Initial evaluation of a peer recovery coach program in a large hospital system
Recovery coaches are typically individuals with “lived experience” of substance use disorder (SUD) recovery who have specialized training to help peers navigate the challenges of early recovery. While recovery coaches have been central to community-based recovery support services since their inception, they are starting to be integrated into mainstream general hospital settings. In this initial evaluation of a peer recovery coach program in a large hospital system, researchers compared how individuals fared clinically in the 6 months before and after meeting with a recovery coach. For individuals who were prescribed buprenorphine, the researchers also examined whether recovery coach contact was associated with buprenorphine engagement and opioid abstinence outcomes.
In the past few years, state and federal agencies have been expanding recovery coach programs. Recovery coach models have been implemented in state healthcare systems in Vermont and Massachusetts, primary care delivered by the Veterans Administration, and emergency departments all over the country.
A qualitative study showed that recovery coaches can offer social support and help with health system navigation. One systematic review found that recovery coaches may improve patients’ substance use and recovery-related outcomes. While these early studies report that recovery coach models are innovative, popular, and cost-effective, there is little empirical evidence on clinical or cost outcomes. Knowledge of how patients fare when they engage with recovery coaches in clinical settings is not well-established.
In this study, Magidson and colleagues used electronic healthcare record data from a large general hospital system to provide some estimates of how patients fare clinically after engaging with a peer recovery coach.
HOW WAS THIS STUDY CONDUCTED?
This study was an evaluation of the recovery coach program at the Massachusetts General Hospital in Boston, MA. It included 1,171 patients who had their initial coach encounter between January 2015 and September 2017.
The hospital’s recovery coach program employed 1 recovery coach manager and 9 coaches stationed in community health centers, primary care offices, and an outpatient substance use disorder clinic. Recovery coaches were required to be in recovery for at least 2 years and complete a week-long training course on themes like ethics, boundaries, self-care, and motivational interviewing. Coaches provided in-person support to patients in clinical practice settings by accompanying patients to medical appointments, helping to navigate social services, and making connections to community-based recovery support services. Coaches also offered remote support to patients, which involved phone calls or text messages.
To estimate the impact of the coaching program on clinical outcomes, the researchers compared hospitalizations, outpatient appointments, and emergency department visits in the 6-month periods before and after engaging with a recovery coach using patients’ electronic health records.
In terms of outpatient encounters, the researchers examined changes in the type of outpatient encounter among four common types (primary care, community health center, mental health, and laboratory visit).
Among patients who were prescribed buprenorphine (often prescribed in formulation with naloxone and known by the brand name Suboxone) before or within 30 days of their first contact with a recovery coach, the study also assessed buprenorphine engagement and opioid abstinence.
Buprenorphine engagement was based on whether an individual received a buprenorphine prescription in a given month. The researchers also conducted the analyses where buprenorphine engagement was defined as both receiving a prescription and having buprenorphine in their urine toxicology screen to see if defining engagement this way made a difference to analyses.
Opioid abstinence was based on monthly toxicology results extracted from chart review. Patients were considered abstinent in a given month if all toxicology screens were negative for all tested opioids (e.g., heroin, oxycodone, fentanyl, etc.). Patients were considered non-abstinent if: 1) they did not have a toxicology screen in their chart for a given month or 2) they had one or more toxicology screens positive for an opioid. Not exceeding a period of 12 months, patient data was collected from the last buprenorphine prescription or six months before the initial recovery coach contact, then continuing for six months after initial coach contact.
To assess how current-month recovery coach contact was associated with opioid abstinence, researchers compared recovery coach contact with monthly prescription data and negative toxicology screening results with observation beginning on the day the patient initiated coaching and continuing for 6 months. To assess prior-month recovery coach contact, the researchers conducted the same analysis, with observation beginning 30 days after initiated coaching and continuing for 5 months.
It is important to note that the research team focused on recovery coaching engagement and subsequent healthcare utilization. They did not provide any data on patient characteristics (e.g., demographics, substance of choice, treatment history, etc.) in this study.
WHAT DID THIS STUDY FIND?
Patients spent a median of 120 minutes with a coach and contacted a coach an average of 4 times total. Among 1,171 patients who initiated recovery coach contact between January 2015 and September 15, patients were in communication with a coach (first to final contact) over a median duration of 51 days. In terms of communication channel, 50% of patients contacted a coach in person, 44% by phone call with a client, and 6% by phone call on behalf of a client.
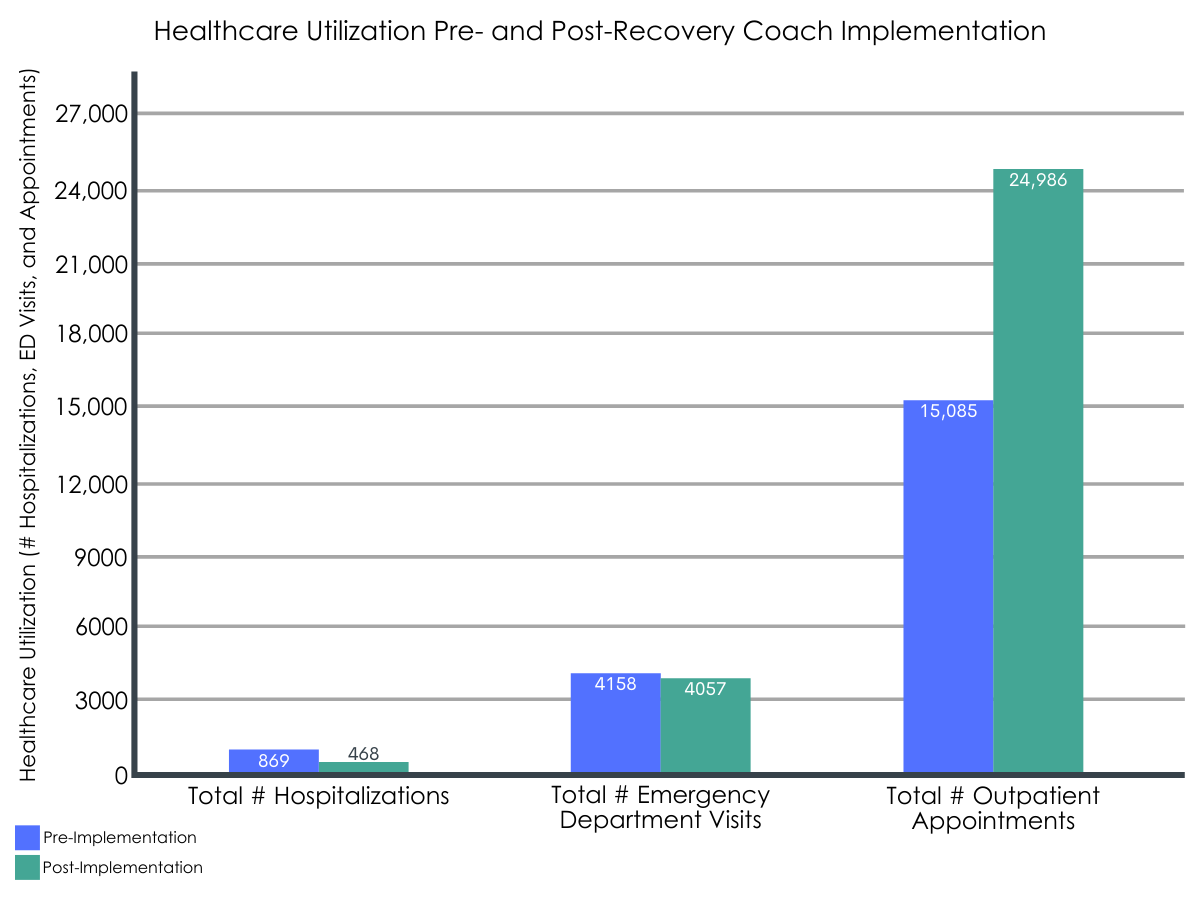
Hospitalizations and emergency department visits decreased in the period after engaging with a recovery coach.
After engaging with a recovery coach, there was a significant decrease in the percentage of patients hospitalized from the 6-month pre-period (41%) to the 6-month post-period (23%). There was also a significant decrease in the total number of hospitalizations from the 6-month pre-period (N=869) to the 6-month post-period (N=468).
After engaging with a recovery coach, there was a small nonsignificant decrease in the percentage of patients with emergency department visits from the 6-month pre-period (47%) to the 6-month post-period (43%). There was also a small, nonsignificant decrease in the total number of emergency department visits from the 6-month pre-period (N=4,158) to the 6-month post-period (N=4,057).
Outpatient appointments increased in the period after engaging with a recovery coach.
After engaging with a recovery coach, there was a significant increase in the percentage of patients with outpatient appointments from the 6-month pre-period (86%) to the 6-month post-period (91%). There was also a significant increase in the total number of outpatient appointments from the 6-month pre-period (N=15,085) to the 6-month post-period (N=24,986).
Across primary care, community health, mental health, and lab visits, there were significant increases in number of encounters and number of patients with that encounter for all services. Notably, the percentage of patients with mental health visits increased from the 6-month pre-period (44%) to the 6-month post-period (56%).
Figure 1.
Meeting with a recovery coach was associated with a greater likelihood of treatment engagement and opioid abstinence during the same month, but not during the following month.
Out of 1,620 patient months aggregated from the 12-month period across the subsample of patients who were prescribed buprenorphine, the rate was significantly higher when patients had coaching contact during the current month (61% vs. 39%) and prior month (52% vs. 42%), compared to the rate of receiving both a buprenorphine prescription and negative toxicology screen in a typical month (44%).
Recovery coach contact was associated with a 1.9-times greater likelihood of treatment engagement and 1.3-times greater likelihood of opioid abstinence during that same month in the 6-month period after recovery coach contact. However, recovery coach contact was not associated with greater odds of treatment engagement or opioid abstinence during the following month in the 6-month period following recovery coach contact.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study offers some early insights about how patients with substance use disorder may fare clinically over time in the 6-month periods before and after meeting engaging with a recovery coach.
Notably, after engaging with a recovery coach, substance use disorder patients had significantly lower rates of hospitalizations and significantly greater rates of outpatient treatment. Despite this, no significant change was observed in emergency department visits, although these did decrease slightly once patients engaged with recovery coaches. These results provide some initial support for the potential benefits of recovery coach contact on reducing the need for more expensive, acute care intensive hospital use and more engagement with more cost-effective outpatient services.
Interestingly, compared to the previous month, patients who were prescribed buprenorphine showed a greater likelihood of buprenorphine engagement and opioid abstinence after meeting with a recovery coach in the current month. However, compared to the previous month, there was no significant difference in buprenorphine engagement or opioid abstinence in the following month after meeting with a recovery coach. Thus, it is possible that patients may be meeting with their recovery coach precisely because they were faring better clinically and not the other way around.
These preliminary findings suggest that peer recovery coaches may serve as a beneficial resource for addiction patients. Specifically, recovery coaches, in facilitating the process of navigating outpatient healthcare services, may reduce the need for more acute care like hospitalization. These promising findings build upon past studies that summarized peer-led recovery support services and evaluated a patient navigator program involving peers in recovery, both of which suggested that meeting with recovery coaches was associated with greater treatment engagement. Further research would help establish best practices for how healthcare systems may incorporate recovery coaches into their treatment programs to better support substance use disorder patients.
However, without a comparison group, it is impossible to establish whether these findings were attributable to the recovery coach program. Also, without patient sample characteristics, it is not possible to know how generalizable these results may be to other patient groups. Therefore, while this study suggests recovery coaches may be helpful to individuals with substance use disorder in a general medical hospital context, further research addressing these limitations is necessary to investigate the specific value and effects of peer recovery coaches at a hospital system level.
Because the study did not include a comparison group of patients without recovery coach contact, these healthcare utilization and buprenorphine treatment outcomes may not be specifically attributable to recovery coaches. This study design limits the conclusions that may be drawn about the specific impact of recovery coach models.
The study did not include demographic data on patient sample characteristics, which made it difficult to know whether these findings would hold up in other patient groups, clinical settings, or healthcare systems. Information on clinical severity or initial recovery-related indicators (e.g., motivation to change, social support, etc.) would allow the researchers to model and control for these variables in order to better isolate the unique positive effects from recovery coaching.
The subsample of patients who were prescribed buprenorphine was small, which limited the study’s ability to detect a significant effect on certain measures like subsequent month engagement.
BOTTOM LINE
This study found that substance use disorder patients in a large hospital system had a lower hospitalization rate and greater rate of outpatient treatment utilization in the 6-month period after meeting with a recovery coach, compared to the same 6-month period before contact. Furthermore, compared to the previous month, patients with SUD who were prescribed buprenorphine showed greater buprenorphine engagement and opioid abstinence in the same month they met with a recovery coach, but did not show differences in buprenorphine engagement and opioid abstinence in the month after meeting with a recovery coach in the following month making it unclear whether recovery coaches actually produce medication engagement benefits.
For individuals and families seeking recovery: Patients with substance use disorder showed some beneficial changes in healthcare utilization and buprenorphine treatment outcomes between the 6-month periods before and after contact with a peer recovery coach, based on electronic healthcare record data collected by a large hospital system. However, this study did not properly test the effectiveness of recovery coach contact on these clinical outcomes. While research on the effects of recovery coaching is ongoing, early findings are promising.
For treatment professionals and treatment systems: This study’s findings suggest that recovery coaches may be a helpful resource for linking substance use disorder patients with outpatient healthcare services, which may reduce the need for intensive and costly acute care. Integrated into a patient’s outpatient management team, recovery coaches may be able to leverage their lived experience to facilitate the process of navigating healthcare services and maintaining treatment engagement. More research is needed to determine the specific effect of recovery coaches on clinical outcomes, which may generalize across patient groups.
For scientists:This study’s findings offer some early support regarding the potential of peer recovery coaches in facilitating beneficial healthcare utilization among patients with substance use disorder. Specifically, there was a significant decrease in hospitalizations, significant increase in outpatient appointments, and nonsignificant decrease in emergency department visits between the 6-month periods before and after initiating contact with a recovery coach. Furthermore, buprenorphine engagement and opioid abstinence were more common with current and prior recovery coach contact, than for the months without contact. However, the lack of a well-matched comparison group limited the ability to determine whether recovery coaching was causally related to the outcomes tested here.
For policy makers: This study’s findings suggest that recovery coach models may facilitate beneficial healthcare utilization, including an increase in outpatient appointments and decrease in hospitalizations. A reduction in the use of acute care would also lead to cost-savings long-term for hospitals and public health systems. However, more research is needed to properly determine the effectiveness of recovery coaches on economic and clinical outcomes. More funding directed to research and program evaluations of peer recovery coaching programs can help determine the utility and potential best practices associated with these growing and popular recovery coaching care models.
In the past few years, state and federal agencies have been expanding recovery coach programs. Recovery coach models have been implemented in state healthcare systems in Vermont and Massachusetts, primary care delivered by the Veterans Administration, and emergency departments all over the country.
A qualitative study showed that recovery coaches can offer social support and help with health system navigation. One systematic review found that recovery coaches may improve patients’ substance use and recovery-related outcomes. While these early studies report that recovery coach models are innovative, popular, and cost-effective, there is little empirical evidence on clinical or cost outcomes. Knowledge of how patients fare when they engage with recovery coaches in clinical settings is not well-established.
In this study, Magidson and colleagues used electronic healthcare record data from a large general hospital system to provide some estimates of how patients fare clinically after engaging with a peer recovery coach.
HOW WAS THIS STUDY CONDUCTED?
This study was an evaluation of the recovery coach program at the Massachusetts General Hospital in Boston, MA. It included 1,171 patients who had their initial coach encounter between January 2015 and September 2017.
The hospital’s recovery coach program employed 1 recovery coach manager and 9 coaches stationed in community health centers, primary care offices, and an outpatient substance use disorder clinic. Recovery coaches were required to be in recovery for at least 2 years and complete a week-long training course on themes like ethics, boundaries, self-care, and motivational interviewing. Coaches provided in-person support to patients in clinical practice settings by accompanying patients to medical appointments, helping to navigate social services, and making connections to community-based recovery support services. Coaches also offered remote support to patients, which involved phone calls or text messages.
To estimate the impact of the coaching program on clinical outcomes, the researchers compared hospitalizations, outpatient appointments, and emergency department visits in the 6-month periods before and after engaging with a recovery coach using patients’ electronic health records.
In terms of outpatient encounters, the researchers examined changes in the type of outpatient encounter among four common types (primary care, community health center, mental health, and laboratory visit).
Among patients who were prescribed buprenorphine (often prescribed in formulation with naloxone and known by the brand name Suboxone) before or within 30 days of their first contact with a recovery coach, the study also assessed buprenorphine engagement and opioid abstinence.
Buprenorphine engagement was based on whether an individual received a buprenorphine prescription in a given month. The researchers also conducted the analyses where buprenorphine engagement was defined as both receiving a prescription and having buprenorphine in their urine toxicology screen to see if defining engagement this way made a difference to analyses.
Opioid abstinence was based on monthly toxicology results extracted from chart review. Patients were considered abstinent in a given month if all toxicology screens were negative for all tested opioids (e.g., heroin, oxycodone, fentanyl, etc.). Patients were considered non-abstinent if: 1) they did not have a toxicology screen in their chart for a given month or 2) they had one or more toxicology screens positive for an opioid. Not exceeding a period of 12 months, patient data was collected from the last buprenorphine prescription or six months before the initial recovery coach contact, then continuing for six months after initial coach contact.
To assess how current-month recovery coach contact was associated with opioid abstinence, researchers compared recovery coach contact with monthly prescription data and negative toxicology screening results with observation beginning on the day the patient initiated coaching and continuing for 6 months. To assess prior-month recovery coach contact, the researchers conducted the same analysis, with observation beginning 30 days after initiated coaching and continuing for 5 months.
It is important to note that the research team focused on recovery coaching engagement and subsequent healthcare utilization. They did not provide any data on patient characteristics (e.g., demographics, substance of choice, treatment history, etc.) in this study.
WHAT DID THIS STUDY FIND?
Patients spent a median of 120 minutes with a coach and contacted a coach an average of 4 times total. Among 1,171 patients who initiated recovery coach contact between January 2015 and September 15, patients were in communication with a coach (first to final contact) over a median duration of 51 days. In terms of communication channel, 50% of patients contacted a coach in person, 44% by phone call with a client, and 6% by phone call on behalf of a client.
Hospitalizations and emergency department visits decreased in the period after engaging with a recovery coach.
After engaging with a recovery coach, there was a significant decrease in the percentage of patients hospitalized from the 6-month pre-period (41%) to the 6-month post-period (23%). There was also a significant decrease in the total number of hospitalizations from the 6-month pre-period (N=869) to the 6-month post-period (N=468).
After engaging with a recovery coach, there was a small nonsignificant decrease in the percentage of patients with emergency department visits from the 6-month pre-period (47%) to the 6-month post-period (43%). There was also a small, nonsignificant decrease in the total number of emergency department visits from the 6-month pre-period (N=4,158) to the 6-month post-period (N=4,057).
Outpatient appointments increased in the period after engaging with a recovery coach.
After engaging with a recovery coach, there was a significant increase in the percentage of patients with outpatient appointments from the 6-month pre-period (86%) to the 6-month post-period (91%). There was also a significant increase in the total number of outpatient appointments from the 6-month pre-period (N=15,085) to the 6-month post-period (N=24,986).
Across primary care, community health, mental health, and lab visits, there were significant increases in number of encounters and number of patients with that encounter for all services. Notably, the percentage of patients with mental health visits increased from the 6-month pre-period (44%) to the 6-month post-period (56%).
Figure 1.
Meeting with a recovery coach was associated with a greater likelihood of treatment engagement and opioid abstinence during the same month, but not during the following month.
Out of 1,620 patient months aggregated from the 12-month period across the subsample of patients who were prescribed buprenorphine, the rate was significantly higher when patients had coaching contact during the current month (61% vs. 39%) and prior month (52% vs. 42%), compared to the rate of receiving both a buprenorphine prescription and negative toxicology screen in a typical month (44%).
Recovery coach contact was associated with a 1.9-times greater likelihood of treatment engagement and 1.3-times greater likelihood of opioid abstinence during that same month in the 6-month period after recovery coach contact. However, recovery coach contact was not associated with greater odds of treatment engagement or opioid abstinence during the following month in the 6-month period following recovery coach contact.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study offers some early insights about how patients with substance use disorder may fare clinically over time in the 6-month periods before and after meeting engaging with a recovery coach.
Notably, after engaging with a recovery coach, substance use disorder patients had significantly lower rates of hospitalizations and significantly greater rates of outpatient treatment. Despite this, no significant change was observed in emergency department visits, although these did decrease slightly once patients engaged with recovery coaches. These results provide some initial support for the potential benefits of recovery coach contact on reducing the need for more expensive, acute care intensive hospital use and more engagement with more cost-effective outpatient services.
Interestingly, compared to the previous month, patients who were prescribed buprenorphine showed a greater likelihood of buprenorphine engagement and opioid abstinence after meeting with a recovery coach in the current month. However, compared to the previous month, there was no significant difference in buprenorphine engagement or opioid abstinence in the following month after meeting with a recovery coach. Thus, it is possible that patients may be meeting with their recovery coach precisely because they were faring better clinically and not the other way around.
These preliminary findings suggest that peer recovery coaches may serve as a beneficial resource for addiction patients. Specifically, recovery coaches, in facilitating the process of navigating outpatient healthcare services, may reduce the need for more acute care like hospitalization. These promising findings build upon past studies that summarized peer-led recovery support services and evaluated a patient navigator program involving peers in recovery, both of which suggested that meeting with recovery coaches was associated with greater treatment engagement. Further research would help establish best practices for how healthcare systems may incorporate recovery coaches into their treatment programs to better support substance use disorder patients.
However, without a comparison group, it is impossible to establish whether these findings were attributable to the recovery coach program. Also, without patient sample characteristics, it is not possible to know how generalizable these results may be to other patient groups. Therefore, while this study suggests recovery coaches may be helpful to individuals with substance use disorder in a general medical hospital context, further research addressing these limitations is necessary to investigate the specific value and effects of peer recovery coaches at a hospital system level.
Because the study did not include a comparison group of patients without recovery coach contact, these healthcare utilization and buprenorphine treatment outcomes may not be specifically attributable to recovery coaches. This study design limits the conclusions that may be drawn about the specific impact of recovery coach models.
The study did not include demographic data on patient sample characteristics, which made it difficult to know whether these findings would hold up in other patient groups, clinical settings, or healthcare systems. Information on clinical severity or initial recovery-related indicators (e.g., motivation to change, social support, etc.) would allow the researchers to model and control for these variables in order to better isolate the unique positive effects from recovery coaching.
The subsample of patients who were prescribed buprenorphine was small, which limited the study’s ability to detect a significant effect on certain measures like subsequent month engagement.
BOTTOM LINE
This study found that substance use disorder patients in a large hospital system had a lower hospitalization rate and greater rate of outpatient treatment utilization in the 6-month period after meeting with a recovery coach, compared to the same 6-month period before contact. Furthermore, compared to the previous month, patients with SUD who were prescribed buprenorphine showed greater buprenorphine engagement and opioid abstinence in the same month they met with a recovery coach, but did not show differences in buprenorphine engagement and opioid abstinence in the month after meeting with a recovery coach in the following month making it unclear whether recovery coaches actually produce medication engagement benefits.
For individuals and families seeking recovery: Patients with substance use disorder showed some beneficial changes in healthcare utilization and buprenorphine treatment outcomes between the 6-month periods before and after contact with a peer recovery coach, based on electronic healthcare record data collected by a large hospital system. However, this study did not properly test the effectiveness of recovery coach contact on these clinical outcomes. While research on the effects of recovery coaching is ongoing, early findings are promising.
For treatment professionals and treatment systems: This study’s findings suggest that recovery coaches may be a helpful resource for linking substance use disorder patients with outpatient healthcare services, which may reduce the need for intensive and costly acute care. Integrated into a patient’s outpatient management team, recovery coaches may be able to leverage their lived experience to facilitate the process of navigating healthcare services and maintaining treatment engagement. More research is needed to determine the specific effect of recovery coaches on clinical outcomes, which may generalize across patient groups.
For scientists:This study’s findings offer some early support regarding the potential of peer recovery coaches in facilitating beneficial healthcare utilization among patients with substance use disorder. Specifically, there was a significant decrease in hospitalizations, significant increase in outpatient appointments, and nonsignificant decrease in emergency department visits between the 6-month periods before and after initiating contact with a recovery coach. Furthermore, buprenorphine engagement and opioid abstinence were more common with current and prior recovery coach contact, than for the months without contact. However, the lack of a well-matched comparison group limited the ability to determine whether recovery coaching was causally related to the outcomes tested here.
For policy makers: This study’s findings suggest that recovery coach models may facilitate beneficial healthcare utilization, including an increase in outpatient appointments and decrease in hospitalizations. A reduction in the use of acute care would also lead to cost-savings long-term for hospitals and public health systems. However, more research is needed to properly determine the effectiveness of recovery coaches on economic and clinical outcomes. More funding directed to research and program evaluations of peer recovery coaching programs can help determine the utility and potential best practices associated with these growing and popular recovery coaching care models.
In the past few years, state and federal agencies have been expanding recovery coach programs. Recovery coach models have been implemented in state healthcare systems in Vermont and Massachusetts, primary care delivered by the Veterans Administration, and emergency departments all over the country.
A qualitative study showed that recovery coaches can offer social support and help with health system navigation. One systematic review found that recovery coaches may improve patients’ substance use and recovery-related outcomes. While these early studies report that recovery coach models are innovative, popular, and cost-effective, there is little empirical evidence on clinical or cost outcomes. Knowledge of how patients fare when they engage with recovery coaches in clinical settings is not well-established.
In this study, Magidson and colleagues used electronic healthcare record data from a large general hospital system to provide some estimates of how patients fare clinically after engaging with a peer recovery coach.
HOW WAS THIS STUDY CONDUCTED?
This study was an evaluation of the recovery coach program at the Massachusetts General Hospital in Boston, MA. It included 1,171 patients who had their initial coach encounter between January 2015 and September 2017.
The hospital’s recovery coach program employed 1 recovery coach manager and 9 coaches stationed in community health centers, primary care offices, and an outpatient substance use disorder clinic. Recovery coaches were required to be in recovery for at least 2 years and complete a week-long training course on themes like ethics, boundaries, self-care, and motivational interviewing. Coaches provided in-person support to patients in clinical practice settings by accompanying patients to medical appointments, helping to navigate social services, and making connections to community-based recovery support services. Coaches also offered remote support to patients, which involved phone calls or text messages.
To estimate the impact of the coaching program on clinical outcomes, the researchers compared hospitalizations, outpatient appointments, and emergency department visits in the 6-month periods before and after engaging with a recovery coach using patients’ electronic health records.
In terms of outpatient encounters, the researchers examined changes in the type of outpatient encounter among four common types (primary care, community health center, mental health, and laboratory visit).
Among patients who were prescribed buprenorphine (often prescribed in formulation with naloxone and known by the brand name Suboxone) before or within 30 days of their first contact with a recovery coach, the study also assessed buprenorphine engagement and opioid abstinence.
Buprenorphine engagement was based on whether an individual received a buprenorphine prescription in a given month. The researchers also conducted the analyses where buprenorphine engagement was defined as both receiving a prescription and having buprenorphine in their urine toxicology screen to see if defining engagement this way made a difference to analyses.
Opioid abstinence was based on monthly toxicology results extracted from chart review. Patients were considered abstinent in a given month if all toxicology screens were negative for all tested opioids (e.g., heroin, oxycodone, fentanyl, etc.). Patients were considered non-abstinent if: 1) they did not have a toxicology screen in their chart for a given month or 2) they had one or more toxicology screens positive for an opioid. Not exceeding a period of 12 months, patient data was collected from the last buprenorphine prescription or six months before the initial recovery coach contact, then continuing for six months after initial coach contact.
To assess how current-month recovery coach contact was associated with opioid abstinence, researchers compared recovery coach contact with monthly prescription data and negative toxicology screening results with observation beginning on the day the patient initiated coaching and continuing for 6 months. To assess prior-month recovery coach contact, the researchers conducted the same analysis, with observation beginning 30 days after initiated coaching and continuing for 5 months.
It is important to note that the research team focused on recovery coaching engagement and subsequent healthcare utilization. They did not provide any data on patient characteristics (e.g., demographics, substance of choice, treatment history, etc.) in this study.
WHAT DID THIS STUDY FIND?
Patients spent a median of 120 minutes with a coach and contacted a coach an average of 4 times total. Among 1,171 patients who initiated recovery coach contact between January 2015 and September 15, patients were in communication with a coach (first to final contact) over a median duration of 51 days. In terms of communication channel, 50% of patients contacted a coach in person, 44% by phone call with a client, and 6% by phone call on behalf of a client.
Hospitalizations and emergency department visits decreased in the period after engaging with a recovery coach.
After engaging with a recovery coach, there was a significant decrease in the percentage of patients hospitalized from the 6-month pre-period (41%) to the 6-month post-period (23%). There was also a significant decrease in the total number of hospitalizations from the 6-month pre-period (N=869) to the 6-month post-period (N=468).
After engaging with a recovery coach, there was a small nonsignificant decrease in the percentage of patients with emergency department visits from the 6-month pre-period (47%) to the 6-month post-period (43%). There was also a small, nonsignificant decrease in the total number of emergency department visits from the 6-month pre-period (N=4,158) to the 6-month post-period (N=4,057).
Outpatient appointments increased in the period after engaging with a recovery coach.
After engaging with a recovery coach, there was a significant increase in the percentage of patients with outpatient appointments from the 6-month pre-period (86%) to the 6-month post-period (91%). There was also a significant increase in the total number of outpatient appointments from the 6-month pre-period (N=15,085) to the 6-month post-period (N=24,986).
Across primary care, community health, mental health, and lab visits, there were significant increases in number of encounters and number of patients with that encounter for all services. Notably, the percentage of patients with mental health visits increased from the 6-month pre-period (44%) to the 6-month post-period (56%).
Figure 1.
Meeting with a recovery coach was associated with a greater likelihood of treatment engagement and opioid abstinence during the same month, but not during the following month.
Out of 1,620 patient months aggregated from the 12-month period across the subsample of patients who were prescribed buprenorphine, the rate was significantly higher when patients had coaching contact during the current month (61% vs. 39%) and prior month (52% vs. 42%), compared to the rate of receiving both a buprenorphine prescription and negative toxicology screen in a typical month (44%).
Recovery coach contact was associated with a 1.9-times greater likelihood of treatment engagement and 1.3-times greater likelihood of opioid abstinence during that same month in the 6-month period after recovery coach contact. However, recovery coach contact was not associated with greater odds of treatment engagement or opioid abstinence during the following month in the 6-month period following recovery coach contact.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study offers some early insights about how patients with substance use disorder may fare clinically over time in the 6-month periods before and after meeting engaging with a recovery coach.
Notably, after engaging with a recovery coach, substance use disorder patients had significantly lower rates of hospitalizations and significantly greater rates of outpatient treatment. Despite this, no significant change was observed in emergency department visits, although these did decrease slightly once patients engaged with recovery coaches. These results provide some initial support for the potential benefits of recovery coach contact on reducing the need for more expensive, acute care intensive hospital use and more engagement with more cost-effective outpatient services.
Interestingly, compared to the previous month, patients who were prescribed buprenorphine showed a greater likelihood of buprenorphine engagement and opioid abstinence after meeting with a recovery coach in the current month. However, compared to the previous month, there was no significant difference in buprenorphine engagement or opioid abstinence in the following month after meeting with a recovery coach. Thus, it is possible that patients may be meeting with their recovery coach precisely because they were faring better clinically and not the other way around.
These preliminary findings suggest that peer recovery coaches may serve as a beneficial resource for addiction patients. Specifically, recovery coaches, in facilitating the process of navigating outpatient healthcare services, may reduce the need for more acute care like hospitalization. These promising findings build upon past studies that summarized peer-led recovery support services and evaluated a patient navigator program involving peers in recovery, both of which suggested that meeting with recovery coaches was associated with greater treatment engagement. Further research would help establish best practices for how healthcare systems may incorporate recovery coaches into their treatment programs to better support substance use disorder patients.
However, without a comparison group, it is impossible to establish whether these findings were attributable to the recovery coach program. Also, without patient sample characteristics, it is not possible to know how generalizable these results may be to other patient groups. Therefore, while this study suggests recovery coaches may be helpful to individuals with substance use disorder in a general medical hospital context, further research addressing these limitations is necessary to investigate the specific value and effects of peer recovery coaches at a hospital system level.
Because the study did not include a comparison group of patients without recovery coach contact, these healthcare utilization and buprenorphine treatment outcomes may not be specifically attributable to recovery coaches. This study design limits the conclusions that may be drawn about the specific impact of recovery coach models.
The study did not include demographic data on patient sample characteristics, which made it difficult to know whether these findings would hold up in other patient groups, clinical settings, or healthcare systems. Information on clinical severity or initial recovery-related indicators (e.g., motivation to change, social support, etc.) would allow the researchers to model and control for these variables in order to better isolate the unique positive effects from recovery coaching.
The subsample of patients who were prescribed buprenorphine was small, which limited the study’s ability to detect a significant effect on certain measures like subsequent month engagement.
BOTTOM LINE
This study found that substance use disorder patients in a large hospital system had a lower hospitalization rate and greater rate of outpatient treatment utilization in the 6-month period after meeting with a recovery coach, compared to the same 6-month period before contact. Furthermore, compared to the previous month, patients with SUD who were prescribed buprenorphine showed greater buprenorphine engagement and opioid abstinence in the same month they met with a recovery coach, but did not show differences in buprenorphine engagement and opioid abstinence in the month after meeting with a recovery coach in the following month making it unclear whether recovery coaches actually produce medication engagement benefits.
For individuals and families seeking recovery: Patients with substance use disorder showed some beneficial changes in healthcare utilization and buprenorphine treatment outcomes between the 6-month periods before and after contact with a peer recovery coach, based on electronic healthcare record data collected by a large hospital system. However, this study did not properly test the effectiveness of recovery coach contact on these clinical outcomes. While research on the effects of recovery coaching is ongoing, early findings are promising.
For treatment professionals and treatment systems: This study’s findings suggest that recovery coaches may be a helpful resource for linking substance use disorder patients with outpatient healthcare services, which may reduce the need for intensive and costly acute care. Integrated into a patient’s outpatient management team, recovery coaches may be able to leverage their lived experience to facilitate the process of navigating healthcare services and maintaining treatment engagement. More research is needed to determine the specific effect of recovery coaches on clinical outcomes, which may generalize across patient groups.
For scientists:This study’s findings offer some early support regarding the potential of peer recovery coaches in facilitating beneficial healthcare utilization among patients with substance use disorder. Specifically, there was a significant decrease in hospitalizations, significant increase in outpatient appointments, and nonsignificant decrease in emergency department visits between the 6-month periods before and after initiating contact with a recovery coach. Furthermore, buprenorphine engagement and opioid abstinence were more common with current and prior recovery coach contact, than for the months without contact. However, the lack of a well-matched comparison group limited the ability to determine whether recovery coaching was causally related to the outcomes tested here.
For policy makers: This study’s findings suggest that recovery coach models may facilitate beneficial healthcare utilization, including an increase in outpatient appointments and decrease in hospitalizations. A reduction in the use of acute care would also lead to cost-savings long-term for hospitals and public health systems. However, more research is needed to properly determine the effectiveness of recovery coaches on economic and clinical outcomes. More funding directed to research and program evaluations of peer recovery coaching programs can help determine the utility and potential best practices associated with these growing and popular recovery coaching care models.