For incarcerated individuals with high-risk drug use, re-incarceration risk increased by heavy alcohol use and mitigated by addiction treatment
Substance use substantially increases the risk for incarceration. To understand what psychosocial and medical factors can be addressed to prevent it, or which types of individuals need additional support post-release, this study examined predictors of reincarceration among individuals with a history of injection drug use or HIV.
For example, they may face discrimination or stigma that gets in the way of finding safe housing or steady work. These are barriers that can increase stress levels, reduce acquisition of coping skills or other necessary resources for daily life, and lead back into substance use and behaviors that initially got them into trouble. This study examined what factors are most likely to contribute to an individual’s reincarceration among individuals who use drugs. By understanding the factors that predict reincarceration, policies and services can be geared to best prevent recidivism in these vulnerable groups of individuals who use drugs.
HOW WAS THIS STUDY CONDUCTED?
This was secondary data analysis using longitudinal data from two cohorts in Vancouver, Canada. The first cohort, the AIDS Care Cohort to Evaluate Exposure to Survival Services (ACCESS), enrolled adults that used any illicit substance other than or in addition to cannabis and are living with HIV. The second cohort, the Vancouver Injection Drug Users Study (VIDUS), enrolled adults who injected drugs and are HIV-negative. In this secondary analysis, participants were included if they were in either cohort from June 2006 to November 2018, reported an incarceration event at any point during the study period, and had one subsequent study visit. A participant’s baseline in this analysis was considered their time of first reported incarceration during the study period. Participants who had not had an interview in the 2 years before the study period end of 2018 were considered lost to follow-up. The total sample across both cohorts was 2350, but only 468 of those experienced incarceration and completed a follow-up visit and are included in this analysis.
The assessments were conducted by trained interviewers with participants at baseline and every 6 months. The assessments covered substance use, sexual experiences, and other things like criminal legal involvement. The primary outcome – reincarceration – was defined as a reincarceration event during the study period in a provincial (i.e., the Canadian equivalent of a US state) prison or federal penitentiary.
The analysis explored the following factors that should not change over time (time invariant) as binary indicators (yes/no) associated with reincarceration: self-identified men (versus women and non-binary gender), ethnicity/ancestry (white vs. Indigenous vs. other), education at baseline (less than high school diploma vs. high school diploma or more), service use in jail during baseline incarceration (e.g., including services such as anger management or substance use), and baseline HIV status. There were also factors included in the models that were updated over time, as appropriate, including age at study visit, HIV status, homelessness, sex work, engagement in community judicial supervision, stimulant use, opioid use, any injection drug use, and heavy alcohol use (defined using the NIAAA 2010 criteria for men and women), self-reported mental illness diagnosis, calendar year of study visit, reincarceration events during the study period (none, one, two or more), and accessing addiction treatment.
Of the 468 participants in this study, the median age was 40 years (75% of the sample was between 34-46 years), 74% were men, and 38% identified as Indigenous. Individuals were reincarcerated between 0 and 11 times with nearly half experiencing at least one reincarceration event.
WHAT DID THIS STUDY FIND?
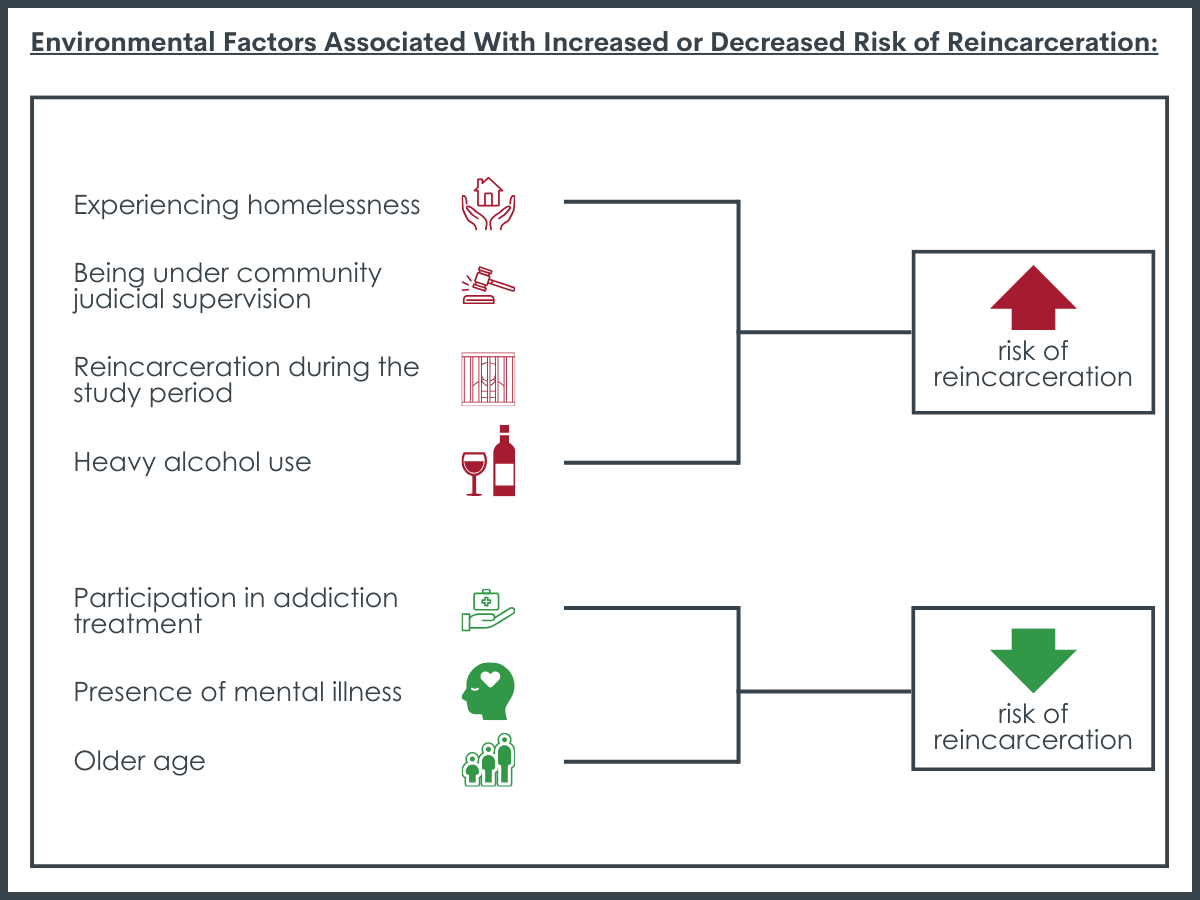
Environmental-level factors were most strongly associated with reincarceration.
In the analysis that adjusted for several factors at once, the presence of 4 factors were more likely to be linked to reincarceration while the presence of 3 other factors were likely to reduce the potential of reincarceration. Experiencing homelessness, being under community judicial supervision, and heavy alcohol use were factors related to an increased risk of reincarceration. Reincarceration during the study period was also associated with increased risk of reincarceration, suggesting that among those who were reincarcerated once, their risk of being incarcerated again increased. Among those factors found to increase one’s risk for reincarceration, being under community judicial supervision presented the greatest risk, nearly double that of the other factors with the exception of homelessness. Yet, participation in addiction treatment, the presence of a mental illness, and older age, were negatively related to reincarceration risk. Among those factors found to decrease one’s risk for reincarceration, being older was the strongest predictor, but was similar in magnitude to the other factors.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study of individuals who used drugs in Canada and had been incarcerated, the odds of being reincarcerated no better than the flip of a coin, suggesting there are a lot of opportunities to make a difference. Importantly, several of the factors implicated in this relationship are areas that communities can address with targeted programming, intervention, and recovery supports.
Experiencing homelessness was linked to increased reincarceration while engagement in addiction treatment was linked to reduced reincarceration. These findings suggest that actively linking individuals leaving jail or prison with stable housing, including recovery-supportive housing such as sober homes, may be an important way to reduce their risk of reincarceration.
Although this study conducted visits with participants whether or not they were incarcerated at the time of the study visit, the researchers were unable to reach some participants. This is a limitation as there may be important differences between those who were available for follow-up study visits and those who could not be reached. For example, individuals who missed study visits were more likely to have been reincarcerated than those who did not miss study visits.
Access to, and use of, treatment and recovery supports after incarceration was not documented in a detailed manner. So, beyond a binary measure of addiction treatment attendance, it is unclear to what degree individuals received any of these supports and how they might have influenced their risk of reincarceration.
BOTTOM LINE
In this study of individuals who used drugs in Canada and had been incarcerated, nearly half were reincarcerated. Several system-level factors were linked to greater odds of reincarceration, including experiencing homelessness, while receiving treatment was linked to reduced odds of reincarceration. These findings suggest that criminal justice efforts – to prevent the additional financial and human costs of reincarceration – should seek to increase access to these key supports for individuals leaving a supervised setting. One key individual-level factor linked to increased reincarceration was heavy alcohol use, suggesting that greater attention be paid to addressing alcohol use among incarcerated populations.
For individuals and families seeking recovery: Individuals who use drugs are also more likely to experience incarceration, and if incarcerated, to experience reincarceration. These individuals are likely to benefit from interventions for re-entry and recovery from treatment professionals and connections to the larger community to build their recovery capital. Addressing basic needs, such as housing, can go a long way in preventing recidivism.
For treatment professionals and treatment systems: Individuals leaving incarceration who also have a history of substance use are likely to benefit from continued support and interventions for re-entry and recovery from treatment professionals to prevent reincarceration. In addition to addressing substance use treatment needs, providers working with these individuals may also assist patients with modifying behaviors that may interfere with successful engagement with re-entry (e.g., motivation, other barriers to participation in treatment, etc.) and through linkage to other community recovery supports.
For scientists: This study identifies some key risks for reincarceration among individuals who use drugs and points to gaps in our understanding of these relationships. Future work that examines trajectories of these individuals, while including factors such as type of substance use, community-recovery support services, and a wider array of individual-, social- and community-level risk and protective factors will help advance the field’s understanding of how best to support individuals leaving prison or jail settings. Because of substantial economic costs of reincarceration, cost-benefit analysis of addressing gaps in recovery capital for individuals’ post-incarceration could help highlight where resources might be better spent (e.g., on providing housing, job training/access, treatment, vs further incarceration costs).
For policy makers: More funding and research to address community re-entry supports after incarceration for individuals with a substance use history can help clarify aspects of programming that are effective and cost-effective and areas where community infrastructure needs additional support. Access to sustainable housing is a key source of stress in the early re-entry days and one that can lead to future incarceration. Funding and research to address these linkages could help support these vital community-based resources. Given that diversion programs, such as drug or recovery courts can also reduce substance use and recidivism, and addiction treatment was a protective factor against reincarceration in this study, ensuring access to these services is likely to have broader benefits for the criminal justice system and society at large.
For example, they may face discrimination or stigma that gets in the way of finding safe housing or steady work. These are barriers that can increase stress levels, reduce acquisition of coping skills or other necessary resources for daily life, and lead back into substance use and behaviors that initially got them into trouble. This study examined what factors are most likely to contribute to an individual’s reincarceration among individuals who use drugs. By understanding the factors that predict reincarceration, policies and services can be geared to best prevent recidivism in these vulnerable groups of individuals who use drugs.
HOW WAS THIS STUDY CONDUCTED?
This was secondary data analysis using longitudinal data from two cohorts in Vancouver, Canada. The first cohort, the AIDS Care Cohort to Evaluate Exposure to Survival Services (ACCESS), enrolled adults that used any illicit substance other than or in addition to cannabis and are living with HIV. The second cohort, the Vancouver Injection Drug Users Study (VIDUS), enrolled adults who injected drugs and are HIV-negative. In this secondary analysis, participants were included if they were in either cohort from June 2006 to November 2018, reported an incarceration event at any point during the study period, and had one subsequent study visit. A participant’s baseline in this analysis was considered their time of first reported incarceration during the study period. Participants who had not had an interview in the 2 years before the study period end of 2018 were considered lost to follow-up. The total sample across both cohorts was 2350, but only 468 of those experienced incarceration and completed a follow-up visit and are included in this analysis.
The assessments were conducted by trained interviewers with participants at baseline and every 6 months. The assessments covered substance use, sexual experiences, and other things like criminal legal involvement. The primary outcome – reincarceration – was defined as a reincarceration event during the study period in a provincial (i.e., the Canadian equivalent of a US state) prison or federal penitentiary.
The analysis explored the following factors that should not change over time (time invariant) as binary indicators (yes/no) associated with reincarceration: self-identified men (versus women and non-binary gender), ethnicity/ancestry (white vs. Indigenous vs. other), education at baseline (less than high school diploma vs. high school diploma or more), service use in jail during baseline incarceration (e.g., including services such as anger management or substance use), and baseline HIV status. There were also factors included in the models that were updated over time, as appropriate, including age at study visit, HIV status, homelessness, sex work, engagement in community judicial supervision, stimulant use, opioid use, any injection drug use, and heavy alcohol use (defined using the NIAAA 2010 criteria for men and women), self-reported mental illness diagnosis, calendar year of study visit, reincarceration events during the study period (none, one, two or more), and accessing addiction treatment.
Of the 468 participants in this study, the median age was 40 years (75% of the sample was between 34-46 years), 74% were men, and 38% identified as Indigenous. Individuals were reincarcerated between 0 and 11 times with nearly half experiencing at least one reincarceration event.
WHAT DID THIS STUDY FIND?
Environmental-level factors were most strongly associated with reincarceration.
In the analysis that adjusted for several factors at once, the presence of 4 factors were more likely to be linked to reincarceration while the presence of 3 other factors were likely to reduce the potential of reincarceration. Experiencing homelessness, being under community judicial supervision, and heavy alcohol use were factors related to an increased risk of reincarceration. Reincarceration during the study period was also associated with increased risk of reincarceration, suggesting that among those who were reincarcerated once, their risk of being incarcerated again increased. Among those factors found to increase one’s risk for reincarceration, being under community judicial supervision presented the greatest risk, nearly double that of the other factors with the exception of homelessness. Yet, participation in addiction treatment, the presence of a mental illness, and older age, were negatively related to reincarceration risk. Among those factors found to decrease one’s risk for reincarceration, being older was the strongest predictor, but was similar in magnitude to the other factors.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study of individuals who used drugs in Canada and had been incarcerated, the odds of being reincarcerated no better than the flip of a coin, suggesting there are a lot of opportunities to make a difference. Importantly, several of the factors implicated in this relationship are areas that communities can address with targeted programming, intervention, and recovery supports.
Experiencing homelessness was linked to increased reincarceration while engagement in addiction treatment was linked to reduced reincarceration. These findings suggest that actively linking individuals leaving jail or prison with stable housing, including recovery-supportive housing such as sober homes, may be an important way to reduce their risk of reincarceration.
Although this study conducted visits with participants whether or not they were incarcerated at the time of the study visit, the researchers were unable to reach some participants. This is a limitation as there may be important differences between those who were available for follow-up study visits and those who could not be reached. For example, individuals who missed study visits were more likely to have been reincarcerated than those who did not miss study visits.
Access to, and use of, treatment and recovery supports after incarceration was not documented in a detailed manner. So, beyond a binary measure of addiction treatment attendance, it is unclear to what degree individuals received any of these supports and how they might have influenced their risk of reincarceration.
BOTTOM LINE
In this study of individuals who used drugs in Canada and had been incarcerated, nearly half were reincarcerated. Several system-level factors were linked to greater odds of reincarceration, including experiencing homelessness, while receiving treatment was linked to reduced odds of reincarceration. These findings suggest that criminal justice efforts – to prevent the additional financial and human costs of reincarceration – should seek to increase access to these key supports for individuals leaving a supervised setting. One key individual-level factor linked to increased reincarceration was heavy alcohol use, suggesting that greater attention be paid to addressing alcohol use among incarcerated populations.
For individuals and families seeking recovery: Individuals who use drugs are also more likely to experience incarceration, and if incarcerated, to experience reincarceration. These individuals are likely to benefit from interventions for re-entry and recovery from treatment professionals and connections to the larger community to build their recovery capital. Addressing basic needs, such as housing, can go a long way in preventing recidivism.
For treatment professionals and treatment systems: Individuals leaving incarceration who also have a history of substance use are likely to benefit from continued support and interventions for re-entry and recovery from treatment professionals to prevent reincarceration. In addition to addressing substance use treatment needs, providers working with these individuals may also assist patients with modifying behaviors that may interfere with successful engagement with re-entry (e.g., motivation, other barriers to participation in treatment, etc.) and through linkage to other community recovery supports.
For scientists: This study identifies some key risks for reincarceration among individuals who use drugs and points to gaps in our understanding of these relationships. Future work that examines trajectories of these individuals, while including factors such as type of substance use, community-recovery support services, and a wider array of individual-, social- and community-level risk and protective factors will help advance the field’s understanding of how best to support individuals leaving prison or jail settings. Because of substantial economic costs of reincarceration, cost-benefit analysis of addressing gaps in recovery capital for individuals’ post-incarceration could help highlight where resources might be better spent (e.g., on providing housing, job training/access, treatment, vs further incarceration costs).
For policy makers: More funding and research to address community re-entry supports after incarceration for individuals with a substance use history can help clarify aspects of programming that are effective and cost-effective and areas where community infrastructure needs additional support. Access to sustainable housing is a key source of stress in the early re-entry days and one that can lead to future incarceration. Funding and research to address these linkages could help support these vital community-based resources. Given that diversion programs, such as drug or recovery courts can also reduce substance use and recidivism, and addiction treatment was a protective factor against reincarceration in this study, ensuring access to these services is likely to have broader benefits for the criminal justice system and society at large.
For example, they may face discrimination or stigma that gets in the way of finding safe housing or steady work. These are barriers that can increase stress levels, reduce acquisition of coping skills or other necessary resources for daily life, and lead back into substance use and behaviors that initially got them into trouble. This study examined what factors are most likely to contribute to an individual’s reincarceration among individuals who use drugs. By understanding the factors that predict reincarceration, policies and services can be geared to best prevent recidivism in these vulnerable groups of individuals who use drugs.
HOW WAS THIS STUDY CONDUCTED?
This was secondary data analysis using longitudinal data from two cohorts in Vancouver, Canada. The first cohort, the AIDS Care Cohort to Evaluate Exposure to Survival Services (ACCESS), enrolled adults that used any illicit substance other than or in addition to cannabis and are living with HIV. The second cohort, the Vancouver Injection Drug Users Study (VIDUS), enrolled adults who injected drugs and are HIV-negative. In this secondary analysis, participants were included if they were in either cohort from June 2006 to November 2018, reported an incarceration event at any point during the study period, and had one subsequent study visit. A participant’s baseline in this analysis was considered their time of first reported incarceration during the study period. Participants who had not had an interview in the 2 years before the study period end of 2018 were considered lost to follow-up. The total sample across both cohorts was 2350, but only 468 of those experienced incarceration and completed a follow-up visit and are included in this analysis.
The assessments were conducted by trained interviewers with participants at baseline and every 6 months. The assessments covered substance use, sexual experiences, and other things like criminal legal involvement. The primary outcome – reincarceration – was defined as a reincarceration event during the study period in a provincial (i.e., the Canadian equivalent of a US state) prison or federal penitentiary.
The analysis explored the following factors that should not change over time (time invariant) as binary indicators (yes/no) associated with reincarceration: self-identified men (versus women and non-binary gender), ethnicity/ancestry (white vs. Indigenous vs. other), education at baseline (less than high school diploma vs. high school diploma or more), service use in jail during baseline incarceration (e.g., including services such as anger management or substance use), and baseline HIV status. There were also factors included in the models that were updated over time, as appropriate, including age at study visit, HIV status, homelessness, sex work, engagement in community judicial supervision, stimulant use, opioid use, any injection drug use, and heavy alcohol use (defined using the NIAAA 2010 criteria for men and women), self-reported mental illness diagnosis, calendar year of study visit, reincarceration events during the study period (none, one, two or more), and accessing addiction treatment.
Of the 468 participants in this study, the median age was 40 years (75% of the sample was between 34-46 years), 74% were men, and 38% identified as Indigenous. Individuals were reincarcerated between 0 and 11 times with nearly half experiencing at least one reincarceration event.
WHAT DID THIS STUDY FIND?
Environmental-level factors were most strongly associated with reincarceration.
In the analysis that adjusted for several factors at once, the presence of 4 factors were more likely to be linked to reincarceration while the presence of 3 other factors were likely to reduce the potential of reincarceration. Experiencing homelessness, being under community judicial supervision, and heavy alcohol use were factors related to an increased risk of reincarceration. Reincarceration during the study period was also associated with increased risk of reincarceration, suggesting that among those who were reincarcerated once, their risk of being incarcerated again increased. Among those factors found to increase one’s risk for reincarceration, being under community judicial supervision presented the greatest risk, nearly double that of the other factors with the exception of homelessness. Yet, participation in addiction treatment, the presence of a mental illness, and older age, were negatively related to reincarceration risk. Among those factors found to decrease one’s risk for reincarceration, being older was the strongest predictor, but was similar in magnitude to the other factors.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study of individuals who used drugs in Canada and had been incarcerated, the odds of being reincarcerated no better than the flip of a coin, suggesting there are a lot of opportunities to make a difference. Importantly, several of the factors implicated in this relationship are areas that communities can address with targeted programming, intervention, and recovery supports.
Experiencing homelessness was linked to increased reincarceration while engagement in addiction treatment was linked to reduced reincarceration. These findings suggest that actively linking individuals leaving jail or prison with stable housing, including recovery-supportive housing such as sober homes, may be an important way to reduce their risk of reincarceration.
Although this study conducted visits with participants whether or not they were incarcerated at the time of the study visit, the researchers were unable to reach some participants. This is a limitation as there may be important differences between those who were available for follow-up study visits and those who could not be reached. For example, individuals who missed study visits were more likely to have been reincarcerated than those who did not miss study visits.
Access to, and use of, treatment and recovery supports after incarceration was not documented in a detailed manner. So, beyond a binary measure of addiction treatment attendance, it is unclear to what degree individuals received any of these supports and how they might have influenced their risk of reincarceration.
BOTTOM LINE
In this study of individuals who used drugs in Canada and had been incarcerated, nearly half were reincarcerated. Several system-level factors were linked to greater odds of reincarceration, including experiencing homelessness, while receiving treatment was linked to reduced odds of reincarceration. These findings suggest that criminal justice efforts – to prevent the additional financial and human costs of reincarceration – should seek to increase access to these key supports for individuals leaving a supervised setting. One key individual-level factor linked to increased reincarceration was heavy alcohol use, suggesting that greater attention be paid to addressing alcohol use among incarcerated populations.
For individuals and families seeking recovery: Individuals who use drugs are also more likely to experience incarceration, and if incarcerated, to experience reincarceration. These individuals are likely to benefit from interventions for re-entry and recovery from treatment professionals and connections to the larger community to build their recovery capital. Addressing basic needs, such as housing, can go a long way in preventing recidivism.
For treatment professionals and treatment systems: Individuals leaving incarceration who also have a history of substance use are likely to benefit from continued support and interventions for re-entry and recovery from treatment professionals to prevent reincarceration. In addition to addressing substance use treatment needs, providers working with these individuals may also assist patients with modifying behaviors that may interfere with successful engagement with re-entry (e.g., motivation, other barriers to participation in treatment, etc.) and through linkage to other community recovery supports.
For scientists: This study identifies some key risks for reincarceration among individuals who use drugs and points to gaps in our understanding of these relationships. Future work that examines trajectories of these individuals, while including factors such as type of substance use, community-recovery support services, and a wider array of individual-, social- and community-level risk and protective factors will help advance the field’s understanding of how best to support individuals leaving prison or jail settings. Because of substantial economic costs of reincarceration, cost-benefit analysis of addressing gaps in recovery capital for individuals’ post-incarceration could help highlight where resources might be better spent (e.g., on providing housing, job training/access, treatment, vs further incarceration costs).
For policy makers: More funding and research to address community re-entry supports after incarceration for individuals with a substance use history can help clarify aspects of programming that are effective and cost-effective and areas where community infrastructure needs additional support. Access to sustainable housing is a key source of stress in the early re-entry days and one that can lead to future incarceration. Funding and research to address these linkages could help support these vital community-based resources. Given that diversion programs, such as drug or recovery courts can also reduce substance use and recidivism, and addiction treatment was a protective factor against reincarceration in this study, ensuring access to these services is likely to have broader benefits for the criminal justice system and society at large.