Disparities in alcohol use treatment utilization among Hispanic Americans: The role of gender and insurance coverage
Black and Hispanic people in the US may encounter barriers to alcohol use disorder treatment. However, it is unclear how such treatment usage may vary at the intersection of racial/ethnic and gender identities, and how health insurance coverage might play a role. This study analyzed national survey data to examine how alcohol treatment utilization varied by race, ethnicity, and gender, and whether any disparities differed by insurance coverage.
There are many effective therapies, medications, and recovery support options for individuals with alcohol use disorder. However, evidence suggests that treatment may be underutilized by many who need it. A common barrier to treatment is the cost of care. Regardless of insurance coverage, those needing treatment may not be able to afford it due to variability in the types of services covered by insurance. This is especially problematic for those on Medicaid– public health insurance for low-income people. Despite over 72 million people in the US being on Medicaid, there is evidence that this insurance modality may constrain options for patients interested in alcohol use disorder treatment. Medicaid also disproportionately serves racially/ethnically minority groups (e.g., Black and Hispanic Americans). Despite Medicaid being a critical provider of care in the US it is unclear how effective it is at providing alcohol treatment to patients. Separately, because Medicaid is available only to those in lower socioeconomic strata, it may be a marker for a host of other challenges that make it hard for individuals to access and remain in care (i.e., limited recovery capital). In addition, it is unknown if differences in alcohol treatment utilization exist across intersecting social identities (racial and ethnic minority groups and women). Identifying disparities with this intersectional framework can help inform strategies to address barriers to accessing care among marginalized groups. This study conducted an intersectional analysis of national survey data to determine how treatment usage varied across racial, ethnic, and gender identities as well as insurance coverage.
HOW WAS THIS STUDY CONDUCTED?
The study was a cross-sectional analysis of 3 years of pooled data (2017-2019) from the National Survey on Drug Use and Health. The National Survey on Drug Use and Health is an annual survey conducted by the Substance Use and Mental Health Services Administration (SAMHSA) to gather information on substance use and mental health issues among the US population. Data are collected across all 50 states and the District of Columbia. Only non-institutionalized (e.g., non-incarcerated) individuals 12 years or older are sampled.
Participants were included in the present analyses if they 1) met Diagnostic and Statistical Manual of Mental Disorders, 4th edition criteria for alcohol use disorder (i.e., “alcohol dependence” or “alcohol abuse”) in the past year, 2) reported only having Medicaid, private insurance, or being uninsured, and 3) identified as White, Black, or Latinx. The primary outcome of this study was past year alcohol use disorder treatment utilization. This was defined as receiving any kind of alcohol use disorder treatment in a specialty facility including hospitals (inpatient), rehabilitation facilities (inpatient or outpatient), or mental health centers.
The primary goal of the present study was to examine rates of alcohol use disorder treatment utilization among those who report alcohol use disorder symptomology. Specifically, this work set out to examine how alcohol use disorder treatment use varied based on an individual’s race, ethnicity, gender, and insurance coverage. To do this, the authors used multivariable logistic regression models– a type of statistical approach where the probability of an outcome is determined based on multiple independent variables, adjusting statistically for self-rated health status, co-occurring substance use disorders (e.g., stimulant or opioid use disorder in addition to alcohol use disorder), past-year major depressive episode (yes/no), elevated psychological distress (based on an accepted cut-off from a validated scale), age, marital status, and survey year (2017, 2018, or 2019). Through this analysis, the authors were able to demonstrate how actual rates of alcohol use disorder treatment varied across groups. In the present analysis the authors compared all groups to White men. The rational for this is that compared to other demographics, White men have higher income, lower unemployment, and more healthcare coverage. Data in the present analysis were weighted– that is adjusted for potential biases and differences between the target population and the sample.
The final sample was comprised of 7782 respondents from across the US. The sample consisted of White males (42%), White females (29%), Latino males (12%), Latina females (7%), Black males (6%), and Black females (5%). Most participants reported having private insurance (68.9%) with the remainder indicating they had Medicaid (15.7%) or were uninsured (15.4%). Participants’ age ranged from 18-64 years.
WHAT DID THIS STUDY FIND?
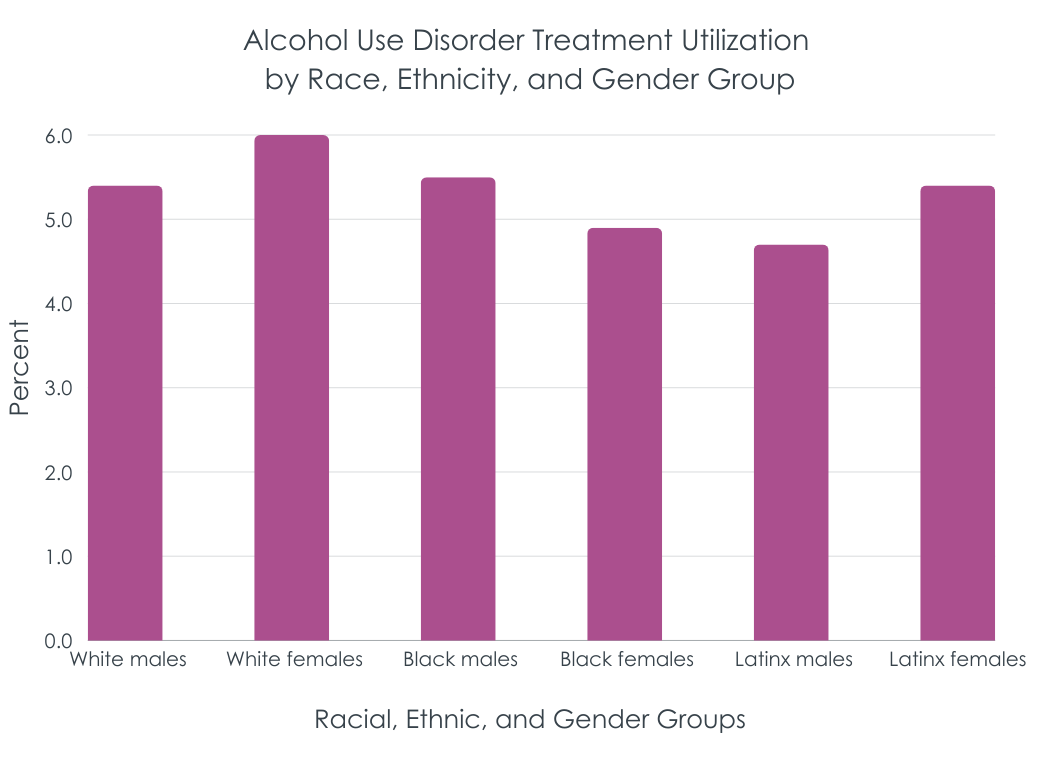
Only 5.4% of adults with an alcohol use disorder received alcohol use disorder treatment
The vast majority of US adults with alcohol use disorder did not receive specialty treatment. Treatment seeking rates were similar across participant race, ethnicity, gender, and insurance coverage.
Latina women on Medicaid and uninsured Latino men reported the lowest usage of alcohol use disorder treatment
The rate of Latina females on Medicaid who received alcohol use disorder treatment was 3.2% compared to 9.3% of White males on Medicaid, a statistically significant difference. Only 1.8% of Latino men who were uninsured reported past year alcohol use disorder treatment utilization compared to 6.2% of uninsured White men, also statistically significant. Among those with private insurance, gender/race sub-groups exhibiting very similar rates of treatment seeking.
Disparities for Latina women on Medicaid and Latino men without insurance persisted even when adjusting for other individual factors
The study also examined whether factors like criminal legal system involvement (e.g., ever having been arrested), education (e.g., having a college degree), and employment status (e.g., unemployment) might explain these disparities. If they did, such disparities would abate when accounting for these factors. Even when accounting for these variables, however, the disparities for these Latinx subgroups among Medicaid/uninsured individuals persisted. This suggests other factors are at play.
Notably, Latina women who were on Medicaid used alcohol use disorder treatment less often than White men on Medicaid, independent of several indicators of clinical severity, such as co-occurring substance use disorders (e.g., opioid or stimulant), major depressive disorder, and overall current mental health. Similarly, uninsured Latino men reported lower alcohol use disorder treatment than White men who were uninsured. The authors controlled for factors relevant to healthcare access (e.g., education and criminal justice involvement) but found that these disparities persisted. This suggests unique barriers to treatment seeking for Latinx individuals in lower socioeconomic strata. Such barriers may be grounded in working class Latinx culture or language barriers in these under-resourced Spanish-speaking communities though such post-hoc explanations were not tested here. Interestingly, in another representative sample of US adults with alcohol use disorder, Latinx individuals were also less likely to attend Alcoholics Anonymous (AA) than their White counterparts. Given that AA is a free resource in the communities where people live and work, barriers to Latinx help-seeking may be unlikely to be financially driven, and possibly more likely to be grounded in cultural or language differences, but more explicit focused research is needed to understand the exact causes of these disparities.
These findings underscore the need for tailored strategies that address structural barriers within the U.S. healthcare system, especially for Medicaid enrollees, who often include racial and ethnic minoritized populations. Addressing these disparities can inform targeted policy adjustments, such as enhancing Medicaid coverage for alcohol use disorder treatments, expanding access to culturally specific and culturally sensitive support services, and strengthening provider networks in communities with high unmet treatment needs.
The current study used a narrow definition of alcohol use disorder treatment- alcohol use disorder treatment in specialty care facilities (e.g., inpatient rehabilitation centers). This likely only captured treatment for the most severe cases of alcohol use disorder and ignores the myriad other treatment options available for alcohol use disorder treatment (e.g., medications like naltrexone). It is possible that this narrow definition artificially deflated rates of alcohol use disorder treatment among participants.
The study employed national survey data which used the older DSM-IV “abuse” and “dependence” diagnostic categories which are not exactly the same as the current single “alcohol use disorder” diagnostic category used in the DSM 5. Consequently, results in this study may not comport completely with current diagnoses of alcohol use disorder.
Though analyses examining disparities in service utilization were independent of several clinical variables including co-occurring substance use disorders, the study did not include measures of alcohol use disorder severity or chronicity. To the extent that any clinical severity measures not included in analyses may have differed among groups, these may have partly explained treatment usage differences.
Interviewers for the National Survey on Drugs use and Health are instructed to report the respondent’s gender based on their “own assessment” (i.e., that of the interviewer). This approach to gender measurement may be problematic for some. First, it is unclear what “own assessment” means- it can be assumed this indicates that interviewers visually assessed participants and assumed their gender based on secondary sex characteristics and/or other gender signifiers. Given that participants do not self-report gender, there is no way to confirm if the interviewers’ assumptions about gender are accurate. Second, given that there are only 2 categories for gender in this study (“male” or “female”) there is no way to determine how treatment disparities may vary across transgender/non-binary populations. This is an issue as there are disparities in substance use care between cisgender and transgender populations.
Due to concerns about statistical power the author restricted their measurement of race/ethnicity to Black, Hispanic, and White respondents. This obscures other potentially significant intersectional health disparities across other marginalized groups. For example, research suggests that within the Asian American community, notable disparities in alcohol use disorder exist across the life course. Disparities among American Indian and Alaska Natives have also been noted. Treatment access may vary at the intersection of other racially marginalized groups, but these data cannot shed light on this phenomenon.
BOTTOM LINE
This study found that alcohol use disorder treatment usage is underutilized by those in the US who could potentially benefit from it. Only 5.4% of sampled adults with alcohol use disorder reported receiving specialty alcohol use disorder treatment. Additionally, this study highlights significant disparities in alcohol use disorder treatment access among uninsured and Medicaid-enrolled Hispanic individuals in the US. Latino men without insurance and Latina women with Medicaid coverage were found to utilize services less. These findings suggest that marginalized communities face compounded challenges in obtaining substance use disorder care. Improving Medicaid’s reach and culturally tailoring support to better serve the Latino community may help address these alcohol treatment disparities. Identifying and addressing alcohol treatment service gaps is essential to reducing health inequities and improving alcohol-related health outcomes in the US.
For individuals and families seeking recovery: The present study found that most people who had alcohol use disorder did not receive treatment. This suggests that individuals and families seeking recovery from alcohol use disorder may need to explore a variety of treatment options. For example, utilizing mutual help groups like Alcoholics Anonymous if faced with barriers related to insurance coverage or provider availability. However, it is also important to point out that the Latino individuals on Medicaid and who were uninsured were even less likely to receive alcohol use treatment. For those from the Latino community it may be helpful to seek out culturally specific recovery groups. Additionally, families and individuals may want to consider seeking providers that prioritize culturally humility in care, as these providers may better equipped to meet the unique needs of minoritized community members in recovery.
For treatment professionals and treatment systems: The present study suggests that alcohol use disorder treatment is underutilized in the US- particularly by Hispanic individuals who are on Medicaid or who are uninsured. More research is needed to understand the exact reasons for this. It may be important for those working within treatment systems to prioritize culturally responsive care and accessibility. Professionals would do well to practice cultural humility– that is engage in an ongoing practice of self-reflection of social positionality and engage in active listening with patients to better understand their needs. Furthermore, treatment systems could make structural changes designed to improve access to care. For example, expanding services for Medicaid recipients and offering sliding-scale or low-cost options for uninsured individuals. To better serve the Hispanic community, such changes could also include providing bilingual patient advocates.
For scientists: Scientists could help uncover unique reasons for potential underutilization of alcohol use treatment among the US population. Such work could focus on how variations in Medicaid coverage might be associated with different access to alcohol use disorder treatment. That is, although Medicaid is a national program, individual states decide how to implement it (e.g., enrollment eligibility). In addition, future research would do well to investigate the specific ways intersectional identities impact alcohol treatment seeking. That is, while research has examined barriers to care across racial, ethnic, and gender identities, less work has been done examining how care access is influenced by the social forces acting upon these identities concurrently.
For policy makers: Policy makers could help address inequities for Latinx individuals who receive Medicaid or who are uninsured by expanding and improving access to alcohol use disorder treatment for underserved racial and ethnic minority groups. Policies that enhance Medicaid coverage for alcohol use disorder treatment and support providers who offer low-cost or sliding-scale options can significantly reduce treatment disparities, particularly for Hispanic individuals. Policymakers should also support initiatives for cultural humility training for healthcare providers, enabling them to deliver care that respects and aligns with patients’ cultural values and experiences. Additionally, funding should be allocated to community-based and minority-led treatment programs, which may be better positioned to serve culturally diverse communities effectively. Research funding that examines how social determinants of health—such as socioeconomic status, criminal justice involvement, and geographic location—impact treatment access and outcomes can further guide effective policy interventions. These steps would help create a more equitable healthcare system that improves both access and outcomes for those most affected by alcohol-related health disparities.
There are many effective therapies, medications, and recovery support options for individuals with alcohol use disorder. However, evidence suggests that treatment may be underutilized by many who need it. A common barrier to treatment is the cost of care. Regardless of insurance coverage, those needing treatment may not be able to afford it due to variability in the types of services covered by insurance. This is especially problematic for those on Medicaid– public health insurance for low-income people. Despite over 72 million people in the US being on Medicaid, there is evidence that this insurance modality may constrain options for patients interested in alcohol use disorder treatment. Medicaid also disproportionately serves racially/ethnically minority groups (e.g., Black and Hispanic Americans). Despite Medicaid being a critical provider of care in the US it is unclear how effective it is at providing alcohol treatment to patients. Separately, because Medicaid is available only to those in lower socioeconomic strata, it may be a marker for a host of other challenges that make it hard for individuals to access and remain in care (i.e., limited recovery capital). In addition, it is unknown if differences in alcohol treatment utilization exist across intersecting social identities (racial and ethnic minority groups and women). Identifying disparities with this intersectional framework can help inform strategies to address barriers to accessing care among marginalized groups. This study conducted an intersectional analysis of national survey data to determine how treatment usage varied across racial, ethnic, and gender identities as well as insurance coverage.
HOW WAS THIS STUDY CONDUCTED?
The study was a cross-sectional analysis of 3 years of pooled data (2017-2019) from the National Survey on Drug Use and Health. The National Survey on Drug Use and Health is an annual survey conducted by the Substance Use and Mental Health Services Administration (SAMHSA) to gather information on substance use and mental health issues among the US population. Data are collected across all 50 states and the District of Columbia. Only non-institutionalized (e.g., non-incarcerated) individuals 12 years or older are sampled.
Participants were included in the present analyses if they 1) met Diagnostic and Statistical Manual of Mental Disorders, 4th edition criteria for alcohol use disorder (i.e., “alcohol dependence” or “alcohol abuse”) in the past year, 2) reported only having Medicaid, private insurance, or being uninsured, and 3) identified as White, Black, or Latinx. The primary outcome of this study was past year alcohol use disorder treatment utilization. This was defined as receiving any kind of alcohol use disorder treatment in a specialty facility including hospitals (inpatient), rehabilitation facilities (inpatient or outpatient), or mental health centers.
The primary goal of the present study was to examine rates of alcohol use disorder treatment utilization among those who report alcohol use disorder symptomology. Specifically, this work set out to examine how alcohol use disorder treatment use varied based on an individual’s race, ethnicity, gender, and insurance coverage. To do this, the authors used multivariable logistic regression models– a type of statistical approach where the probability of an outcome is determined based on multiple independent variables, adjusting statistically for self-rated health status, co-occurring substance use disorders (e.g., stimulant or opioid use disorder in addition to alcohol use disorder), past-year major depressive episode (yes/no), elevated psychological distress (based on an accepted cut-off from a validated scale), age, marital status, and survey year (2017, 2018, or 2019). Through this analysis, the authors were able to demonstrate how actual rates of alcohol use disorder treatment varied across groups. In the present analysis the authors compared all groups to White men. The rational for this is that compared to other demographics, White men have higher income, lower unemployment, and more healthcare coverage. Data in the present analysis were weighted– that is adjusted for potential biases and differences between the target population and the sample.
The final sample was comprised of 7782 respondents from across the US. The sample consisted of White males (42%), White females (29%), Latino males (12%), Latina females (7%), Black males (6%), and Black females (5%). Most participants reported having private insurance (68.9%) with the remainder indicating they had Medicaid (15.7%) or were uninsured (15.4%). Participants’ age ranged from 18-64 years.
WHAT DID THIS STUDY FIND?
Only 5.4% of adults with an alcohol use disorder received alcohol use disorder treatment
The vast majority of US adults with alcohol use disorder did not receive specialty treatment. Treatment seeking rates were similar across participant race, ethnicity, gender, and insurance coverage.
Latina women on Medicaid and uninsured Latino men reported the lowest usage of alcohol use disorder treatment
The rate of Latina females on Medicaid who received alcohol use disorder treatment was 3.2% compared to 9.3% of White males on Medicaid, a statistically significant difference. Only 1.8% of Latino men who were uninsured reported past year alcohol use disorder treatment utilization compared to 6.2% of uninsured White men, also statistically significant. Among those with private insurance, gender/race sub-groups exhibiting very similar rates of treatment seeking.
Disparities for Latina women on Medicaid and Latino men without insurance persisted even when adjusting for other individual factors
The study also examined whether factors like criminal legal system involvement (e.g., ever having been arrested), education (e.g., having a college degree), and employment status (e.g., unemployment) might explain these disparities. If they did, such disparities would abate when accounting for these factors. Even when accounting for these variables, however, the disparities for these Latinx subgroups among Medicaid/uninsured individuals persisted. This suggests other factors are at play.
Notably, Latina women who were on Medicaid used alcohol use disorder treatment less often than White men on Medicaid, independent of several indicators of clinical severity, such as co-occurring substance use disorders (e.g., opioid or stimulant), major depressive disorder, and overall current mental health. Similarly, uninsured Latino men reported lower alcohol use disorder treatment than White men who were uninsured. The authors controlled for factors relevant to healthcare access (e.g., education and criminal justice involvement) but found that these disparities persisted. This suggests unique barriers to treatment seeking for Latinx individuals in lower socioeconomic strata. Such barriers may be grounded in working class Latinx culture or language barriers in these under-resourced Spanish-speaking communities though such post-hoc explanations were not tested here. Interestingly, in another representative sample of US adults with alcohol use disorder, Latinx individuals were also less likely to attend Alcoholics Anonymous (AA) than their White counterparts. Given that AA is a free resource in the communities where people live and work, barriers to Latinx help-seeking may be unlikely to be financially driven, and possibly more likely to be grounded in cultural or language differences, but more explicit focused research is needed to understand the exact causes of these disparities.
These findings underscore the need for tailored strategies that address structural barriers within the U.S. healthcare system, especially for Medicaid enrollees, who often include racial and ethnic minoritized populations. Addressing these disparities can inform targeted policy adjustments, such as enhancing Medicaid coverage for alcohol use disorder treatments, expanding access to culturally specific and culturally sensitive support services, and strengthening provider networks in communities with high unmet treatment needs.
The current study used a narrow definition of alcohol use disorder treatment- alcohol use disorder treatment in specialty care facilities (e.g., inpatient rehabilitation centers). This likely only captured treatment for the most severe cases of alcohol use disorder and ignores the myriad other treatment options available for alcohol use disorder treatment (e.g., medications like naltrexone). It is possible that this narrow definition artificially deflated rates of alcohol use disorder treatment among participants.
The study employed national survey data which used the older DSM-IV “abuse” and “dependence” diagnostic categories which are not exactly the same as the current single “alcohol use disorder” diagnostic category used in the DSM 5. Consequently, results in this study may not comport completely with current diagnoses of alcohol use disorder.
Though analyses examining disparities in service utilization were independent of several clinical variables including co-occurring substance use disorders, the study did not include measures of alcohol use disorder severity or chronicity. To the extent that any clinical severity measures not included in analyses may have differed among groups, these may have partly explained treatment usage differences.
Interviewers for the National Survey on Drugs use and Health are instructed to report the respondent’s gender based on their “own assessment” (i.e., that of the interviewer). This approach to gender measurement may be problematic for some. First, it is unclear what “own assessment” means- it can be assumed this indicates that interviewers visually assessed participants and assumed their gender based on secondary sex characteristics and/or other gender signifiers. Given that participants do not self-report gender, there is no way to confirm if the interviewers’ assumptions about gender are accurate. Second, given that there are only 2 categories for gender in this study (“male” or “female”) there is no way to determine how treatment disparities may vary across transgender/non-binary populations. This is an issue as there are disparities in substance use care between cisgender and transgender populations.
Due to concerns about statistical power the author restricted their measurement of race/ethnicity to Black, Hispanic, and White respondents. This obscures other potentially significant intersectional health disparities across other marginalized groups. For example, research suggests that within the Asian American community, notable disparities in alcohol use disorder exist across the life course. Disparities among American Indian and Alaska Natives have also been noted. Treatment access may vary at the intersection of other racially marginalized groups, but these data cannot shed light on this phenomenon.
BOTTOM LINE
This study found that alcohol use disorder treatment usage is underutilized by those in the US who could potentially benefit from it. Only 5.4% of sampled adults with alcohol use disorder reported receiving specialty alcohol use disorder treatment. Additionally, this study highlights significant disparities in alcohol use disorder treatment access among uninsured and Medicaid-enrolled Hispanic individuals in the US. Latino men without insurance and Latina women with Medicaid coverage were found to utilize services less. These findings suggest that marginalized communities face compounded challenges in obtaining substance use disorder care. Improving Medicaid’s reach and culturally tailoring support to better serve the Latino community may help address these alcohol treatment disparities. Identifying and addressing alcohol treatment service gaps is essential to reducing health inequities and improving alcohol-related health outcomes in the US.
For individuals and families seeking recovery: The present study found that most people who had alcohol use disorder did not receive treatment. This suggests that individuals and families seeking recovery from alcohol use disorder may need to explore a variety of treatment options. For example, utilizing mutual help groups like Alcoholics Anonymous if faced with barriers related to insurance coverage or provider availability. However, it is also important to point out that the Latino individuals on Medicaid and who were uninsured were even less likely to receive alcohol use treatment. For those from the Latino community it may be helpful to seek out culturally specific recovery groups. Additionally, families and individuals may want to consider seeking providers that prioritize culturally humility in care, as these providers may better equipped to meet the unique needs of minoritized community members in recovery.
For treatment professionals and treatment systems: The present study suggests that alcohol use disorder treatment is underutilized in the US- particularly by Hispanic individuals who are on Medicaid or who are uninsured. More research is needed to understand the exact reasons for this. It may be important for those working within treatment systems to prioritize culturally responsive care and accessibility. Professionals would do well to practice cultural humility– that is engage in an ongoing practice of self-reflection of social positionality and engage in active listening with patients to better understand their needs. Furthermore, treatment systems could make structural changes designed to improve access to care. For example, expanding services for Medicaid recipients and offering sliding-scale or low-cost options for uninsured individuals. To better serve the Hispanic community, such changes could also include providing bilingual patient advocates.
For scientists: Scientists could help uncover unique reasons for potential underutilization of alcohol use treatment among the US population. Such work could focus on how variations in Medicaid coverage might be associated with different access to alcohol use disorder treatment. That is, although Medicaid is a national program, individual states decide how to implement it (e.g., enrollment eligibility). In addition, future research would do well to investigate the specific ways intersectional identities impact alcohol treatment seeking. That is, while research has examined barriers to care across racial, ethnic, and gender identities, less work has been done examining how care access is influenced by the social forces acting upon these identities concurrently.
For policy makers: Policy makers could help address inequities for Latinx individuals who receive Medicaid or who are uninsured by expanding and improving access to alcohol use disorder treatment for underserved racial and ethnic minority groups. Policies that enhance Medicaid coverage for alcohol use disorder treatment and support providers who offer low-cost or sliding-scale options can significantly reduce treatment disparities, particularly for Hispanic individuals. Policymakers should also support initiatives for cultural humility training for healthcare providers, enabling them to deliver care that respects and aligns with patients’ cultural values and experiences. Additionally, funding should be allocated to community-based and minority-led treatment programs, which may be better positioned to serve culturally diverse communities effectively. Research funding that examines how social determinants of health—such as socioeconomic status, criminal justice involvement, and geographic location—impact treatment access and outcomes can further guide effective policy interventions. These steps would help create a more equitable healthcare system that improves both access and outcomes for those most affected by alcohol-related health disparities.
There are many effective therapies, medications, and recovery support options for individuals with alcohol use disorder. However, evidence suggests that treatment may be underutilized by many who need it. A common barrier to treatment is the cost of care. Regardless of insurance coverage, those needing treatment may not be able to afford it due to variability in the types of services covered by insurance. This is especially problematic for those on Medicaid– public health insurance for low-income people. Despite over 72 million people in the US being on Medicaid, there is evidence that this insurance modality may constrain options for patients interested in alcohol use disorder treatment. Medicaid also disproportionately serves racially/ethnically minority groups (e.g., Black and Hispanic Americans). Despite Medicaid being a critical provider of care in the US it is unclear how effective it is at providing alcohol treatment to patients. Separately, because Medicaid is available only to those in lower socioeconomic strata, it may be a marker for a host of other challenges that make it hard for individuals to access and remain in care (i.e., limited recovery capital). In addition, it is unknown if differences in alcohol treatment utilization exist across intersecting social identities (racial and ethnic minority groups and women). Identifying disparities with this intersectional framework can help inform strategies to address barriers to accessing care among marginalized groups. This study conducted an intersectional analysis of national survey data to determine how treatment usage varied across racial, ethnic, and gender identities as well as insurance coverage.
HOW WAS THIS STUDY CONDUCTED?
The study was a cross-sectional analysis of 3 years of pooled data (2017-2019) from the National Survey on Drug Use and Health. The National Survey on Drug Use and Health is an annual survey conducted by the Substance Use and Mental Health Services Administration (SAMHSA) to gather information on substance use and mental health issues among the US population. Data are collected across all 50 states and the District of Columbia. Only non-institutionalized (e.g., non-incarcerated) individuals 12 years or older are sampled.
Participants were included in the present analyses if they 1) met Diagnostic and Statistical Manual of Mental Disorders, 4th edition criteria for alcohol use disorder (i.e., “alcohol dependence” or “alcohol abuse”) in the past year, 2) reported only having Medicaid, private insurance, or being uninsured, and 3) identified as White, Black, or Latinx. The primary outcome of this study was past year alcohol use disorder treatment utilization. This was defined as receiving any kind of alcohol use disorder treatment in a specialty facility including hospitals (inpatient), rehabilitation facilities (inpatient or outpatient), or mental health centers.
The primary goal of the present study was to examine rates of alcohol use disorder treatment utilization among those who report alcohol use disorder symptomology. Specifically, this work set out to examine how alcohol use disorder treatment use varied based on an individual’s race, ethnicity, gender, and insurance coverage. To do this, the authors used multivariable logistic regression models– a type of statistical approach where the probability of an outcome is determined based on multiple independent variables, adjusting statistically for self-rated health status, co-occurring substance use disorders (e.g., stimulant or opioid use disorder in addition to alcohol use disorder), past-year major depressive episode (yes/no), elevated psychological distress (based on an accepted cut-off from a validated scale), age, marital status, and survey year (2017, 2018, or 2019). Through this analysis, the authors were able to demonstrate how actual rates of alcohol use disorder treatment varied across groups. In the present analysis the authors compared all groups to White men. The rational for this is that compared to other demographics, White men have higher income, lower unemployment, and more healthcare coverage. Data in the present analysis were weighted– that is adjusted for potential biases and differences between the target population and the sample.
The final sample was comprised of 7782 respondents from across the US. The sample consisted of White males (42%), White females (29%), Latino males (12%), Latina females (7%), Black males (6%), and Black females (5%). Most participants reported having private insurance (68.9%) with the remainder indicating they had Medicaid (15.7%) or were uninsured (15.4%). Participants’ age ranged from 18-64 years.
WHAT DID THIS STUDY FIND?
Only 5.4% of adults with an alcohol use disorder received alcohol use disorder treatment
The vast majority of US adults with alcohol use disorder did not receive specialty treatment. Treatment seeking rates were similar across participant race, ethnicity, gender, and insurance coverage.
Latina women on Medicaid and uninsured Latino men reported the lowest usage of alcohol use disorder treatment
The rate of Latina females on Medicaid who received alcohol use disorder treatment was 3.2% compared to 9.3% of White males on Medicaid, a statistically significant difference. Only 1.8% of Latino men who were uninsured reported past year alcohol use disorder treatment utilization compared to 6.2% of uninsured White men, also statistically significant. Among those with private insurance, gender/race sub-groups exhibiting very similar rates of treatment seeking.
Disparities for Latina women on Medicaid and Latino men without insurance persisted even when adjusting for other individual factors
The study also examined whether factors like criminal legal system involvement (e.g., ever having been arrested), education (e.g., having a college degree), and employment status (e.g., unemployment) might explain these disparities. If they did, such disparities would abate when accounting for these factors. Even when accounting for these variables, however, the disparities for these Latinx subgroups among Medicaid/uninsured individuals persisted. This suggests other factors are at play.
Notably, Latina women who were on Medicaid used alcohol use disorder treatment less often than White men on Medicaid, independent of several indicators of clinical severity, such as co-occurring substance use disorders (e.g., opioid or stimulant), major depressive disorder, and overall current mental health. Similarly, uninsured Latino men reported lower alcohol use disorder treatment than White men who were uninsured. The authors controlled for factors relevant to healthcare access (e.g., education and criminal justice involvement) but found that these disparities persisted. This suggests unique barriers to treatment seeking for Latinx individuals in lower socioeconomic strata. Such barriers may be grounded in working class Latinx culture or language barriers in these under-resourced Spanish-speaking communities though such post-hoc explanations were not tested here. Interestingly, in another representative sample of US adults with alcohol use disorder, Latinx individuals were also less likely to attend Alcoholics Anonymous (AA) than their White counterparts. Given that AA is a free resource in the communities where people live and work, barriers to Latinx help-seeking may be unlikely to be financially driven, and possibly more likely to be grounded in cultural or language differences, but more explicit focused research is needed to understand the exact causes of these disparities.
These findings underscore the need for tailored strategies that address structural barriers within the U.S. healthcare system, especially for Medicaid enrollees, who often include racial and ethnic minoritized populations. Addressing these disparities can inform targeted policy adjustments, such as enhancing Medicaid coverage for alcohol use disorder treatments, expanding access to culturally specific and culturally sensitive support services, and strengthening provider networks in communities with high unmet treatment needs.
The current study used a narrow definition of alcohol use disorder treatment- alcohol use disorder treatment in specialty care facilities (e.g., inpatient rehabilitation centers). This likely only captured treatment for the most severe cases of alcohol use disorder and ignores the myriad other treatment options available for alcohol use disorder treatment (e.g., medications like naltrexone). It is possible that this narrow definition artificially deflated rates of alcohol use disorder treatment among participants.
The study employed national survey data which used the older DSM-IV “abuse” and “dependence” diagnostic categories which are not exactly the same as the current single “alcohol use disorder” diagnostic category used in the DSM 5. Consequently, results in this study may not comport completely with current diagnoses of alcohol use disorder.
Though analyses examining disparities in service utilization were independent of several clinical variables including co-occurring substance use disorders, the study did not include measures of alcohol use disorder severity or chronicity. To the extent that any clinical severity measures not included in analyses may have differed among groups, these may have partly explained treatment usage differences.
Interviewers for the National Survey on Drugs use and Health are instructed to report the respondent’s gender based on their “own assessment” (i.e., that of the interviewer). This approach to gender measurement may be problematic for some. First, it is unclear what “own assessment” means- it can be assumed this indicates that interviewers visually assessed participants and assumed their gender based on secondary sex characteristics and/or other gender signifiers. Given that participants do not self-report gender, there is no way to confirm if the interviewers’ assumptions about gender are accurate. Second, given that there are only 2 categories for gender in this study (“male” or “female”) there is no way to determine how treatment disparities may vary across transgender/non-binary populations. This is an issue as there are disparities in substance use care between cisgender and transgender populations.
Due to concerns about statistical power the author restricted their measurement of race/ethnicity to Black, Hispanic, and White respondents. This obscures other potentially significant intersectional health disparities across other marginalized groups. For example, research suggests that within the Asian American community, notable disparities in alcohol use disorder exist across the life course. Disparities among American Indian and Alaska Natives have also been noted. Treatment access may vary at the intersection of other racially marginalized groups, but these data cannot shed light on this phenomenon.
BOTTOM LINE
This study found that alcohol use disorder treatment usage is underutilized by those in the US who could potentially benefit from it. Only 5.4% of sampled adults with alcohol use disorder reported receiving specialty alcohol use disorder treatment. Additionally, this study highlights significant disparities in alcohol use disorder treatment access among uninsured and Medicaid-enrolled Hispanic individuals in the US. Latino men without insurance and Latina women with Medicaid coverage were found to utilize services less. These findings suggest that marginalized communities face compounded challenges in obtaining substance use disorder care. Improving Medicaid’s reach and culturally tailoring support to better serve the Latino community may help address these alcohol treatment disparities. Identifying and addressing alcohol treatment service gaps is essential to reducing health inequities and improving alcohol-related health outcomes in the US.
For individuals and families seeking recovery: The present study found that most people who had alcohol use disorder did not receive treatment. This suggests that individuals and families seeking recovery from alcohol use disorder may need to explore a variety of treatment options. For example, utilizing mutual help groups like Alcoholics Anonymous if faced with barriers related to insurance coverage or provider availability. However, it is also important to point out that the Latino individuals on Medicaid and who were uninsured were even less likely to receive alcohol use treatment. For those from the Latino community it may be helpful to seek out culturally specific recovery groups. Additionally, families and individuals may want to consider seeking providers that prioritize culturally humility in care, as these providers may better equipped to meet the unique needs of minoritized community members in recovery.
For treatment professionals and treatment systems: The present study suggests that alcohol use disorder treatment is underutilized in the US- particularly by Hispanic individuals who are on Medicaid or who are uninsured. More research is needed to understand the exact reasons for this. It may be important for those working within treatment systems to prioritize culturally responsive care and accessibility. Professionals would do well to practice cultural humility– that is engage in an ongoing practice of self-reflection of social positionality and engage in active listening with patients to better understand their needs. Furthermore, treatment systems could make structural changes designed to improve access to care. For example, expanding services for Medicaid recipients and offering sliding-scale or low-cost options for uninsured individuals. To better serve the Hispanic community, such changes could also include providing bilingual patient advocates.
For scientists: Scientists could help uncover unique reasons for potential underutilization of alcohol use treatment among the US population. Such work could focus on how variations in Medicaid coverage might be associated with different access to alcohol use disorder treatment. That is, although Medicaid is a national program, individual states decide how to implement it (e.g., enrollment eligibility). In addition, future research would do well to investigate the specific ways intersectional identities impact alcohol treatment seeking. That is, while research has examined barriers to care across racial, ethnic, and gender identities, less work has been done examining how care access is influenced by the social forces acting upon these identities concurrently.
For policy makers: Policy makers could help address inequities for Latinx individuals who receive Medicaid or who are uninsured by expanding and improving access to alcohol use disorder treatment for underserved racial and ethnic minority groups. Policies that enhance Medicaid coverage for alcohol use disorder treatment and support providers who offer low-cost or sliding-scale options can significantly reduce treatment disparities, particularly for Hispanic individuals. Policymakers should also support initiatives for cultural humility training for healthcare providers, enabling them to deliver care that respects and aligns with patients’ cultural values and experiences. Additionally, funding should be allocated to community-based and minority-led treatment programs, which may be better positioned to serve culturally diverse communities effectively. Research funding that examines how social determinants of health—such as socioeconomic status, criminal justice involvement, and geographic location—impact treatment access and outcomes can further guide effective policy interventions. These steps would help create a more equitable healthcare system that improves both access and outcomes for those most affected by alcohol-related health disparities.