Large-scale implementation of evidence-based approaches to reduce overdose proves challenging
Clinical trials and naturalistic studies have produced several evidence-based practices for opioid use disorder and overdose risk reduction, but how best to implement these strategies remains an open question. This major NIH-funded study tested large-scale, community-wide interventions for expanding evidence-based practices, and assessed its effects on overdose death rates.
Rates of opioid-related overdose deaths have substantially increased over the last couple of decades. Evidence–basedpractices shown to reduce opioid-related overdose deaths include overdose prevention education, naloxone distribution, use of medication treatments for opioid use disorder like buprenorphine and methadone, and use of safer opioid prescribing and dispensing practices. National associations and government officials have encouraged the use of these evidence-based practices to curb high rates of opioid overdose and associated deaths. However, strategies to implement these practices in real-world settings must address or overcome many barriers include stigmatizing attitudes towards individuals with opioid use disorder, limited options for transportation to medical care, limited access to prescribers of opioid use disorder medication treatment, and limited access to naloxone (i.e. medication that reverses opioid overdose).
Research suggests that comprehensive public-health approaches that increase access and linkage to overdose education, harm-reduction services (e.g., naloxone distribution), and treatment are needed to sufficiently tackle the overdose crisis. Developing new interventions that aim to increase uptake and use of evidence-based practices may ultimately help to reduce high rates of opioid overdose and death. This study developed a new community-based intervention to rapidly increase access to evidence-based practices, and tested its effects on overdose death rates in communities particularly affected by the overdose epidemic.
HOW WAS THIS STUDY CONDUCTED?
This study was a multisite, community-level, randomized controlled trial to evaluate the effects of a community-engaged intervention (i.e. ‘Communities That HEAL’ intervention) on opioid-related overdose death rates among adults. Sixty-seven communities, in 4 states (Kentucky, Massachusetts, New York, Ohio) with a particularly high prevalence of opioid-overdose deaths, participated in the trial.
Communities were randomly assigned to receive the active intervention (n=34 communities) or a wait-list control condition (n=33). An equal number of communities in each state were assigned to the active and control study conditions. Group assignment was also balanced across states, community type (rural vs. urban), baseline overdose rates, and community population size. All of these variables were also controlled for in the study analyses.
The ‘Communities That HEAL’ intervention was developed as part of the ‘HEALing (Helping to End Addiction Long-term Initiative) Communities Study’, a large-scale study funded by the National Institutes of Health that aims to establish best practices for community adoption/integration of addiction prevention and treatment strategies. The intervention was adapted from the ‘Communities That Care’ intervention, which is shown to help communities with implementing evidence-based practices to prevent youth substance use. Intervention development was informed by community members who had lived experience with opioid use disorder or who had experience working with individuals with opioid use disorder. Local community data was used to assess gaps in, and resources for, increasing the delivery and use of evidence-based practices for preventing overdose death. The goal of the intervention was to rapidly increase community access to evidence-based practices to reduce overdose death rates.
The intervention consisted of community-based health communication campaigns (6 objectives) and efforts to expand implementation of evidence-based practices (4 objectives).
Health communication campaigns aimed to:
1. Increase availability/access to overdose education and naloxone (opioid overdose reversal drug) distribution
2. Increase availability/access to medications for opioid use disorder treatment
3. Increase treatment retention
4. Increase access to recovery support services
5. Improve prescription opioid safety
6. Reduce stigma with stigma-reduction messages (via print/digital, radio, outdoor adverts, & social media)
Efforts to expand implementation of evidence-based practices aimed to:
1. Increase delivery of overdose education and naloxone distribution (e.g., active delivery of overdose education and naloxone distribution at venues with high-risk populations)
2. Increase delivery of opioid use disorder medication treatments, including buprenorphine and methadone (e.g., enhancing public treatment delivery approaches, expanding treatment availability in criminal justice settings)
3. Identify and engage high-risk populations in overdose education, naloxone distribution, and medication treatment (e.g., creating new record systems for high-risk populations, new programs for linkage to treatment/recovery services)
4. Improve prescription opioid safety (e.g., safe prescription drug disposal programs, new practices for prescribing opioids for chronic pain)
As part of the intervention, communities were given funds to implement health communication campaigns and evidence-based strategies for expanding evidence-based practices. The average funds given to each community ranged from $672,000 to $1.72 million, depending on their needs and population size affected by overdose.
The intervention was delivered over 2.5 years (January 2020 – June 2022), but most intervention activities occurred after September 2020, due to COVID-related public health constraints (e.g., physical distancing guidelines). Communities assigned to the active intervention newly implemented a total of 165 communication campaigns and 615 evidence-based practice strategies within the 2.5-year study period. Of the evidence-based practice strategies implemented, 41% of strategies involved overdose education and naloxone distribution, 42% involved the use of opioid use disorder medication treatment, and 17% involved safer opioid prescribing practices.
Outcomes were assessed for group differences between communities in the active intervention and control groups, over a 12-month period (July 2021 – June 2022) when the majority of the intervention strategies were implemented (38% implemented prior to July 2021). Baseline rates were assessed as the average rate in a given community over a 2-year period just prior to intervention implementation.
The primary outcome was the number of opioid-related overdose deaths per 100,000 adults in each community, averaged across communities. Overdose deaths were determined via death certificates that indicated opioid overdose as an underlying cause of death.
Because death certificates can take up to 11 months to process, the researchers also examined rates of opioid-overdose-related emergency medical service runs, which become available after a much shorter period of time (within 3 months). This data was used to measure: (1) the average number of emergency medical service runs for suspected opioid overdoses that occurred per 1,000 residents in each community; (2) the total number of times a community’s monthly rate of emergency service runs increased compared to its average rate in the prior 3 months: more than 3 standard deviations (moderate increase) or 4 standard deviations (severe increase).
Assessed communities were primarily urban (70%) with a collective population of 8.2 million adults. Communities included 48 counties and 19 municipalities or rural clusters of municipalities across the 4 states.
WHAT DID THIS STUDY FIND?
The intervention did not significantly reduce overdose death rates in the initial year of its implementation
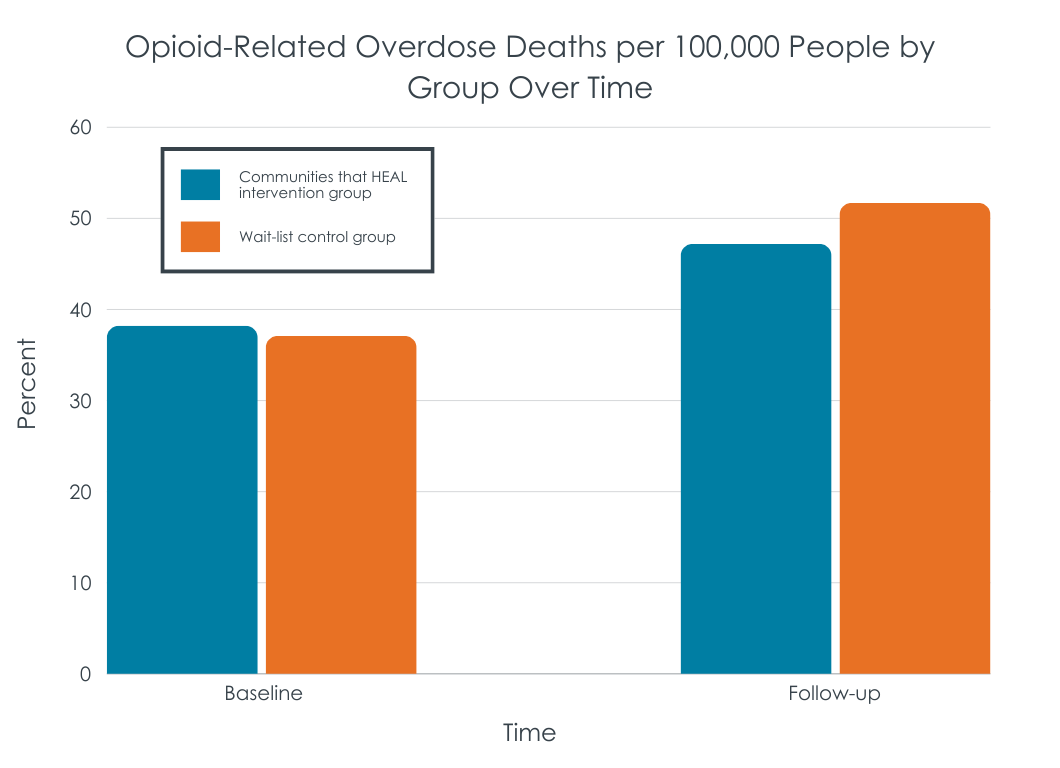
The average rate of opioid-related overdose deaths was similar in the intervention and control groups before the community-based intervention began (see figure below). During the first year of intervention implementation, overdose deaths increased across both study groups, which did not significantly differ despite death rates being slightly lower in the active intervention group than the control group.
The intervention did not significantly affect rates of overdose-related emergency medical service runs
Though the intervention group showed slightly lower average community rates of emergency medical service runs for suspected opioid overdoses, the intervention and control groups did not significantly differ in the research analyses. Similar results were seen for the occurrence of moderate and severe increases in service runs for suspected opioid overdoses.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study investigated the impact of an ongoing community-based intervention on rates of opioid-related overdose deaths in communities that have been particularly affected by the overdose epidemic. Results suggest that community-based interventions like this one may not be enough to sufficiently curb the overdose epidemic, at least not in the initial stages of implementation. Though overdose death rates were slightly lower in communities that received the intervention, these rates were not low enough to be significantly different from death rates in control communities.
There are many possible reasons why the intervention did not have a significant effect on overdose death rates. First, outcomes were assessed while the majority of the intervention strategies were still being implemented – only 38% of the intervention strategies were conducted prior to the study follow-up period. Only about 10 months had passed between the start of intervention implementation and evaluation of outcomes within a given community. Second, this intervention began 2 months prior to the nationwide COVID public health emergency, which disrupted and delayed efforts to implement evidence-based practices in communities. A slow start to intervention implementation meant that the duration of service implementation and delivery prior to follow-up was curtailed. Interventions can take time to yield an observable effect in the real world and more time may therefore be needed to determine the efficacy of the ‘Communities That HEAL’ intervention. Implementing strategies for evidence-based practices can involve hiring new staff, changing clinical practice operations, and developing collaborations to get new services up and running. The intervention that this study was based on (the ‘Communities That Care’ intervention for youth) yielded positive outcomes 3 years after its implementation. Thus, not enough time may have passed for the current study’s community-based strategies to take full effect. Simulated models predict that such efforts to reduce overdose death rates could take up to 10 years to show an observable effect.
Third, fentanyl and xylazine also became more prevalent in the drug supply during the study period. These substances pose new challenges for opioid overdose prevention and treatment. Fentanyl is a highly potent opioid with increased risk for overdose relative to other opioids like heroin and prescription opioids. In addition, Xylazine is a non-opioid sedative that is becoming increasingly more common in the opioid drug supply as an adulterant and does not respond to the opioid overdose reversal drug, naloxone. Community-based efforts to curb the overdose epidemic did not focus on addressing this rise in fentanyl or xylazine related overdoses and this may have hampered the overall effect of the intervention on overdose rates.
The COVID pandemic was also a time of isolation and increased vulnerability for many individuals with substance use disorders and overdose rates increased during this time, as was reflected in increased overdose death rates seen here across the intervention and control groups. The increase in overdoses during this time was not uniform across states. Public funds became more available in response to increased overdose deaths during the pandemic, which may have allowed control communities to implement evidence-based practices, which would have reduced observable differences between the intervention and control groups. The number of people who accessed evidence-based services as part of this study, and outside of this study, was not examined here, calling for additional longitudinal research to determine the scope and magnitude of the effect of community-based interventions on opioid-related overdose death rates.
This study only assessed data from 4 US states and the intervention’s effects may not translate to communities in other states and countries.
This intervention was partially implemented during the COVID pandemic in 2020, when overdose rates increased and fentanyl became more prevalent in the opioid drug supply, and it is unclear how this impacted the study data or outcomes of the intervention.
The majority (62%) of the intervention strategies were implemented in communities during the follow-up period assessed (July 2021 – June 2022). The intervention’s impact beyond the early stages of implementation needs to be assessed to better understand the full extent of its short- and long-term effects.
BOTTOM LINE
The ‘Communities That HEAL’ intervention mobilized communities to implement over 600 evidence-based practices for reducing/preventing opioid-related overdose deaths. Though the intervention group had marginally lower rates of overdose death approximately 12 months after intervention implementation, differences between the intervention and control group were not large enough to yield a significant effect. More time between the implementation of community-based interventions and evaluation of outcomes may be needed for new strategies to become established, gain traction, and have a substantial positive impact on the community population. Additional efforts might also be required to address overdose amid changes in drug supply and drug use patterns (e.g., increased rates of fentanyl and xylazine in the opioid drug supply and increased deaths due to smoking drugs as opposed to injecting them).
For individuals and families seeking recovery: Opioid-related overdose deaths continue to rise and expanding access to evidence-based practices like naloxone for overdose reversal and medication treatment for opioid use disorder can help prevent overdose deaths. Though community-based interventions that aim to expand access to these services can take time to have an observable effect on the communities they target, efforts like this are necessary to help curb the overdose epidemic. Individuals who use drugs are encouraged to talk to their doctors and local community providers to obtain information on naloxone, medication treatment, and other services that can help them avoid overdose and prevent death.
For treatment professionals and treatment systems: This study helps us better understand the impact of community efforts on preventing opioid-related overdose deaths, which can ultimately help inform public health efforts and better address the overdose epidemic. Though this community intervention did not significantly affect death rates, possibly because not enough time had passed before outcomes were assessed, it did help expand the number of services available to help prevent overdose (e.g., naloxone distribution, medication treatment access). Healthcare initiatives that help expand access to these services are shown to be effective in other studies and are needed to help reduce drug-related harms and prevent overdose deaths in the long run.
For scientists: Additional research is needed to develop and test community-based interventions that expand access to evidence-based practices, and to assess their impact on overdose death rates. National studies representing all states and territories with longer follow-up periods are needed to obtain an accurate understanding of the impact of community interventions on overdose death prevalence across the United States and outside of the context of the Covid pandemic. Given changes in drug supply and opioid use patterns since this study was conducted (e.g., increased rates of fentanyl/xylazine involved deaths), additional development and evaluation of intervention components that address these shifts are needed. Prospective investigations evaluating the impact of such interventions on additional community and individual outcomes beyond overdose death are also warranted.
For policy makers: As opioid overdose death rates continue to remain high, novel community-based approaches to address the overdose epidemic are needed. Expanding access to overdose education and services scientifically shown to prevent or reduce overdose are essential. Given that this study experienced COVID-related setbacks and evaluated outcomes only 10-12 months after intervention implementation, research examining these effects over a longer period of time may help inform local, state, and federal policy decisions.
Rates of opioid-related overdose deaths have substantially increased over the last couple of decades. Evidence–basedpractices shown to reduce opioid-related overdose deaths include overdose prevention education, naloxone distribution, use of medication treatments for opioid use disorder like buprenorphine and methadone, and use of safer opioid prescribing and dispensing practices. National associations and government officials have encouraged the use of these evidence-based practices to curb high rates of opioid overdose and associated deaths. However, strategies to implement these practices in real-world settings must address or overcome many barriers include stigmatizing attitudes towards individuals with opioid use disorder, limited options for transportation to medical care, limited access to prescribers of opioid use disorder medication treatment, and limited access to naloxone (i.e. medication that reverses opioid overdose).
Research suggests that comprehensive public-health approaches that increase access and linkage to overdose education, harm-reduction services (e.g., naloxone distribution), and treatment are needed to sufficiently tackle the overdose crisis. Developing new interventions that aim to increase uptake and use of evidence-based practices may ultimately help to reduce high rates of opioid overdose and death. This study developed a new community-based intervention to rapidly increase access to evidence-based practices, and tested its effects on overdose death rates in communities particularly affected by the overdose epidemic.
HOW WAS THIS STUDY CONDUCTED?
This study was a multisite, community-level, randomized controlled trial to evaluate the effects of a community-engaged intervention (i.e. ‘Communities That HEAL’ intervention) on opioid-related overdose death rates among adults. Sixty-seven communities, in 4 states (Kentucky, Massachusetts, New York, Ohio) with a particularly high prevalence of opioid-overdose deaths, participated in the trial.
Communities were randomly assigned to receive the active intervention (n=34 communities) or a wait-list control condition (n=33). An equal number of communities in each state were assigned to the active and control study conditions. Group assignment was also balanced across states, community type (rural vs. urban), baseline overdose rates, and community population size. All of these variables were also controlled for in the study analyses.
The ‘Communities That HEAL’ intervention was developed as part of the ‘HEALing (Helping to End Addiction Long-term Initiative) Communities Study’, a large-scale study funded by the National Institutes of Health that aims to establish best practices for community adoption/integration of addiction prevention and treatment strategies. The intervention was adapted from the ‘Communities That Care’ intervention, which is shown to help communities with implementing evidence-based practices to prevent youth substance use. Intervention development was informed by community members who had lived experience with opioid use disorder or who had experience working with individuals with opioid use disorder. Local community data was used to assess gaps in, and resources for, increasing the delivery and use of evidence-based practices for preventing overdose death. The goal of the intervention was to rapidly increase community access to evidence-based practices to reduce overdose death rates.
The intervention consisted of community-based health communication campaigns (6 objectives) and efforts to expand implementation of evidence-based practices (4 objectives).
Health communication campaigns aimed to:
1. Increase availability/access to overdose education and naloxone (opioid overdose reversal drug) distribution
2. Increase availability/access to medications for opioid use disorder treatment
3. Increase treatment retention
4. Increase access to recovery support services
5. Improve prescription opioid safety
6. Reduce stigma with stigma-reduction messages (via print/digital, radio, outdoor adverts, & social media)
Efforts to expand implementation of evidence-based practices aimed to:
1. Increase delivery of overdose education and naloxone distribution (e.g., active delivery of overdose education and naloxone distribution at venues with high-risk populations)
2. Increase delivery of opioid use disorder medication treatments, including buprenorphine and methadone (e.g., enhancing public treatment delivery approaches, expanding treatment availability in criminal justice settings)
3. Identify and engage high-risk populations in overdose education, naloxone distribution, and medication treatment (e.g., creating new record systems for high-risk populations, new programs for linkage to treatment/recovery services)
4. Improve prescription opioid safety (e.g., safe prescription drug disposal programs, new practices for prescribing opioids for chronic pain)
As part of the intervention, communities were given funds to implement health communication campaigns and evidence-based strategies for expanding evidence-based practices. The average funds given to each community ranged from $672,000 to $1.72 million, depending on their needs and population size affected by overdose.
The intervention was delivered over 2.5 years (January 2020 – June 2022), but most intervention activities occurred after September 2020, due to COVID-related public health constraints (e.g., physical distancing guidelines). Communities assigned to the active intervention newly implemented a total of 165 communication campaigns and 615 evidence-based practice strategies within the 2.5-year study period. Of the evidence-based practice strategies implemented, 41% of strategies involved overdose education and naloxone distribution, 42% involved the use of opioid use disorder medication treatment, and 17% involved safer opioid prescribing practices.
Outcomes were assessed for group differences between communities in the active intervention and control groups, over a 12-month period (July 2021 – June 2022) when the majority of the intervention strategies were implemented (38% implemented prior to July 2021). Baseline rates were assessed as the average rate in a given community over a 2-year period just prior to intervention implementation.
The primary outcome was the number of opioid-related overdose deaths per 100,000 adults in each community, averaged across communities. Overdose deaths were determined via death certificates that indicated opioid overdose as an underlying cause of death.
Because death certificates can take up to 11 months to process, the researchers also examined rates of opioid-overdose-related emergency medical service runs, which become available after a much shorter period of time (within 3 months). This data was used to measure: (1) the average number of emergency medical service runs for suspected opioid overdoses that occurred per 1,000 residents in each community; (2) the total number of times a community’s monthly rate of emergency service runs increased compared to its average rate in the prior 3 months: more than 3 standard deviations (moderate increase) or 4 standard deviations (severe increase).
Assessed communities were primarily urban (70%) with a collective population of 8.2 million adults. Communities included 48 counties and 19 municipalities or rural clusters of municipalities across the 4 states.
WHAT DID THIS STUDY FIND?
The intervention did not significantly reduce overdose death rates in the initial year of its implementation
The average rate of opioid-related overdose deaths was similar in the intervention and control groups before the community-based intervention began (see figure below). During the first year of intervention implementation, overdose deaths increased across both study groups, which did not significantly differ despite death rates being slightly lower in the active intervention group than the control group.
The intervention did not significantly affect rates of overdose-related emergency medical service runs
Though the intervention group showed slightly lower average community rates of emergency medical service runs for suspected opioid overdoses, the intervention and control groups did not significantly differ in the research analyses. Similar results were seen for the occurrence of moderate and severe increases in service runs for suspected opioid overdoses.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study investigated the impact of an ongoing community-based intervention on rates of opioid-related overdose deaths in communities that have been particularly affected by the overdose epidemic. Results suggest that community-based interventions like this one may not be enough to sufficiently curb the overdose epidemic, at least not in the initial stages of implementation. Though overdose death rates were slightly lower in communities that received the intervention, these rates were not low enough to be significantly different from death rates in control communities.
There are many possible reasons why the intervention did not have a significant effect on overdose death rates. First, outcomes were assessed while the majority of the intervention strategies were still being implemented – only 38% of the intervention strategies were conducted prior to the study follow-up period. Only about 10 months had passed between the start of intervention implementation and evaluation of outcomes within a given community. Second, this intervention began 2 months prior to the nationwide COVID public health emergency, which disrupted and delayed efforts to implement evidence-based practices in communities. A slow start to intervention implementation meant that the duration of service implementation and delivery prior to follow-up was curtailed. Interventions can take time to yield an observable effect in the real world and more time may therefore be needed to determine the efficacy of the ‘Communities That HEAL’ intervention. Implementing strategies for evidence-based practices can involve hiring new staff, changing clinical practice operations, and developing collaborations to get new services up and running. The intervention that this study was based on (the ‘Communities That Care’ intervention for youth) yielded positive outcomes 3 years after its implementation. Thus, not enough time may have passed for the current study’s community-based strategies to take full effect. Simulated models predict that such efforts to reduce overdose death rates could take up to 10 years to show an observable effect.
Third, fentanyl and xylazine also became more prevalent in the drug supply during the study period. These substances pose new challenges for opioid overdose prevention and treatment. Fentanyl is a highly potent opioid with increased risk for overdose relative to other opioids like heroin and prescription opioids. In addition, Xylazine is a non-opioid sedative that is becoming increasingly more common in the opioid drug supply as an adulterant and does not respond to the opioid overdose reversal drug, naloxone. Community-based efforts to curb the overdose epidemic did not focus on addressing this rise in fentanyl or xylazine related overdoses and this may have hampered the overall effect of the intervention on overdose rates.
The COVID pandemic was also a time of isolation and increased vulnerability for many individuals with substance use disorders and overdose rates increased during this time, as was reflected in increased overdose death rates seen here across the intervention and control groups. The increase in overdoses during this time was not uniform across states. Public funds became more available in response to increased overdose deaths during the pandemic, which may have allowed control communities to implement evidence-based practices, which would have reduced observable differences between the intervention and control groups. The number of people who accessed evidence-based services as part of this study, and outside of this study, was not examined here, calling for additional longitudinal research to determine the scope and magnitude of the effect of community-based interventions on opioid-related overdose death rates.
This study only assessed data from 4 US states and the intervention’s effects may not translate to communities in other states and countries.
This intervention was partially implemented during the COVID pandemic in 2020, when overdose rates increased and fentanyl became more prevalent in the opioid drug supply, and it is unclear how this impacted the study data or outcomes of the intervention.
The majority (62%) of the intervention strategies were implemented in communities during the follow-up period assessed (July 2021 – June 2022). The intervention’s impact beyond the early stages of implementation needs to be assessed to better understand the full extent of its short- and long-term effects.
BOTTOM LINE
The ‘Communities That HEAL’ intervention mobilized communities to implement over 600 evidence-based practices for reducing/preventing opioid-related overdose deaths. Though the intervention group had marginally lower rates of overdose death approximately 12 months after intervention implementation, differences between the intervention and control group were not large enough to yield a significant effect. More time between the implementation of community-based interventions and evaluation of outcomes may be needed for new strategies to become established, gain traction, and have a substantial positive impact on the community population. Additional efforts might also be required to address overdose amid changes in drug supply and drug use patterns (e.g., increased rates of fentanyl and xylazine in the opioid drug supply and increased deaths due to smoking drugs as opposed to injecting them).
For individuals and families seeking recovery: Opioid-related overdose deaths continue to rise and expanding access to evidence-based practices like naloxone for overdose reversal and medication treatment for opioid use disorder can help prevent overdose deaths. Though community-based interventions that aim to expand access to these services can take time to have an observable effect on the communities they target, efforts like this are necessary to help curb the overdose epidemic. Individuals who use drugs are encouraged to talk to their doctors and local community providers to obtain information on naloxone, medication treatment, and other services that can help them avoid overdose and prevent death.
For treatment professionals and treatment systems: This study helps us better understand the impact of community efforts on preventing opioid-related overdose deaths, which can ultimately help inform public health efforts and better address the overdose epidemic. Though this community intervention did not significantly affect death rates, possibly because not enough time had passed before outcomes were assessed, it did help expand the number of services available to help prevent overdose (e.g., naloxone distribution, medication treatment access). Healthcare initiatives that help expand access to these services are shown to be effective in other studies and are needed to help reduce drug-related harms and prevent overdose deaths in the long run.
For scientists: Additional research is needed to develop and test community-based interventions that expand access to evidence-based practices, and to assess their impact on overdose death rates. National studies representing all states and territories with longer follow-up periods are needed to obtain an accurate understanding of the impact of community interventions on overdose death prevalence across the United States and outside of the context of the Covid pandemic. Given changes in drug supply and opioid use patterns since this study was conducted (e.g., increased rates of fentanyl/xylazine involved deaths), additional development and evaluation of intervention components that address these shifts are needed. Prospective investigations evaluating the impact of such interventions on additional community and individual outcomes beyond overdose death are also warranted.
For policy makers: As opioid overdose death rates continue to remain high, novel community-based approaches to address the overdose epidemic are needed. Expanding access to overdose education and services scientifically shown to prevent or reduce overdose are essential. Given that this study experienced COVID-related setbacks and evaluated outcomes only 10-12 months after intervention implementation, research examining these effects over a longer period of time may help inform local, state, and federal policy decisions.
Rates of opioid-related overdose deaths have substantially increased over the last couple of decades. Evidence–basedpractices shown to reduce opioid-related overdose deaths include overdose prevention education, naloxone distribution, use of medication treatments for opioid use disorder like buprenorphine and methadone, and use of safer opioid prescribing and dispensing practices. National associations and government officials have encouraged the use of these evidence-based practices to curb high rates of opioid overdose and associated deaths. However, strategies to implement these practices in real-world settings must address or overcome many barriers include stigmatizing attitudes towards individuals with opioid use disorder, limited options for transportation to medical care, limited access to prescribers of opioid use disorder medication treatment, and limited access to naloxone (i.e. medication that reverses opioid overdose).
Research suggests that comprehensive public-health approaches that increase access and linkage to overdose education, harm-reduction services (e.g., naloxone distribution), and treatment are needed to sufficiently tackle the overdose crisis. Developing new interventions that aim to increase uptake and use of evidence-based practices may ultimately help to reduce high rates of opioid overdose and death. This study developed a new community-based intervention to rapidly increase access to evidence-based practices, and tested its effects on overdose death rates in communities particularly affected by the overdose epidemic.
HOW WAS THIS STUDY CONDUCTED?
This study was a multisite, community-level, randomized controlled trial to evaluate the effects of a community-engaged intervention (i.e. ‘Communities That HEAL’ intervention) on opioid-related overdose death rates among adults. Sixty-seven communities, in 4 states (Kentucky, Massachusetts, New York, Ohio) with a particularly high prevalence of opioid-overdose deaths, participated in the trial.
Communities were randomly assigned to receive the active intervention (n=34 communities) or a wait-list control condition (n=33). An equal number of communities in each state were assigned to the active and control study conditions. Group assignment was also balanced across states, community type (rural vs. urban), baseline overdose rates, and community population size. All of these variables were also controlled for in the study analyses.
The ‘Communities That HEAL’ intervention was developed as part of the ‘HEALing (Helping to End Addiction Long-term Initiative) Communities Study’, a large-scale study funded by the National Institutes of Health that aims to establish best practices for community adoption/integration of addiction prevention and treatment strategies. The intervention was adapted from the ‘Communities That Care’ intervention, which is shown to help communities with implementing evidence-based practices to prevent youth substance use. Intervention development was informed by community members who had lived experience with opioid use disorder or who had experience working with individuals with opioid use disorder. Local community data was used to assess gaps in, and resources for, increasing the delivery and use of evidence-based practices for preventing overdose death. The goal of the intervention was to rapidly increase community access to evidence-based practices to reduce overdose death rates.
The intervention consisted of community-based health communication campaigns (6 objectives) and efforts to expand implementation of evidence-based practices (4 objectives).
Health communication campaigns aimed to:
1. Increase availability/access to overdose education and naloxone (opioid overdose reversal drug) distribution
2. Increase availability/access to medications for opioid use disorder treatment
3. Increase treatment retention
4. Increase access to recovery support services
5. Improve prescription opioid safety
6. Reduce stigma with stigma-reduction messages (via print/digital, radio, outdoor adverts, & social media)
Efforts to expand implementation of evidence-based practices aimed to:
1. Increase delivery of overdose education and naloxone distribution (e.g., active delivery of overdose education and naloxone distribution at venues with high-risk populations)
2. Increase delivery of opioid use disorder medication treatments, including buprenorphine and methadone (e.g., enhancing public treatment delivery approaches, expanding treatment availability in criminal justice settings)
3. Identify and engage high-risk populations in overdose education, naloxone distribution, and medication treatment (e.g., creating new record systems for high-risk populations, new programs for linkage to treatment/recovery services)
4. Improve prescription opioid safety (e.g., safe prescription drug disposal programs, new practices for prescribing opioids for chronic pain)
As part of the intervention, communities were given funds to implement health communication campaigns and evidence-based strategies for expanding evidence-based practices. The average funds given to each community ranged from $672,000 to $1.72 million, depending on their needs and population size affected by overdose.
The intervention was delivered over 2.5 years (January 2020 – June 2022), but most intervention activities occurred after September 2020, due to COVID-related public health constraints (e.g., physical distancing guidelines). Communities assigned to the active intervention newly implemented a total of 165 communication campaigns and 615 evidence-based practice strategies within the 2.5-year study period. Of the evidence-based practice strategies implemented, 41% of strategies involved overdose education and naloxone distribution, 42% involved the use of opioid use disorder medication treatment, and 17% involved safer opioid prescribing practices.
Outcomes were assessed for group differences between communities in the active intervention and control groups, over a 12-month period (July 2021 – June 2022) when the majority of the intervention strategies were implemented (38% implemented prior to July 2021). Baseline rates were assessed as the average rate in a given community over a 2-year period just prior to intervention implementation.
The primary outcome was the number of opioid-related overdose deaths per 100,000 adults in each community, averaged across communities. Overdose deaths were determined via death certificates that indicated opioid overdose as an underlying cause of death.
Because death certificates can take up to 11 months to process, the researchers also examined rates of opioid-overdose-related emergency medical service runs, which become available after a much shorter period of time (within 3 months). This data was used to measure: (1) the average number of emergency medical service runs for suspected opioid overdoses that occurred per 1,000 residents in each community; (2) the total number of times a community’s monthly rate of emergency service runs increased compared to its average rate in the prior 3 months: more than 3 standard deviations (moderate increase) or 4 standard deviations (severe increase).
Assessed communities were primarily urban (70%) with a collective population of 8.2 million adults. Communities included 48 counties and 19 municipalities or rural clusters of municipalities across the 4 states.
WHAT DID THIS STUDY FIND?
The intervention did not significantly reduce overdose death rates in the initial year of its implementation
The average rate of opioid-related overdose deaths was similar in the intervention and control groups before the community-based intervention began (see figure below). During the first year of intervention implementation, overdose deaths increased across both study groups, which did not significantly differ despite death rates being slightly lower in the active intervention group than the control group.
The intervention did not significantly affect rates of overdose-related emergency medical service runs
Though the intervention group showed slightly lower average community rates of emergency medical service runs for suspected opioid overdoses, the intervention and control groups did not significantly differ in the research analyses. Similar results were seen for the occurrence of moderate and severe increases in service runs for suspected opioid overdoses.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study investigated the impact of an ongoing community-based intervention on rates of opioid-related overdose deaths in communities that have been particularly affected by the overdose epidemic. Results suggest that community-based interventions like this one may not be enough to sufficiently curb the overdose epidemic, at least not in the initial stages of implementation. Though overdose death rates were slightly lower in communities that received the intervention, these rates were not low enough to be significantly different from death rates in control communities.
There are many possible reasons why the intervention did not have a significant effect on overdose death rates. First, outcomes were assessed while the majority of the intervention strategies were still being implemented – only 38% of the intervention strategies were conducted prior to the study follow-up period. Only about 10 months had passed between the start of intervention implementation and evaluation of outcomes within a given community. Second, this intervention began 2 months prior to the nationwide COVID public health emergency, which disrupted and delayed efforts to implement evidence-based practices in communities. A slow start to intervention implementation meant that the duration of service implementation and delivery prior to follow-up was curtailed. Interventions can take time to yield an observable effect in the real world and more time may therefore be needed to determine the efficacy of the ‘Communities That HEAL’ intervention. Implementing strategies for evidence-based practices can involve hiring new staff, changing clinical practice operations, and developing collaborations to get new services up and running. The intervention that this study was based on (the ‘Communities That Care’ intervention for youth) yielded positive outcomes 3 years after its implementation. Thus, not enough time may have passed for the current study’s community-based strategies to take full effect. Simulated models predict that such efforts to reduce overdose death rates could take up to 10 years to show an observable effect.
Third, fentanyl and xylazine also became more prevalent in the drug supply during the study period. These substances pose new challenges for opioid overdose prevention and treatment. Fentanyl is a highly potent opioid with increased risk for overdose relative to other opioids like heroin and prescription opioids. In addition, Xylazine is a non-opioid sedative that is becoming increasingly more common in the opioid drug supply as an adulterant and does not respond to the opioid overdose reversal drug, naloxone. Community-based efforts to curb the overdose epidemic did not focus on addressing this rise in fentanyl or xylazine related overdoses and this may have hampered the overall effect of the intervention on overdose rates.
The COVID pandemic was also a time of isolation and increased vulnerability for many individuals with substance use disorders and overdose rates increased during this time, as was reflected in increased overdose death rates seen here across the intervention and control groups. The increase in overdoses during this time was not uniform across states. Public funds became more available in response to increased overdose deaths during the pandemic, which may have allowed control communities to implement evidence-based practices, which would have reduced observable differences between the intervention and control groups. The number of people who accessed evidence-based services as part of this study, and outside of this study, was not examined here, calling for additional longitudinal research to determine the scope and magnitude of the effect of community-based interventions on opioid-related overdose death rates.
This study only assessed data from 4 US states and the intervention’s effects may not translate to communities in other states and countries.
This intervention was partially implemented during the COVID pandemic in 2020, when overdose rates increased and fentanyl became more prevalent in the opioid drug supply, and it is unclear how this impacted the study data or outcomes of the intervention.
The majority (62%) of the intervention strategies were implemented in communities during the follow-up period assessed (July 2021 – June 2022). The intervention’s impact beyond the early stages of implementation needs to be assessed to better understand the full extent of its short- and long-term effects.
BOTTOM LINE
The ‘Communities That HEAL’ intervention mobilized communities to implement over 600 evidence-based practices for reducing/preventing opioid-related overdose deaths. Though the intervention group had marginally lower rates of overdose death approximately 12 months after intervention implementation, differences between the intervention and control group were not large enough to yield a significant effect. More time between the implementation of community-based interventions and evaluation of outcomes may be needed for new strategies to become established, gain traction, and have a substantial positive impact on the community population. Additional efforts might also be required to address overdose amid changes in drug supply and drug use patterns (e.g., increased rates of fentanyl and xylazine in the opioid drug supply and increased deaths due to smoking drugs as opposed to injecting them).
For individuals and families seeking recovery: Opioid-related overdose deaths continue to rise and expanding access to evidence-based practices like naloxone for overdose reversal and medication treatment for opioid use disorder can help prevent overdose deaths. Though community-based interventions that aim to expand access to these services can take time to have an observable effect on the communities they target, efforts like this are necessary to help curb the overdose epidemic. Individuals who use drugs are encouraged to talk to their doctors and local community providers to obtain information on naloxone, medication treatment, and other services that can help them avoid overdose and prevent death.
For treatment professionals and treatment systems: This study helps us better understand the impact of community efforts on preventing opioid-related overdose deaths, which can ultimately help inform public health efforts and better address the overdose epidemic. Though this community intervention did not significantly affect death rates, possibly because not enough time had passed before outcomes were assessed, it did help expand the number of services available to help prevent overdose (e.g., naloxone distribution, medication treatment access). Healthcare initiatives that help expand access to these services are shown to be effective in other studies and are needed to help reduce drug-related harms and prevent overdose deaths in the long run.
For scientists: Additional research is needed to develop and test community-based interventions that expand access to evidence-based practices, and to assess their impact on overdose death rates. National studies representing all states and territories with longer follow-up periods are needed to obtain an accurate understanding of the impact of community interventions on overdose death prevalence across the United States and outside of the context of the Covid pandemic. Given changes in drug supply and opioid use patterns since this study was conducted (e.g., increased rates of fentanyl/xylazine involved deaths), additional development and evaluation of intervention components that address these shifts are needed. Prospective investigations evaluating the impact of such interventions on additional community and individual outcomes beyond overdose death are also warranted.
For policy makers: As opioid overdose death rates continue to remain high, novel community-based approaches to address the overdose epidemic are needed. Expanding access to overdose education and services scientifically shown to prevent or reduce overdose are essential. Given that this study experienced COVID-related setbacks and evaluated outcomes only 10-12 months after intervention implementation, research examining these effects over a longer period of time may help inform local, state, and federal policy decisions.