In-person versus online meetings: Which are better?
In light of the increased use of online mutual-help group meetings during and after COVID-19, a pressing question remains: are online meetings as helpful as in-person meetings for supporting recovery? This study examined how the two types were associated with participation patterns and alcohol outcomes.
Mutual-help groups (e.g., Alcoholics Anonymous, SMART Recovery) are the most widelyused recovery support options for alcohol use disorder. Research consistently shows that in-person mutual-help group participation promotes improved alcohol-related outcomes (e.g., increased abstinence, decreased alcohol-related consequences). Mutual-help group meetings have increasingly been implemented in online settings, with their overall engagement receiving a rapid uptake during and after social distancing restrictions associated with COVID-19, which limited access to in-person services. While many are participating in online mutual-help groups, little is known about whether this participation is helpful, and to what degree, when compared to in-person options. This study sought to address this knowledge gap by examining whether different types of attendance (in-person only meeting attendance, online only meeting attendance, both in-person and online meeting attendance) were associated with mutual-help group participation (number of meetings attended, level of involvement) and alcohol outcomes (alcohol abstinence, heavy drinking, and alcohol-related problems).
HOW WAS THIS STUDY CONDUCTED?
This was a naturalistic, longitudinal secondary data analysis from the Peer Alternatives for Addiction Study 2021 cohort. All participants (n = 531) were adults, had a lifetime diagnosis of alcohol use disorder (endorsed >2 DSM-5 criteria over the course of one’s life – not necessarily within a given year – measured using the Composite International Diagnostic Interview), and attended at least 1 in-person or online mutual-help group alternative to 12-step groups (i.e., Women for Sobriety, LifeRing Secular Recovery, SMART Recovery) in the previous 30 days at baseline. They were recruited from October to December 2021. Follow-up assessments were administered at 6- and 12-months after baseline.
Measures for mutual-help group participation were assessed at baseline and follow-ups and accounted for the number of in-person and online meetings attended in the prior 30 days. This measure was used to categorize participants as having attended in-person only, online only, or both in-person and online meetings. Total meeting attendance was also calculated and dichotomized into either having attended 8 or more meetings or less than 8 meetings in the prior 30 days.
Past 30-day mutual-help group involvement was also assessed at each time point and operationalized using 8 binary (yes/no) items. Four out of the 8 items were adapted from the Alcoholics Anonymous Affiliation Scale. These items asked about whether the respondent had a regular or “home” group, whether they had a close friend or “sponsor” they could rely on for help, whether they had any leadership roles in a meeting over the previous 30 days, and whether they had done any volunteer work at a meeting during the same time period. The remaining 4 mutual-help group involvement items were developed by the researchers to account for both online and in-person meetings, capturing whether participants, in the past 30 days, shared openly during a meeting, met in-person with other group members outside of the meeting, exchanged one-on-one mobile communications with another group member, and spent time socializing with other group members before and after meetings. Alcohol outcomes were assessed at all timepoints and included self-reported alcohol abstinence (past 6 months), heavy drinking (number of days during the past month consumed 4 or more drinks for women or 5 or more drinks for men), and 1+ alcohol problems (from a possible 5 items from the Short Index of Alcohol Problems; e.g., failed to meet expectations because of drinking).
For the analysis, the researchers first determined whether there were differences in participants’ demographics (age, race/ethnicity, marital status, education, employment status, annual household income, and urbanicity) and clinical characteristics (alcohol use disorder severity, lifetime drug use problems) at baseline associated with mutual-help group participation mode (online only, in-person only, both in-person and online). They then controlled for differences in baseline characteristics by mutual-help group participation mode in subsequent analyses, in which they examined associations between participation mode and mutual-help group participation and alcohol use outcomes. This approach was used to ensure that any differences in outcomes were more likely to be due to type of mutual-help group participation, rather than any differences in participants’ characteristics that were already present at baseline.
Two-thirds of the sample were female, while 84% were White, 6% Black, and 9% identified a race/ethnicity other than White or Black. On average, participants were 48 years old. Over the course of their lifetime, participants met an average of 10 (of 11) alcohol use disorder criteria; 52% had an alcohol use goal of abstinence. Their primary mutual-help group was well distributed across 12-step (20%), LifeRing (26%), SMART (30%), and Women for Sobriety (25%).
WHAT DID THIS STUDY FIND?
Online attendance was more common than in-person attendance, attendance mode associated with recovery goals
Most (87.4%) participants endorsed at least some online meeting attendance during the 30 days before entering the study. More than half (53.7%) indicated they had only attended online meetings, and about 1 in 3 (33.7%) had attended both online and in-person meetings during this time period. Almost half of participants (46.3%) had attended at least 1 in-person meeting in the last 30 days, but only slightly more than 1 in 10 (12.6%) had attended only in-person meetings. Participants who attended both online and in-person meetings were younger and more likely to be in the lowest income category compared to participants who endorsed either in-person only or online only attendance. Online only attendees were more likely to have a graduate degree. Alcohol use disorder severity and drug use problems were highest among participants who attended both in-person and online meetings and lowest among those who attended only online meetings. Additionally, those who only attended in-person only were more likely to report an alcohol recovery goal of lifetime abstinence than those who attended online only or a combination of online and in-person meetings.
Online meeting attendees (online only, both in-person and online) attended more meetings, but had lower active involvement
After controlling for covariates, those who attended both in-person and online meetings were over 4 times more likely to have attended 8+ meetings in the prior 30 days compared to those who attended only in-person meetings. Online only meeting attendees were also more than 1.5 times as likely to have attended 8+ meetings in the last 30 days compared to in-person only attendees. However, individuals who attended only online meetings were less involved in mutual-help groups – e.g., having a sponsor/close friend to rely on, verbally sharing during a meeting, etc.
Online and in-person meeting attendance produced comparable benefit
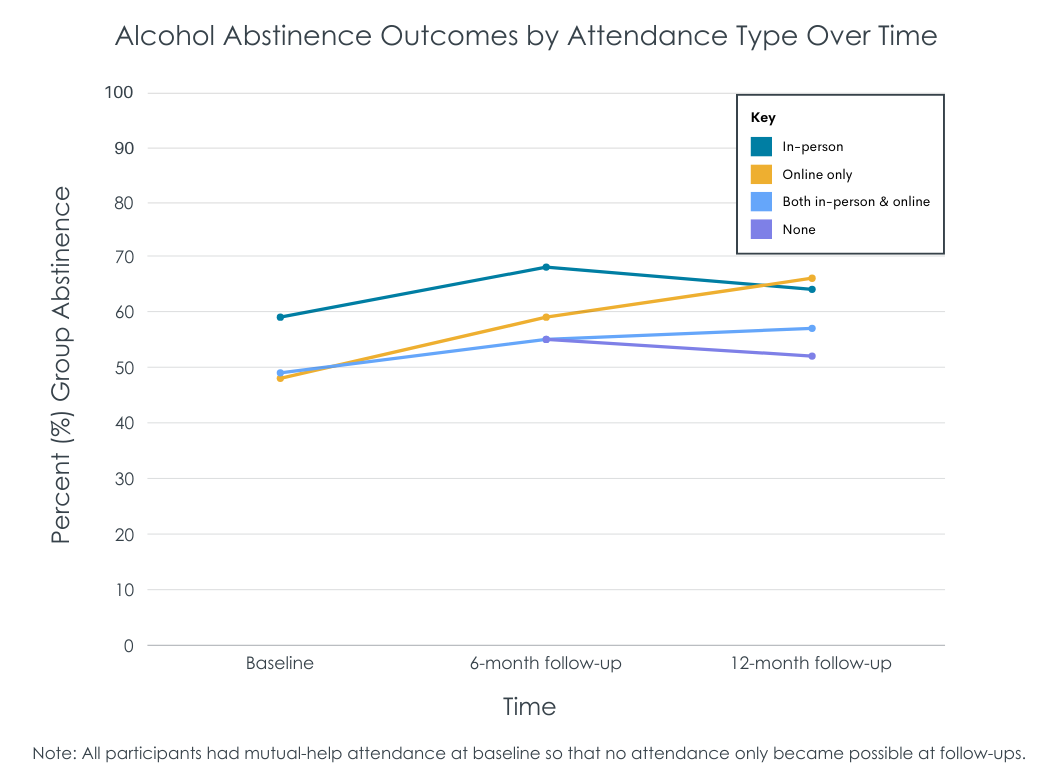
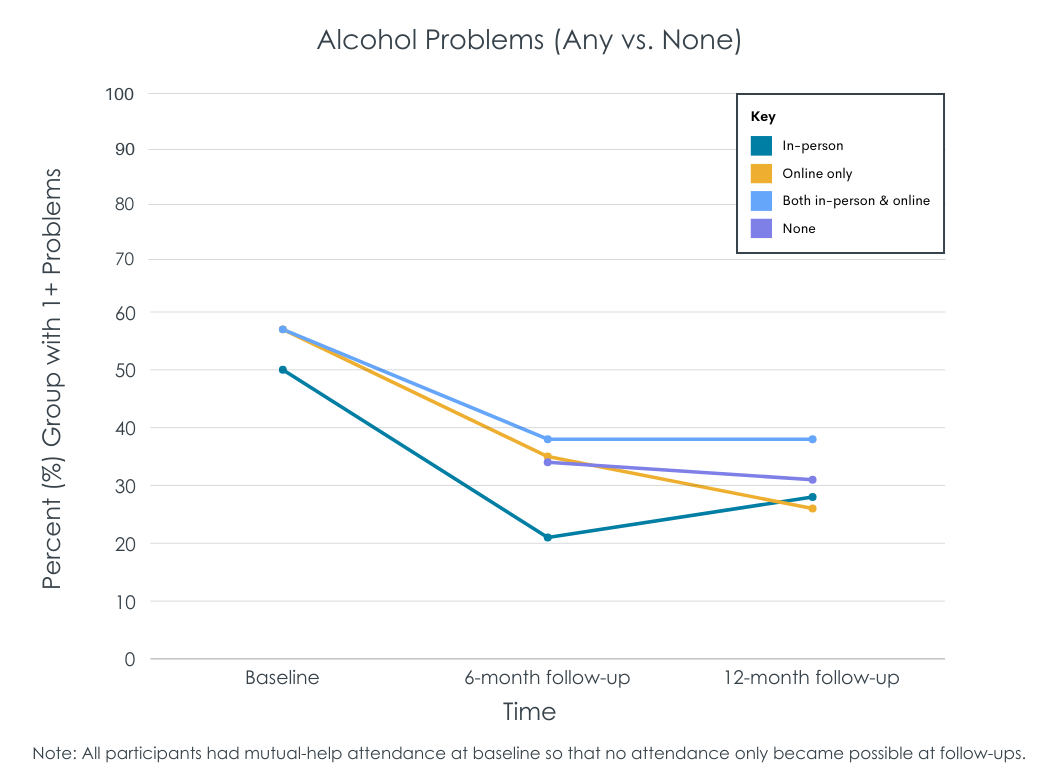
After controlling for covariates, alcohol outcomes improved from baseline to 6-month follow-up and baseline to 12-month follow-up, such that any form of mutual-help group participation was associated with increased odds of alcohol abstinence, decreased odds of heavy drinking, and decreased odds of 1+ alcohol problem. There were no significant differences in alcohol outcome across mutual-help group attendance modes. Those who stopped attending meetings (i.e., all individuals were attending meetings at baseline given the inclusion criteria) had more than twice as many heavy drinking days as in-person only meeting attendees.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Findings from this study of mutual-help attendees with lifetime alcohol use disorder suggest that attending mutual-help group meetings, whether online, in-person, or both, is associated with improved alcohol use outcomes up to 1 year later and highlights the importance of continued engagement in mutual-help groups, regardless of the meeting format.
This study found that online meeting attendance (either alone or in combination with in-person attendance) is associated with a higher likelihood of frequent meeting attendance (8 or more meetings in the last 30 days). This is in line with recent findings from a sample of participants in online Narcotics Anonymous meetings who attended an average of almost 15 online meetings per month and who largely perceived online meeting attendance as comfortable, convenient, and supportive of abstinence. Prior research has demonstrated that mutual-help attendance, especially in Alcoholics Anonymous, and clinical treatments that actively link patients with these community-based meetings, improve alcohol use and other recovery outcomes. While online meeting formats may increase accessibility, especially for those facing barriers to in-person meeting attendance, participants in this study who attended only online meetings were less involved (e.g., leading a meeting, volunteering, meeting with other group members outside of meetings) than in-person attendees. Importantly, mutual-help group involvement is a strong predictor of better alcohol-related outcomes even after accounting for meeting attendance (see here and here, for example). Developing and testing ways to enhance mutual help-group involvement among online meeting attendees may help to enhance alcohol-related outcomes for those who are not engaged with in-person mutual-help groups.
Finally, participants who attended online meetings alone or in combination with in-person meetings were less likely to endorse a recovery goal of lifetime abstinence compared to those who attended only in-person meetings. In fact, more than 2/3 of online only meeting attendees did not wish to abstain from alcohol entirely. This suggests that individuals who intend to reduce their drinking without quitting altogether may feel more comfortable engaging with online meetings. The lower levels of effort needed to attend may also be a good fit for those who are contemplating, but not quite ready, to change their drinking. Moving forward, it will be crucial to provide and evaluate a variety of online and in-person options to support individuals affected by alcohol use disorder who prefer a moderation goal, to comprehensively address prodigious, widespread harms associated with alcohol use.
As noted in the study, sample selection biases cannot be ruled out, meaning the findings may not be generalizable to broader populations of mutual-help group participants. For example, given that recruitment and surveys were administered online, it may be that the participants were already more knowledgeable about or comfortable with using online mutual help-group meetings compared to the general population of mutual help-group attendees.
This study relies on self-report data, which can introduce bias. For example, in line with social desirability bias, it is possible that participants underreported alcohol use and problems at 6- and 12-month follow-ups.
Outcomes were dichotomous (e.g., abstinence, any heavy drinking, any alcohol use problem). Future research should also examine online (vs. in-person) attendance effects on continuous measures, which may be more sensitive to change over time.
BOTTOM LINE
For individuals in or seeking recovery from alcohol use disorder, both online and in-person mutual-help group meetings are associated with improved alcohol use outcomes including abstinence, less heavy drinking, and fewer alcohol problems. Participants who attended online meetings (either exclusively or in combination with in-person meetings) went to more meetings but were generally less involved with their respective mutual-help groups (e.g., leading meetings, volunteering, meeting with other group members outside of meetings). Regardless of the mode of mutual-help group participation, alcohol-related outcomes similarly improved from baseline to 6- and 12-month follow-ups. Online meetings – both on their own and as adjuncts to in-person meetings – may increase accessibility and help to support recovery. However, more research is needed to explore the long-term effects of online mutual-help group meeting participation, understand the mechanisms through which online meeting participation may provide benefits, and determine whether standalone or hybrid combinations of in-person and online attendance are most beneficial and for whom. For people with alcohol use disorder who have never been to mutual-help groups before but are starting a recovery attempt, in-person options might be optimal to build connection and support, as they allow for conversations before and after the meeting where informal discourse can occur that can allow for exchange of contact information for supportive phone/text contact between the more formal meetings. On the other hand, for more initially ambivalent and/or anxious new recoverees, online options may allow people to “try out” and ease into mutual-help options without too much investment in time or resources before immersing themselves in in-person options.
For individuals and families seeking recovery: Participation in either in-person or online mutual-help groups or both can support alcohol use disorder recovery. For those facing barriers to attending in-person offerings (e.g., stigma, personal and family obligations like work or childcare) or simply looking to supplement in-person attendance, online meetings may provide a viable option. However, in-person meeting attendance may offer additional means through which to become more highly involved (e.g., leadership, volunteering, meeting with other group members outside of meetings), which is a strong predictor of positive outcomes. Despite format of meeting attendance, maintaining regular attendance over time is of high importance.
For treatment professionals and treatment systems: Treatment programs and professionals can encourage their patients to engage in mutual-help group options (in-person, online, both) that best fit their lifestyle and preferences. In-person options may be more suitable for those who endorse an abstinence goal and who would like to become more highly involved in groups (e.g., leading groups, volunteering, meeting with other group members outside of meetings). Both abstinence and higher involvementin mutual-help groups are associated with better outcomes. Online meetings may be more accessible to some individuals and may be preferred by those who have a drinking moderation goal.
For scientists: Though this study is a step forward in demonstrating that online mutual-help group meeting attendance can support recovery from alcohol use disorder, further research evaluating the long-term effectiveness of online mutual-help group meeting participation is warranted. There is also a need to explore and test ways for enhancing involvement among online meeting participants, as in-person only attendees tended to be more highly involved. Online meeting participation presents a lower threshold and potentially preferred option for those with a desire to cut down on their drinking but who do not wish to abstain entirely. For these individuals, online meeting attendance may serve as a “stepping stone” to later in-person attendance, greater involvement, and eventual adoption of an abstinence goal; however, research has yet to determine if this is the case. Finally, it is not yet known if online mutual-help group meetings confer benefits to participants through the same mechanisms as in-person options (e.g., adaptive social network changes). Though online offerings have been theorized to confer benefits to participants in a similar manner to in-person meeting participation, results from this study indicated in-person attendees tended to be more highly involved (e.g., leading meetings, volunteering, meeting with other group members outside of meetings) than online only attendees. It is possible that while there may be shared mechanisms through which in-person and online meeting attendance is associated with beneficial outcomes, there may be distinct mechanisms for each of these types of meetings, which may prove more or less useful to certain individuals. Also, for people with alcohol use disorder who have never been to mutual-help groups before but are starting a new alcohol use disorder recovery attempt, in-person options might be optimal to build connection and support as they allow for conversations before and after the meeting where informal discourse can occur that can allow for exchange of contact information for supportive phone/text contact between the more formal meetings. On the other hand, for more initially ambivalent and/or anxious new recoverees, online options may allow people to “try out” and ease into mutual-help options without too much investment in time or resources before immersing themselves in in-person options. Research should examine these possibilities.
For policy makers: Findings from this study suggest online recovery supports, such as online mutual-help group meetings, can be effective for helping people to quit or cut down on their drinking. However, research on the topic is still in its infancy and aforementioned online recovery supports have yet to be clinically tested for their efficacy. Increased funding for rigorously designed longitudinal studies (e.g., randomized clinical trials) could help to build a robust body of evidence on the clinical effectiveness of various combinations of online offerings, their mechanisms of action, and for whom these options may be best suited.
Mutual-help groups (e.g., Alcoholics Anonymous, SMART Recovery) are the most widelyused recovery support options for alcohol use disorder. Research consistently shows that in-person mutual-help group participation promotes improved alcohol-related outcomes (e.g., increased abstinence, decreased alcohol-related consequences). Mutual-help group meetings have increasingly been implemented in online settings, with their overall engagement receiving a rapid uptake during and after social distancing restrictions associated with COVID-19, which limited access to in-person services. While many are participating in online mutual-help groups, little is known about whether this participation is helpful, and to what degree, when compared to in-person options. This study sought to address this knowledge gap by examining whether different types of attendance (in-person only meeting attendance, online only meeting attendance, both in-person and online meeting attendance) were associated with mutual-help group participation (number of meetings attended, level of involvement) and alcohol outcomes (alcohol abstinence, heavy drinking, and alcohol-related problems).
HOW WAS THIS STUDY CONDUCTED?
This was a naturalistic, longitudinal secondary data analysis from the Peer Alternatives for Addiction Study 2021 cohort. All participants (n = 531) were adults, had a lifetime diagnosis of alcohol use disorder (endorsed >2 DSM-5 criteria over the course of one’s life – not necessarily within a given year – measured using the Composite International Diagnostic Interview), and attended at least 1 in-person or online mutual-help group alternative to 12-step groups (i.e., Women for Sobriety, LifeRing Secular Recovery, SMART Recovery) in the previous 30 days at baseline. They were recruited from October to December 2021. Follow-up assessments were administered at 6- and 12-months after baseline.
Measures for mutual-help group participation were assessed at baseline and follow-ups and accounted for the number of in-person and online meetings attended in the prior 30 days. This measure was used to categorize participants as having attended in-person only, online only, or both in-person and online meetings. Total meeting attendance was also calculated and dichotomized into either having attended 8 or more meetings or less than 8 meetings in the prior 30 days.
Past 30-day mutual-help group involvement was also assessed at each time point and operationalized using 8 binary (yes/no) items. Four out of the 8 items were adapted from the Alcoholics Anonymous Affiliation Scale. These items asked about whether the respondent had a regular or “home” group, whether they had a close friend or “sponsor” they could rely on for help, whether they had any leadership roles in a meeting over the previous 30 days, and whether they had done any volunteer work at a meeting during the same time period. The remaining 4 mutual-help group involvement items were developed by the researchers to account for both online and in-person meetings, capturing whether participants, in the past 30 days, shared openly during a meeting, met in-person with other group members outside of the meeting, exchanged one-on-one mobile communications with another group member, and spent time socializing with other group members before and after meetings. Alcohol outcomes were assessed at all timepoints and included self-reported alcohol abstinence (past 6 months), heavy drinking (number of days during the past month consumed 4 or more drinks for women or 5 or more drinks for men), and 1+ alcohol problems (from a possible 5 items from the Short Index of Alcohol Problems; e.g., failed to meet expectations because of drinking).
For the analysis, the researchers first determined whether there were differences in participants’ demographics (age, race/ethnicity, marital status, education, employment status, annual household income, and urbanicity) and clinical characteristics (alcohol use disorder severity, lifetime drug use problems) at baseline associated with mutual-help group participation mode (online only, in-person only, both in-person and online). They then controlled for differences in baseline characteristics by mutual-help group participation mode in subsequent analyses, in which they examined associations between participation mode and mutual-help group participation and alcohol use outcomes. This approach was used to ensure that any differences in outcomes were more likely to be due to type of mutual-help group participation, rather than any differences in participants’ characteristics that were already present at baseline.
Two-thirds of the sample were female, while 84% were White, 6% Black, and 9% identified a race/ethnicity other than White or Black. On average, participants were 48 years old. Over the course of their lifetime, participants met an average of 10 (of 11) alcohol use disorder criteria; 52% had an alcohol use goal of abstinence. Their primary mutual-help group was well distributed across 12-step (20%), LifeRing (26%), SMART (30%), and Women for Sobriety (25%).
WHAT DID THIS STUDY FIND?
Online attendance was more common than in-person attendance, attendance mode associated with recovery goals
Most (87.4%) participants endorsed at least some online meeting attendance during the 30 days before entering the study. More than half (53.7%) indicated they had only attended online meetings, and about 1 in 3 (33.7%) had attended both online and in-person meetings during this time period. Almost half of participants (46.3%) had attended at least 1 in-person meeting in the last 30 days, but only slightly more than 1 in 10 (12.6%) had attended only in-person meetings. Participants who attended both online and in-person meetings were younger and more likely to be in the lowest income category compared to participants who endorsed either in-person only or online only attendance. Online only attendees were more likely to have a graduate degree. Alcohol use disorder severity and drug use problems were highest among participants who attended both in-person and online meetings and lowest among those who attended only online meetings. Additionally, those who only attended in-person only were more likely to report an alcohol recovery goal of lifetime abstinence than those who attended online only or a combination of online and in-person meetings.
Online meeting attendees (online only, both in-person and online) attended more meetings, but had lower active involvement
After controlling for covariates, those who attended both in-person and online meetings were over 4 times more likely to have attended 8+ meetings in the prior 30 days compared to those who attended only in-person meetings. Online only meeting attendees were also more than 1.5 times as likely to have attended 8+ meetings in the last 30 days compared to in-person only attendees. However, individuals who attended only online meetings were less involved in mutual-help groups – e.g., having a sponsor/close friend to rely on, verbally sharing during a meeting, etc.
Online and in-person meeting attendance produced comparable benefit
After controlling for covariates, alcohol outcomes improved from baseline to 6-month follow-up and baseline to 12-month follow-up, such that any form of mutual-help group participation was associated with increased odds of alcohol abstinence, decreased odds of heavy drinking, and decreased odds of 1+ alcohol problem. There were no significant differences in alcohol outcome across mutual-help group attendance modes. Those who stopped attending meetings (i.e., all individuals were attending meetings at baseline given the inclusion criteria) had more than twice as many heavy drinking days as in-person only meeting attendees.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Findings from this study of mutual-help attendees with lifetime alcohol use disorder suggest that attending mutual-help group meetings, whether online, in-person, or both, is associated with improved alcohol use outcomes up to 1 year later and highlights the importance of continued engagement in mutual-help groups, regardless of the meeting format.
This study found that online meeting attendance (either alone or in combination with in-person attendance) is associated with a higher likelihood of frequent meeting attendance (8 or more meetings in the last 30 days). This is in line with recent findings from a sample of participants in online Narcotics Anonymous meetings who attended an average of almost 15 online meetings per month and who largely perceived online meeting attendance as comfortable, convenient, and supportive of abstinence. Prior research has demonstrated that mutual-help attendance, especially in Alcoholics Anonymous, and clinical treatments that actively link patients with these community-based meetings, improve alcohol use and other recovery outcomes. While online meeting formats may increase accessibility, especially for those facing barriers to in-person meeting attendance, participants in this study who attended only online meetings were less involved (e.g., leading a meeting, volunteering, meeting with other group members outside of meetings) than in-person attendees. Importantly, mutual-help group involvement is a strong predictor of better alcohol-related outcomes even after accounting for meeting attendance (see here and here, for example). Developing and testing ways to enhance mutual help-group involvement among online meeting attendees may help to enhance alcohol-related outcomes for those who are not engaged with in-person mutual-help groups.
Finally, participants who attended online meetings alone or in combination with in-person meetings were less likely to endorse a recovery goal of lifetime abstinence compared to those who attended only in-person meetings. In fact, more than 2/3 of online only meeting attendees did not wish to abstain from alcohol entirely. This suggests that individuals who intend to reduce their drinking without quitting altogether may feel more comfortable engaging with online meetings. The lower levels of effort needed to attend may also be a good fit for those who are contemplating, but not quite ready, to change their drinking. Moving forward, it will be crucial to provide and evaluate a variety of online and in-person options to support individuals affected by alcohol use disorder who prefer a moderation goal, to comprehensively address prodigious, widespread harms associated with alcohol use.
As noted in the study, sample selection biases cannot be ruled out, meaning the findings may not be generalizable to broader populations of mutual-help group participants. For example, given that recruitment and surveys were administered online, it may be that the participants were already more knowledgeable about or comfortable with using online mutual help-group meetings compared to the general population of mutual help-group attendees.
This study relies on self-report data, which can introduce bias. For example, in line with social desirability bias, it is possible that participants underreported alcohol use and problems at 6- and 12-month follow-ups.
Outcomes were dichotomous (e.g., abstinence, any heavy drinking, any alcohol use problem). Future research should also examine online (vs. in-person) attendance effects on continuous measures, which may be more sensitive to change over time.
BOTTOM LINE
For individuals in or seeking recovery from alcohol use disorder, both online and in-person mutual-help group meetings are associated with improved alcohol use outcomes including abstinence, less heavy drinking, and fewer alcohol problems. Participants who attended online meetings (either exclusively or in combination with in-person meetings) went to more meetings but were generally less involved with their respective mutual-help groups (e.g., leading meetings, volunteering, meeting with other group members outside of meetings). Regardless of the mode of mutual-help group participation, alcohol-related outcomes similarly improved from baseline to 6- and 12-month follow-ups. Online meetings – both on their own and as adjuncts to in-person meetings – may increase accessibility and help to support recovery. However, more research is needed to explore the long-term effects of online mutual-help group meeting participation, understand the mechanisms through which online meeting participation may provide benefits, and determine whether standalone or hybrid combinations of in-person and online attendance are most beneficial and for whom. For people with alcohol use disorder who have never been to mutual-help groups before but are starting a recovery attempt, in-person options might be optimal to build connection and support, as they allow for conversations before and after the meeting where informal discourse can occur that can allow for exchange of contact information for supportive phone/text contact between the more formal meetings. On the other hand, for more initially ambivalent and/or anxious new recoverees, online options may allow people to “try out” and ease into mutual-help options without too much investment in time or resources before immersing themselves in in-person options.
For individuals and families seeking recovery: Participation in either in-person or online mutual-help groups or both can support alcohol use disorder recovery. For those facing barriers to attending in-person offerings (e.g., stigma, personal and family obligations like work or childcare) or simply looking to supplement in-person attendance, online meetings may provide a viable option. However, in-person meeting attendance may offer additional means through which to become more highly involved (e.g., leadership, volunteering, meeting with other group members outside of meetings), which is a strong predictor of positive outcomes. Despite format of meeting attendance, maintaining regular attendance over time is of high importance.
For treatment professionals and treatment systems: Treatment programs and professionals can encourage their patients to engage in mutual-help group options (in-person, online, both) that best fit their lifestyle and preferences. In-person options may be more suitable for those who endorse an abstinence goal and who would like to become more highly involved in groups (e.g., leading groups, volunteering, meeting with other group members outside of meetings). Both abstinence and higher involvementin mutual-help groups are associated with better outcomes. Online meetings may be more accessible to some individuals and may be preferred by those who have a drinking moderation goal.
For scientists: Though this study is a step forward in demonstrating that online mutual-help group meeting attendance can support recovery from alcohol use disorder, further research evaluating the long-term effectiveness of online mutual-help group meeting participation is warranted. There is also a need to explore and test ways for enhancing involvement among online meeting participants, as in-person only attendees tended to be more highly involved. Online meeting participation presents a lower threshold and potentially preferred option for those with a desire to cut down on their drinking but who do not wish to abstain entirely. For these individuals, online meeting attendance may serve as a “stepping stone” to later in-person attendance, greater involvement, and eventual adoption of an abstinence goal; however, research has yet to determine if this is the case. Finally, it is not yet known if online mutual-help group meetings confer benefits to participants through the same mechanisms as in-person options (e.g., adaptive social network changes). Though online offerings have been theorized to confer benefits to participants in a similar manner to in-person meeting participation, results from this study indicated in-person attendees tended to be more highly involved (e.g., leading meetings, volunteering, meeting with other group members outside of meetings) than online only attendees. It is possible that while there may be shared mechanisms through which in-person and online meeting attendance is associated with beneficial outcomes, there may be distinct mechanisms for each of these types of meetings, which may prove more or less useful to certain individuals. Also, for people with alcohol use disorder who have never been to mutual-help groups before but are starting a new alcohol use disorder recovery attempt, in-person options might be optimal to build connection and support as they allow for conversations before and after the meeting where informal discourse can occur that can allow for exchange of contact information for supportive phone/text contact between the more formal meetings. On the other hand, for more initially ambivalent and/or anxious new recoverees, online options may allow people to “try out” and ease into mutual-help options without too much investment in time or resources before immersing themselves in in-person options. Research should examine these possibilities.
For policy makers: Findings from this study suggest online recovery supports, such as online mutual-help group meetings, can be effective for helping people to quit or cut down on their drinking. However, research on the topic is still in its infancy and aforementioned online recovery supports have yet to be clinically tested for their efficacy. Increased funding for rigorously designed longitudinal studies (e.g., randomized clinical trials) could help to build a robust body of evidence on the clinical effectiveness of various combinations of online offerings, their mechanisms of action, and for whom these options may be best suited.
Mutual-help groups (e.g., Alcoholics Anonymous, SMART Recovery) are the most widelyused recovery support options for alcohol use disorder. Research consistently shows that in-person mutual-help group participation promotes improved alcohol-related outcomes (e.g., increased abstinence, decreased alcohol-related consequences). Mutual-help group meetings have increasingly been implemented in online settings, with their overall engagement receiving a rapid uptake during and after social distancing restrictions associated with COVID-19, which limited access to in-person services. While many are participating in online mutual-help groups, little is known about whether this participation is helpful, and to what degree, when compared to in-person options. This study sought to address this knowledge gap by examining whether different types of attendance (in-person only meeting attendance, online only meeting attendance, both in-person and online meeting attendance) were associated with mutual-help group participation (number of meetings attended, level of involvement) and alcohol outcomes (alcohol abstinence, heavy drinking, and alcohol-related problems).
HOW WAS THIS STUDY CONDUCTED?
This was a naturalistic, longitudinal secondary data analysis from the Peer Alternatives for Addiction Study 2021 cohort. All participants (n = 531) were adults, had a lifetime diagnosis of alcohol use disorder (endorsed >2 DSM-5 criteria over the course of one’s life – not necessarily within a given year – measured using the Composite International Diagnostic Interview), and attended at least 1 in-person or online mutual-help group alternative to 12-step groups (i.e., Women for Sobriety, LifeRing Secular Recovery, SMART Recovery) in the previous 30 days at baseline. They were recruited from October to December 2021. Follow-up assessments were administered at 6- and 12-months after baseline.
Measures for mutual-help group participation were assessed at baseline and follow-ups and accounted for the number of in-person and online meetings attended in the prior 30 days. This measure was used to categorize participants as having attended in-person only, online only, or both in-person and online meetings. Total meeting attendance was also calculated and dichotomized into either having attended 8 or more meetings or less than 8 meetings in the prior 30 days.
Past 30-day mutual-help group involvement was also assessed at each time point and operationalized using 8 binary (yes/no) items. Four out of the 8 items were adapted from the Alcoholics Anonymous Affiliation Scale. These items asked about whether the respondent had a regular or “home” group, whether they had a close friend or “sponsor” they could rely on for help, whether they had any leadership roles in a meeting over the previous 30 days, and whether they had done any volunteer work at a meeting during the same time period. The remaining 4 mutual-help group involvement items were developed by the researchers to account for both online and in-person meetings, capturing whether participants, in the past 30 days, shared openly during a meeting, met in-person with other group members outside of the meeting, exchanged one-on-one mobile communications with another group member, and spent time socializing with other group members before and after meetings. Alcohol outcomes were assessed at all timepoints and included self-reported alcohol abstinence (past 6 months), heavy drinking (number of days during the past month consumed 4 or more drinks for women or 5 or more drinks for men), and 1+ alcohol problems (from a possible 5 items from the Short Index of Alcohol Problems; e.g., failed to meet expectations because of drinking).
For the analysis, the researchers first determined whether there were differences in participants’ demographics (age, race/ethnicity, marital status, education, employment status, annual household income, and urbanicity) and clinical characteristics (alcohol use disorder severity, lifetime drug use problems) at baseline associated with mutual-help group participation mode (online only, in-person only, both in-person and online). They then controlled for differences in baseline characteristics by mutual-help group participation mode in subsequent analyses, in which they examined associations between participation mode and mutual-help group participation and alcohol use outcomes. This approach was used to ensure that any differences in outcomes were more likely to be due to type of mutual-help group participation, rather than any differences in participants’ characteristics that were already present at baseline.
Two-thirds of the sample were female, while 84% were White, 6% Black, and 9% identified a race/ethnicity other than White or Black. On average, participants were 48 years old. Over the course of their lifetime, participants met an average of 10 (of 11) alcohol use disorder criteria; 52% had an alcohol use goal of abstinence. Their primary mutual-help group was well distributed across 12-step (20%), LifeRing (26%), SMART (30%), and Women for Sobriety (25%).
WHAT DID THIS STUDY FIND?
Online attendance was more common than in-person attendance, attendance mode associated with recovery goals
Most (87.4%) participants endorsed at least some online meeting attendance during the 30 days before entering the study. More than half (53.7%) indicated they had only attended online meetings, and about 1 in 3 (33.7%) had attended both online and in-person meetings during this time period. Almost half of participants (46.3%) had attended at least 1 in-person meeting in the last 30 days, but only slightly more than 1 in 10 (12.6%) had attended only in-person meetings. Participants who attended both online and in-person meetings were younger and more likely to be in the lowest income category compared to participants who endorsed either in-person only or online only attendance. Online only attendees were more likely to have a graduate degree. Alcohol use disorder severity and drug use problems were highest among participants who attended both in-person and online meetings and lowest among those who attended only online meetings. Additionally, those who only attended in-person only were more likely to report an alcohol recovery goal of lifetime abstinence than those who attended online only or a combination of online and in-person meetings.
Online meeting attendees (online only, both in-person and online) attended more meetings, but had lower active involvement
After controlling for covariates, those who attended both in-person and online meetings were over 4 times more likely to have attended 8+ meetings in the prior 30 days compared to those who attended only in-person meetings. Online only meeting attendees were also more than 1.5 times as likely to have attended 8+ meetings in the last 30 days compared to in-person only attendees. However, individuals who attended only online meetings were less involved in mutual-help groups – e.g., having a sponsor/close friend to rely on, verbally sharing during a meeting, etc.
Online and in-person meeting attendance produced comparable benefit
After controlling for covariates, alcohol outcomes improved from baseline to 6-month follow-up and baseline to 12-month follow-up, such that any form of mutual-help group participation was associated with increased odds of alcohol abstinence, decreased odds of heavy drinking, and decreased odds of 1+ alcohol problem. There were no significant differences in alcohol outcome across mutual-help group attendance modes. Those who stopped attending meetings (i.e., all individuals were attending meetings at baseline given the inclusion criteria) had more than twice as many heavy drinking days as in-person only meeting attendees.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Findings from this study of mutual-help attendees with lifetime alcohol use disorder suggest that attending mutual-help group meetings, whether online, in-person, or both, is associated with improved alcohol use outcomes up to 1 year later and highlights the importance of continued engagement in mutual-help groups, regardless of the meeting format.
This study found that online meeting attendance (either alone or in combination with in-person attendance) is associated with a higher likelihood of frequent meeting attendance (8 or more meetings in the last 30 days). This is in line with recent findings from a sample of participants in online Narcotics Anonymous meetings who attended an average of almost 15 online meetings per month and who largely perceived online meeting attendance as comfortable, convenient, and supportive of abstinence. Prior research has demonstrated that mutual-help attendance, especially in Alcoholics Anonymous, and clinical treatments that actively link patients with these community-based meetings, improve alcohol use and other recovery outcomes. While online meeting formats may increase accessibility, especially for those facing barriers to in-person meeting attendance, participants in this study who attended only online meetings were less involved (e.g., leading a meeting, volunteering, meeting with other group members outside of meetings) than in-person attendees. Importantly, mutual-help group involvement is a strong predictor of better alcohol-related outcomes even after accounting for meeting attendance (see here and here, for example). Developing and testing ways to enhance mutual help-group involvement among online meeting attendees may help to enhance alcohol-related outcomes for those who are not engaged with in-person mutual-help groups.
Finally, participants who attended online meetings alone or in combination with in-person meetings were less likely to endorse a recovery goal of lifetime abstinence compared to those who attended only in-person meetings. In fact, more than 2/3 of online only meeting attendees did not wish to abstain from alcohol entirely. This suggests that individuals who intend to reduce their drinking without quitting altogether may feel more comfortable engaging with online meetings. The lower levels of effort needed to attend may also be a good fit for those who are contemplating, but not quite ready, to change their drinking. Moving forward, it will be crucial to provide and evaluate a variety of online and in-person options to support individuals affected by alcohol use disorder who prefer a moderation goal, to comprehensively address prodigious, widespread harms associated with alcohol use.
As noted in the study, sample selection biases cannot be ruled out, meaning the findings may not be generalizable to broader populations of mutual-help group participants. For example, given that recruitment and surveys were administered online, it may be that the participants were already more knowledgeable about or comfortable with using online mutual help-group meetings compared to the general population of mutual help-group attendees.
This study relies on self-report data, which can introduce bias. For example, in line with social desirability bias, it is possible that participants underreported alcohol use and problems at 6- and 12-month follow-ups.
Outcomes were dichotomous (e.g., abstinence, any heavy drinking, any alcohol use problem). Future research should also examine online (vs. in-person) attendance effects on continuous measures, which may be more sensitive to change over time.
BOTTOM LINE
For individuals in or seeking recovery from alcohol use disorder, both online and in-person mutual-help group meetings are associated with improved alcohol use outcomes including abstinence, less heavy drinking, and fewer alcohol problems. Participants who attended online meetings (either exclusively or in combination with in-person meetings) went to more meetings but were generally less involved with their respective mutual-help groups (e.g., leading meetings, volunteering, meeting with other group members outside of meetings). Regardless of the mode of mutual-help group participation, alcohol-related outcomes similarly improved from baseline to 6- and 12-month follow-ups. Online meetings – both on their own and as adjuncts to in-person meetings – may increase accessibility and help to support recovery. However, more research is needed to explore the long-term effects of online mutual-help group meeting participation, understand the mechanisms through which online meeting participation may provide benefits, and determine whether standalone or hybrid combinations of in-person and online attendance are most beneficial and for whom. For people with alcohol use disorder who have never been to mutual-help groups before but are starting a recovery attempt, in-person options might be optimal to build connection and support, as they allow for conversations before and after the meeting where informal discourse can occur that can allow for exchange of contact information for supportive phone/text contact between the more formal meetings. On the other hand, for more initially ambivalent and/or anxious new recoverees, online options may allow people to “try out” and ease into mutual-help options without too much investment in time or resources before immersing themselves in in-person options.
For individuals and families seeking recovery: Participation in either in-person or online mutual-help groups or both can support alcohol use disorder recovery. For those facing barriers to attending in-person offerings (e.g., stigma, personal and family obligations like work or childcare) or simply looking to supplement in-person attendance, online meetings may provide a viable option. However, in-person meeting attendance may offer additional means through which to become more highly involved (e.g., leadership, volunteering, meeting with other group members outside of meetings), which is a strong predictor of positive outcomes. Despite format of meeting attendance, maintaining regular attendance over time is of high importance.
For treatment professionals and treatment systems: Treatment programs and professionals can encourage their patients to engage in mutual-help group options (in-person, online, both) that best fit their lifestyle and preferences. In-person options may be more suitable for those who endorse an abstinence goal and who would like to become more highly involved in groups (e.g., leading groups, volunteering, meeting with other group members outside of meetings). Both abstinence and higher involvementin mutual-help groups are associated with better outcomes. Online meetings may be more accessible to some individuals and may be preferred by those who have a drinking moderation goal.
For scientists: Though this study is a step forward in demonstrating that online mutual-help group meeting attendance can support recovery from alcohol use disorder, further research evaluating the long-term effectiveness of online mutual-help group meeting participation is warranted. There is also a need to explore and test ways for enhancing involvement among online meeting participants, as in-person only attendees tended to be more highly involved. Online meeting participation presents a lower threshold and potentially preferred option for those with a desire to cut down on their drinking but who do not wish to abstain entirely. For these individuals, online meeting attendance may serve as a “stepping stone” to later in-person attendance, greater involvement, and eventual adoption of an abstinence goal; however, research has yet to determine if this is the case. Finally, it is not yet known if online mutual-help group meetings confer benefits to participants through the same mechanisms as in-person options (e.g., adaptive social network changes). Though online offerings have been theorized to confer benefits to participants in a similar manner to in-person meeting participation, results from this study indicated in-person attendees tended to be more highly involved (e.g., leading meetings, volunteering, meeting with other group members outside of meetings) than online only attendees. It is possible that while there may be shared mechanisms through which in-person and online meeting attendance is associated with beneficial outcomes, there may be distinct mechanisms for each of these types of meetings, which may prove more or less useful to certain individuals. Also, for people with alcohol use disorder who have never been to mutual-help groups before but are starting a new alcohol use disorder recovery attempt, in-person options might be optimal to build connection and support as they allow for conversations before and after the meeting where informal discourse can occur that can allow for exchange of contact information for supportive phone/text contact between the more formal meetings. On the other hand, for more initially ambivalent and/or anxious new recoverees, online options may allow people to “try out” and ease into mutual-help options without too much investment in time or resources before immersing themselves in in-person options. Research should examine these possibilities.
For policy makers: Findings from this study suggest online recovery supports, such as online mutual-help group meetings, can be effective for helping people to quit or cut down on their drinking. However, research on the topic is still in its infancy and aforementioned online recovery supports have yet to be clinically tested for their efficacy. Increased funding for rigorously designed longitudinal studies (e.g., randomized clinical trials) could help to build a robust body of evidence on the clinical effectiveness of various combinations of online offerings, their mechanisms of action, and for whom these options may be best suited.