
Do Young Adults Need Both Clinical & Non-clinical Continuing Care After Residential Treatment?
Relative to adolescents and older adults, emerging adults (18-24 years old in the current study) face unique recovery challenges related to their social and contexts, such as lower availability of recovery-supportive peers and environments.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Recent studies have shown emerging adults can benefit from attending residential treatment as well as participating in 12-step mutual-help organizations. However, perhaps due to their unique recovery challenges, their treatment outcomes tend to be worse than older and younger treatment seekers. Continuing care is a crucial piece of a comprehensive treatment approach – it can be professional (e.g., follow-up substance use disorder [SUD] relapse prevention groups) or non-professional (12-step groups, like Alcoholics Anonymous [AA] or Narcotics Anonymous [NA]).
However, very little is known about whether and to what extent emerging adults benefit from engagement with professional continuing care after residential treatment, and even less is known about the combined effects of professional and non-professional services.
HOW WAS THIS STUDY CONDUCTED?
The current study examined engagement with professional continuing care among 284 emerging adults using a naturalistic design that followed patients up to 1 year after an index episode of residential treatment (25 days, on average). Authors used sophisticated analyses (hierarchical linear models) to test whether patients derived recovery benefit (defined as continuous abstinence during a follow-up period) from four types of professional continuing care services for substance use disorder – further residential/inpatient treatment, outpatient treatment, residing in a sober living program, and medication-assisted treatment – across 1-month, 3-month, 6-month, and 12-month follow-up assessments.
Finally, they examined whether patients benefited from active participation in AA/NA (e.g., having a sponsor, contact with other members outside meetings, and verbal participation in meetings) across the same four follow-ups, when statistically controlling for the effects of professional services and other individual factors (e.g., recovery motivation at treatment intake). In other words, the authors determined whether participants received additional benefit from AA/NA over and above any benefits derived from professional treatment.
WHAT DID THIS STUDY FIND?
The young adults were likely to engage with follow-up residential treatment (a less intensive step-down program, relative to the more structured initial residential treatment episode). Outpatient treatment engagement was less likely with no more than 20% engaging with these services in any follow-up period. Between 20 and 35% resided at a recovery residence. Participants were very involved with 12-step groups, actively engaging with 5 or more activities (out of 8) on average across the follow-up assessments.
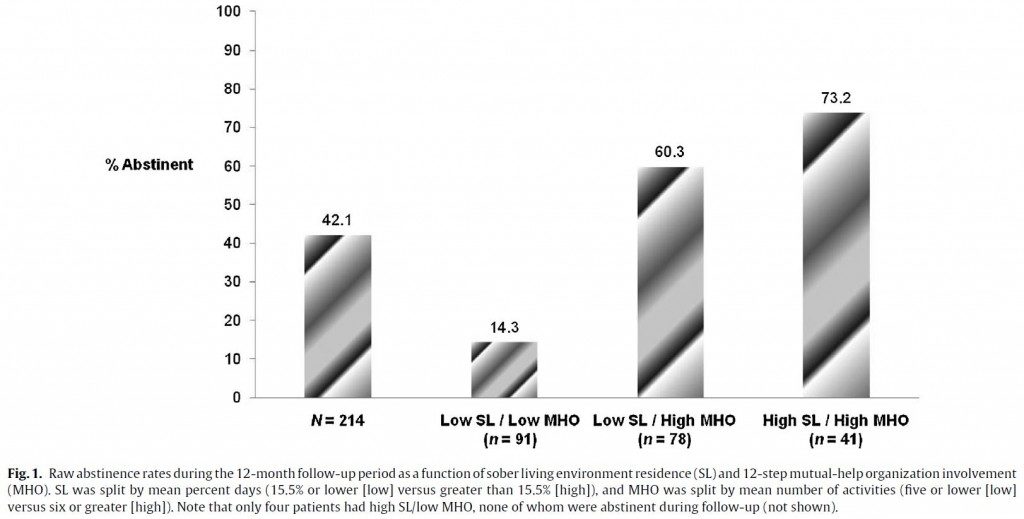
Apart from medication-assisted treatment, patients derived benefit from each of the professional continuing care services. For example, patients who resided in a recovery residence for all days during a follow-up period were 6.2 times more likely to be continuously abstinent than patients who did not reside in such a program.
Over and above the effects of professional services, active 12-step involvement conferred additional recovery benefit. For example, patients involved in 5 12-step activities (the lowest mean number of activities across all follow-ups) were 3.2 times more likely to be abstinent than patients not involved in 12-step groups – even when controlling for the powerful effects of residing in structured settings among other variables. Statistically speaking, because the professional service effects decreased in magnitude when including 12-step involvement in the tested models, it may be that part of the benefit of professional services is explained by ability to link patients to community-based 12-step groups.
The current study suggests that emerging adults benefit from both professional and non-professional AA/NA services after an episode of residential treatment. Furthermore, the effects of professional service engagement, such as residing in a recovery residence and active involvement in 12-step groups, may be additive, meaning that each is helpful, but together they offer a more potent recovery benefit.
WHY IS THIS STUDY IMPORTANT?
Based on the current study, residential programs should strongly consider engaging patients with structured and supportive continuing care services and link patients to community-based 12-step mutual-help organizations like AA and NA.
- LIMITATIONS
-
- The sample was predominantly male (about 75%) and Caucasian (about 95%), and recruited from a high quality residential 12-step-oriented treatment program. Thus, caution must be taken in generalizing to the entire population of emerging adults in substance use disorder treatment.
- Also, although authors controlled for alternative explanations for the benefit of continuing care, because patients were not randomized to continuing care services, enhanced abstinence rates observed as a function of engagement cannot be attributed entirely to the continuing care services.
NEXT STEPS
Follow-up studies using randomized designs may test whether continuing care approaches previously supported in the treatment of adolescents (see here) and adults (see here) might further enhance outcomes for emerging adults.
BOTTOM LINE
- For individuals & families seeking recovery: Continuing care services after treatment is likely to improve your chances of recovery.
- For scientists: More research, including randomized trials and studies with more ethnically diverse samples from other treatment settings, is needed to say more definitively whether emerging adults benefit from substance use disorder continuing care.
- For policy makers: Consider initiatives to fund and/or reimburse for continuing care services such as recovery residences. Engagement with these services may enhance treatment outcomes and is highly cost-effective in older adults (see here).
- For treatment professionals and treatment systems: Strongly consider working with your patients to develop a thorough continuing care plan that includes a structured, recovery residence at least within the first several months of discharge, and active involvement in 12-step mutual-help groups.
CITATIONS
Bergman, B. G., Hoeppner, B. B., Nelson, L. M., Slaymaker, V., & Kelly, J. F. (2015). The effects of continuing care on emerging adult outcomes following residential addiction treatment. Drug Alcohol Depend. doi: 10.1016/j.drugalcdep.2015.05.017
**Note: One or more authors of this study were Recovery Research Institute Staff, including the director and/or other research scientists. As with all summaries, staff made the greatest possible effort to recognize and account for any potential biases in the review of this article.
