
Group Exercise to Improve Quality of Life in Addiction Patients
The benefits of exercise extend beyond the physical. Exercise has been shown to have a positive impact on psychological symptoms such as anxiety, depression, and self-esteem, and physically active patients who initiate exercise after the onset of a substance use disorder (SUD) are less likely to relapse than sedentary patients.
Since it can be difficult for individuals to find the motivation to exercise, people in substance use disorder treatment represent a vulnerable population who could greatly benefit from an exercise-based intervention, but may be difficult to engage due to competing health-related priorities.
Muller and Clausen implemented a volunteer-based, non-random study featuring a 10-week low-intensity group exercise pilot program to examine if participation would lead to improvements in the quality of life (QoL) of SUD patients.
To maximize participation and retention, the program featured:
- three different 30-minute weekly sessions (walking/running, ball games, and strength-training)
- coaches to motivate patients
- text message reminders about upcoming sessions
- fitness-related incentives (e.g. monthly gym memberships)
Patients (N = 35) were recruited from four residential treatment facilities in Oslo, Norway. All participants were sedentary—defined as exercising less than 20 minutes a day, 3 days a week for the past 3 months—before the start of the intervention.
Patients were classified as “completers” if they attended at least one session over the 10-week period, while “non-completers” did not attend any sessions. Three quarters of participants were male and over 90% were of Norwegian/Nordic descent. The average age was 41. Over 90% of participants had previously received inpatient treatment for their substance use disorder (SUD). Half reported clinical anxiety, and another half reported clinical depression. At baseline, completers had more somatic conditions and more mental health distress as compared to non-completers. There was no difference in addiction severity between the two groups.
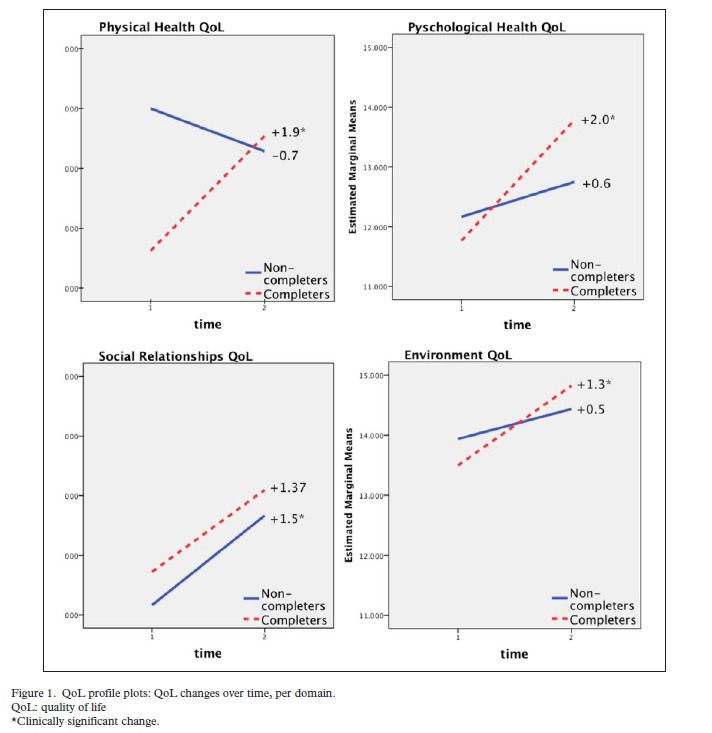
The main outcome, changes in quality of life (QoL), was measured using the World Health Organization Quality of Life Brief. The questionnaire assesses QoL in different domains (physical health, psychological health, social relationships, and environment) to capture aspects of a patient’s SUD that may be missed through traditional clinical measures.
The authors determined which significant changes associated with exercise were also clinically meaningful by calculating the minimum clinically important difference (0.5 of the standard deviation of change).
There was a clinically significant increase in completers’ physical health quality of life (QoL) and psychological health QoL. The decrease in the physical health domain for non-completers was not clinically significant. The improvements for both groups seen in the social relationships and environment domains were not significant.
For completers, anxiety decreased from 74% at baseline to 46% at the end of the intervention, and depression decreased from 78% to 36%. More non-completers (63%) reported substance use at the end of the program as compared to completers (26%).
IN CONTEXT
An important finding is that those who participated in this low-intensity exercise program reported better quality of life (QoL) and substance use outcomes. These QoL improvements appear to be independent of actual physical fitness improvements as participants only exercised for an average of 13 out of 30 sessions (approximately 1-2 times per week).
- LIMITATIONS
-
findings should be interpreted with the nature of the intervention in mind. The authors chose a group exercise intervention with a variety of session types and motivational coaches to decrease attrition; individual exercise programs may be more difficult to adhere to and produce fewer benefits as a result. The authors noted that the fitness-based incentives were not considered to be a strength of the program by participants; other types of incentives (e.g. a pass to leave the treatment facility for the afternoon or a prize raffle) could be more reinforcing. Also, significantly greater physical and psychological distress for completers (vs. non-completers) at the beginning of the study may have increased their motivation for participation, making the results difficult to interpret. Since this was an observational study, a randomized controlled trial is necessary before the QoL improvements can be attributed to exercise.
BOTTOM LINE
- For individuals & families seeking recovery: Exercise has been proven to offer myriad health benefit including increasing an overall sense of well-being. Try adding it to a daily or weekly routine.
- For scientists: More evidence is needed to show a causal link between exercise and quality of life improvements for people with SUDs. Studies evaluating different types of fitness programs are also necessary to determine if certain interventions are more beneficial. The effects of exercise might be both direct (increasing physical robustness) and indirect (representing a behavior that provides new structure and can compete with drug use).
- For policy makers: If exercise-based interventions continue to be supported in the literature, cost benefit analyses should be conducted to determine feasibility of widespread program implementation.
- For treatment professionals and treatment systems: Unless medically contraindicated, encourage patients to exercise as a supplement to their existing treatment plan.
CITATIONS
Muller, A. E., & Clausen, T. (2015). Group exercise to improve quality of life among substance use disorder patients. Scandinavian journal of public health, 43(2), 146-152.
