miscoded or incorrect.
Generalizing these study findings should be done with caution given differences in addiction treatment systems and heterogeneity of civil commitments across countries and states.
Only 2 outcome measures were used, which were healthcare utilization measures. It is unclear if 1 or both groups also reduced drinking or achieved alcohol use disorder remission.
BOTTOM LINE
This study examined healthcare utilization before and after involuntary treatment for severe alcohol use disorder compared with a matched group of patients who underwent voluntary treatment. Researchers found that emergency department visits and unplanned hospital admissions were reduced 1 year after people received involuntary treatment as much as those who received voluntary treatment, suggesting that involuntary treatment may produce similar benefits in reducing healthcare utilization compared with voluntary treatment for severely alcohol addicted individuals who are at high risk of adverse events.
For individuals and families seeking recovery: Involuntary treatment might provide an opportunity for individuals with severe alcohol use disorders to access needed treatment that they would have otherwise not receive. However, these potential benefits should be weighed with any potential harms. Voluntary treatment is more ideal and preferred and should be pursued first, though involuntary treatment might serve as a last option in special circumstances.
For treatment professionals and treatment systems: Involuntary treatment might provide an opportunity for individuals with severe alcohol use disorders to access needed treatment that they would have otherwise not received. However, these potential benefits should be weighed with any potential harms. Given the loss of freedom and privacy as well as the fact that involuntary treatment is resource intensive and more expensive, voluntary treatment is preferred and should be pursued first, though involuntary treatment might serve as a last option in special circumstances. Involuntary treatment should be evidence-based, comprised of “best practice” standards of clinical care, delivered in an appropriate treatment environment, and consistent with patients’ diverse treatment needs and preferences. Making voluntary treatment more flexible, accessible, and attractive, such as providing same-day treatment and diversifying treatment options to align with a variety of patient preferences, might increase uptake of this form of treatment and circumvent the need for involuntary treatment in many cases.
For scientists: This a retrospective cohort study using linked administrative databases to measure the change in healthcare utilization measures before and after involuntary treatment for alcohol use disorder compared with a matched control group that underwent voluntary treatment. The comparison group was matched using propensity score matching but did not include a measure for severity in the propensity scores that certainly introduced residual confounding. The researchers also used a Bayesian approach since they found null findings in a similar study with a broader sample size of all types of substance use disorders. Evidence for involuntary commitments is mixed and sparse, calling for more rigorous research to better understand the benefits and risks of civil commitments. Also, the real-world counterfactual to involuntary treatment is no treatment, so a more rigorous study design for future studies would be comparing involuntary treatment to no treatment or harm reduction services only, although this ideal study design is likely unrealistic and infeasible due to the nature of severe alcohol use disorder.
For policy makers: Although more research is needed, the findings of this study add support to the notion of involuntary treatment as a last option under the special circumstances described above. Involuntary treatment might provide an opportunity for individuals with severe alcohol use disorders who are deemed at particularly high risk for adverse events or harm to others to access needed treatment that they would have otherwise not receive. However, these potential benefits should be weighed with any potential harms. If civil commitment laws are in place, policymakers should provide funding to better understand if the benefits outweigh the risks and for which specific cases in particular. Involuntary treatment should consist of “best practice” standards of clinical care, delivered in an appropriate treatment facility, and be consistent with patients’ diverse treatment needs and preferences. Efforts to increase treatment access and provide diversified treatment options may make voluntary treatment more attractive and possible circumvent the need for involuntary treatment in many cases. This is important given that involuntary commitment can be a much costlier option.
Involuntary treatment, also known as civil commitment, is a legal mechanism that allows family members, healthcare professionals, and others to seek court-mandated treatment for an individual who poses a significant threat of harming themselves or others, but is unwilling to attend treatment. Involuntary treatment is sometimes used for those with substance use disorders, for example if a person is at considerable risk for overdose. This form of treatment is different than coercive treatment, such as drug courts, where individuals have a choice, albeit sometimes a very narrow one between treatment and incarceration. The role of involuntary treatment in substance use disorder is a contentious issue. In addition to potentially violating an individual’s rights through infringement of autonomy and privacy, evidence for involuntary commitments is mixed with some studies suggesting potential harms. On the other hand, it may save someone’s life and the lives of others, especially for those at the most severe levels of impairment. There is stronger empirical evidence that certain types of involuntary treatment can benefit health and safety for individuals with other forms of severe mental illness.
Given the dearth of empirical evidence on whether involuntary treatment actual helps individuals with substance use disorders, more research is needed, especially in settings outside of the criminal justice system. A statute in New South Wales, Australia allows for involuntary treatment in special circumstances as an approach of last resort for substance use disorder. In a previous evaluation study of this statute, researchers found that, although this form of treatment improved measured outcomes up to 1 year after treatment completion, this improvement did not differ from a comparison group suggesting similar outcomes relative to treatment as usual. In the current study, researchers examined the differences between involuntary and voluntary treatment for alcohol use disorder on subsequent healthcare utilization measures.
HOW WAS THIS STUDY CONDUCTED?
This a retrospective cohort study using linked administrative databases to measure the change in healthcare utilization measures before and after involuntary treatment for alcohol use disorder compared with a matched control group that underwent voluntary treatment.
The study took place in New South Wales, Australia from 2012 to 2018. The Involuntary Drug and Alcohol Program began in 2012 under a statute that allowed for involuntary treatment of substance use disorders as a last resort when certain conditions were met. There had to be robust evidence of:
Severe substance use disorder
Care or treatment necessary to protect from serious harm
Likely to benefit from treatment for substance use disorder and has previously refused treatment
No other appropriate and less restrictive means was available
Involuntary treatment consisted of medically supervised alcohol detoxification, comprehensive assessment, rehabilitation, and support for up to 28 days with voluntary aftercare for up to 6 months. Treatment took place in a locked ward of 1 of 2 hospitals in New South Wales.
Researchers limited the sample to individuals who identified alcohol as the principal drug of concern resulting in 231 eligible individuals between 2012 and 2018. These individuals were identified through the New South Wales Minimum Data Set for Drug and Alcohol Treatment Services. Since some individuals had more than 1 episode of involuntary treatment in the data set, the first episode of care was used for this study, called the index treatment episode.
The variables of interest were changes in 2 healthcare utilization measures: the change in the number of emergency department visits recorded in the 12 months prior to the index treatment episode and in the 12 months after the index treatment was completed, which was identified from the New South Wales Emergency Department Data Collection, and the change in the number of unplanned hospital admissions recorded in the 12 months prior to the index treatment episode and in the 12 months after the index treatment was completed, which was identified from the New South Wales Admitted Patient Data Collection.
A comparison group of individuals receiving voluntary treatment was constructed to compare the outcomes with involuntarily committed and treated individuals. Nearly 5000 individuals were identified as having a medical condition that resulted from harmful use of alcohol and received at least 1 of 3 forms of voluntary treatment consisting of medically supervised detoxification, rehabilitation, and/or pharmacotherapies for alcohol use disorder. Then, researchers used a statistical technique to identify 231 individuals in the control group that were most similar to the 231 individuals in the involuntary treatment group based on the pre-treatment variables of interest (emergency department visits and unplanned hospital admissions). Analyses also controlled for demographic characteristics as well as a summary variable capturing clinical complexity based on number of medical comorbidities, co-occurring psychiatric disorder, and social comorbidity (e.g., employment status) to try and equate the groups as closely as possible.
There were minimal demographic and clinical differences between the treatment and the comparison group. The only statistical differences were that there was a higher proportion of males in the voluntarily treated (control) group, and there were a higher proportion of individuals with no previous alcohol treatment episodes and more than 5 previous alcohol episodes in the involuntarily committed treatment group.
WHAT DID THIS STUDY FIND?
There was a reduction in healthcare utilization measures after involuntary treatment.
After the index treatment, emergency department visits were reduced by 44% on average and unplanned hospital admissions were reduced by 51% on average for people that received involuntary treatment.
This reduction was statistically similar to the comparison group.
The intervention effect, which measures the difference in emergency department visits and unplanned hospital admissions between those that received involuntary treatment and those that received voluntary treatment, was statistically similar, meaning that there was no difference between the 2 groups.
Sensitivity analyses showed that voluntary treatment might have been better at reducing healthcare utilization than involuntary treatment.
Even though the difference in outcomes was statistically similar between the 2 groups, the effect size favored the group that received voluntary treatment. When the researchers modified their assumptions in the model as a sensitivity analysis to test the robustness of their results, the effect size mostly favored the group that received voluntary treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers found that emergency department visits were reduced by 44% on average and unplanned hospital admissions were reduced by 51% on average for people that received involuntary treatment, although this reduction was similar for the control group that received voluntary treatment, suggesting that involuntary treatment was just as effective, but not more effective, in reducing these healthcare utilization measures than voluntary treatment.
A major limitation of this study is that individuals who are civilly committed are an especially high-risk group, and this high-risk group was compared to a group that underwent voluntary treatment without controlling for the severity of alcohol use disorder. In addition, motivation for change, an important factor in treatment outcomes, was likely higher in those who voluntary sought treatment for their alcohol use disorder compared with those who underwent involuntary treatment, which the study could not control for. However, some research suggests that motivation to change is unexpectedly high for patients undergoing involuntary treatment, although lower than patients undergoing voluntary treatment.
In light of these limitations, the study findings show that involuntary treatment was successful in reducing the measured healthcare utilization outcomes of subsequent emergency department visits and unplanned hospital admissions up to 1 year after the index treatment. This is an important finding given that it usually takes multiple serious attempts to resolve an alcohol problem and the vast majority of people with an alcohol use disorder do not perceive a need for treatment. Stated differently, involuntary treatment might provide an opportunity for individuals with severe alcohol use disorders who are especially at risk for adverse events to access needed treatment that they would have otherwise not received, beginning, or reinitiating the recovery process. However, these potential benefits should be balanced against any potential harms. For example, a civil commitment for someone with a similarly severe opioid use disorder that does not include medication could put that person at increased risk for overdose upon treatment completion (e.g., due to a lowered physiological tolerance to opioids acquired with total abstinence during an extended treatment residential phase). At the very least, involuntary treatment should be properly evidence-based, adhere to the “best practice” standards of clinical care, be delivered in an appropriate treatment facility, and be consistent with patients’ diverse treatment needs and preferences. The degree to which involuntary treatment programs use such approaches in cases of involuntary commitment is very much in question.
Although involuntary treatment was found to be no better or worse than voluntary treatment on the measured outcomes and timepoints, it is more ideal if an individual can decide for themselves whether they want to enter treatment or not for a number of reasons. In addition to violating someone’s autonomy and privacy, involuntary treatment is very resource intensive and thus more expensive also. Although involuntary treatment may serve as a last option for individuals with severe alcohol use disorder who have refused voluntary treatment and are at immediate risk of harm to themselves or others, all possible efforts should be made to encourage and enhance access to voluntary treatment. This might be done by increasing the flexibility, accessibility, and attractiveness of treatment, such as providing same-day treatment options and diversifying treatments to align with a variety of patient preferences.
This study compared involuntary treatment to voluntary treatment. However, the real-world counterfactual to involuntary treatment would be receiving no treatment. In other words, a critical question that this study does not address is whether there is benefit and/or harm from placing an individual in involuntary treatment compared to that person not receiving any treatment at all. However, identifying and measuring outcomes in a group receiving no treatment may be unrealistic given difficulty in monitoring and observing an untreated group with severe alcohol use disorder and the fact that the stakes are high for these individuals in terms of harm to themselves and others. Also, this study examined individuals with alcohol use disorder. Much of the recent criticism towards involuntary treatment pertains to individuals with opioid use disorder in light of current opioid overdose crisis, who are at increased risk for premature mortality particularly with fentanyl infusions into the drug supply. Generalizing the results of this study to individuals with other types of substance use disorders, including opioid use disorder, should be done with caution.
Civil commitments are common in other countries. In the United States, 36 states and the District of Columbia have some form of civil commitment for substance use disorder. Civil commitment statutes show wide variability in the law itself and utilization of the law, with some states with civil commitment statutes rarely using this form of involuntary treatment while others use it much more frequently. More research is needed to better understand the benefits and risks of civil commitments.
Even though the researchers used propensity score matching to reduce confounding, this was not a randomized controlled trial and other variables could have biased the results. For example, there was no measure for severity of addiction, which may have been very different between the 2 groups.
There were around 100 patients who underwent involuntary treatment that were excluded from the study because of missing data. If these individuals were different from individuals included in the study, it would bias the results.
This is a data-linkage study that relies on several linked administrative databases. Some of the data entered by clinicians or administrators could be miscoded or incorrect.
Generalizing these study findings should be done with caution given differences in addiction treatment systems and heterogeneity of civil commitments across countries and states.
Only 2 outcome measures were used, which were healthcare utilization measures. It is unclear if 1 or both groups also reduced drinking or achieved alcohol use disorder remission.
BOTTOM LINE
This study examined healthcare utilization before and after involuntary treatment for severe alcohol use disorder compared with a matched group of patients who underwent voluntary treatment. Researchers found that emergency department visits and unplanned hospital admissions were reduced 1 year after people received involuntary treatment as much as those who received voluntary treatment, suggesting that involuntary treatment may produce similar benefits in reducing healthcare utilization compared with voluntary treatment for severely alcohol addicted individuals who are at high risk of adverse events.
For individuals and families seeking recovery: Involuntary treatment might provide an opportunity for individuals with severe alcohol use disorders to access needed treatment that they would have otherwise not receive. However, these potential benefits should be weighed with any potential harms. Voluntary treatment is more ideal and preferred and should be pursued first, though involuntary treatment might serve as a last option in special circumstances.
For treatment professionals and treatment systems: Involuntary treatment might provide an opportunity for individuals with severe alcohol use disorders to access needed treatment that they would have otherwise not received. However, these potential benefits should be weighed with any potential harms. Given the loss of freedom and privacy as well as the fact that involuntary treatment is resource intensive and more expensive, voluntary treatment is preferred and should be pursued first, though involuntary treatment might serve as a last option in special circumstances. Involuntary treatment should be evidence-based, comprised of “best practice” standards of clinical care, delivered in an appropriate treatment environment, and consistent with patients’ diverse treatment needs and preferences. Making voluntary treatment more flexible, accessible, and attractive, such as providing same-day treatment and diversifying treatment options to align with a variety of patient preferences, might increase uptake of this form of treatment and circumvent the need for involuntary treatment in many cases.
For scientists: This a retrospective cohort study using linked administrative databases to measure the change in healthcare utilization measures before and after involuntary treatment for alcohol use disorder compared with a matched control group that underwent voluntary treatment. The comparison group was matched using propensity score matching but did not include a measure for severity in the propensity scores that certainly introduced residual confounding. The researchers also used a Bayesian approach since they found null findings in a similar study with a broader sample size of all types of substance use disorders. Evidence for involuntary commitments is mixed and sparse, calling for more rigorous research to better understand the benefits and risks of civil commitments. Also, the real-world counterfactual to involuntary treatment is no treatment, so a more rigorous study design for future studies would be comparing involuntary treatment to no treatment or harm reduction services only, although this ideal study design is likely unrealistic and infeasible due to the nature of severe alcohol use disorder.
For policy makers: Although more research is needed, the findings of this study add support to the notion of involuntary treatment as a last option under the special circumstances described above. Involuntary treatment might provide an opportunity for individuals with severe alcohol use disorders who are deemed at particularly high risk for adverse events or harm to others to access needed treatment that they would have otherwise not receive. However, these potential benefits should be weighed with any potential harms. If civil commitment laws are in place, policymakers should provide funding to better understand if the benefits outweigh the risks and for which specific cases in particular. Involuntary treatment should consist of “best practice” standards of clinical care, delivered in an appropriate treatment facility, and be consistent with patients’ diverse treatment needs and preferences. Efforts to increase treatment access and provide diversified treatment options may make voluntary treatment more attractive and possible circumvent the need for involuntary treatment in many cases. This is important given that involuntary commitment can be a much costlier option.