Exploring equity in AA: How does sexual minority status impact attendance?
Sexual minorities, including lesbian, gay, and bisexual identified individuals, experience alcohol use disorder at much higher rates than those identifying as heterosexual. Alcoholics Anonymous (AA) serves as the most common source of recovery support for alcohol-related problems in the United States. This study examining the rates of predictors of sexual minority involvement in AA has important implications for best practices and public health recommendations for these high-risk individuals.
This was a secondary analysis of data from the National Alcohol Survey that sought to establish and compare rates of lifetime AA attendance across sexual orientations, and compare relationships between AA attendance and individual factors (e.g., alcohol use disorder severity, demographic factors). The study sample included 7,862 adults that endorsed at least one lifetime symptom of DSM-5 alcohol use disorder.
The National Alcohol Survey is a nationally representative survey of adults ages 18 and older conducted every 5 years by the Alcohol Research Group, which is funded by the National Institute on Alcohol Abuse and Alcoholism (NIAAA). To ensure enough data from sexual minority individuals were available for the analyses, this study pooled data from five independent waves of the survey (1995–2015).
Respondents who endorsed ever having spoken to someone about a drinking problem were asked about their lifetime AA attendance with the question: “Have you ever gone to an Alcoholics Anonymous meeting for your drinking?” AA attendance was analyzed as a binary variable (yes/no). The authors also measured lifetime alcohol use disorder severity with a 17-item measure developed by the Alcohol Research Group, and whether individuals identified as religious or not (yes or no).
Questions asked all survey participants to indicate their sexual preference/orientation (“Which of the following statements best describes your sexual preference?” (1995 and 2000); “Which of the following statements best describes your sexual orientation?” (2005, 2010, and 2015)).
Overall, 39.74% of heterosexual male, 40.58% of bisexual male, 45.61% of gay male, 19.52% of heterosexual female, 46.53% of bisexual female, and 48.60% of lesbian female respondents to the National Alcohol Survey reported at least one symptom of alcohol use disorder and were included in this study. After screening out participants with zero symptoms of alcohol use disorder, the combined surveys yielded 4,576 heterosexual male, 2,919 heterosexual female, 56 bisexual male, 94 bisexual female, 130 gay male, and 87 lesbian female respondents.
WHAT DID THIS STUDY FIND?
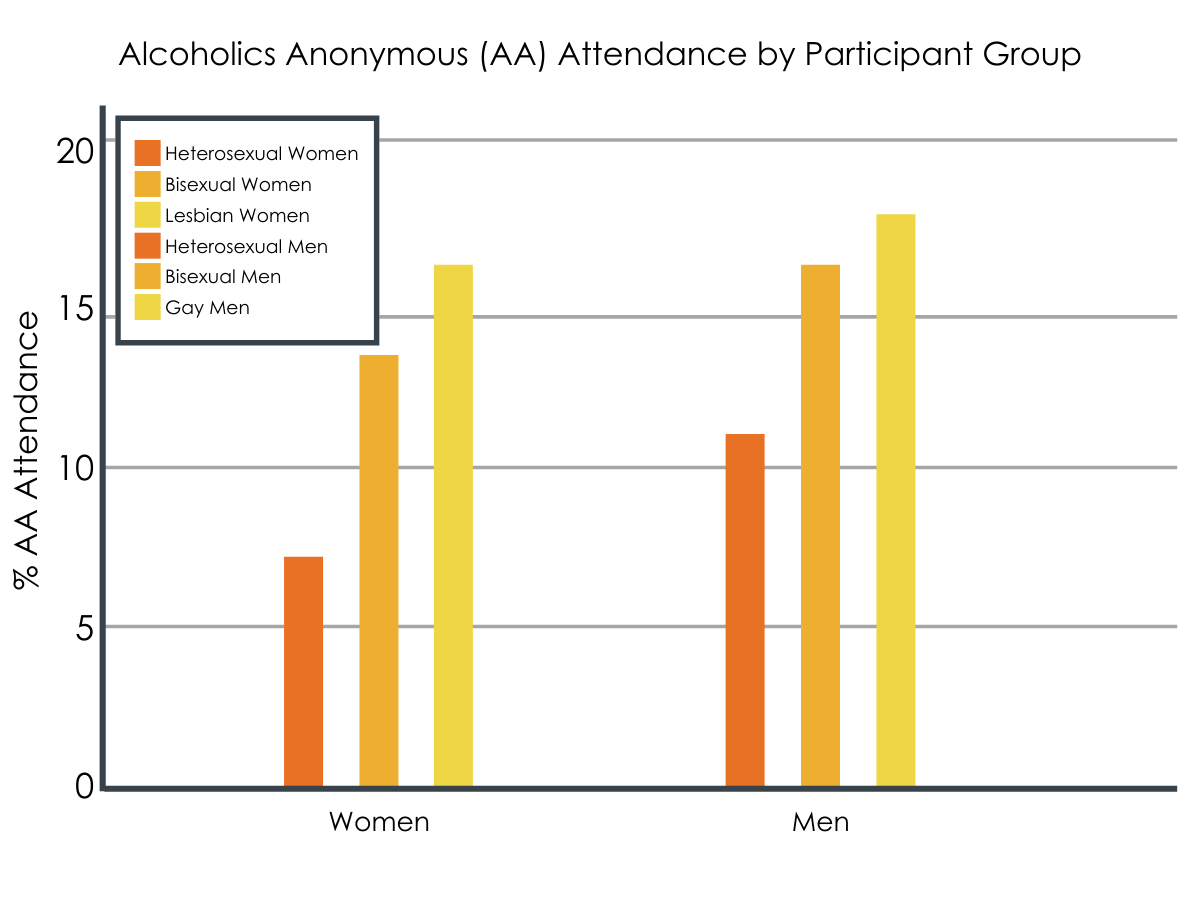
Both gay/lesbian and bisexual respondents had greater odds of ever attending AA compared to heterosexual respondents, but attendance was also influenced by other individual characteristics like sex and race.
Overall, both gay/lesbian and bisexual respondents had greater odds of ever attending AA compared to heterosexual respondents, after controlling for individual factors like lifetime alcohol use disorder severity, gender, race/ethnicity, age, religiosity, and current income. Other predictors of higher odds of AA attendance included greater alcohol use disorder severity, older age, and lower income. Female gender and Black and Latino/Latina/Latinx race/ethnicity were uniquely associated with lower odds of attending AA relative to male and White respondents, respectively. The model showed no association between religiosity and AA attendance.
AA attendance by participant group. After controlling for individual factors like alcohol use disorder severity, the apparent above differences between groups for men were not statistically significant, meaning it cannot be determined if the change between male groups was attributable to group differences, or just random chance.
When analyzed separately, women and men had differing patterns of relationships between individual characteristics and AA attendance.
To determine if these observed associations held for both men and women, the researchers repeated this analysis for men and women separately. They also explored whether the associations each of alcohol use disorder severity, race/ethnicity, age, religiosity, and current income with AA attendance were conditional on sexual minority status – that is, whether these relationships were stronger or weaker among sexual minorities relative to heterosexual identified individuals (i.e., the conducted statistical interaction tests).
For women, the results closely mirrored the findings in the overall sample. Both lesbian and bisexual women respondents showed greater odds of attending AA than their heterosexual counterparts after controlling for lifetime alcohol use disorder severity and demographic characteristics. Among women, other predictors of higher odds of AA attendance included greater alcohol use disorder severity, older age, and lower income. Black and Latina race/ethnicity was associated with lower odds of attending AA relative to White respondents. The models showed no association between religiosity and AA attendance among female respondents.
In the female specific analysis, interaction effects were also observed. Among sexual minority women, there was a stronger association between older age and AA attendance, a stronger association between greater religiosity and AA attendance, and a weaker association between lifetime alcohol use disorder severity and AA attendance, compared to heterosexual women. For example, identifying with a religion was associated with AA attendance for sexual minority, but not heterosexual, women.
For men, the models showed fewer associations between measured characteristics and AA attendance. As with the overall model including both men and women, greater alcohol use disorder severity and older age predicted higher odds of AA attendance, and the models showed no association between religiosity and AA attendance. Unlike the aggregated analysis, however, sexual orientation, race/ethnicity, and income were not associated with AA attendance for men. The models showed no statistically significant interactions between sexual orientation and these other factors.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study, the authors compared sexual minority and heterosexual individuals on AA attendance and explored associated factors. In the first model including all participants (i.e., both women and men), the study authors found that gay/lesbian and bisexual individuals were more likely to have attended AA than their heterosexual counterparts. This may be in part because sexual minority identifying individuals, on average, tend to have more psychosocial challenges and more severe substance use histories compared to their heterosexual peers.
In their subsequent analysis where women and men were considered separately, they found that lesbian and bisexual women were more than twice as likely as heterosexual women to have ever attended AA meetings. However, gay and bisexual men had similar rates of AA attendance to their heterosexual counterparts. This suggests that observed differences in AA attendance between sexual minority and sexual majority individuals in the initial statistical model were being driven by the women in the sample and highlights the importance of considering gender in such research (i.e., rather than assuming gay men and lesbian women are the same).
As the research team noted, one possible explanation for the finding that sexual minority women are more likely than heterosexual women to attend AA is a possible greater need for social support for alcohol-related problems. In support of this idea, past research has shown that on average, sexual minority women have less social support and greater social support need than their heterosexual counterparts. Furthermore, for many people, and particularly for women, AA is an important source of social support. Given these previous findings, it would make sense that sexual minority women may be more inclined to utilize the social support offered by attending AA.
Findings for men were more mixed, with the authors’ results suggesting that sexual minority men are similar to heterosexual men in terms of ever attending AA. The study authors suggest that alcohol use disorder severity may have been influencing results for men because gay men showed higher alcohol use disorder (AUD) severity than their heterosexual counterparts. At the same time, it is possible gay and heterosexual men are simply not different in terms of attending AA. In other words, while sexual minorities have higher alcohol use disorder severity overall, and individuals with more severe alcohol use disorder tend have higher rates of AA attendance, severity accounts for sexual minority men’s greater attendance. In women, however, there may be something unique about sexual minority status driving this greater AA attendance.
It will be important for future studies to explore alcohol use disorder severity when exploring AA attendance among sexual minority males. The study also highlights the importance of modeling so-called ‘intersectionality’—relationships among multiple categories of social identification such as gender, race/ethnicity, and sexual identification—in research on alcohol use disorder treatment and recovery support services.
As noted by the researchers:
The study’s measure of AA attendance indicated only whether respondents had ever attended an AA meeting. It can’t be known from these results whether sexual monitory individuals differed from heterosexual individuals in continued AA attendance or degree of AA involvement.
This study utilized a binary gender classification system, which precludes the analysis of gender non-binary individuals. Also, the study did not account for transgender identification.
The study’s sexual orientation measure may potentially limit this study’s generalizability. Though this study considered bisexual respondents separately from monosexual participants (i.e., gay and lesbian), this sexuality classification scheme does not include the entire spectrum of sexual orientations.
The cross-sectional design (i.e., a survey conducted in a single point in time) and lengthy period of data collection limits this study. It may be difficult for participants to recall past AUD severity.
AA attendance may influence retrospective reporting of past AUD severity, perhaps by leading participants to reflect on past alcohol-related distress and impairment and report greater problem severity.
Additionally:
Though this study had a large sample size (N= 7,862), only 367 participants identified as sexual minority individuals. Imbalanced samples like this can lead to problems in statistical models such as over- or under-estimating effects and reduce confidence in findings.
BOTTOM LINE
In this study comparing lifetime AA attendance and factors associated with attendance, in sexual minority versus heterosexual identified individuals with at least one alcohol use disorder symptom, sexual minority women were more likely to endorse ever attending an AA meeting relative to heterosexual women, while sexual minority men endorsed a similar rate of ever attending an AA meeting relative to heterosexual men. Additionally, among sexual minority women, relative to heterosexual women, older as well as more religious women were more likely to have attended AA; also, relative to heterosexual women, the relation between alcohol use disorder symptom severity and lifetime AA attendance was weaker. Though the study’s findings cannot speak to potential benefits associated with AA attendance for sexual minority individuals, these findings signal that sexual minority women, especially those who are older and more religious have a greater propensity to attend AA compared to their heterosexual counterparts.
For individuals and families seeking recovery: Sexual minority women were more likely to endorse ever attending an AA meeting relative to heterosexual women, while sexual minority men endorsed a similar rate of ever attending an AA meeting relative to heterosexual men. Though more work is needed to better understand how sexual minority individuals may or may not benefit from AA relative to heterosexual individuals, AA is an effective approach for addressing alcohol use disorder when used alone or in combination with formal treatment.
For treatment professionals and treatment systems: Sexual minority women were more likely to endorse ever attending an AA meeting relative to heterosexual women, while sexual minority men endorsed a similar rate of ever attending an AA meeting relative to heterosexual men. Helping sexual minority women patients connect with social supports may be particularly important. Though more work is needed to better understand how sexual minority individuals may or may not benefit from AA relative to heterosexual individuals, AA is an effective approach for addressing alcohol use disorder when used alone or in combination with formal treatment. For those whom AA does not feel like a good fit, non-traditional mutual-help programs that might also facilitate social support, like SMART Recovery, LifeRing, and Women for Sobriety as well as exercise-based recovery support services like The Phoenix, may be helpful.
For scientists:Sexual minority women were more likely to endorse ever attending an AA meeting relative to heterosexual women, while sexual minority men endorsed a similar rate of ever attending an AA meeting relative to heterosexual men. More work is needed to better understand how sexual minority individuals may or may not benefit from AA relative to heterosexual individuals. In such research it will be important to consider the role of alcohol use disorder severity.
For policy makers: Sexual minority women were more likely to endorse ever attending an AA meeting relative to heterosexual women, while sexual minority men endorsed a similar rate of ever attending an AA meeting relative to heterosexual men. Findings from this study, as well as prior research, suggest sexual minority women have additional need for social support. Greater social support infrastructure is needed, particularly for sexual minority women. Such infrastructure can be created through supporting recovery community centers and non-traditional mutual-help programs like SMART Recovery, LifeRing, and Women for Sobriety as well as exercise-based recovery support services like The Phoenix.
This was a secondary analysis of data from the National Alcohol Survey that sought to establish and compare rates of lifetime AA attendance across sexual orientations, and compare relationships between AA attendance and individual factors (e.g., alcohol use disorder severity, demographic factors). The study sample included 7,862 adults that endorsed at least one lifetime symptom of DSM-5 alcohol use disorder.
The National Alcohol Survey is a nationally representative survey of adults ages 18 and older conducted every 5 years by the Alcohol Research Group, which is funded by the National Institute on Alcohol Abuse and Alcoholism (NIAAA). To ensure enough data from sexual minority individuals were available for the analyses, this study pooled data from five independent waves of the survey (1995–2015).
Respondents who endorsed ever having spoken to someone about a drinking problem were asked about their lifetime AA attendance with the question: “Have you ever gone to an Alcoholics Anonymous meeting for your drinking?” AA attendance was analyzed as a binary variable (yes/no). The authors also measured lifetime alcohol use disorder severity with a 17-item measure developed by the Alcohol Research Group, and whether individuals identified as religious or not (yes or no).
Questions asked all survey participants to indicate their sexual preference/orientation (“Which of the following statements best describes your sexual preference?” (1995 and 2000); “Which of the following statements best describes your sexual orientation?” (2005, 2010, and 2015)).
Overall, 39.74% of heterosexual male, 40.58% of bisexual male, 45.61% of gay male, 19.52% of heterosexual female, 46.53% of bisexual female, and 48.60% of lesbian female respondents to the National Alcohol Survey reported at least one symptom of alcohol use disorder and were included in this study. After screening out participants with zero symptoms of alcohol use disorder, the combined surveys yielded 4,576 heterosexual male, 2,919 heterosexual female, 56 bisexual male, 94 bisexual female, 130 gay male, and 87 lesbian female respondents.
WHAT DID THIS STUDY FIND?
Both gay/lesbian and bisexual respondents had greater odds of ever attending AA compared to heterosexual respondents, but attendance was also influenced by other individual characteristics like sex and race.
Overall, both gay/lesbian and bisexual respondents had greater odds of ever attending AA compared to heterosexual respondents, after controlling for individual factors like lifetime alcohol use disorder severity, gender, race/ethnicity, age, religiosity, and current income. Other predictors of higher odds of AA attendance included greater alcohol use disorder severity, older age, and lower income. Female gender and Black and Latino/Latina/Latinx race/ethnicity were uniquely associated with lower odds of attending AA relative to male and White respondents, respectively. The model showed no association between religiosity and AA attendance.
AA attendance by participant group. After controlling for individual factors like alcohol use disorder severity, the apparent above differences between groups for men were not statistically significant, meaning it cannot be determined if the change between male groups was attributable to group differences, or just random chance.
When analyzed separately, women and men had differing patterns of relationships between individual characteristics and AA attendance.
To determine if these observed associations held for both men and women, the researchers repeated this analysis for men and women separately. They also explored whether the associations each of alcohol use disorder severity, race/ethnicity, age, religiosity, and current income with AA attendance were conditional on sexual minority status – that is, whether these relationships were stronger or weaker among sexual minorities relative to heterosexual identified individuals (i.e., the conducted statistical interaction tests).
For women, the results closely mirrored the findings in the overall sample. Both lesbian and bisexual women respondents showed greater odds of attending AA than their heterosexual counterparts after controlling for lifetime alcohol use disorder severity and demographic characteristics. Among women, other predictors of higher odds of AA attendance included greater alcohol use disorder severity, older age, and lower income. Black and Latina race/ethnicity was associated with lower odds of attending AA relative to White respondents. The models showed no association between religiosity and AA attendance among female respondents.
In the female specific analysis, interaction effects were also observed. Among sexual minority women, there was a stronger association between older age and AA attendance, a stronger association between greater religiosity and AA attendance, and a weaker association between lifetime alcohol use disorder severity and AA attendance, compared to heterosexual women. For example, identifying with a religion was associated with AA attendance for sexual minority, but not heterosexual, women.
For men, the models showed fewer associations between measured characteristics and AA attendance. As with the overall model including both men and women, greater alcohol use disorder severity and older age predicted higher odds of AA attendance, and the models showed no association between religiosity and AA attendance. Unlike the aggregated analysis, however, sexual orientation, race/ethnicity, and income were not associated with AA attendance for men. The models showed no statistically significant interactions between sexual orientation and these other factors.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study, the authors compared sexual minority and heterosexual individuals on AA attendance and explored associated factors. In the first model including all participants (i.e., both women and men), the study authors found that gay/lesbian and bisexual individuals were more likely to have attended AA than their heterosexual counterparts. This may be in part because sexual minority identifying individuals, on average, tend to have more psychosocial challenges and more severe substance use histories compared to their heterosexual peers.
In their subsequent analysis where women and men were considered separately, they found that lesbian and bisexual women were more than twice as likely as heterosexual women to have ever attended AA meetings. However, gay and bisexual men had similar rates of AA attendance to their heterosexual counterparts. This suggests that observed differences in AA attendance between sexual minority and sexual majority individuals in the initial statistical model were being driven by the women in the sample and highlights the importance of considering gender in such research (i.e., rather than assuming gay men and lesbian women are the same).
As the research team noted, one possible explanation for the finding that sexual minority women are more likely than heterosexual women to attend AA is a possible greater need for social support for alcohol-related problems. In support of this idea, past research has shown that on average, sexual minority women have less social support and greater social support need than their heterosexual counterparts. Furthermore, for many people, and particularly for women, AA is an important source of social support. Given these previous findings, it would make sense that sexual minority women may be more inclined to utilize the social support offered by attending AA.
Findings for men were more mixed, with the authors’ results suggesting that sexual minority men are similar to heterosexual men in terms of ever attending AA. The study authors suggest that alcohol use disorder severity may have been influencing results for men because gay men showed higher alcohol use disorder (AUD) severity than their heterosexual counterparts. At the same time, it is possible gay and heterosexual men are simply not different in terms of attending AA. In other words, while sexual minorities have higher alcohol use disorder severity overall, and individuals with more severe alcohol use disorder tend have higher rates of AA attendance, severity accounts for sexual minority men’s greater attendance. In women, however, there may be something unique about sexual minority status driving this greater AA attendance.
It will be important for future studies to explore alcohol use disorder severity when exploring AA attendance among sexual minority males. The study also highlights the importance of modeling so-called ‘intersectionality’—relationships among multiple categories of social identification such as gender, race/ethnicity, and sexual identification—in research on alcohol use disorder treatment and recovery support services.
As noted by the researchers:
The study’s measure of AA attendance indicated only whether respondents had ever attended an AA meeting. It can’t be known from these results whether sexual monitory individuals differed from heterosexual individuals in continued AA attendance or degree of AA involvement.
This study utilized a binary gender classification system, which precludes the analysis of gender non-binary individuals. Also, the study did not account for transgender identification.
The study’s sexual orientation measure may potentially limit this study’s generalizability. Though this study considered bisexual respondents separately from monosexual participants (i.e., gay and lesbian), this sexuality classification scheme does not include the entire spectrum of sexual orientations.
The cross-sectional design (i.e., a survey conducted in a single point in time) and lengthy period of data collection limits this study. It may be difficult for participants to recall past AUD severity.
AA attendance may influence retrospective reporting of past AUD severity, perhaps by leading participants to reflect on past alcohol-related distress and impairment and report greater problem severity.
Additionally:
Though this study had a large sample size (N= 7,862), only 367 participants identified as sexual minority individuals. Imbalanced samples like this can lead to problems in statistical models such as over- or under-estimating effects and reduce confidence in findings.
BOTTOM LINE
In this study comparing lifetime AA attendance and factors associated with attendance, in sexual minority versus heterosexual identified individuals with at least one alcohol use disorder symptom, sexual minority women were more likely to endorse ever attending an AA meeting relative to heterosexual women, while sexual minority men endorsed a similar rate of ever attending an AA meeting relative to heterosexual men. Additionally, among sexual minority women, relative to heterosexual women, older as well as more religious women were more likely to have attended AA; also, relative to heterosexual women, the relation between alcohol use disorder symptom severity and lifetime AA attendance was weaker. Though the study’s findings cannot speak to potential benefits associated with AA attendance for sexual minority individuals, these findings signal that sexual minority women, especially those who are older and more religious have a greater propensity to attend AA compared to their heterosexual counterparts.
For individuals and families seeking recovery: Sexual minority women were more likely to endorse ever attending an AA meeting relative to heterosexual women, while sexual minority men endorsed a similar rate of ever attending an AA meeting relative to heterosexual men. Though more work is needed to better understand how sexual minority individuals may or may not benefit from AA relative to heterosexual individuals, AA is an effective approach for addressing alcohol use disorder when used alone or in combination with formal treatment.
For treatment professionals and treatment systems: Sexual minority women were more likely to endorse ever attending an AA meeting relative to heterosexual women, while sexual minority men endorsed a similar rate of ever attending an AA meeting relative to heterosexual men. Helping sexual minority women patients connect with social supports may be particularly important. Though more work is needed to better understand how sexual minority individuals may or may not benefit from AA relative to heterosexual individuals, AA is an effective approach for addressing alcohol use disorder when used alone or in combination with formal treatment. For those whom AA does not feel like a good fit, non-traditional mutual-help programs that might also facilitate social support, like SMART Recovery, LifeRing, and Women for Sobriety as well as exercise-based recovery support services like The Phoenix, may be helpful.
For scientists:Sexual minority women were more likely to endorse ever attending an AA meeting relative to heterosexual women, while sexual minority men endorsed a similar rate of ever attending an AA meeting relative to heterosexual men. More work is needed to better understand how sexual minority individuals may or may not benefit from AA relative to heterosexual individuals. In such research it will be important to consider the role of alcohol use disorder severity.
For policy makers: Sexual minority women were more likely to endorse ever attending an AA meeting relative to heterosexual women, while sexual minority men endorsed a similar rate of ever attending an AA meeting relative to heterosexual men. Findings from this study, as well as prior research, suggest sexual minority women have additional need for social support. Greater social support infrastructure is needed, particularly for sexual minority women. Such infrastructure can be created through supporting recovery community centers and non-traditional mutual-help programs like SMART Recovery, LifeRing, and Women for Sobriety as well as exercise-based recovery support services like The Phoenix.
This was a secondary analysis of data from the National Alcohol Survey that sought to establish and compare rates of lifetime AA attendance across sexual orientations, and compare relationships between AA attendance and individual factors (e.g., alcohol use disorder severity, demographic factors). The study sample included 7,862 adults that endorsed at least one lifetime symptom of DSM-5 alcohol use disorder.
The National Alcohol Survey is a nationally representative survey of adults ages 18 and older conducted every 5 years by the Alcohol Research Group, which is funded by the National Institute on Alcohol Abuse and Alcoholism (NIAAA). To ensure enough data from sexual minority individuals were available for the analyses, this study pooled data from five independent waves of the survey (1995–2015).
Respondents who endorsed ever having spoken to someone about a drinking problem were asked about their lifetime AA attendance with the question: “Have you ever gone to an Alcoholics Anonymous meeting for your drinking?” AA attendance was analyzed as a binary variable (yes/no). The authors also measured lifetime alcohol use disorder severity with a 17-item measure developed by the Alcohol Research Group, and whether individuals identified as religious or not (yes or no).
Questions asked all survey participants to indicate their sexual preference/orientation (“Which of the following statements best describes your sexual preference?” (1995 and 2000); “Which of the following statements best describes your sexual orientation?” (2005, 2010, and 2015)).
Overall, 39.74% of heterosexual male, 40.58% of bisexual male, 45.61% of gay male, 19.52% of heterosexual female, 46.53% of bisexual female, and 48.60% of lesbian female respondents to the National Alcohol Survey reported at least one symptom of alcohol use disorder and were included in this study. After screening out participants with zero symptoms of alcohol use disorder, the combined surveys yielded 4,576 heterosexual male, 2,919 heterosexual female, 56 bisexual male, 94 bisexual female, 130 gay male, and 87 lesbian female respondents.
WHAT DID THIS STUDY FIND?
Both gay/lesbian and bisexual respondents had greater odds of ever attending AA compared to heterosexual respondents, but attendance was also influenced by other individual characteristics like sex and race.
Overall, both gay/lesbian and bisexual respondents had greater odds of ever attending AA compared to heterosexual respondents, after controlling for individual factors like lifetime alcohol use disorder severity, gender, race/ethnicity, age, religiosity, and current income. Other predictors of higher odds of AA attendance included greater alcohol use disorder severity, older age, and lower income. Female gender and Black and Latino/Latina/Latinx race/ethnicity were uniquely associated with lower odds of attending AA relative to male and White respondents, respectively. The model showed no association between religiosity and AA attendance.
AA attendance by participant group. After controlling for individual factors like alcohol use disorder severity, the apparent above differences between groups for men were not statistically significant, meaning it cannot be determined if the change between male groups was attributable to group differences, or just random chance.
When analyzed separately, women and men had differing patterns of relationships between individual characteristics and AA attendance.
To determine if these observed associations held for both men and women, the researchers repeated this analysis for men and women separately. They also explored whether the associations each of alcohol use disorder severity, race/ethnicity, age, religiosity, and current income with AA attendance were conditional on sexual minority status – that is, whether these relationships were stronger or weaker among sexual minorities relative to heterosexual identified individuals (i.e., the conducted statistical interaction tests).
For women, the results closely mirrored the findings in the overall sample. Both lesbian and bisexual women respondents showed greater odds of attending AA than their heterosexual counterparts after controlling for lifetime alcohol use disorder severity and demographic characteristics. Among women, other predictors of higher odds of AA attendance included greater alcohol use disorder severity, older age, and lower income. Black and Latina race/ethnicity was associated with lower odds of attending AA relative to White respondents. The models showed no association between religiosity and AA attendance among female respondents.
In the female specific analysis, interaction effects were also observed. Among sexual minority women, there was a stronger association between older age and AA attendance, a stronger association between greater religiosity and AA attendance, and a weaker association between lifetime alcohol use disorder severity and AA attendance, compared to heterosexual women. For example, identifying with a religion was associated with AA attendance for sexual minority, but not heterosexual, women.
For men, the models showed fewer associations between measured characteristics and AA attendance. As with the overall model including both men and women, greater alcohol use disorder severity and older age predicted higher odds of AA attendance, and the models showed no association between religiosity and AA attendance. Unlike the aggregated analysis, however, sexual orientation, race/ethnicity, and income were not associated with AA attendance for men. The models showed no statistically significant interactions between sexual orientation and these other factors.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study, the authors compared sexual minority and heterosexual individuals on AA attendance and explored associated factors. In the first model including all participants (i.e., both women and men), the study authors found that gay/lesbian and bisexual individuals were more likely to have attended AA than their heterosexual counterparts. This may be in part because sexual minority identifying individuals, on average, tend to have more psychosocial challenges and more severe substance use histories compared to their heterosexual peers.
In their subsequent analysis where women and men were considered separately, they found that lesbian and bisexual women were more than twice as likely as heterosexual women to have ever attended AA meetings. However, gay and bisexual men had similar rates of AA attendance to their heterosexual counterparts. This suggests that observed differences in AA attendance between sexual minority and sexual majority individuals in the initial statistical model were being driven by the women in the sample and highlights the importance of considering gender in such research (i.e., rather than assuming gay men and lesbian women are the same).
As the research team noted, one possible explanation for the finding that sexual minority women are more likely than heterosexual women to attend AA is a possible greater need for social support for alcohol-related problems. In support of this idea, past research has shown that on average, sexual minority women have less social support and greater social support need than their heterosexual counterparts. Furthermore, for many people, and particularly for women, AA is an important source of social support. Given these previous findings, it would make sense that sexual minority women may be more inclined to utilize the social support offered by attending AA.
Findings for men were more mixed, with the authors’ results suggesting that sexual minority men are similar to heterosexual men in terms of ever attending AA. The study authors suggest that alcohol use disorder severity may have been influencing results for men because gay men showed higher alcohol use disorder (AUD) severity than their heterosexual counterparts. At the same time, it is possible gay and heterosexual men are simply not different in terms of attending AA. In other words, while sexual minorities have higher alcohol use disorder severity overall, and individuals with more severe alcohol use disorder tend have higher rates of AA attendance, severity accounts for sexual minority men’s greater attendance. In women, however, there may be something unique about sexual minority status driving this greater AA attendance.
It will be important for future studies to explore alcohol use disorder severity when exploring AA attendance among sexual minority males. The study also highlights the importance of modeling so-called ‘intersectionality’—relationships among multiple categories of social identification such as gender, race/ethnicity, and sexual identification—in research on alcohol use disorder treatment and recovery support services.
As noted by the researchers:
The study’s measure of AA attendance indicated only whether respondents had ever attended an AA meeting. It can’t be known from these results whether sexual monitory individuals differed from heterosexual individuals in continued AA attendance or degree of AA involvement.
This study utilized a binary gender classification system, which precludes the analysis of gender non-binary individuals. Also, the study did not account for transgender identification.
The study’s sexual orientation measure may potentially limit this study’s generalizability. Though this study considered bisexual respondents separately from monosexual participants (i.e., gay and lesbian), this sexuality classification scheme does not include the entire spectrum of sexual orientations.
The cross-sectional design (i.e., a survey conducted in a single point in time) and lengthy period of data collection limits this study. It may be difficult for participants to recall past AUD severity.
AA attendance may influence retrospective reporting of past AUD severity, perhaps by leading participants to reflect on past alcohol-related distress and impairment and report greater problem severity.
Additionally:
Though this study had a large sample size (N= 7,862), only 367 participants identified as sexual minority individuals. Imbalanced samples like this can lead to problems in statistical models such as over- or under-estimating effects and reduce confidence in findings.
BOTTOM LINE
In this study comparing lifetime AA attendance and factors associated with attendance, in sexual minority versus heterosexual identified individuals with at least one alcohol use disorder symptom, sexual minority women were more likely to endorse ever attending an AA meeting relative to heterosexual women, while sexual minority men endorsed a similar rate of ever attending an AA meeting relative to heterosexual men. Additionally, among sexual minority women, relative to heterosexual women, older as well as more religious women were more likely to have attended AA; also, relative to heterosexual women, the relation between alcohol use disorder symptom severity and lifetime AA attendance was weaker. Though the study’s findings cannot speak to potential benefits associated with AA attendance for sexual minority individuals, these findings signal that sexual minority women, especially those who are older and more religious have a greater propensity to attend AA compared to their heterosexual counterparts.
For individuals and families seeking recovery: Sexual minority women were more likely to endorse ever attending an AA meeting relative to heterosexual women, while sexual minority men endorsed a similar rate of ever attending an AA meeting relative to heterosexual men. Though more work is needed to better understand how sexual minority individuals may or may not benefit from AA relative to heterosexual individuals, AA is an effective approach for addressing alcohol use disorder when used alone or in combination with formal treatment.
For treatment professionals and treatment systems: Sexual minority women were more likely to endorse ever attending an AA meeting relative to heterosexual women, while sexual minority men endorsed a similar rate of ever attending an AA meeting relative to heterosexual men. Helping sexual minority women patients connect with social supports may be particularly important. Though more work is needed to better understand how sexual minority individuals may or may not benefit from AA relative to heterosexual individuals, AA is an effective approach for addressing alcohol use disorder when used alone or in combination with formal treatment. For those whom AA does not feel like a good fit, non-traditional mutual-help programs that might also facilitate social support, like SMART Recovery, LifeRing, and Women for Sobriety as well as exercise-based recovery support services like The Phoenix, may be helpful.
For scientists:Sexual minority women were more likely to endorse ever attending an AA meeting relative to heterosexual women, while sexual minority men endorsed a similar rate of ever attending an AA meeting relative to heterosexual men. More work is needed to better understand how sexual minority individuals may or may not benefit from AA relative to heterosexual individuals. In such research it will be important to consider the role of alcohol use disorder severity.
For policy makers: Sexual minority women were more likely to endorse ever attending an AA meeting relative to heterosexual women, while sexual minority men endorsed a similar rate of ever attending an AA meeting relative to heterosexual men. Findings from this study, as well as prior research, suggest sexual minority women have additional need for social support. Greater social support infrastructure is needed, particularly for sexual minority women. Such infrastructure can be created through supporting recovery community centers and non-traditional mutual-help programs like SMART Recovery, LifeRing, and Women for Sobriety as well as exercise-based recovery support services like The Phoenix.