Does reduced craving explain why opioid use disorder medications are helpful?
The relationship between opioid use disorder medication treatment, opioid craving, and illicit opioid use is not entirely understood. This study investigated the extent to which craving explained the effects of buprenorphine and methadone treatment on opioid use.
Medication treatments for opioid use disorder like buprenorphine and methadone ease symptoms of opioid withdrawal and craving, and ultimately help to support reduced substance use and positive recovery outcomes. However, many individuals continue to use illicit opioids during medication treatment. Craving has been proposed as a possible factor contributing to ongoing opioid misuse during treatment, but research examining craving is limited and has yielded mixedfindings thus far, possibly due to the varying research methods used across different studies (e.g., different populations of interest, length of time between assessment of craving and opioid use). For example, one study observed no association between pre-treatment craving and subsequent opioid use during 12-weeks of buprenorphine treatment for prescription opioid use disorder. Another investigation found that craving predicted subsequent opioid use (2-week intervals) during a 3-month course of buprenorphine treatment for opioid use disorder. While another study conducted among individuals with heroin use problems found that craving was associated with heroin use in subsequent days.
Recent research suggests that, relative to methadone, buprenorphine treatment may result in less opioid use and fewer craving symptoms. Yet, the small number of studies conducted prevent formal conclusions and the extent to which reduced craving impacts the relationship between medication treatment type and illicit opioid use has yet to be determined. Understanding the factors that influence medication treatment progress and outcomes is important because it can ultimately reveal risk factors that can help guide individualized treatment approaches and enhance positive treatment outcomes.
To better understand the role of craving in medication treatment, this study examined the effect of medication treatment (i.e. buprenorphine vs. methadone) on illicit opioid use and craving, the relationship between craving and opioid use, and the extent to which craving explained the relationship between medication type and opioid use.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of a multi-site randomized controlled trial (i.e. OPTIMA trial) that examined the relationship between medication treatment (i.e. buprenorphine vs. methadone), illicit opioid use, and opioid craving among 270 adults with “prescription-type” opioid use disorder, which includes prescription opioids and synthetic opioids like fentanyl. Though details are not provided regarding the specific opioid use disorder diagnosis of the participants, one-third used fentanyl at some point during the study including baseline. While two-thirds had a lifetime history of heroin use, those for whom heroin was the most commonly used opioid in the last 30 days were excluded.
More specifically, this study assessed:
(1) The effect of medication treatment type (buprenorphine vs. methadone) on past-week opioid use and past-24-hour opioid craving, averaged across the 24-week trial.
(2) The relationship between average craving and average opioid use over the 24-week trial.
(3) The degree to which craving explains the relationship between medication type and opioid use, including the direct effect (effect of medication treatment on opioid use taking into account craving), indirect effect (effect of medication treatment on opioid use that operates through craving), and total effect (indirect + direct effect) of medication treatment on opioid use.
Participants were randomized to receive 24 weeks of flexible take-home buprenorphine (n=137) or supervised methadone (n=133) treatment at 1 of 7 participating research sites across Canada. Take-home doses were provided by study physicians at their discretion. Take-home doses were also available for methadone but, if provided, they were prescribed later in the course of treatment than buprenorphine take-home doses, given their different safety profiles (e.g., time to stabilization, overdose risk) during the early stages of treatment. Study prescribers were advised to offer buprenorphine patients 1 week’s worth of take-home doses after two weeks of treatment, and 2 weeks’ worth of take-home doses after 4 weeks of treatment. For methadone, prescribers were advised to offer patients take-home doses of methadone after 2-3 months of treatment, but only if they presented as clinically stable. Participants were not excluded from the study if they discontinued their medication treatment or switched from one medication type to another (n=30 individuals receiving buprenorphine & n=17 receiving methadone switch to a different medication type). However, only 28% of those randomized to either methadone or buprenorphine were receiving any opioid agonist medication by the end of the 24-week study period – meaning 72% were not taking buprenorphine or methadone 6 months later. In the study analyses, buprenorphine and methadone groups were determined using the participant’s originally assigned medication treatment at the start of the study.
Opioid craving over the past 24 hours was measured with the Brief Substance Craving Scale at baseline (i.e. before starting treatment) and weeks 2, 6, 10, 14, 18 and 22 after treatment initiation, with possible scores ranging from 0 (no craving) to 64 (extreme craving). Past-week opioid use was measured with the Timeline Followback at baseline (past 30-days opioid use) and every 2 weeks (opioid use since the last study visit) until the end of the study. In their analyses, the researchers examined the number of days that participants used opioids in the week following craving-scale administration. If opioid-use data in the week following a given craving assessment was missing, opioid use reported for the week prior to baseline was used, with the assumption that the participant had returned to their former opioid use patterns at the time of the missed assessment. Of note, study attrition was relatively high, with only about 39% of those assigned to buprenorphine and 47% of those assigned to methadone providing data on craving and substance use at the 22-week follow up. All analyses controlled for trial site, lifetime history of heroin use, study visit, opioid positive drug tests at last visit, sex, age, fentanyl use at baseline, and anxiety and depressive symptoms at baseline.
The majority of participants were White (67%) men (66%) in their late thirties, who had a moderate or severe prescription-type opioid use disorder (e.g., fentanyl). About 45% of the sample had unstable housing and psychiatric comorbidities, and 69% had a lifetime history of heroin use.
WHAT DID THIS STUDY FIND?
Assignment to buprenorphine associated with marginally less opioid use and craving
Relative to individuals who were assigned to methadone treatment, those assigned to buprenorphine had an average of 0.6 fewer days of weekly opioid use and 1 point lower on the craving scale, during the 24-week follow-up. In both treatment groups, greater opioid craving was associated with a greater number of days using opioids in the following week.
Craving accounted for one-quarter of the effect of treatment on opioid use
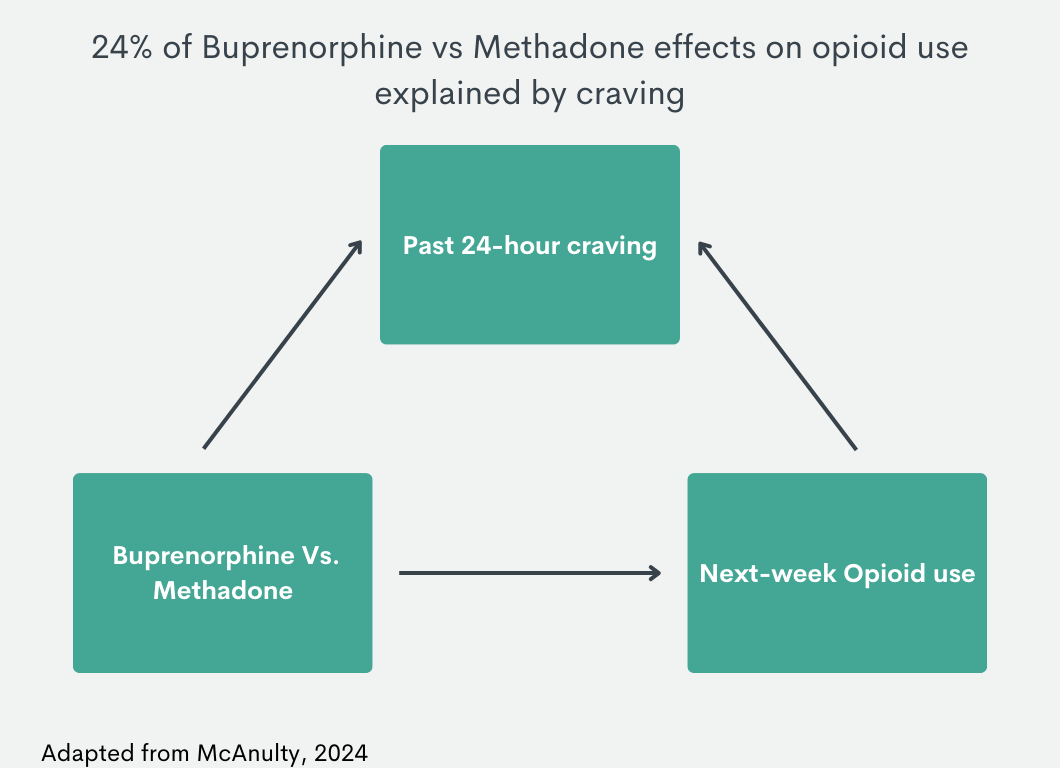
Taken together, craving accounted for about 24% (i.e. indirect effect divided by total effect) of the effect of medication treatment type on opioid use, and the magnitude of this mediating effect was consistent across the 2 medication treatments (24.1% for buprenorphine and 23.1% for methadone).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study, opioid craving partially mediated the effect of medication treatment type on next-week opioid use, accounting for about one-quarter of the effect observed. This means that differences in opioid use between the methadone and buprenorphine groups were partially explained by differences in craving (i.e. lower craving partially accounted for less frequent opioid use in the buprenorphine group). Given that about 75% of the effect of treatment type on opioid use was not explained by craving, additional factors are likely to explain this effect. For example, severity of withdrawal symptoms and mental health comorbidities often improve during buprenorphine and methadone treatment, and these factors may variably influence the relationship between medication treatment and opioid use depending on the medication type. Use of adjunct services like psychotherapy (e.g., people often learn additional alternative skills to manage cravings without resorting to opioid use) and mutual-help organizations (e.g., Narcotics Anonymous) as well as patient characteristics like impulsivity may also influence the relationship between medication treatment, craving, and opioid use. Still, reduced craving is very likely an important factor to consider with regard to successful treatment progress and outcomes, like reductions in illicit opioid use.
It is also worth noting that craving levels in this study sample were relatively low in both treatment groups, warranting additional study in populations experiencing a greater degree of opioid craving during treatment. Moreover, participant retention in the study and retention in treatment can impact statistical analyses and results. In this study, craving and opioid use measures gathered after baseline were only available for 39% – 61% of participants across study visits, less than one-third of participants continued with their assigned medication treatment throughout the study, and only 30% were taking an opioid agonist medication of any kind by the end of the 6-month trial. Thus, this study may reflect findings from individuals who have more follow up data and may therefore represent individuals who are more likely to benefit from treatment. Medication dose is also an important factor to consider, which this study did not control for. Thus, additional longitudinal research is required to make formal conclusions about the relationship between medication treatment, craving, and opioid use. Nonetheless, research on this topic is limited and mixed findings exist, demanding additional research with consideration of medication type, dose, and other factors relevant to craving, opioid use, and treatment effectiveness (e.g., primary opioid of choice, patient demographics, use of additional therapies/services, comorbidities).
This study’s findings are somewhat inconsistent with prior research showing that substance use outcomes are by and large comparable between individuals receiving buprenorphine and methadone treatment. This study suggested that, relative to methadone, buprenorphine may be associated with lower levels of craving and less frequent opioid use, although admittedly the difference observed here was small (0.6 fewer days of weekly opioid use and 1 point lower on the craving scale) and more people assigned to buprenorphine switched to another medication – but were included in the “buprenorphine group”.
Overall, the clinical implications in this study are unclear and require further investigation. In both treatment groups, higher levels of opioid craving were associated with more frequent opioid use in the following week. Similar findings have been observed in studies of buprenorphine or methadone treatment, where a relationship between opioid craving and use has been demonstrated among individuals with prescription opioid use disorder, individuals with a primary heroin use problem, and individuals with comorbid opioid and cocaine use disorders. Models that incorporate other variables such as the level of motivation to reduce or not use opioids and patients’ ability to deploy alternative coping skills to not use opioids when experiencing craving are also important to test. Additional research will help shed additional light on the complex dynamic relationship between craving and illicit opioid use during opioid use disorder medication treatment.
Individuals who did not continue with their assigned medication during the study were included in analyses and only a small number of participants were adherent to treatment over the entire 24-week trial, which may have influenced outcomes. It is also possible that individuals who engaged in ongoing illicit opioid use may have experienced lower levels of craving, which could have weakened the relationship between craving and subsequent opioid use.
Findings may not apply to individuals with a primary heroin problem or unstable comorbid psychiatric/physical conditions, as these were exclusionary in the current study.
This study was conducted in Canada and treatment conditions for buprenorphine and methadone generally followed Canadian treatment guidelines, which may differ from the prescribing and treatment guidelines of other countries. Additionally, prescribers from this study were allowed to use their clinical judgment to prescribe buprenorphine and methadone outside of the prescribing guidelines (e.g., changing the schedule of dose increases, changing the target dose, etc.), and it is unclear how this may have affected outcomes.
BOTTOM LINE
Craving accounted for about one-quarter of the effect of medication treatment type on opioid use. This study highlights the important role that craving plays in illicit opioid use during medication treatment, and also suggests that there are likely many other individual factors (e.g., impulsivity, mental health comorbidities, medication dose, and adherence) contributing to the effects of buprenorphine and methadone treatment on opioid use that were not assessed here. Additional research will help clarify the individual, treatment, and system-level factors that influence medication treatment progress and outcomes, which can ultimately help inform individualized treatment approaches that enhance positive recovery outcomes.
For individuals and families seeking recovery: Though additional research is needed to make formal conclusions about the relationship between medication treatments for opioid use disorder, craving, and opioid use, craving appears to be an important factor to consider when it comes to patient progress and outcomes. People who are undergoing medication treatment and experiencing ongoing opioid craving are encouraged to speak with their doctors about increasing medication doses or switching to a different medication to reduce opioid craving and, in turn, reduce risk of illicit opioid use.
For treatment professionals and treatment systems: Studies like this help us better understand the factors that influence opioid use disorder treatment outcomes, which can ultimately help guide individualized treatment approaches and inform patient risk factors that need addressing to promote successful treatment progress and outcomes. Given that craving accounted for ~25% of the effect of medication treatment on opioid use, assessing craving in healthcare settings is likely to be important for gauging a patient’s treatment progress and might help inform potential tweaks to treatment plans. Still, there are likely many other factors that influence patient outcomes that weren’t assessed here such as level of recovery motivation and patients’ levels of cognitive and behavioral coping skills to address craving in other ways beyond using opioids.
For scientists: Additional research examining the mediating effect of craving on the relationship between medication treatment and opioid use is needed among individuals who are adherent to treatment and in studies with higher follow-up rates. Evaluation of other potential mediators is needed, including withdrawal symptoms, mental-health comorbidities, impulsivity, medication dose/regimen, and use of adjunct treatments and recovery support services, among others. Assessment of medications other than sublingual buprenorphine and oral methadone will also help enhance our understanding of medication treatment and its relationship to patient outcomes.
For policy makers: Understanding how opioid use disorder medication treatments impact patient progress and outcomes can help inform individualized treatment approaches that enhance positive outcomes and sustained recovery to help address the ongoing opioid epidemic. Given mixed findings among a small number of studies examining the relationship between medication treatment, illicit opioid use, and factors that mediate this relationship, additional research funds will help clarify inconsistent findings, and will expand our understanding of the factors influencing treatment and how they can be leveraged to improve treatment efficacy.
Medication treatments for opioid use disorder like buprenorphine and methadone ease symptoms of opioid withdrawal and craving, and ultimately help to support reduced substance use and positive recovery outcomes. However, many individuals continue to use illicit opioids during medication treatment. Craving has been proposed as a possible factor contributing to ongoing opioid misuse during treatment, but research examining craving is limited and has yielded mixedfindings thus far, possibly due to the varying research methods used across different studies (e.g., different populations of interest, length of time between assessment of craving and opioid use). For example, one study observed no association between pre-treatment craving and subsequent opioid use during 12-weeks of buprenorphine treatment for prescription opioid use disorder. Another investigation found that craving predicted subsequent opioid use (2-week intervals) during a 3-month course of buprenorphine treatment for opioid use disorder. While another study conducted among individuals with heroin use problems found that craving was associated with heroin use in subsequent days.
Recent research suggests that, relative to methadone, buprenorphine treatment may result in less opioid use and fewer craving symptoms. Yet, the small number of studies conducted prevent formal conclusions and the extent to which reduced craving impacts the relationship between medication treatment type and illicit opioid use has yet to be determined. Understanding the factors that influence medication treatment progress and outcomes is important because it can ultimately reveal risk factors that can help guide individualized treatment approaches and enhance positive treatment outcomes.
To better understand the role of craving in medication treatment, this study examined the effect of medication treatment (i.e. buprenorphine vs. methadone) on illicit opioid use and craving, the relationship between craving and opioid use, and the extent to which craving explained the relationship between medication type and opioid use.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of a multi-site randomized controlled trial (i.e. OPTIMA trial) that examined the relationship between medication treatment (i.e. buprenorphine vs. methadone), illicit opioid use, and opioid craving among 270 adults with “prescription-type” opioid use disorder, which includes prescription opioids and synthetic opioids like fentanyl. Though details are not provided regarding the specific opioid use disorder diagnosis of the participants, one-third used fentanyl at some point during the study including baseline. While two-thirds had a lifetime history of heroin use, those for whom heroin was the most commonly used opioid in the last 30 days were excluded.
More specifically, this study assessed:
(1) The effect of medication treatment type (buprenorphine vs. methadone) on past-week opioid use and past-24-hour opioid craving, averaged across the 24-week trial.
(2) The relationship between average craving and average opioid use over the 24-week trial.
(3) The degree to which craving explains the relationship between medication type and opioid use, including the direct effect (effect of medication treatment on opioid use taking into account craving), indirect effect (effect of medication treatment on opioid use that operates through craving), and total effect (indirect + direct effect) of medication treatment on opioid use.
Participants were randomized to receive 24 weeks of flexible take-home buprenorphine (n=137) or supervised methadone (n=133) treatment at 1 of 7 participating research sites across Canada. Take-home doses were provided by study physicians at their discretion. Take-home doses were also available for methadone but, if provided, they were prescribed later in the course of treatment than buprenorphine take-home doses, given their different safety profiles (e.g., time to stabilization, overdose risk) during the early stages of treatment. Study prescribers were advised to offer buprenorphine patients 1 week’s worth of take-home doses after two weeks of treatment, and 2 weeks’ worth of take-home doses after 4 weeks of treatment. For methadone, prescribers were advised to offer patients take-home doses of methadone after 2-3 months of treatment, but only if they presented as clinically stable. Participants were not excluded from the study if they discontinued their medication treatment or switched from one medication type to another (n=30 individuals receiving buprenorphine & n=17 receiving methadone switch to a different medication type). However, only 28% of those randomized to either methadone or buprenorphine were receiving any opioid agonist medication by the end of the 24-week study period – meaning 72% were not taking buprenorphine or methadone 6 months later. In the study analyses, buprenorphine and methadone groups were determined using the participant’s originally assigned medication treatment at the start of the study.
Opioid craving over the past 24 hours was measured with the Brief Substance Craving Scale at baseline (i.e. before starting treatment) and weeks 2, 6, 10, 14, 18 and 22 after treatment initiation, with possible scores ranging from 0 (no craving) to 64 (extreme craving). Past-week opioid use was measured with the Timeline Followback at baseline (past 30-days opioid use) and every 2 weeks (opioid use since the last study visit) until the end of the study. In their analyses, the researchers examined the number of days that participants used opioids in the week following craving-scale administration. If opioid-use data in the week following a given craving assessment was missing, opioid use reported for the week prior to baseline was used, with the assumption that the participant had returned to their former opioid use patterns at the time of the missed assessment. Of note, study attrition was relatively high, with only about 39% of those assigned to buprenorphine and 47% of those assigned to methadone providing data on craving and substance use at the 22-week follow up. All analyses controlled for trial site, lifetime history of heroin use, study visit, opioid positive drug tests at last visit, sex, age, fentanyl use at baseline, and anxiety and depressive symptoms at baseline.
The majority of participants were White (67%) men (66%) in their late thirties, who had a moderate or severe prescription-type opioid use disorder (e.g., fentanyl). About 45% of the sample had unstable housing and psychiatric comorbidities, and 69% had a lifetime history of heroin use.
WHAT DID THIS STUDY FIND?
Assignment to buprenorphine associated with marginally less opioid use and craving
Relative to individuals who were assigned to methadone treatment, those assigned to buprenorphine had an average of 0.6 fewer days of weekly opioid use and 1 point lower on the craving scale, during the 24-week follow-up. In both treatment groups, greater opioid craving was associated with a greater number of days using opioids in the following week.
Craving accounted for one-quarter of the effect of treatment on opioid use
Taken together, craving accounted for about 24% (i.e. indirect effect divided by total effect) of the effect of medication treatment type on opioid use, and the magnitude of this mediating effect was consistent across the 2 medication treatments (24.1% for buprenorphine and 23.1% for methadone).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study, opioid craving partially mediated the effect of medication treatment type on next-week opioid use, accounting for about one-quarter of the effect observed. This means that differences in opioid use between the methadone and buprenorphine groups were partially explained by differences in craving (i.e. lower craving partially accounted for less frequent opioid use in the buprenorphine group). Given that about 75% of the effect of treatment type on opioid use was not explained by craving, additional factors are likely to explain this effect. For example, severity of withdrawal symptoms and mental health comorbidities often improve during buprenorphine and methadone treatment, and these factors may variably influence the relationship between medication treatment and opioid use depending on the medication type. Use of adjunct services like psychotherapy (e.g., people often learn additional alternative skills to manage cravings without resorting to opioid use) and mutual-help organizations (e.g., Narcotics Anonymous) as well as patient characteristics like impulsivity may also influence the relationship between medication treatment, craving, and opioid use. Still, reduced craving is very likely an important factor to consider with regard to successful treatment progress and outcomes, like reductions in illicit opioid use.
It is also worth noting that craving levels in this study sample were relatively low in both treatment groups, warranting additional study in populations experiencing a greater degree of opioid craving during treatment. Moreover, participant retention in the study and retention in treatment can impact statistical analyses and results. In this study, craving and opioid use measures gathered after baseline were only available for 39% – 61% of participants across study visits, less than one-third of participants continued with their assigned medication treatment throughout the study, and only 30% were taking an opioid agonist medication of any kind by the end of the 6-month trial. Thus, this study may reflect findings from individuals who have more follow up data and may therefore represent individuals who are more likely to benefit from treatment. Medication dose is also an important factor to consider, which this study did not control for. Thus, additional longitudinal research is required to make formal conclusions about the relationship between medication treatment, craving, and opioid use. Nonetheless, research on this topic is limited and mixed findings exist, demanding additional research with consideration of medication type, dose, and other factors relevant to craving, opioid use, and treatment effectiveness (e.g., primary opioid of choice, patient demographics, use of additional therapies/services, comorbidities).
This study’s findings are somewhat inconsistent with prior research showing that substance use outcomes are by and large comparable between individuals receiving buprenorphine and methadone treatment. This study suggested that, relative to methadone, buprenorphine may be associated with lower levels of craving and less frequent opioid use, although admittedly the difference observed here was small (0.6 fewer days of weekly opioid use and 1 point lower on the craving scale) and more people assigned to buprenorphine switched to another medication – but were included in the “buprenorphine group”.
Overall, the clinical implications in this study are unclear and require further investigation. In both treatment groups, higher levels of opioid craving were associated with more frequent opioid use in the following week. Similar findings have been observed in studies of buprenorphine or methadone treatment, where a relationship between opioid craving and use has been demonstrated among individuals with prescription opioid use disorder, individuals with a primary heroin use problem, and individuals with comorbid opioid and cocaine use disorders. Models that incorporate other variables such as the level of motivation to reduce or not use opioids and patients’ ability to deploy alternative coping skills to not use opioids when experiencing craving are also important to test. Additional research will help shed additional light on the complex dynamic relationship between craving and illicit opioid use during opioid use disorder medication treatment.
Individuals who did not continue with their assigned medication during the study were included in analyses and only a small number of participants were adherent to treatment over the entire 24-week trial, which may have influenced outcomes. It is also possible that individuals who engaged in ongoing illicit opioid use may have experienced lower levels of craving, which could have weakened the relationship between craving and subsequent opioid use.
Findings may not apply to individuals with a primary heroin problem or unstable comorbid psychiatric/physical conditions, as these were exclusionary in the current study.
This study was conducted in Canada and treatment conditions for buprenorphine and methadone generally followed Canadian treatment guidelines, which may differ from the prescribing and treatment guidelines of other countries. Additionally, prescribers from this study were allowed to use their clinical judgment to prescribe buprenorphine and methadone outside of the prescribing guidelines (e.g., changing the schedule of dose increases, changing the target dose, etc.), and it is unclear how this may have affected outcomes.
BOTTOM LINE
Craving accounted for about one-quarter of the effect of medication treatment type on opioid use. This study highlights the important role that craving plays in illicit opioid use during medication treatment, and also suggests that there are likely many other individual factors (e.g., impulsivity, mental health comorbidities, medication dose, and adherence) contributing to the effects of buprenorphine and methadone treatment on opioid use that were not assessed here. Additional research will help clarify the individual, treatment, and system-level factors that influence medication treatment progress and outcomes, which can ultimately help inform individualized treatment approaches that enhance positive recovery outcomes.
For individuals and families seeking recovery: Though additional research is needed to make formal conclusions about the relationship between medication treatments for opioid use disorder, craving, and opioid use, craving appears to be an important factor to consider when it comes to patient progress and outcomes. People who are undergoing medication treatment and experiencing ongoing opioid craving are encouraged to speak with their doctors about increasing medication doses or switching to a different medication to reduce opioid craving and, in turn, reduce risk of illicit opioid use.
For treatment professionals and treatment systems: Studies like this help us better understand the factors that influence opioid use disorder treatment outcomes, which can ultimately help guide individualized treatment approaches and inform patient risk factors that need addressing to promote successful treatment progress and outcomes. Given that craving accounted for ~25% of the effect of medication treatment on opioid use, assessing craving in healthcare settings is likely to be important for gauging a patient’s treatment progress and might help inform potential tweaks to treatment plans. Still, there are likely many other factors that influence patient outcomes that weren’t assessed here such as level of recovery motivation and patients’ levels of cognitive and behavioral coping skills to address craving in other ways beyond using opioids.
For scientists: Additional research examining the mediating effect of craving on the relationship between medication treatment and opioid use is needed among individuals who are adherent to treatment and in studies with higher follow-up rates. Evaluation of other potential mediators is needed, including withdrawal symptoms, mental-health comorbidities, impulsivity, medication dose/regimen, and use of adjunct treatments and recovery support services, among others. Assessment of medications other than sublingual buprenorphine and oral methadone will also help enhance our understanding of medication treatment and its relationship to patient outcomes.
For policy makers: Understanding how opioid use disorder medication treatments impact patient progress and outcomes can help inform individualized treatment approaches that enhance positive outcomes and sustained recovery to help address the ongoing opioid epidemic. Given mixed findings among a small number of studies examining the relationship between medication treatment, illicit opioid use, and factors that mediate this relationship, additional research funds will help clarify inconsistent findings, and will expand our understanding of the factors influencing treatment and how they can be leveraged to improve treatment efficacy.
Medication treatments for opioid use disorder like buprenorphine and methadone ease symptoms of opioid withdrawal and craving, and ultimately help to support reduced substance use and positive recovery outcomes. However, many individuals continue to use illicit opioids during medication treatment. Craving has been proposed as a possible factor contributing to ongoing opioid misuse during treatment, but research examining craving is limited and has yielded mixedfindings thus far, possibly due to the varying research methods used across different studies (e.g., different populations of interest, length of time between assessment of craving and opioid use). For example, one study observed no association between pre-treatment craving and subsequent opioid use during 12-weeks of buprenorphine treatment for prescription opioid use disorder. Another investigation found that craving predicted subsequent opioid use (2-week intervals) during a 3-month course of buprenorphine treatment for opioid use disorder. While another study conducted among individuals with heroin use problems found that craving was associated with heroin use in subsequent days.
Recent research suggests that, relative to methadone, buprenorphine treatment may result in less opioid use and fewer craving symptoms. Yet, the small number of studies conducted prevent formal conclusions and the extent to which reduced craving impacts the relationship between medication treatment type and illicit opioid use has yet to be determined. Understanding the factors that influence medication treatment progress and outcomes is important because it can ultimately reveal risk factors that can help guide individualized treatment approaches and enhance positive treatment outcomes.
To better understand the role of craving in medication treatment, this study examined the effect of medication treatment (i.e. buprenorphine vs. methadone) on illicit opioid use and craving, the relationship between craving and opioid use, and the extent to which craving explained the relationship between medication type and opioid use.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of a multi-site randomized controlled trial (i.e. OPTIMA trial) that examined the relationship between medication treatment (i.e. buprenorphine vs. methadone), illicit opioid use, and opioid craving among 270 adults with “prescription-type” opioid use disorder, which includes prescription opioids and synthetic opioids like fentanyl. Though details are not provided regarding the specific opioid use disorder diagnosis of the participants, one-third used fentanyl at some point during the study including baseline. While two-thirds had a lifetime history of heroin use, those for whom heroin was the most commonly used opioid in the last 30 days were excluded.
More specifically, this study assessed:
(1) The effect of medication treatment type (buprenorphine vs. methadone) on past-week opioid use and past-24-hour opioid craving, averaged across the 24-week trial.
(2) The relationship between average craving and average opioid use over the 24-week trial.
(3) The degree to which craving explains the relationship between medication type and opioid use, including the direct effect (effect of medication treatment on opioid use taking into account craving), indirect effect (effect of medication treatment on opioid use that operates through craving), and total effect (indirect + direct effect) of medication treatment on opioid use.
Participants were randomized to receive 24 weeks of flexible take-home buprenorphine (n=137) or supervised methadone (n=133) treatment at 1 of 7 participating research sites across Canada. Take-home doses were provided by study physicians at their discretion. Take-home doses were also available for methadone but, if provided, they were prescribed later in the course of treatment than buprenorphine take-home doses, given their different safety profiles (e.g., time to stabilization, overdose risk) during the early stages of treatment. Study prescribers were advised to offer buprenorphine patients 1 week’s worth of take-home doses after two weeks of treatment, and 2 weeks’ worth of take-home doses after 4 weeks of treatment. For methadone, prescribers were advised to offer patients take-home doses of methadone after 2-3 months of treatment, but only if they presented as clinically stable. Participants were not excluded from the study if they discontinued their medication treatment or switched from one medication type to another (n=30 individuals receiving buprenorphine & n=17 receiving methadone switch to a different medication type). However, only 28% of those randomized to either methadone or buprenorphine were receiving any opioid agonist medication by the end of the 24-week study period – meaning 72% were not taking buprenorphine or methadone 6 months later. In the study analyses, buprenorphine and methadone groups were determined using the participant’s originally assigned medication treatment at the start of the study.
Opioid craving over the past 24 hours was measured with the Brief Substance Craving Scale at baseline (i.e. before starting treatment) and weeks 2, 6, 10, 14, 18 and 22 after treatment initiation, with possible scores ranging from 0 (no craving) to 64 (extreme craving). Past-week opioid use was measured with the Timeline Followback at baseline (past 30-days opioid use) and every 2 weeks (opioid use since the last study visit) until the end of the study. In their analyses, the researchers examined the number of days that participants used opioids in the week following craving-scale administration. If opioid-use data in the week following a given craving assessment was missing, opioid use reported for the week prior to baseline was used, with the assumption that the participant had returned to their former opioid use patterns at the time of the missed assessment. Of note, study attrition was relatively high, with only about 39% of those assigned to buprenorphine and 47% of those assigned to methadone providing data on craving and substance use at the 22-week follow up. All analyses controlled for trial site, lifetime history of heroin use, study visit, opioid positive drug tests at last visit, sex, age, fentanyl use at baseline, and anxiety and depressive symptoms at baseline.
The majority of participants were White (67%) men (66%) in their late thirties, who had a moderate or severe prescription-type opioid use disorder (e.g., fentanyl). About 45% of the sample had unstable housing and psychiatric comorbidities, and 69% had a lifetime history of heroin use.
WHAT DID THIS STUDY FIND?
Assignment to buprenorphine associated with marginally less opioid use and craving
Relative to individuals who were assigned to methadone treatment, those assigned to buprenorphine had an average of 0.6 fewer days of weekly opioid use and 1 point lower on the craving scale, during the 24-week follow-up. In both treatment groups, greater opioid craving was associated with a greater number of days using opioids in the following week.
Craving accounted for one-quarter of the effect of treatment on opioid use
Taken together, craving accounted for about 24% (i.e. indirect effect divided by total effect) of the effect of medication treatment type on opioid use, and the magnitude of this mediating effect was consistent across the 2 medication treatments (24.1% for buprenorphine and 23.1% for methadone).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study, opioid craving partially mediated the effect of medication treatment type on next-week opioid use, accounting for about one-quarter of the effect observed. This means that differences in opioid use between the methadone and buprenorphine groups were partially explained by differences in craving (i.e. lower craving partially accounted for less frequent opioid use in the buprenorphine group). Given that about 75% of the effect of treatment type on opioid use was not explained by craving, additional factors are likely to explain this effect. For example, severity of withdrawal symptoms and mental health comorbidities often improve during buprenorphine and methadone treatment, and these factors may variably influence the relationship between medication treatment and opioid use depending on the medication type. Use of adjunct services like psychotherapy (e.g., people often learn additional alternative skills to manage cravings without resorting to opioid use) and mutual-help organizations (e.g., Narcotics Anonymous) as well as patient characteristics like impulsivity may also influence the relationship between medication treatment, craving, and opioid use. Still, reduced craving is very likely an important factor to consider with regard to successful treatment progress and outcomes, like reductions in illicit opioid use.
It is also worth noting that craving levels in this study sample were relatively low in both treatment groups, warranting additional study in populations experiencing a greater degree of opioid craving during treatment. Moreover, participant retention in the study and retention in treatment can impact statistical analyses and results. In this study, craving and opioid use measures gathered after baseline were only available for 39% – 61% of participants across study visits, less than one-third of participants continued with their assigned medication treatment throughout the study, and only 30% were taking an opioid agonist medication of any kind by the end of the 6-month trial. Thus, this study may reflect findings from individuals who have more follow up data and may therefore represent individuals who are more likely to benefit from treatment. Medication dose is also an important factor to consider, which this study did not control for. Thus, additional longitudinal research is required to make formal conclusions about the relationship between medication treatment, craving, and opioid use. Nonetheless, research on this topic is limited and mixed findings exist, demanding additional research with consideration of medication type, dose, and other factors relevant to craving, opioid use, and treatment effectiveness (e.g., primary opioid of choice, patient demographics, use of additional therapies/services, comorbidities).
This study’s findings are somewhat inconsistent with prior research showing that substance use outcomes are by and large comparable between individuals receiving buprenorphine and methadone treatment. This study suggested that, relative to methadone, buprenorphine may be associated with lower levels of craving and less frequent opioid use, although admittedly the difference observed here was small (0.6 fewer days of weekly opioid use and 1 point lower on the craving scale) and more people assigned to buprenorphine switched to another medication – but were included in the “buprenorphine group”.
Overall, the clinical implications in this study are unclear and require further investigation. In both treatment groups, higher levels of opioid craving were associated with more frequent opioid use in the following week. Similar findings have been observed in studies of buprenorphine or methadone treatment, where a relationship between opioid craving and use has been demonstrated among individuals with prescription opioid use disorder, individuals with a primary heroin use problem, and individuals with comorbid opioid and cocaine use disorders. Models that incorporate other variables such as the level of motivation to reduce or not use opioids and patients’ ability to deploy alternative coping skills to not use opioids when experiencing craving are also important to test. Additional research will help shed additional light on the complex dynamic relationship between craving and illicit opioid use during opioid use disorder medication treatment.
Individuals who did not continue with their assigned medication during the study were included in analyses and only a small number of participants were adherent to treatment over the entire 24-week trial, which may have influenced outcomes. It is also possible that individuals who engaged in ongoing illicit opioid use may have experienced lower levels of craving, which could have weakened the relationship between craving and subsequent opioid use.
Findings may not apply to individuals with a primary heroin problem or unstable comorbid psychiatric/physical conditions, as these were exclusionary in the current study.
This study was conducted in Canada and treatment conditions for buprenorphine and methadone generally followed Canadian treatment guidelines, which may differ from the prescribing and treatment guidelines of other countries. Additionally, prescribers from this study were allowed to use their clinical judgment to prescribe buprenorphine and methadone outside of the prescribing guidelines (e.g., changing the schedule of dose increases, changing the target dose, etc.), and it is unclear how this may have affected outcomes.
BOTTOM LINE
Craving accounted for about one-quarter of the effect of medication treatment type on opioid use. This study highlights the important role that craving plays in illicit opioid use during medication treatment, and also suggests that there are likely many other individual factors (e.g., impulsivity, mental health comorbidities, medication dose, and adherence) contributing to the effects of buprenorphine and methadone treatment on opioid use that were not assessed here. Additional research will help clarify the individual, treatment, and system-level factors that influence medication treatment progress and outcomes, which can ultimately help inform individualized treatment approaches that enhance positive recovery outcomes.
For individuals and families seeking recovery: Though additional research is needed to make formal conclusions about the relationship between medication treatments for opioid use disorder, craving, and opioid use, craving appears to be an important factor to consider when it comes to patient progress and outcomes. People who are undergoing medication treatment and experiencing ongoing opioid craving are encouraged to speak with their doctors about increasing medication doses or switching to a different medication to reduce opioid craving and, in turn, reduce risk of illicit opioid use.
For treatment professionals and treatment systems: Studies like this help us better understand the factors that influence opioid use disorder treatment outcomes, which can ultimately help guide individualized treatment approaches and inform patient risk factors that need addressing to promote successful treatment progress and outcomes. Given that craving accounted for ~25% of the effect of medication treatment on opioid use, assessing craving in healthcare settings is likely to be important for gauging a patient’s treatment progress and might help inform potential tweaks to treatment plans. Still, there are likely many other factors that influence patient outcomes that weren’t assessed here such as level of recovery motivation and patients’ levels of cognitive and behavioral coping skills to address craving in other ways beyond using opioids.
For scientists: Additional research examining the mediating effect of craving on the relationship between medication treatment and opioid use is needed among individuals who are adherent to treatment and in studies with higher follow-up rates. Evaluation of other potential mediators is needed, including withdrawal symptoms, mental-health comorbidities, impulsivity, medication dose/regimen, and use of adjunct treatments and recovery support services, among others. Assessment of medications other than sublingual buprenorphine and oral methadone will also help enhance our understanding of medication treatment and its relationship to patient outcomes.
For policy makers: Understanding how opioid use disorder medication treatments impact patient progress and outcomes can help inform individualized treatment approaches that enhance positive outcomes and sustained recovery to help address the ongoing opioid epidemic. Given mixed findings among a small number of studies examining the relationship between medication treatment, illicit opioid use, and factors that mediate this relationship, additional research funds will help clarify inconsistent findings, and will expand our understanding of the factors influencing treatment and how they can be leveraged to improve treatment efficacy.