Increasing cannabis use worsens depression for most young adults
Cannabis use among young adults is linked to depressive symptoms, but the direction of the relationship is unclear; that is, whether increased use leads to increased depression or if increased depression leads to increased use of cannabis. This longitudinal study of youth in the community explored this relationship between cannabis use and depression from teen through young adult years.
Long-term cannabis use, beginning during one’s teenage years and persisting into adulthood is associated with a range of negative consequences, including mental health challenges such as depression. Although cannabis use has been linked to depressive symptoms, it is possible both that increased use leads to increased depression — a substance-induced pathway – or that experiencing depression leads to use of cannabis — a “self-medication” pathway. Although both pathways have been documented, it may be the case that one is more likely, on average, to happen to young adults who use cannabis. This is because there are different reasons why these two experiences are related.
On the one hand, someone might have depressive symptoms or experience worsening depression directly because of long-term cannabis use. This is because cannabis use can alter how the brain functions, impacting the same areas of the brain that are responsible for depressive symptoms. On the other hand, young adults may use cannabis to cope with feeling sad, distressed, or anxious. The use of cannabis may be exaggerated in those coping with highly negative events, occurring in their childhood, such as experiencing physical or sexual abuse or witnessing parental violence (these are called “adverse childhood experiences” or ACES). While cannabis use and depression may exacerbate each other, another theory, related to the “self-medication” hypothesis, is that cannabis use could also help individuals cope with depression and other emotional difficulties.
This longitudinal study explored pathways between cannabis use and depression, following teens in the community through young adulthood. It also explored whether there were differences in the experience of cannabis use and depression by whether young adults had experienced an adverse childhood event.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of data from a longitudinal cohort study assessing an initial group of 2,234 youth and young adults annually recruited in 6th and 7th grade starting in 2008. Participants were aged 17-24 years in this analysis, representing 5 waves of data. Participants were recruited from 16 middle schools in California and most still lived there during the time of the study waves used in this analysis. The larger study was an examination of the afterschool substance use prevention program, CHOICE (the CHOICE program effects on substance use initiation were not found to last longer than 1 year after the intervention).
The primary outcomes in this analysis were the past month days of cannabis use (0-30 days) and depression symptoms (scores could range from 0-21). They used the Adverse Childhood Experiences scale to group participants for the analysis focused on differences between those who had experienced any adverse events in their childhood (prior to age 18) and those who had not.
The analysis examined the relationship between cannabis use and depression in two ways. First, the analysis examined whether levels of one variable at one timepoint (e.g., level of depression) was associated with later changes to one’s behavior (e.g., level of cannabis use). Next, the analysis examined how changes in one variable (e.g., changes in cannabis use between time points) are associated with degree of change in another variable (e.g., changes in depression). Both analyses controlled for potentially important factors including past-month alcohol and tobacco use from the initial year of data used for this study (Wave 8) and the participant’s CHOICE intervention status, although the intervention did not have lasting effects after year 1 (as noted above).
Of this sample of 2,234 young adults, 54% were female, 24% reported past month cannabis use and 6% reported daily use of cannabis, 12% met the cutoff for significant depression (i.e., “probable depressive disorder”), and 28% had at least one adverse childhood event.
WHAT DID THIS STUDY FIND?
Increasing cannabis use was associated with increased depression over time.
Young adults who had greater increases in cannabis use between two prior ages (e.g., 18 and 19 years) also reported greater increases in depressive symptoms between two later ages (e.g., 19 and 20 years). Furthermore, among young adults who increase cannabis use, even when cannabis use drops later, depression appears to remain at higher levels. Young adults who reported greater prior levels of depression symptoms in early waves decreased their cannabis use as they grew older.
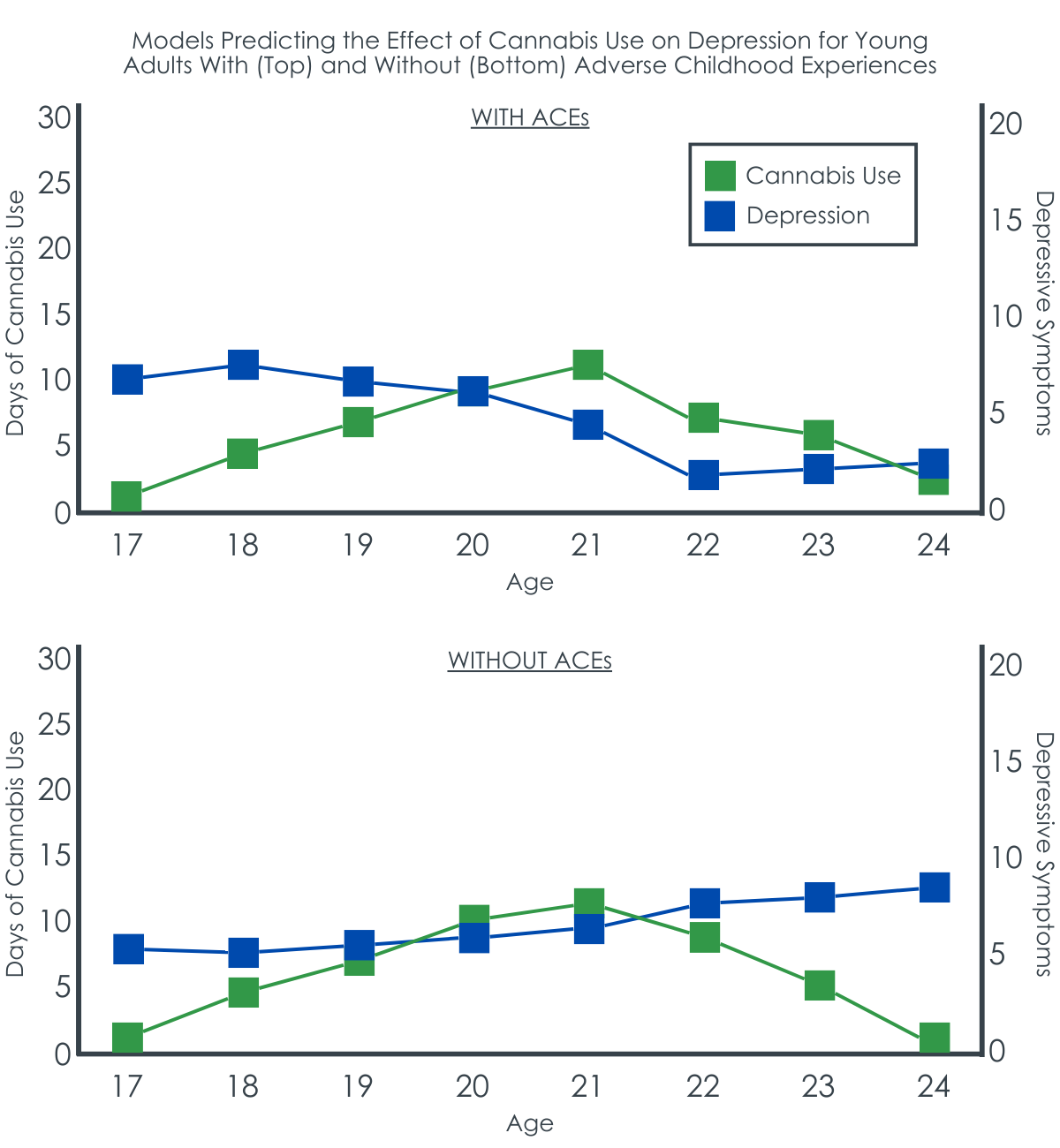
Experiencing Adverse Childhood Events was associated with changes in the relationship between cannabis use and depression.
Among young adults who had not experienced adverse childhood events, as their cannabis use increased, there was an accompanying increase in depression. Yet, for young adults who had experienced one or more adverse childhood events, as their cannabis use increased, there was a subsequent decrease in depression.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study of over 2000 young adults, increasing cannabis use was associated with increasing depressive symptoms at a later time period. Although cannabis use may have decreased later, the depressive symptoms remained elevated, suggesting potential lasting effects that may be due to the increased cannabis use during a critical developmental period. Yet, for young adults who had experienced adverse childhood events, there was the opposite effect, where increased cannabis use was associated with reduced depression over time. While it appeared there were some potentially helpful aspects of cannabis use in the group who experienced trauma, i.e., in reduced depression symptoms, use of cannabis – especially during this critical developmental period – increases risks of other side effects and adverse events including cannabis use disorder. Notably, there are evidence-based treatments, including behavioral or medication-based treatments to address depression that could be used instead with fewer harms to health.
Long-term cannabis use or use that begins in youth and persists into adulthood is associated with a range of negative health and social consequences, including depression as this study indicates. As well, for those with an underlying vulnerability, cannabis use can have other severe risks including catalyzing psychotic disorders. Yet, early intervention and treatment may be key to addressing both cannabis use and depression as there are some evidence-based cannabis use treatments that can decrease both. There may be some unique needs for young adults with experiences of adverse childhood events that should be identified and addressed.
This study analyzed data from a previous intervention study. Thus, the data were collected with different aims in mind (intervention efficacy) and the relationships examined here are exploratory in nature.
Given changes in the drug supply and increases in cannabis use potency over time, it is possible the relationships with cannabis use and mental health conditions such as depression are stronger than this study indicates as the cohort in this study was from over 5 years ago.
BOTTOM LINE
Increasing cannabis use during emerging adulthood was associated with increases in depressive symptoms. Depressive symptoms remained even when cannabis use decreased, suggesting some potentially lasting effects from the increased cannabis use during a critical developmental period. Yet, young adults who had experienced adverse childhood events had reduced depression with increased cannabis use. This suggests that for young adults with a history of trauma in childhood, there is a need to link them to effective treatments which will support reducing their depression symptoms in place of cannabis use, which itself can produce unwanted psychiatric side effects including cannabis use disorder.
For individuals and families seeking recovery: Individuals with depression are more likely to use cannabis, but this increasing cannabis use may lead to worsening depression. There are evidence-based treatments that can address both cannabis use and depression. It is important to seek out a provider to discuss concerns with them and the best ways to address both challenges.
For treatment professionals and treatment systems: Clinicians working with young adults should screen for cannabis use and depressive symptoms and discuss alternative ways to cope with depressive symptoms if cannabis is being used to reduce symptoms. Identifying whether an individual has experienced adverse childhood events is important, as there may be some unique intervention needs for these young adults with those experiences.
For scientists: This study highlights an innovative approach to understanding causal effects of naturalistically occurring behaviors over time. In this study, the authors found that the effects of depression on later cannabis use (and vice versa) were different depending on whether the predictor was operationalized as symptom severity at a single point in time or was operationalized as changes in symptoms over time. These are key methodological considerations for future examination. There is also a need for the development and testing of novel treatments for young adults using cannabis to cope with depression, stress, and traumatic childhood events.
Long-term cannabis use, beginning during one’s teenage years and persisting into adulthood is associated with a range of negative consequences, including mental health challenges such as depression. Although cannabis use has been linked to depressive symptoms, it is possible both that increased use leads to increased depression — a substance-induced pathway – or that experiencing depression leads to use of cannabis — a “self-medication” pathway. Although both pathways have been documented, it may be the case that one is more likely, on average, to happen to young adults who use cannabis. This is because there are different reasons why these two experiences are related.
On the one hand, someone might have depressive symptoms or experience worsening depression directly because of long-term cannabis use. This is because cannabis use can alter how the brain functions, impacting the same areas of the brain that are responsible for depressive symptoms. On the other hand, young adults may use cannabis to cope with feeling sad, distressed, or anxious. The use of cannabis may be exaggerated in those coping with highly negative events, occurring in their childhood, such as experiencing physical or sexual abuse or witnessing parental violence (these are called “adverse childhood experiences” or ACES). While cannabis use and depression may exacerbate each other, another theory, related to the “self-medication” hypothesis, is that cannabis use could also help individuals cope with depression and other emotional difficulties.
This longitudinal study explored pathways between cannabis use and depression, following teens in the community through young adulthood. It also explored whether there were differences in the experience of cannabis use and depression by whether young adults had experienced an adverse childhood event.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of data from a longitudinal cohort study assessing an initial group of 2,234 youth and young adults annually recruited in 6th and 7th grade starting in 2008. Participants were aged 17-24 years in this analysis, representing 5 waves of data. Participants were recruited from 16 middle schools in California and most still lived there during the time of the study waves used in this analysis. The larger study was an examination of the afterschool substance use prevention program, CHOICE (the CHOICE program effects on substance use initiation were not found to last longer than 1 year after the intervention).
The primary outcomes in this analysis were the past month days of cannabis use (0-30 days) and depression symptoms (scores could range from 0-21). They used the Adverse Childhood Experiences scale to group participants for the analysis focused on differences between those who had experienced any adverse events in their childhood (prior to age 18) and those who had not.
The analysis examined the relationship between cannabis use and depression in two ways. First, the analysis examined whether levels of one variable at one timepoint (e.g., level of depression) was associated with later changes to one’s behavior (e.g., level of cannabis use). Next, the analysis examined how changes in one variable (e.g., changes in cannabis use between time points) are associated with degree of change in another variable (e.g., changes in depression). Both analyses controlled for potentially important factors including past-month alcohol and tobacco use from the initial year of data used for this study (Wave 8) and the participant’s CHOICE intervention status, although the intervention did not have lasting effects after year 1 (as noted above).
Of this sample of 2,234 young adults, 54% were female, 24% reported past month cannabis use and 6% reported daily use of cannabis, 12% met the cutoff for significant depression (i.e., “probable depressive disorder”), and 28% had at least one adverse childhood event.
WHAT DID THIS STUDY FIND?
Increasing cannabis use was associated with increased depression over time.
Young adults who had greater increases in cannabis use between two prior ages (e.g., 18 and 19 years) also reported greater increases in depressive symptoms between two later ages (e.g., 19 and 20 years). Furthermore, among young adults who increase cannabis use, even when cannabis use drops later, depression appears to remain at higher levels. Young adults who reported greater prior levels of depression symptoms in early waves decreased their cannabis use as they grew older.
Experiencing Adverse Childhood Events was associated with changes in the relationship between cannabis use and depression.
Among young adults who had not experienced adverse childhood events, as their cannabis use increased, there was an accompanying increase in depression. Yet, for young adults who had experienced one or more adverse childhood events, as their cannabis use increased, there was a subsequent decrease in depression.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study of over 2000 young adults, increasing cannabis use was associated with increasing depressive symptoms at a later time period. Although cannabis use may have decreased later, the depressive symptoms remained elevated, suggesting potential lasting effects that may be due to the increased cannabis use during a critical developmental period. Yet, for young adults who had experienced adverse childhood events, there was the opposite effect, where increased cannabis use was associated with reduced depression over time. While it appeared there were some potentially helpful aspects of cannabis use in the group who experienced trauma, i.e., in reduced depression symptoms, use of cannabis – especially during this critical developmental period – increases risks of other side effects and adverse events including cannabis use disorder. Notably, there are evidence-based treatments, including behavioral or medication-based treatments to address depression that could be used instead with fewer harms to health.
Long-term cannabis use or use that begins in youth and persists into adulthood is associated with a range of negative health and social consequences, including depression as this study indicates. As well, for those with an underlying vulnerability, cannabis use can have other severe risks including catalyzing psychotic disorders. Yet, early intervention and treatment may be key to addressing both cannabis use and depression as there are some evidence-based cannabis use treatments that can decrease both. There may be some unique needs for young adults with experiences of adverse childhood events that should be identified and addressed.
This study analyzed data from a previous intervention study. Thus, the data were collected with different aims in mind (intervention efficacy) and the relationships examined here are exploratory in nature.
Given changes in the drug supply and increases in cannabis use potency over time, it is possible the relationships with cannabis use and mental health conditions such as depression are stronger than this study indicates as the cohort in this study was from over 5 years ago.
BOTTOM LINE
Increasing cannabis use during emerging adulthood was associated with increases in depressive symptoms. Depressive symptoms remained even when cannabis use decreased, suggesting some potentially lasting effects from the increased cannabis use during a critical developmental period. Yet, young adults who had experienced adverse childhood events had reduced depression with increased cannabis use. This suggests that for young adults with a history of trauma in childhood, there is a need to link them to effective treatments which will support reducing their depression symptoms in place of cannabis use, which itself can produce unwanted psychiatric side effects including cannabis use disorder.
For individuals and families seeking recovery: Individuals with depression are more likely to use cannabis, but this increasing cannabis use may lead to worsening depression. There are evidence-based treatments that can address both cannabis use and depression. It is important to seek out a provider to discuss concerns with them and the best ways to address both challenges.
For treatment professionals and treatment systems: Clinicians working with young adults should screen for cannabis use and depressive symptoms and discuss alternative ways to cope with depressive symptoms if cannabis is being used to reduce symptoms. Identifying whether an individual has experienced adverse childhood events is important, as there may be some unique intervention needs for these young adults with those experiences.
For scientists: This study highlights an innovative approach to understanding causal effects of naturalistically occurring behaviors over time. In this study, the authors found that the effects of depression on later cannabis use (and vice versa) were different depending on whether the predictor was operationalized as symptom severity at a single point in time or was operationalized as changes in symptoms over time. These are key methodological considerations for future examination. There is also a need for the development and testing of novel treatments for young adults using cannabis to cope with depression, stress, and traumatic childhood events.
Long-term cannabis use, beginning during one’s teenage years and persisting into adulthood is associated with a range of negative consequences, including mental health challenges such as depression. Although cannabis use has been linked to depressive symptoms, it is possible both that increased use leads to increased depression — a substance-induced pathway – or that experiencing depression leads to use of cannabis — a “self-medication” pathway. Although both pathways have been documented, it may be the case that one is more likely, on average, to happen to young adults who use cannabis. This is because there are different reasons why these two experiences are related.
On the one hand, someone might have depressive symptoms or experience worsening depression directly because of long-term cannabis use. This is because cannabis use can alter how the brain functions, impacting the same areas of the brain that are responsible for depressive symptoms. On the other hand, young adults may use cannabis to cope with feeling sad, distressed, or anxious. The use of cannabis may be exaggerated in those coping with highly negative events, occurring in their childhood, such as experiencing physical or sexual abuse or witnessing parental violence (these are called “adverse childhood experiences” or ACES). While cannabis use and depression may exacerbate each other, another theory, related to the “self-medication” hypothesis, is that cannabis use could also help individuals cope with depression and other emotional difficulties.
This longitudinal study explored pathways between cannabis use and depression, following teens in the community through young adulthood. It also explored whether there were differences in the experience of cannabis use and depression by whether young adults had experienced an adverse childhood event.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of data from a longitudinal cohort study assessing an initial group of 2,234 youth and young adults annually recruited in 6th and 7th grade starting in 2008. Participants were aged 17-24 years in this analysis, representing 5 waves of data. Participants were recruited from 16 middle schools in California and most still lived there during the time of the study waves used in this analysis. The larger study was an examination of the afterschool substance use prevention program, CHOICE (the CHOICE program effects on substance use initiation were not found to last longer than 1 year after the intervention).
The primary outcomes in this analysis were the past month days of cannabis use (0-30 days) and depression symptoms (scores could range from 0-21). They used the Adverse Childhood Experiences scale to group participants for the analysis focused on differences between those who had experienced any adverse events in their childhood (prior to age 18) and those who had not.
The analysis examined the relationship between cannabis use and depression in two ways. First, the analysis examined whether levels of one variable at one timepoint (e.g., level of depression) was associated with later changes to one’s behavior (e.g., level of cannabis use). Next, the analysis examined how changes in one variable (e.g., changes in cannabis use between time points) are associated with degree of change in another variable (e.g., changes in depression). Both analyses controlled for potentially important factors including past-month alcohol and tobacco use from the initial year of data used for this study (Wave 8) and the participant’s CHOICE intervention status, although the intervention did not have lasting effects after year 1 (as noted above).
Of this sample of 2,234 young adults, 54% were female, 24% reported past month cannabis use and 6% reported daily use of cannabis, 12% met the cutoff for significant depression (i.e., “probable depressive disorder”), and 28% had at least one adverse childhood event.
WHAT DID THIS STUDY FIND?
Increasing cannabis use was associated with increased depression over time.
Young adults who had greater increases in cannabis use between two prior ages (e.g., 18 and 19 years) also reported greater increases in depressive symptoms between two later ages (e.g., 19 and 20 years). Furthermore, among young adults who increase cannabis use, even when cannabis use drops later, depression appears to remain at higher levels. Young adults who reported greater prior levels of depression symptoms in early waves decreased their cannabis use as they grew older.
Experiencing Adverse Childhood Events was associated with changes in the relationship between cannabis use and depression.
Among young adults who had not experienced adverse childhood events, as their cannabis use increased, there was an accompanying increase in depression. Yet, for young adults who had experienced one or more adverse childhood events, as their cannabis use increased, there was a subsequent decrease in depression.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study of over 2000 young adults, increasing cannabis use was associated with increasing depressive symptoms at a later time period. Although cannabis use may have decreased later, the depressive symptoms remained elevated, suggesting potential lasting effects that may be due to the increased cannabis use during a critical developmental period. Yet, for young adults who had experienced adverse childhood events, there was the opposite effect, where increased cannabis use was associated with reduced depression over time. While it appeared there were some potentially helpful aspects of cannabis use in the group who experienced trauma, i.e., in reduced depression symptoms, use of cannabis – especially during this critical developmental period – increases risks of other side effects and adverse events including cannabis use disorder. Notably, there are evidence-based treatments, including behavioral or medication-based treatments to address depression that could be used instead with fewer harms to health.
Long-term cannabis use or use that begins in youth and persists into adulthood is associated with a range of negative health and social consequences, including depression as this study indicates. As well, for those with an underlying vulnerability, cannabis use can have other severe risks including catalyzing psychotic disorders. Yet, early intervention and treatment may be key to addressing both cannabis use and depression as there are some evidence-based cannabis use treatments that can decrease both. There may be some unique needs for young adults with experiences of adverse childhood events that should be identified and addressed.
This study analyzed data from a previous intervention study. Thus, the data were collected with different aims in mind (intervention efficacy) and the relationships examined here are exploratory in nature.
Given changes in the drug supply and increases in cannabis use potency over time, it is possible the relationships with cannabis use and mental health conditions such as depression are stronger than this study indicates as the cohort in this study was from over 5 years ago.
BOTTOM LINE
Increasing cannabis use during emerging adulthood was associated with increases in depressive symptoms. Depressive symptoms remained even when cannabis use decreased, suggesting some potentially lasting effects from the increased cannabis use during a critical developmental period. Yet, young adults who had experienced adverse childhood events had reduced depression with increased cannabis use. This suggests that for young adults with a history of trauma in childhood, there is a need to link them to effective treatments which will support reducing their depression symptoms in place of cannabis use, which itself can produce unwanted psychiatric side effects including cannabis use disorder.
For individuals and families seeking recovery: Individuals with depression are more likely to use cannabis, but this increasing cannabis use may lead to worsening depression. There are evidence-based treatments that can address both cannabis use and depression. It is important to seek out a provider to discuss concerns with them and the best ways to address both challenges.
For treatment professionals and treatment systems: Clinicians working with young adults should screen for cannabis use and depressive symptoms and discuss alternative ways to cope with depressive symptoms if cannabis is being used to reduce symptoms. Identifying whether an individual has experienced adverse childhood events is important, as there may be some unique intervention needs for these young adults with those experiences.
For scientists: This study highlights an innovative approach to understanding causal effects of naturalistically occurring behaviors over time. In this study, the authors found that the effects of depression on later cannabis use (and vice versa) were different depending on whether the predictor was operationalized as symptom severity at a single point in time or was operationalized as changes in symptoms over time. These are key methodological considerations for future examination. There is also a need for the development and testing of novel treatments for young adults using cannabis to cope with depression, stress, and traumatic childhood events.