Recovery prevalence and pathways of lesbian, gay, and bisexual individuals
Lesbian, gay, and bisexual (LGB) individuals have higher rates of alcohol and other drug problems than those who identify as heterosexual. Research on their recovery experiences can help tailor clinical, community, and public health services for these at-risk groups. This study comparing pathways of recovery and indicators of functioning and well-being among LGB versus heterosexual adults revealed important differences.
Given the high rates of alcohol and drug use problems among the LGB population, it is not surprising that LGB individuals also use substance use disorder treatment services at higher rates than heterosexual people. However, LGB individuals also report more barriers to treatment compared to heterosexual individuals, including limited availability of LGB-affirming treatment programs and fear of experiencing discrimination, stigma, harassment, or being misunderstood when trying to access treatment. So, although LGB adults with alcohol or drug use problems utilize treatment services at higher rates, many LGB adults also delay seeking needed treatment.
Research on the experiences of people who have resolved an alcohol or drug use problem is an emerging area, covering all pathways to change including treatment-seeking individuals. By learning more about how LGB individuals in recovery compare to their heterosexual counterparts on mental health histories, services used, recovery pathways followed, quality of life, and psychological functioning, researchers can help inform and enhance services to better meet the treatment, recovery support service, and public health policy, needs of LGB individuals.
This study reports on the prevalence of LGB adults who have resolved an alcohol or drug use problem in the U.S. Additionally, the researchers compared LGB and heterosexual adults on demographics, clinical characteristics, pathways to recovery, and indicators of psychosocial functioning and well-being, as well as tested which factors might explain any observed disparities between LGB and heterosexual individuals.
Given the high rates of alcohol and drug use problems among the LGB population, it is not surprising that LGB individuals also use substance use disorder treatment services at higher rates than heterosexual people. However, LGB individuals also report more barriers to treatment compared to heterosexual individuals, including limited availability of LGB-affirming treatment programs and fear of experiencing discrimination, stigma, harassment, or being misunderstood when trying to access treatment. So, although LGB adults with alcohol or drug use problems utilize treatment services at higher rates, many LGB adults also delay seeking needed treatment.
Research on the experiences of people who have resolved an alcohol or drug use problem is an emerging area, covering all pathways to change including treatment-seeking individuals. By learning more about how LGB individuals in recovery compare to their heterosexual counterparts on mental health histories, services used, recovery pathways followed, quality of life, and psychological functioning, researchers can help inform and enhance services to better meet the treatment, recovery support service, and public health policy, needs of LGB individuals.
This study reports on the prevalence of LGB adults who have resolved an alcohol or drug use problem in the U.S. Additionally, the researchers compared LGB and heterosexual adults on demographics, clinical characteristics, pathways to recovery, and indicators of psychosocial functioning and well-being, as well as tested which factors might explain any observed disparities between LGB and heterosexual individuals.
HOW WAS THIS STUDY CONDUCTED?
This study is a secondary analysis from the National RecoveryStudy which surveyed a nationally representative sample of adults in the U.S. who responded “yes” to the question, “Did you used to have a problem with drugs or alcohol, but no longer do?” The researchers examined: a) the number of people in the study who identified as lesbian, gay, or bisexual (LGB); b) if LGB participants in the study differed from heterosexual participants on demographics, clinical histories, and indicators of well-being; c) what factors could explain differences in well-being between LGB and heterosexual participants.
Participants in this study were recruited using an online survey response pool company that helps researchers gain access to nationally representative samples. A nationally representative group of 39,809 individuals were sent a screening question via email, to which 25,229 responded (63.4%). Of those who responded, 2,002 indicated they had resolved an alcohol or drug use problem.
Participants were asked to report their sexual orientation with response options: “heterosexual or straight,” “gay or lesbian,” “bisexual,” or “something else.” Participants were grouped as LGB if they selected, gay, lesbian, bisexual, or something else. Of the LGB adults in the sample, 17 selected “something else” other than heterosexual or lesbian, gay, or bisexual and were included in the LGB group.
Participants also were assessed on their prior substance use histories and substance use and mental health treatment and recovery support services utilization, length of recovery, lifetime co-occurring psychiatric diagnoses, their current functioning, quality of life, their degree of comfort in disclosing their substance use histories to other people, a number of indices of well-being, criminal justice history, and several other factors.
The analyses compared the distribution of demographics, clinical characteristics, alcohol and drug use history, problem resolution pathway, and disclosure comfort between LGB and heterosexual participants in the sample. Second, the researchers examined the association between LGB identity and indicators of well-being (i.e., quality of life, psychological distress, happiness, self-esteem, recovery capital). The researchers then examined which of these demographic, clinical, and recovery-related variables on which LGB were different from heterosexual participants might explain differences in well-being outcomes.
Participants were on average middle-aged (LGB average = 44 years old; heterosexual average = 47 years old). About one third were female (LGB group, 35% female; heterosexual group, 40% female). In terms of race and ethnicity, a little more than half of participants were White/non-Hispanic (LGB group, 56%; heterosexual group, 62%), 14% were Black/non-Hispanic (LGB group, 13%; heterosexual group, 14%), and about 17% were Hispanic (LGB group, 18%; heterosexual group, 17%). There were no differences in age, gender, or race/ethnicity between the LGB and heterosexual groups.
WHAT DID THIS STUDY FIND?
LGB adults represent a large proportion of adults in recovery but face more challenges.
LGB participants were almost half as likely to employed than heterosexual participants. LGB participants were 1.5 times more likely to have an arrest history compared to heterosexual participants. LGB and heterosexual participants did not differ on other sociodemographic variables. There were no differences in age, gender, race/ethnicity, household income, or education.
LGB participants were more than 2 times as likely to have a lifetime history of a co-occurring psychiatric diagnosis than heterosexual participants. LGB participants also had a 2.5-times greater odds of reporting opioids as their primary substance compared to heterosexual participants. LGB participants also had fewer years in recovery, on average, 3 fewer than heterosexual participants. There were no differences between LGB and heterosexual participants across other substances, prior inpatient or outpatient treatment history, number of serious quit attempts, disclosure comfort, and age of onset of regular substance use.
LGB participants reported lower quality of life, happiness, self-esteem, recovery capital, and higher levels of psychological distress overall.
LGB participants had lower quality of life, happiness, self-esteem, recovery capital, and higher levels of psychological distress compared to heterosexual participants.
Differences in quality of life, happiness, self-esteem, and recovery capital were no longer present, though, after controlling for employment, time in recovery, arrest history, primary substance, and co-occurring psychiatric diagnoses. In follow-up analyses, the researchers found that higher rates of co-occurring psychiatric diagnoses accounted for most of the differences in well-being outcomes between LGB and heterosexual participants. This suggests that co-occurring psychiatric diagnoses might be a more major factor in helping to explain disparities between LGB and heterosexual participants in functioning and well-being. However, even when accounting for these differences in psychiatric status, LGB participants still had higher levels of psychological distress compared to heterosexual participants, meaning that there are other reasons not accounted for in these analyses that are contributing to this greater psychological distress among LGB individuals in recovery.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
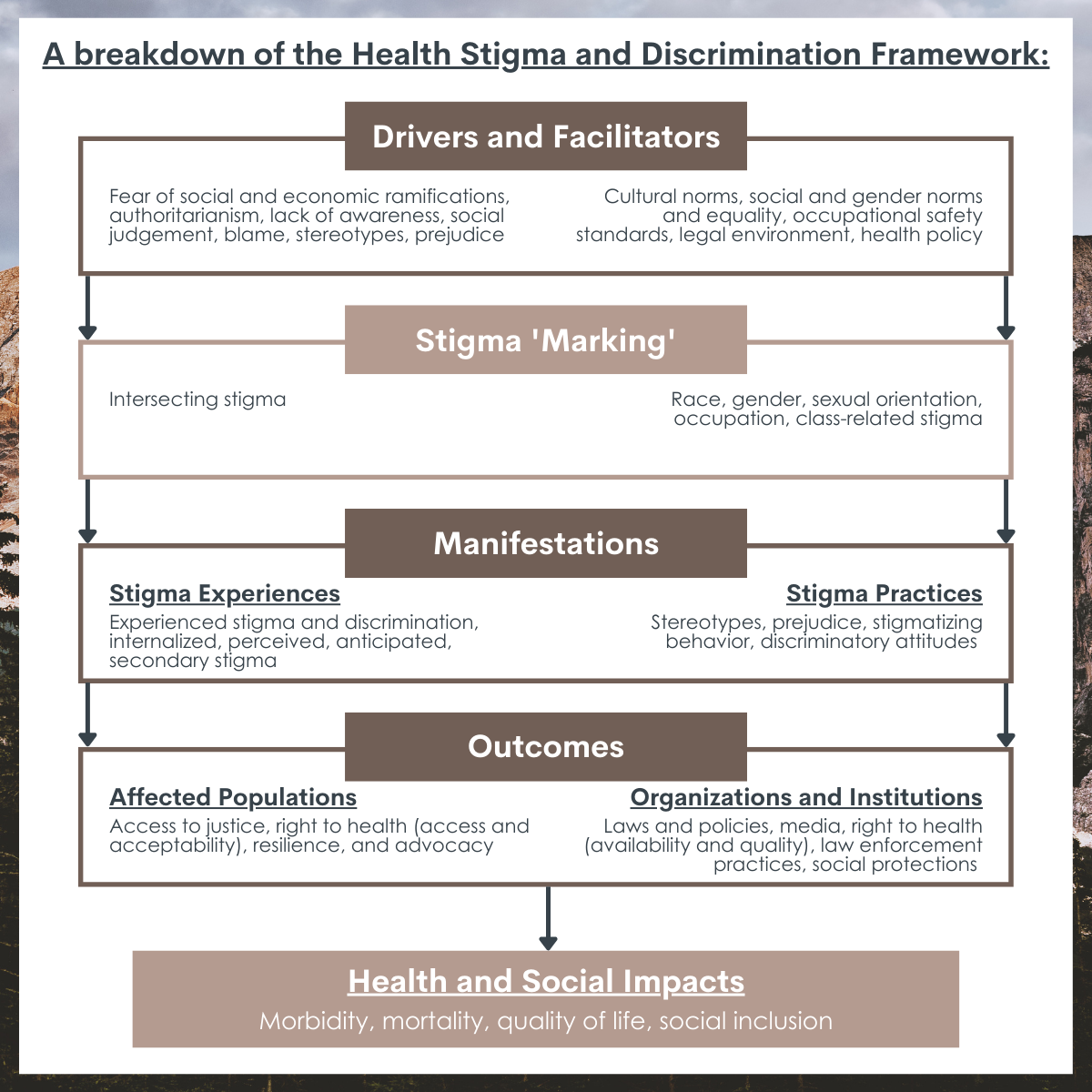
Despite a lack of LGB-affirming recovery services, a high proportion of LGB adults are finding pathways to recovery. It is notable that LGB participants differed from heterosexual participants on a few demographic and clinical history characteristics, including employment, arrest history, years in recovery, primary substance (i.e., opioids), and co-occurring psychiatric diagnoses. Some of these differences, in particular employment, criminal legal system history, and years in recovery may represent downstream effects of structural-level sexual-orientation stigma and discrimination, as structural forms of stigma could affect a person’s socioeconomic status and access to resources. There is also evidence of bias in the diagnosis of certain psychiatric conditions among the LGB population, which could be another form structural or institutional-level stigma. Specifically, LGB individuals are diagnosed with borderline personality disorder at disproportionately high rates, even when controlling for known clinical factors associated with borderline personality disorder (age, gender, comorbid posttraumatic stress disorder, maladaptive personality domains). This suggests that clinicians may be predisposed to provide a borderline personality disorder diagnosis to LGB patients, either through measurement bias or bias among clinicians themselves, that is independent of presenting psychopathology. These kinds of systematic differences in the way LGB individuals are treated suggest how stigma may be being enacted on an institutional or systems level to create disparities, and could affect variables measured in the current study, such as the rates of co-occurring psychiatric disorders reported among LGB participants.
LGB participants also reported lower quality of life, self-esteem, happiness, recovery capital, and psychological distress. These were partially explained by the differences noted above in employment, years in recovery, primary substance, arrest history, and co-occurring psychiatric diagnoses, suggesting that poorer quality of life and well-being indices among the LGB group are in part due to their lack of socioeconomic resources and worse clinical histories.
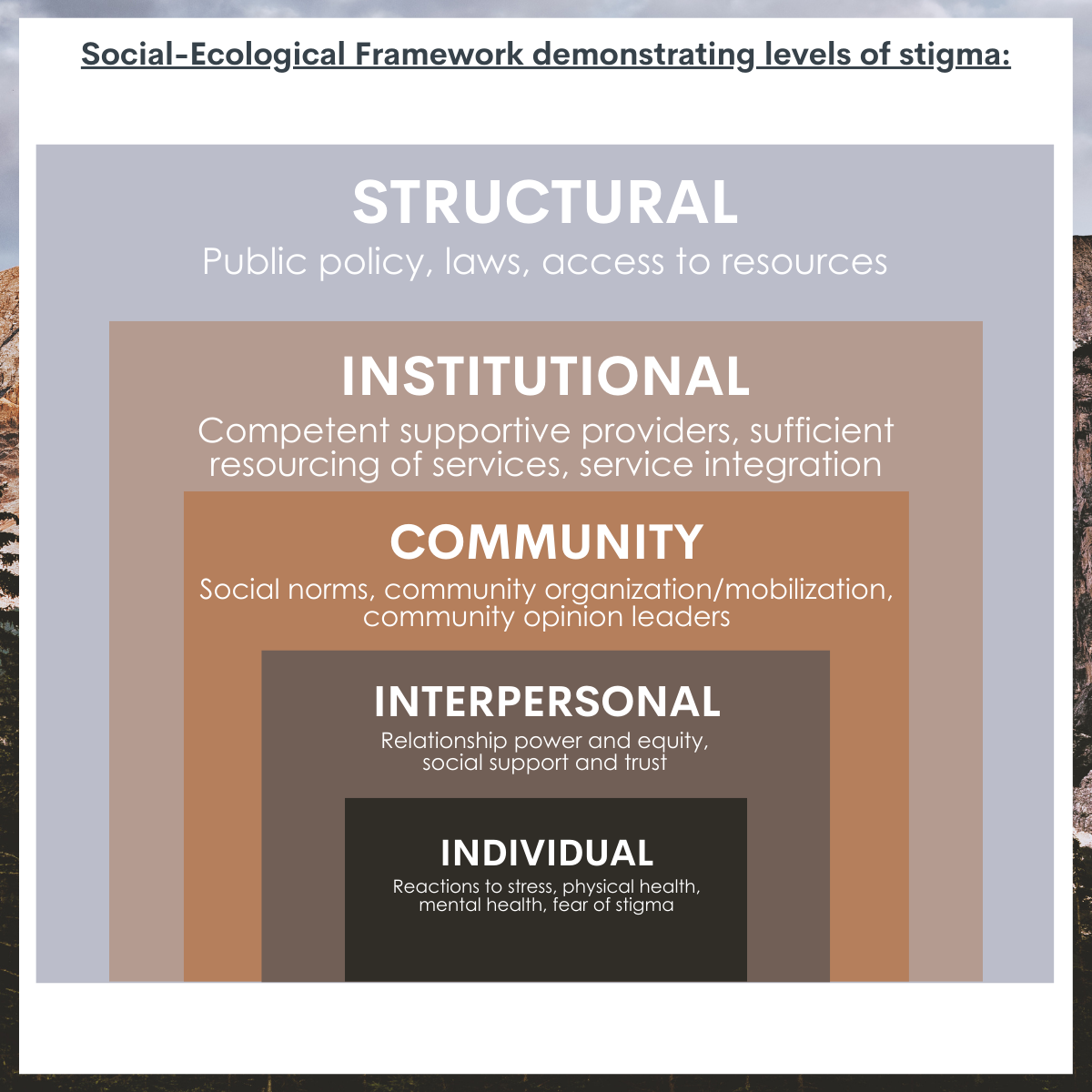
Of note, when controlling for these socioeconomic and clinical history factors (e.g., psychiatric comorbidity), LGB participants still had higher psychological distress than heterosexual participants indicating that other factors not captured in this study are contributing to this elevated stress. One possibility is that LGB individuals continue to suffer discrimination more than heterosexuals because of their more stigmatized sexual minority status. This in turn can perpetuate psychological distress. This perhaps may also be in the form of trauma, as LGB individuals experience elevated rates of physical and sexual assault, harassment, bullying, and hate crime throughout childhood, adolescence, and adulthood. Such violence, trauma, and discrimination has been associated with substance use problems, depression, and suicide among LGB individuals, and likely contributes to health disparities in this population. Future research should examine the role of structural/institutional, interpersonal, and individual forms of stigma on recovery pathways and well-being.
More research is needed to understand differences in opioids as a primary substance among LGB and heterosexual adults in recovery. Perhaps differences in actual or perceived substance use norms among the LGB community would increase the likelihood of those whose primary substance is opioids to seek recovery, rather than those whose primary substance is, for example, alcohol or cannabis. However, this is purely speculation and more research is needed in this area to examine community norms of substance use across specific types of substances. It is also notable that LGB participants had fewer years in recovery than heterosexual participants. This may represent a more turbulent recovery journey that may result in challenges in staying in recovery; and/or decreased access to effective resources for LGB individuals. Future research should ask LGB adults with alcohol or other drug use problems their desires and preferences for recovery-oriented services.
The researchers did not include measures that assess participants’ experiences of discrimination on individual, interpersonal, or structural-levels, which may affect LGB individual’s well-being in recovery. Future research should include more in-depth assessments of sexual identity-specific stigma to measure how this affects pathways to recovery.
LGB participants in this study were grouped together and were not separated by sexual orientation (e.g., lesbian, gay, bisexual). Examining these groups separately is important for future research, as the experiences of lesbian, gay and bisexual individuals in recovery may differ. For example, in a study on treatment utilization, bisexual individuals used mutual help meetings and professional treatment services 2-5 times more than heterosexual individuals. If LGB participants had been grouped together in that study, the researchers may not have seen that bisexual individuals were primarily driving the effect.
This study is cross-sectional, meaning that researchers don’t know when certain factors happened over time and cannot say that one factor caused another. For example, many participants in this study started their recovery journey at various points over the last 40 years and it is possible that more recent legal protections for LGB people (e.g., marriage equality) may affect LGB individuals’ recovery journeys differently. Future research should assess participants over time so they can track changes in access to supports and more confidently say one factor likely caused another.
BOTTOM LINE
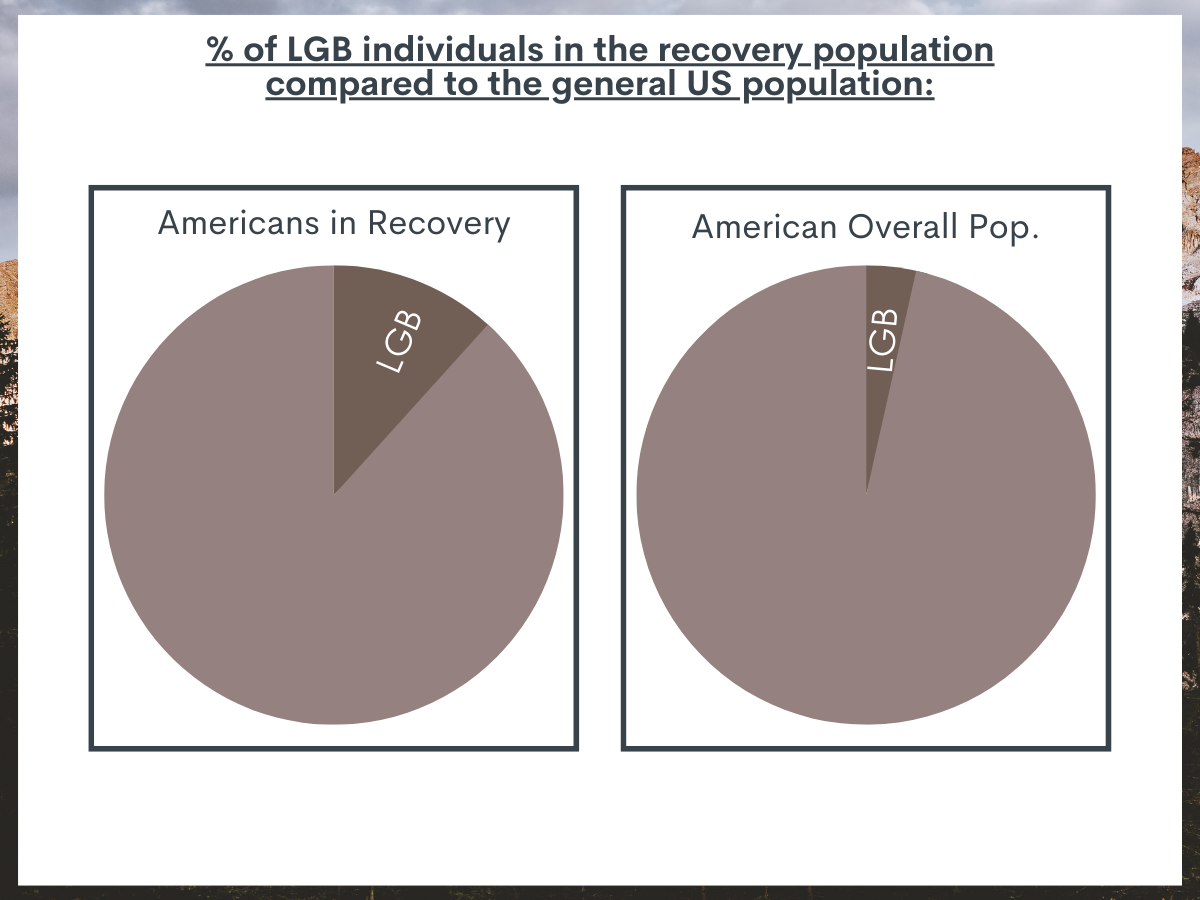
In the U.S., 11.7% of adults in recovery identify as lesbian, gay, or bisexual (LGB). LGB adults in recovery were less likely to be employed, had fewer years in recovery, and were more likely to have an arrest history, report opioids as their primary substance, and have a co-occurring psychiatric diagnosis compared to their heterosexual counterparts. Even after accounting for differences in demographic and clinical/legal histories among LGB and heterosexual groups, LGB adults in recovery still had greater psychological distress.
For individuals and families seeking recovery: A high proportion of LGB people experience alcohol and drug use problems and also are in recovery. Even when accounting for socioeconomic and recovery pathway differences, LGB adults experienced greater psychological distress than heterosexual adults. This may be related to sexual orientation stigma and discrimination, which increases psychological distress and reduces access to resources and supports. Evidence shows that LGBTQ people who have access to spaces that affirm their sexual orientation and gender identity report better mental health. If families can support their LGB loved ones by providing an affirming and accepting space of their sexual and gender identity, this may reduce psychological distress for LGB people with alcohol or drug use problems. Learn more about resources for family members of people who are LGBTQ here.
For treatment professionals and treatment systems: A high proportion of LGB people experience alcohol and drug use problems and are also in recovery. Even when accounting for socioeconomic and recovery pathway differences, LGB adults experienced greater psychological distress than heterosexual adults. This may be related to sexual orientation stigma and discrimination, which increases psychological distress and reduces access to resources and supports. Evidence shows that LGBTQ people who have access to spaces that affirm their sexual orientation and gender identity report better mental health. If treatment providers can offer LGBTQ-affirming care or make their treatment settings affirming, it may improve their LGB patients’ mental health. Providers can obtain additional training on LGBTQ affirming treatment practices here.
For scientists:Findings from this secondary analysis of the National Recovery Study found that 11.7% of adults in recovery identify as lesbian, gay, or bisexual. Survey weight adjusted regression models showed LGB participants were less likely to be employed, more likely to have an arrest history, had fewer years since substance use problem resolution, were more likely to report opioids as their primary substance, and were more likely to report co-occurring psychiatric diagnoses. In unadjusted models, LGB participants reported lower quality of life, happiness, self-esteem, recovery capital, and higher levels of psychological distress. When controlling for group differences in demographic and clinical/legal histories described above, there were no longer significant differences between LGB and heterosexual participants on quality of life, happiness, self-esteem, and recovery capital; however, LGB participants still had significantly higher levels of psychological distress. This suggests that while controlling for structural-level factors like socioeconomic status, and clinical/legal histories and pathways to recovery, other factors could still be influencing psychological distress among LGB adults in recovery. Future studies should examine other factors that could be influencing psychological distress among LGB people longitudinally, such as stigma and discrimination on structural, interpersonal, and individual levels. At the same time, research should also focus on developing and testing clinical and public health approaches to remedy these inequities.
For policy makers: A high proportion of LGB people experience alcohol and drug use problems and are also in recovery. Even when accounting for socioeconomic and recovery pathway differences, LGB adults experienced greater psychological distress than heterosexual adults. This may be related to sexual orientation stigma and discrimination, which increases psychological distress and reduces access to resources and supports. Evidence shows that LGBTQ people, for example, who have access to spaces that affirm their sexual orientation and gender identity report better mental health. In fact, research shows that at the state-level, LGBTQ protective policy is associated with better health outcomes for LGBTQ people. Policy can support structural interventions to reduce stigma, such as legal protections for LGBTQ people in workplace settings, health care, and in schools.
Given the high rates of alcohol and drug use problems among the LGB population, it is not surprising that LGB individuals also use substance use disorder treatment services at higher rates than heterosexual people. However, LGB individuals also report more barriers to treatment compared to heterosexual individuals, including limited availability of LGB-affirming treatment programs and fear of experiencing discrimination, stigma, harassment, or being misunderstood when trying to access treatment. So, although LGB adults with alcohol or drug use problems utilize treatment services at higher rates, many LGB adults also delay seeking needed treatment.
Research on the experiences of people who have resolved an alcohol or drug use problem is an emerging area, covering all pathways to change including treatment-seeking individuals. By learning more about how LGB individuals in recovery compare to their heterosexual counterparts on mental health histories, services used, recovery pathways followed, quality of life, and psychological functioning, researchers can help inform and enhance services to better meet the treatment, recovery support service, and public health policy, needs of LGB individuals.
This study reports on the prevalence of LGB adults who have resolved an alcohol or drug use problem in the U.S. Additionally, the researchers compared LGB and heterosexual adults on demographics, clinical characteristics, pathways to recovery, and indicators of psychosocial functioning and well-being, as well as tested which factors might explain any observed disparities between LGB and heterosexual individuals.
Given the high rates of alcohol and drug use problems among the LGB population, it is not surprising that LGB individuals also use substance use disorder treatment services at higher rates than heterosexual people. However, LGB individuals also report more barriers to treatment compared to heterosexual individuals, including limited availability of LGB-affirming treatment programs and fear of experiencing discrimination, stigma, harassment, or being misunderstood when trying to access treatment. So, although LGB adults with alcohol or drug use problems utilize treatment services at higher rates, many LGB adults also delay seeking needed treatment.
Research on the experiences of people who have resolved an alcohol or drug use problem is an emerging area, covering all pathways to change including treatment-seeking individuals. By learning more about how LGB individuals in recovery compare to their heterosexual counterparts on mental health histories, services used, recovery pathways followed, quality of life, and psychological functioning, researchers can help inform and enhance services to better meet the treatment, recovery support service, and public health policy, needs of LGB individuals.
This study reports on the prevalence of LGB adults who have resolved an alcohol or drug use problem in the U.S. Additionally, the researchers compared LGB and heterosexual adults on demographics, clinical characteristics, pathways to recovery, and indicators of psychosocial functioning and well-being, as well as tested which factors might explain any observed disparities between LGB and heterosexual individuals.
HOW WAS THIS STUDY CONDUCTED?
This study is a secondary analysis from the National RecoveryStudy which surveyed a nationally representative sample of adults in the U.S. who responded “yes” to the question, “Did you used to have a problem with drugs or alcohol, but no longer do?” The researchers examined: a) the number of people in the study who identified as lesbian, gay, or bisexual (LGB); b) if LGB participants in the study differed from heterosexual participants on demographics, clinical histories, and indicators of well-being; c) what factors could explain differences in well-being between LGB and heterosexual participants.
Participants in this study were recruited using an online survey response pool company that helps researchers gain access to nationally representative samples. A nationally representative group of 39,809 individuals were sent a screening question via email, to which 25,229 responded (63.4%). Of those who responded, 2,002 indicated they had resolved an alcohol or drug use problem.
Participants were asked to report their sexual orientation with response options: “heterosexual or straight,” “gay or lesbian,” “bisexual,” or “something else.” Participants were grouped as LGB if they selected, gay, lesbian, bisexual, or something else. Of the LGB adults in the sample, 17 selected “something else” other than heterosexual or lesbian, gay, or bisexual and were included in the LGB group.
Participants also were assessed on their prior substance use histories and substance use and mental health treatment and recovery support services utilization, length of recovery, lifetime co-occurring psychiatric diagnoses, their current functioning, quality of life, their degree of comfort in disclosing their substance use histories to other people, a number of indices of well-being, criminal justice history, and several other factors.
The analyses compared the distribution of demographics, clinical characteristics, alcohol and drug use history, problem resolution pathway, and disclosure comfort between LGB and heterosexual participants in the sample. Second, the researchers examined the association between LGB identity and indicators of well-being (i.e., quality of life, psychological distress, happiness, self-esteem, recovery capital). The researchers then examined which of these demographic, clinical, and recovery-related variables on which LGB were different from heterosexual participants might explain differences in well-being outcomes.
Participants were on average middle-aged (LGB average = 44 years old; heterosexual average = 47 years old). About one third were female (LGB group, 35% female; heterosexual group, 40% female). In terms of race and ethnicity, a little more than half of participants were White/non-Hispanic (LGB group, 56%; heterosexual group, 62%), 14% were Black/non-Hispanic (LGB group, 13%; heterosexual group, 14%), and about 17% were Hispanic (LGB group, 18%; heterosexual group, 17%). There were no differences in age, gender, or race/ethnicity between the LGB and heterosexual groups.
WHAT DID THIS STUDY FIND?
LGB adults represent a large proportion of adults in recovery but face more challenges.
LGB participants were almost half as likely to employed than heterosexual participants. LGB participants were 1.5 times more likely to have an arrest history compared to heterosexual participants. LGB and heterosexual participants did not differ on other sociodemographic variables. There were no differences in age, gender, race/ethnicity, household income, or education.
LGB participants were more than 2 times as likely to have a lifetime history of a co-occurring psychiatric diagnosis than heterosexual participants. LGB participants also had a 2.5-times greater odds of reporting opioids as their primary substance compared to heterosexual participants. LGB participants also had fewer years in recovery, on average, 3 fewer than heterosexual participants. There were no differences between LGB and heterosexual participants across other substances, prior inpatient or outpatient treatment history, number of serious quit attempts, disclosure comfort, and age of onset of regular substance use.
LGB participants reported lower quality of life, happiness, self-esteem, recovery capital, and higher levels of psychological distress overall.
LGB participants had lower quality of life, happiness, self-esteem, recovery capital, and higher levels of psychological distress compared to heterosexual participants.
Differences in quality of life, happiness, self-esteem, and recovery capital were no longer present, though, after controlling for employment, time in recovery, arrest history, primary substance, and co-occurring psychiatric diagnoses. In follow-up analyses, the researchers found that higher rates of co-occurring psychiatric diagnoses accounted for most of the differences in well-being outcomes between LGB and heterosexual participants. This suggests that co-occurring psychiatric diagnoses might be a more major factor in helping to explain disparities between LGB and heterosexual participants in functioning and well-being. However, even when accounting for these differences in psychiatric status, LGB participants still had higher levels of psychological distress compared to heterosexual participants, meaning that there are other reasons not accounted for in these analyses that are contributing to this greater psychological distress among LGB individuals in recovery.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Despite a lack of LGB-affirming recovery services, a high proportion of LGB adults are finding pathways to recovery. It is notable that LGB participants differed from heterosexual participants on a few demographic and clinical history characteristics, including employment, arrest history, years in recovery, primary substance (i.e., opioids), and co-occurring psychiatric diagnoses. Some of these differences, in particular employment, criminal legal system history, and years in recovery may represent downstream effects of structural-level sexual-orientation stigma and discrimination, as structural forms of stigma could affect a person’s socioeconomic status and access to resources. There is also evidence of bias in the diagnosis of certain psychiatric conditions among the LGB population, which could be another form structural or institutional-level stigma. Specifically, LGB individuals are diagnosed with borderline personality disorder at disproportionately high rates, even when controlling for known clinical factors associated with borderline personality disorder (age, gender, comorbid posttraumatic stress disorder, maladaptive personality domains). This suggests that clinicians may be predisposed to provide a borderline personality disorder diagnosis to LGB patients, either through measurement bias or bias among clinicians themselves, that is independent of presenting psychopathology. These kinds of systematic differences in the way LGB individuals are treated suggest how stigma may be being enacted on an institutional or systems level to create disparities, and could affect variables measured in the current study, such as the rates of co-occurring psychiatric disorders reported among LGB participants.
LGB participants also reported lower quality of life, self-esteem, happiness, recovery capital, and psychological distress. These were partially explained by the differences noted above in employment, years in recovery, primary substance, arrest history, and co-occurring psychiatric diagnoses, suggesting that poorer quality of life and well-being indices among the LGB group are in part due to their lack of socioeconomic resources and worse clinical histories.
Of note, when controlling for these socioeconomic and clinical history factors (e.g., psychiatric comorbidity), LGB participants still had higher psychological distress than heterosexual participants indicating that other factors not captured in this study are contributing to this elevated stress. One possibility is that LGB individuals continue to suffer discrimination more than heterosexuals because of their more stigmatized sexual minority status. This in turn can perpetuate psychological distress. This perhaps may also be in the form of trauma, as LGB individuals experience elevated rates of physical and sexual assault, harassment, bullying, and hate crime throughout childhood, adolescence, and adulthood. Such violence, trauma, and discrimination has been associated with substance use problems, depression, and suicide among LGB individuals, and likely contributes to health disparities in this population. Future research should examine the role of structural/institutional, interpersonal, and individual forms of stigma on recovery pathways and well-being.
More research is needed to understand differences in opioids as a primary substance among LGB and heterosexual adults in recovery. Perhaps differences in actual or perceived substance use norms among the LGB community would increase the likelihood of those whose primary substance is opioids to seek recovery, rather than those whose primary substance is, for example, alcohol or cannabis. However, this is purely speculation and more research is needed in this area to examine community norms of substance use across specific types of substances. It is also notable that LGB participants had fewer years in recovery than heterosexual participants. This may represent a more turbulent recovery journey that may result in challenges in staying in recovery; and/or decreased access to effective resources for LGB individuals. Future research should ask LGB adults with alcohol or other drug use problems their desires and preferences for recovery-oriented services.
The researchers did not include measures that assess participants’ experiences of discrimination on individual, interpersonal, or structural-levels, which may affect LGB individual’s well-being in recovery. Future research should include more in-depth assessments of sexual identity-specific stigma to measure how this affects pathways to recovery.
LGB participants in this study were grouped together and were not separated by sexual orientation (e.g., lesbian, gay, bisexual). Examining these groups separately is important for future research, as the experiences of lesbian, gay and bisexual individuals in recovery may differ. For example, in a study on treatment utilization, bisexual individuals used mutual help meetings and professional treatment services 2-5 times more than heterosexual individuals. If LGB participants had been grouped together in that study, the researchers may not have seen that bisexual individuals were primarily driving the effect.
This study is cross-sectional, meaning that researchers don’t know when certain factors happened over time and cannot say that one factor caused another. For example, many participants in this study started their recovery journey at various points over the last 40 years and it is possible that more recent legal protections for LGB people (e.g., marriage equality) may affect LGB individuals’ recovery journeys differently. Future research should assess participants over time so they can track changes in access to supports and more confidently say one factor likely caused another.
BOTTOM LINE
In the U.S., 11.7% of adults in recovery identify as lesbian, gay, or bisexual (LGB). LGB adults in recovery were less likely to be employed, had fewer years in recovery, and were more likely to have an arrest history, report opioids as their primary substance, and have a co-occurring psychiatric diagnosis compared to their heterosexual counterparts. Even after accounting for differences in demographic and clinical/legal histories among LGB and heterosexual groups, LGB adults in recovery still had greater psychological distress.
For individuals and families seeking recovery: A high proportion of LGB people experience alcohol and drug use problems and also are in recovery. Even when accounting for socioeconomic and recovery pathway differences, LGB adults experienced greater psychological distress than heterosexual adults. This may be related to sexual orientation stigma and discrimination, which increases psychological distress and reduces access to resources and supports. Evidence shows that LGBTQ people who have access to spaces that affirm their sexual orientation and gender identity report better mental health. If families can support their LGB loved ones by providing an affirming and accepting space of their sexual and gender identity, this may reduce psychological distress for LGB people with alcohol or drug use problems. Learn more about resources for family members of people who are LGBTQ here.
For treatment professionals and treatment systems: A high proportion of LGB people experience alcohol and drug use problems and are also in recovery. Even when accounting for socioeconomic and recovery pathway differences, LGB adults experienced greater psychological distress than heterosexual adults. This may be related to sexual orientation stigma and discrimination, which increases psychological distress and reduces access to resources and supports. Evidence shows that LGBTQ people who have access to spaces that affirm their sexual orientation and gender identity report better mental health. If treatment providers can offer LGBTQ-affirming care or make their treatment settings affirming, it may improve their LGB patients’ mental health. Providers can obtain additional training on LGBTQ affirming treatment practices here.
For scientists:Findings from this secondary analysis of the National Recovery Study found that 11.7% of adults in recovery identify as lesbian, gay, or bisexual. Survey weight adjusted regression models showed LGB participants were less likely to be employed, more likely to have an arrest history, had fewer years since substance use problem resolution, were more likely to report opioids as their primary substance, and were more likely to report co-occurring psychiatric diagnoses. In unadjusted models, LGB participants reported lower quality of life, happiness, self-esteem, recovery capital, and higher levels of psychological distress. When controlling for group differences in demographic and clinical/legal histories described above, there were no longer significant differences between LGB and heterosexual participants on quality of life, happiness, self-esteem, and recovery capital; however, LGB participants still had significantly higher levels of psychological distress. This suggests that while controlling for structural-level factors like socioeconomic status, and clinical/legal histories and pathways to recovery, other factors could still be influencing psychological distress among LGB adults in recovery. Future studies should examine other factors that could be influencing psychological distress among LGB people longitudinally, such as stigma and discrimination on structural, interpersonal, and individual levels. At the same time, research should also focus on developing and testing clinical and public health approaches to remedy these inequities.
For policy makers: A high proportion of LGB people experience alcohol and drug use problems and are also in recovery. Even when accounting for socioeconomic and recovery pathway differences, LGB adults experienced greater psychological distress than heterosexual adults. This may be related to sexual orientation stigma and discrimination, which increases psychological distress and reduces access to resources and supports. Evidence shows that LGBTQ people, for example, who have access to spaces that affirm their sexual orientation and gender identity report better mental health. In fact, research shows that at the state-level, LGBTQ protective policy is associated with better health outcomes for LGBTQ people. Policy can support structural interventions to reduce stigma, such as legal protections for LGBTQ people in workplace settings, health care, and in schools.
Given the high rates of alcohol and drug use problems among the LGB population, it is not surprising that LGB individuals also use substance use disorder treatment services at higher rates than heterosexual people. However, LGB individuals also report more barriers to treatment compared to heterosexual individuals, including limited availability of LGB-affirming treatment programs and fear of experiencing discrimination, stigma, harassment, or being misunderstood when trying to access treatment. So, although LGB adults with alcohol or drug use problems utilize treatment services at higher rates, many LGB adults also delay seeking needed treatment.
Research on the experiences of people who have resolved an alcohol or drug use problem is an emerging area, covering all pathways to change including treatment-seeking individuals. By learning more about how LGB individuals in recovery compare to their heterosexual counterparts on mental health histories, services used, recovery pathways followed, quality of life, and psychological functioning, researchers can help inform and enhance services to better meet the treatment, recovery support service, and public health policy, needs of LGB individuals.
This study reports on the prevalence of LGB adults who have resolved an alcohol or drug use problem in the U.S. Additionally, the researchers compared LGB and heterosexual adults on demographics, clinical characteristics, pathways to recovery, and indicators of psychosocial functioning and well-being, as well as tested which factors might explain any observed disparities between LGB and heterosexual individuals.
Given the high rates of alcohol and drug use problems among the LGB population, it is not surprising that LGB individuals also use substance use disorder treatment services at higher rates than heterosexual people. However, LGB individuals also report more barriers to treatment compared to heterosexual individuals, including limited availability of LGB-affirming treatment programs and fear of experiencing discrimination, stigma, harassment, or being misunderstood when trying to access treatment. So, although LGB adults with alcohol or drug use problems utilize treatment services at higher rates, many LGB adults also delay seeking needed treatment.
Research on the experiences of people who have resolved an alcohol or drug use problem is an emerging area, covering all pathways to change including treatment-seeking individuals. By learning more about how LGB individuals in recovery compare to their heterosexual counterparts on mental health histories, services used, recovery pathways followed, quality of life, and psychological functioning, researchers can help inform and enhance services to better meet the treatment, recovery support service, and public health policy, needs of LGB individuals.
This study reports on the prevalence of LGB adults who have resolved an alcohol or drug use problem in the U.S. Additionally, the researchers compared LGB and heterosexual adults on demographics, clinical characteristics, pathways to recovery, and indicators of psychosocial functioning and well-being, as well as tested which factors might explain any observed disparities between LGB and heterosexual individuals.
HOW WAS THIS STUDY CONDUCTED?
This study is a secondary analysis from the National RecoveryStudy which surveyed a nationally representative sample of adults in the U.S. who responded “yes” to the question, “Did you used to have a problem with drugs or alcohol, but no longer do?” The researchers examined: a) the number of people in the study who identified as lesbian, gay, or bisexual (LGB); b) if LGB participants in the study differed from heterosexual participants on demographics, clinical histories, and indicators of well-being; c) what factors could explain differences in well-being between LGB and heterosexual participants.
Participants in this study were recruited using an online survey response pool company that helps researchers gain access to nationally representative samples. A nationally representative group of 39,809 individuals were sent a screening question via email, to which 25,229 responded (63.4%). Of those who responded, 2,002 indicated they had resolved an alcohol or drug use problem.
Participants were asked to report their sexual orientation with response options: “heterosexual or straight,” “gay or lesbian,” “bisexual,” or “something else.” Participants were grouped as LGB if they selected, gay, lesbian, bisexual, or something else. Of the LGB adults in the sample, 17 selected “something else” other than heterosexual or lesbian, gay, or bisexual and were included in the LGB group.
Participants also were assessed on their prior substance use histories and substance use and mental health treatment and recovery support services utilization, length of recovery, lifetime co-occurring psychiatric diagnoses, their current functioning, quality of life, their degree of comfort in disclosing their substance use histories to other people, a number of indices of well-being, criminal justice history, and several other factors.
The analyses compared the distribution of demographics, clinical characteristics, alcohol and drug use history, problem resolution pathway, and disclosure comfort between LGB and heterosexual participants in the sample. Second, the researchers examined the association between LGB identity and indicators of well-being (i.e., quality of life, psychological distress, happiness, self-esteem, recovery capital). The researchers then examined which of these demographic, clinical, and recovery-related variables on which LGB were different from heterosexual participants might explain differences in well-being outcomes.
Participants were on average middle-aged (LGB average = 44 years old; heterosexual average = 47 years old). About one third were female (LGB group, 35% female; heterosexual group, 40% female). In terms of race and ethnicity, a little more than half of participants were White/non-Hispanic (LGB group, 56%; heterosexual group, 62%), 14% were Black/non-Hispanic (LGB group, 13%; heterosexual group, 14%), and about 17% were Hispanic (LGB group, 18%; heterosexual group, 17%). There were no differences in age, gender, or race/ethnicity between the LGB and heterosexual groups.
WHAT DID THIS STUDY FIND?
LGB adults represent a large proportion of adults in recovery but face more challenges.
LGB participants were almost half as likely to employed than heterosexual participants. LGB participants were 1.5 times more likely to have an arrest history compared to heterosexual participants. LGB and heterosexual participants did not differ on other sociodemographic variables. There were no differences in age, gender, race/ethnicity, household income, or education.
LGB participants were more than 2 times as likely to have a lifetime history of a co-occurring psychiatric diagnosis than heterosexual participants. LGB participants also had a 2.5-times greater odds of reporting opioids as their primary substance compared to heterosexual participants. LGB participants also had fewer years in recovery, on average, 3 fewer than heterosexual participants. There were no differences between LGB and heterosexual participants across other substances, prior inpatient or outpatient treatment history, number of serious quit attempts, disclosure comfort, and age of onset of regular substance use.
LGB participants reported lower quality of life, happiness, self-esteem, recovery capital, and higher levels of psychological distress overall.
LGB participants had lower quality of life, happiness, self-esteem, recovery capital, and higher levels of psychological distress compared to heterosexual participants.
Differences in quality of life, happiness, self-esteem, and recovery capital were no longer present, though, after controlling for employment, time in recovery, arrest history, primary substance, and co-occurring psychiatric diagnoses. In follow-up analyses, the researchers found that higher rates of co-occurring psychiatric diagnoses accounted for most of the differences in well-being outcomes between LGB and heterosexual participants. This suggests that co-occurring psychiatric diagnoses might be a more major factor in helping to explain disparities between LGB and heterosexual participants in functioning and well-being. However, even when accounting for these differences in psychiatric status, LGB participants still had higher levels of psychological distress compared to heterosexual participants, meaning that there are other reasons not accounted for in these analyses that are contributing to this greater psychological distress among LGB individuals in recovery.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Despite a lack of LGB-affirming recovery services, a high proportion of LGB adults are finding pathways to recovery. It is notable that LGB participants differed from heterosexual participants on a few demographic and clinical history characteristics, including employment, arrest history, years in recovery, primary substance (i.e., opioids), and co-occurring psychiatric diagnoses. Some of these differences, in particular employment, criminal legal system history, and years in recovery may represent downstream effects of structural-level sexual-orientation stigma and discrimination, as structural forms of stigma could affect a person’s socioeconomic status and access to resources. There is also evidence of bias in the diagnosis of certain psychiatric conditions among the LGB population, which could be another form structural or institutional-level stigma. Specifically, LGB individuals are diagnosed with borderline personality disorder at disproportionately high rates, even when controlling for known clinical factors associated with borderline personality disorder (age, gender, comorbid posttraumatic stress disorder, maladaptive personality domains). This suggests that clinicians may be predisposed to provide a borderline personality disorder diagnosis to LGB patients, either through measurement bias or bias among clinicians themselves, that is independent of presenting psychopathology. These kinds of systematic differences in the way LGB individuals are treated suggest how stigma may be being enacted on an institutional or systems level to create disparities, and could affect variables measured in the current study, such as the rates of co-occurring psychiatric disorders reported among LGB participants.
LGB participants also reported lower quality of life, self-esteem, happiness, recovery capital, and psychological distress. These were partially explained by the differences noted above in employment, years in recovery, primary substance, arrest history, and co-occurring psychiatric diagnoses, suggesting that poorer quality of life and well-being indices among the LGB group are in part due to their lack of socioeconomic resources and worse clinical histories.
Of note, when controlling for these socioeconomic and clinical history factors (e.g., psychiatric comorbidity), LGB participants still had higher psychological distress than heterosexual participants indicating that other factors not captured in this study are contributing to this elevated stress. One possibility is that LGB individuals continue to suffer discrimination more than heterosexuals because of their more stigmatized sexual minority status. This in turn can perpetuate psychological distress. This perhaps may also be in the form of trauma, as LGB individuals experience elevated rates of physical and sexual assault, harassment, bullying, and hate crime throughout childhood, adolescence, and adulthood. Such violence, trauma, and discrimination has been associated with substance use problems, depression, and suicide among LGB individuals, and likely contributes to health disparities in this population. Future research should examine the role of structural/institutional, interpersonal, and individual forms of stigma on recovery pathways and well-being.
More research is needed to understand differences in opioids as a primary substance among LGB and heterosexual adults in recovery. Perhaps differences in actual or perceived substance use norms among the LGB community would increase the likelihood of those whose primary substance is opioids to seek recovery, rather than those whose primary substance is, for example, alcohol or cannabis. However, this is purely speculation and more research is needed in this area to examine community norms of substance use across specific types of substances. It is also notable that LGB participants had fewer years in recovery than heterosexual participants. This may represent a more turbulent recovery journey that may result in challenges in staying in recovery; and/or decreased access to effective resources for LGB individuals. Future research should ask LGB adults with alcohol or other drug use problems their desires and preferences for recovery-oriented services.
The researchers did not include measures that assess participants’ experiences of discrimination on individual, interpersonal, or structural-levels, which may affect LGB individual’s well-being in recovery. Future research should include more in-depth assessments of sexual identity-specific stigma to measure how this affects pathways to recovery.
LGB participants in this study were grouped together and were not separated by sexual orientation (e.g., lesbian, gay, bisexual). Examining these groups separately is important for future research, as the experiences of lesbian, gay and bisexual individuals in recovery may differ. For example, in a study on treatment utilization, bisexual individuals used mutual help meetings and professional treatment services 2-5 times more than heterosexual individuals. If LGB participants had been grouped together in that study, the researchers may not have seen that bisexual individuals were primarily driving the effect.
This study is cross-sectional, meaning that researchers don’t know when certain factors happened over time and cannot say that one factor caused another. For example, many participants in this study started their recovery journey at various points over the last 40 years and it is possible that more recent legal protections for LGB people (e.g., marriage equality) may affect LGB individuals’ recovery journeys differently. Future research should assess participants over time so they can track changes in access to supports and more confidently say one factor likely caused another.
BOTTOM LINE
In the U.S., 11.7% of adults in recovery identify as lesbian, gay, or bisexual (LGB). LGB adults in recovery were less likely to be employed, had fewer years in recovery, and were more likely to have an arrest history, report opioids as their primary substance, and have a co-occurring psychiatric diagnosis compared to their heterosexual counterparts. Even after accounting for differences in demographic and clinical/legal histories among LGB and heterosexual groups, LGB adults in recovery still had greater psychological distress.
For individuals and families seeking recovery: A high proportion of LGB people experience alcohol and drug use problems and also are in recovery. Even when accounting for socioeconomic and recovery pathway differences, LGB adults experienced greater psychological distress than heterosexual adults. This may be related to sexual orientation stigma and discrimination, which increases psychological distress and reduces access to resources and supports. Evidence shows that LGBTQ people who have access to spaces that affirm their sexual orientation and gender identity report better mental health. If families can support their LGB loved ones by providing an affirming and accepting space of their sexual and gender identity, this may reduce psychological distress for LGB people with alcohol or drug use problems. Learn more about resources for family members of people who are LGBTQ here.
For treatment professionals and treatment systems: A high proportion of LGB people experience alcohol and drug use problems and are also in recovery. Even when accounting for socioeconomic and recovery pathway differences, LGB adults experienced greater psychological distress than heterosexual adults. This may be related to sexual orientation stigma and discrimination, which increases psychological distress and reduces access to resources and supports. Evidence shows that LGBTQ people who have access to spaces that affirm their sexual orientation and gender identity report better mental health. If treatment providers can offer LGBTQ-affirming care or make their treatment settings affirming, it may improve their LGB patients’ mental health. Providers can obtain additional training on LGBTQ affirming treatment practices here.
For scientists:Findings from this secondary analysis of the National Recovery Study found that 11.7% of adults in recovery identify as lesbian, gay, or bisexual. Survey weight adjusted regression models showed LGB participants were less likely to be employed, more likely to have an arrest history, had fewer years since substance use problem resolution, were more likely to report opioids as their primary substance, and were more likely to report co-occurring psychiatric diagnoses. In unadjusted models, LGB participants reported lower quality of life, happiness, self-esteem, recovery capital, and higher levels of psychological distress. When controlling for group differences in demographic and clinical/legal histories described above, there were no longer significant differences between LGB and heterosexual participants on quality of life, happiness, self-esteem, and recovery capital; however, LGB participants still had significantly higher levels of psychological distress. This suggests that while controlling for structural-level factors like socioeconomic status, and clinical/legal histories and pathways to recovery, other factors could still be influencing psychological distress among LGB adults in recovery. Future studies should examine other factors that could be influencing psychological distress among LGB people longitudinally, such as stigma and discrimination on structural, interpersonal, and individual levels. At the same time, research should also focus on developing and testing clinical and public health approaches to remedy these inequities.
For policy makers: A high proportion of LGB people experience alcohol and drug use problems and are also in recovery. Even when accounting for socioeconomic and recovery pathway differences, LGB adults experienced greater psychological distress than heterosexual adults. This may be related to sexual orientation stigma and discrimination, which increases psychological distress and reduces access to resources and supports. Evidence shows that LGBTQ people, for example, who have access to spaces that affirm their sexual orientation and gender identity report better mental health. In fact, research shows that at the state-level, LGBTQ protective policy is associated with better health outcomes for LGBTQ people. Policy can support structural interventions to reduce stigma, such as legal protections for LGBTQ people in workplace settings, health care, and in schools.