Linking detoxification patients to medication treatment prevents overdose death over the long-term
People with opioid use disorder who do not begin medication treatment during, or immediately after, medically supervised detox are at high risk for overdose. However, starting medication treatment during detox is not standard practice in the United States. This study evaluated the long-term effectiveness and cost-effectiveness of initiating medications for opioid use disorder during inpatient detox programs and linking to outpatient medication treatment.
In the United States, the opioid epidemic continues to be deadly, with approximately 128 people dying every day of a related overdose, and economically costly, with an estimated cost of more than $600 billion between 2015 and 2018. Medically supervised detoxification programs (often referred to simply as “detox”) can help address physical and psychological difficulties associated with opioid withdrawal, yet detox alone is not very effective in preventing a return to opioid use or overdose. Nearly 65% of people return to use within 1 month following detox. Further, although the time immediately after detox is associated with increased overdose risk because of a reduced opioid tolerance, only 3% of people follow up with outpatient treatment.
Initiating helpful medications, such as methadone and buprenorphine (i.e., the active ingredient in the more commonly known drug, Suboxone), during detox and linking patients to outpatient medication treatment following detox could reduce the number of patients who return to use or overdose. Further, because detox programs are often one of the first treatment choices for people with opioid use disorder, detox centers can provide a cost-effective means of initiating medication treatment. Few detox centers, however, report offering medications to patients.
This study used computer simulation making use of existing opioid use disorder research to evaluate the long-term effectiveness and cost-effectiveness of initiating medications for opioid use disorder during inpatient detox programs and linking patients to outpatient medication treatment. Studies like these can shed light on the impact of offering medication to patients during detox.
HOW WAS THIS STUDY CONDUCTED?
The research team used simulation modeling to estimate the impact of medication initiation during detox and linkage to outpatient medication treatment on returning to drug use and fatal overdoses, as well as its cost-effectiveness, in Massachusetts. The type of model used allowed the researchers to account for the movement of people with opioid use disorder into the state as well as the development of new cases and people entering treatment, referred to as the “population model.” However, they also modeled it while not allowing for such movement, referred to as the “detox-only model.” More detail on this type of modeling can be found on the study’s website.
The detox-only models simulated 40,000 people admitted to detox, which they followed for 1 year. That is approximately the number of people who enter detox each year in Massachusetts. The population models simulated all people with opioid use disorder in Massachusetts over a ten-year period, where some accessed detox at different times and others never did. In these simulation models, they compared the “standard of care,” where no patients initiated medications during detox or were linked to outpatient medication providers, to offering medications during detox and linking to outpatient medication treatment.
In the models where patients were offered medications during detox, the researchers simulated all patients who entered detox being offered methadone, buprenorphine, or naltrexone, and 78% accepting the offer. Of these, they simulated that 28% chose buprenorphine, 18% chose methadone, and 32% chose naltrexone injection, based on recent research examining patients’ beliefs and preference for each. The researchers also simulated 2 levels of linking to outpatient medication treatment: (1) perfect linkage with 100% of those who initiated medications during detox being linked to outpatient medication treatment, and (2) moderate-linkage where 50% of those who initiated medications during detox being linked to outpatient medication treatment.
Cost-effectiveness was analyzed in the population models only. For these analyses, costs were estimated in 2019 US dollars and were discounted annually at 3% (which is similar to accounting for inflation). Three sources of costs were included: 1) costs of health-care utilization for all services other than opioid use disorder treatment, (2) costs of opioid use disorder treatment, and (3) costs related to overdose. Researchers also estimated the incremental cost-effectiveness ratio, which estimates costs per life-year saved and quality adjusted life-year saved, which adjusts for the burden of an illness or disorder, where one quality adjusted life year equates to one year in good health.
Data for the models were obtained from the Massachusetts Public Health Data Warehouse, which includes administrative records from over 16 agencies across Massachusetts. The researchers also used data from previous studies to obtain information about the natural course of opioid use disorder and quality of life indicators.
WHAT DID THIS STUDY FIND?
Initiating medication in detox and linkages to community treatment improve opioid outcomes for 1 year.
The detox-only models that did not allow for movement into and out of use and treatment and the state showed that initiating medications for the treatment of opioid use disorder during detox and linking patients to outpatient medication treatment is helpful. Specifically, in comparison to no initiation or linkage, the simulation with 100% linkage resulted in a 21.4% decrease in active opioid use, a 334% (i.e., three-fold) increase in outpatient medication treatment, and a 25.1% reduction in fatal overdoses over the course of 1 year.
The 50% linkage simulation resulted in an 11.0% decrease in active use, a 172% increase in outpatient medication treatment, and a 13.1% reduction in fatal overdoses over the course of 1 year.
Among the population, initiating medication in detox and linkages to community treatment improve opioid outcomes for 10 years.
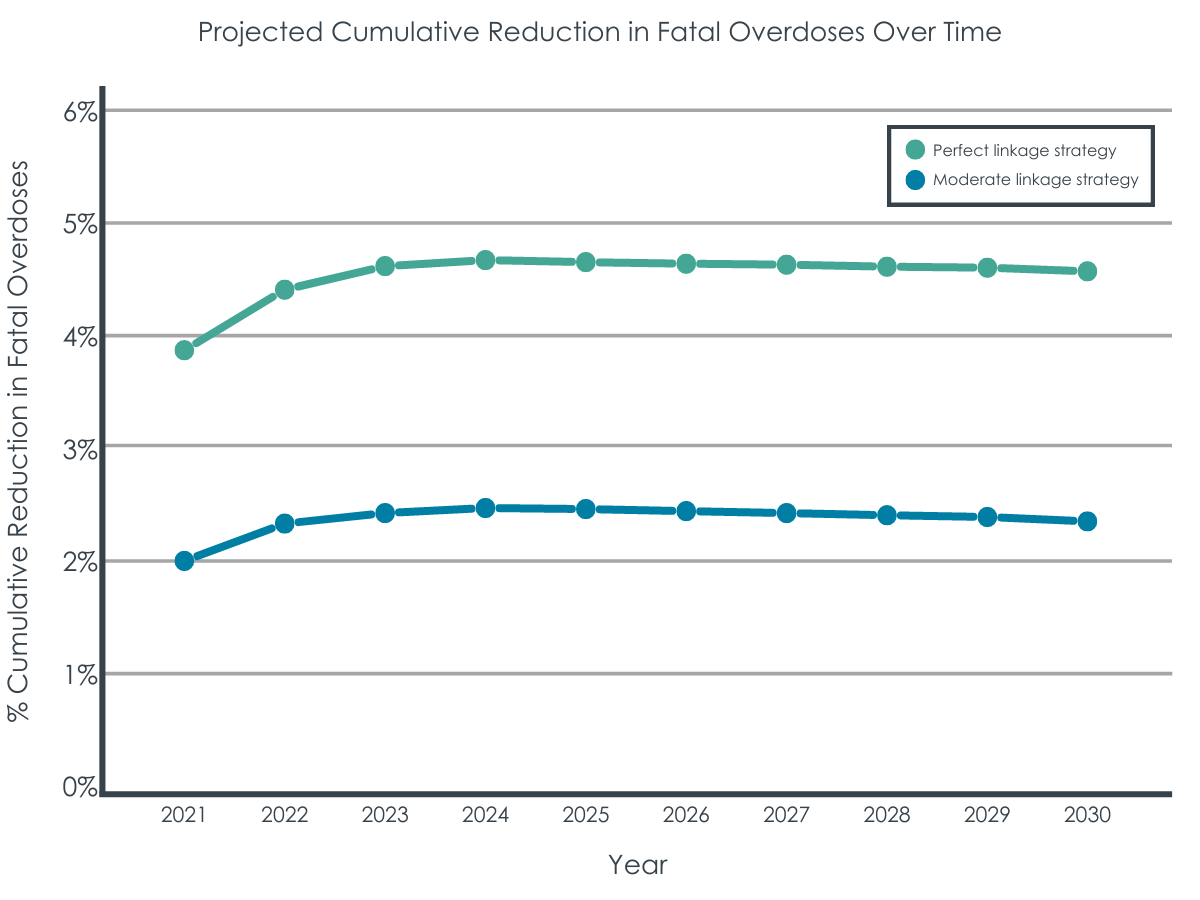
The population models that allowed for movement into and out of use and treatment and the state also showed that initiating medications for the treatment of opioid use disorder during detox and linking patients to outpatient medication treatment is helpful. Specifically, in comparison to no initiation or linkage, the simulation with 100% linkage resulted in a 2.4% decrease in active opioid use, a 26.0% increase in outpatient medication treatment, and prevented 4.5% of fatal overdoses over the course of 10 years.
The 50% linkage simulation resulted 1.2% decrease in active opioid use, a 15.2% increase in outpatient medication treatment, and a 2.3% decrease in fatal overdoses over a 10-year period.
Initiating medication in detox and linkages to community treatment is cost-effective.
In comparison to no initiation or linkage, the simulation with 100% linkage showed that the undiscounted cost of medication initiation and linkage was $629 million dollars over 10 years (i.e., not accounting for inflation). The discounted, incremental cost was $306 million (i.e., accounting for inflation). The incremental cost-effectiveness ratio was $67,600 per life year saved and $55,600 per quality adjusted life year saved.
In comparison to no initiation or linkage, the simulation with 50% linkage showed that the undiscounted cost of medication initiation and linkage was $323 million dollars over 10 years. The discounted, incremental cost was $225 million. The incremental cost-effectiveness ratio was $97,300 per life-years saved and $78,500 per quality adjusted life year saved.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study used simulation modeling to estimate the effectiveness and cost-effectiveness of initiating medications for the treatment of opioid use disorder during detox and linking patients to outpatient medication treatment. In comparison to no medication initiation or linkage, results showed that medication initiation and linkage was helpful at preventing return to drug use and overdose deaths and increasing outpatient treatment.
Medication initiation and linkage through detox centers was also shown to be cost-effective, costing the healthcare sector in Massachusetts approximately $100-$400 per person. This would only require a 0.5-1% increase in the state budget above current spending. This benefit is maximized by delivering the intervention to all eligible detox patients – the cost savings from rationing funding so that only a subset receive the linkage is negligible while the outcomes are half as good.
While the benefits from the population models are more modest, and call into question whether the intervention is worth additional funding, cost-effectiveness analyses like these are important for demonstrating that the ultimate savings from the intervention come from reduced health care and overdose costs. These reductions help to offset the increased costs from funding the medications in the intervention.
Although the study used simulations to estimate the potential impact of medication initiation and linkage, data for the models was drawn from real-world sources and contributes to the growing research base on effective strategies for addressing the opioid epidemic. The results suggest that detox centers can provide a cost-effective place for initiating medications and connecting patients to outpatient medication treatment, which is one strategy that can be an effective part of a larger, comprehensive overdose prevention effort.
The simulation models do not adjust the estimates provided when patients drop out of treatment or die, both of which are likely to occur in real-world scenarios. This could result in the model overestimating the strategy’s effectiveness.
The data used in the simulation models were based on current estimates from Massachusetts. Changes in these trends in the future could affect the estimates of effectiveness and cost-effectiveness, as could using data from other states.
The research team did not have access to data regarding transitions between different medications, so it is unclear if switching medications would affect outcomes.
Because this study involved a simulation, the researchers needed to make several assumptions. For example, they assumed that patients entering detox programs have a high level of interest in medications for treatment, which may or may not be the case. Making different assumptions for the simulations may have resulted in different findings.
This study focused on medication treatment only and did not consider the impact of additional strategies that have been shown to prevent return to drug use, such as harm reduction and recovery support services.
BOTTOM LINE
Results suggest that initiating medications for the treatment of opioid use disorder during detox and linking patients to outpatient medication treatment is a cost-effective strategy for improving and saving lives. It can help reduce overdoses for individuals with opioid use disorder while adding only marginal costs to a state’s substance use budget.
For individuals and families seeking recovery: Initiating medications for the treatment of opioid use disorder during detox and linking patients to outpatient medication treatment may help prevent return to drug use and overdose deaths and increase outpatient treatment engagement that facilitates ongoing use of medications. Accordingly, if individuals with opioid use disorder enter detox and accept medication as part of their treatment, as well as following up with outpatient treatment, they are likely to have better opioid outcomes while reducing risk of overdose. Likewise, families of these individuals are encouraged to support medication treatment during detox and facilitate outpatient treatment following detox.
For treatment professionals and treatment systems: Treatment professionals who work in detox settings may improve patient outcomes by actively linking individuals to community-based treatment that provides FDA-approved opioid use disorder medications. Beyond this, however, return to use and overdose are likely to be further prevented when this strategy is implemented in combination with other efforts, such as connecting patients with recovery peer support and harm reduction.
For scientists: Given that the current study used simulation modeling to estimate the public health benefit of initiating opioid use disorder medication and linkages to community treatment in detox, future research is needed that examines the real-world public health impacts of these interventions. Such research would add to the current findings and shed light on these strategy’s effectiveness and cost-effectiveness when implemented in practice. Further, since the study used data from Massachusetts, future research can also extend the generalizability of the findings to patients in other states.
For policy makers: Supporting policies that promote the availability of medication initiation and linkage as a routine practice could improve and save lives of patients with opioid use disorderwhile adding only modest costs. If such policies were implemented as part of a comprehensive overdose prevention effort, there is likely to be a larger impact with more lives and money saved.
In the United States, the opioid epidemic continues to be deadly, with approximately 128 people dying every day of a related overdose, and economically costly, with an estimated cost of more than $600 billion between 2015 and 2018. Medically supervised detoxification programs (often referred to simply as “detox”) can help address physical and psychological difficulties associated with opioid withdrawal, yet detox alone is not very effective in preventing a return to opioid use or overdose. Nearly 65% of people return to use within 1 month following detox. Further, although the time immediately after detox is associated with increased overdose risk because of a reduced opioid tolerance, only 3% of people follow up with outpatient treatment.
Initiating helpful medications, such as methadone and buprenorphine (i.e., the active ingredient in the more commonly known drug, Suboxone), during detox and linking patients to outpatient medication treatment following detox could reduce the number of patients who return to use or overdose. Further, because detox programs are often one of the first treatment choices for people with opioid use disorder, detox centers can provide a cost-effective means of initiating medication treatment. Few detox centers, however, report offering medications to patients.
This study used computer simulation making use of existing opioid use disorder research to evaluate the long-term effectiveness and cost-effectiveness of initiating medications for opioid use disorder during inpatient detox programs and linking patients to outpatient medication treatment. Studies like these can shed light on the impact of offering medication to patients during detox.
HOW WAS THIS STUDY CONDUCTED?
The research team used simulation modeling to estimate the impact of medication initiation during detox and linkage to outpatient medication treatment on returning to drug use and fatal overdoses, as well as its cost-effectiveness, in Massachusetts. The type of model used allowed the researchers to account for the movement of people with opioid use disorder into the state as well as the development of new cases and people entering treatment, referred to as the “population model.” However, they also modeled it while not allowing for such movement, referred to as the “detox-only model.” More detail on this type of modeling can be found on the study’s website.
The detox-only models simulated 40,000 people admitted to detox, which they followed for 1 year. That is approximately the number of people who enter detox each year in Massachusetts. The population models simulated all people with opioid use disorder in Massachusetts over a ten-year period, where some accessed detox at different times and others never did. In these simulation models, they compared the “standard of care,” where no patients initiated medications during detox or were linked to outpatient medication providers, to offering medications during detox and linking to outpatient medication treatment.
In the models where patients were offered medications during detox, the researchers simulated all patients who entered detox being offered methadone, buprenorphine, or naltrexone, and 78% accepting the offer. Of these, they simulated that 28% chose buprenorphine, 18% chose methadone, and 32% chose naltrexone injection, based on recent research examining patients’ beliefs and preference for each. The researchers also simulated 2 levels of linking to outpatient medication treatment: (1) perfect linkage with 100% of those who initiated medications during detox being linked to outpatient medication treatment, and (2) moderate-linkage where 50% of those who initiated medications during detox being linked to outpatient medication treatment.
Cost-effectiveness was analyzed in the population models only. For these analyses, costs were estimated in 2019 US dollars and were discounted annually at 3% (which is similar to accounting for inflation). Three sources of costs were included: 1) costs of health-care utilization for all services other than opioid use disorder treatment, (2) costs of opioid use disorder treatment, and (3) costs related to overdose. Researchers also estimated the incremental cost-effectiveness ratio, which estimates costs per life-year saved and quality adjusted life-year saved, which adjusts for the burden of an illness or disorder, where one quality adjusted life year equates to one year in good health.
Data for the models were obtained from the Massachusetts Public Health Data Warehouse, which includes administrative records from over 16 agencies across Massachusetts. The researchers also used data from previous studies to obtain information about the natural course of opioid use disorder and quality of life indicators.
WHAT DID THIS STUDY FIND?
Initiating medication in detox and linkages to community treatment improve opioid outcomes for 1 year.
The detox-only models that did not allow for movement into and out of use and treatment and the state showed that initiating medications for the treatment of opioid use disorder during detox and linking patients to outpatient medication treatment is helpful. Specifically, in comparison to no initiation or linkage, the simulation with 100% linkage resulted in a 21.4% decrease in active opioid use, a 334% (i.e., three-fold) increase in outpatient medication treatment, and a 25.1% reduction in fatal overdoses over the course of 1 year.
The 50% linkage simulation resulted in an 11.0% decrease in active use, a 172% increase in outpatient medication treatment, and a 13.1% reduction in fatal overdoses over the course of 1 year.
Among the population, initiating medication in detox and linkages to community treatment improve opioid outcomes for 10 years.
The population models that allowed for movement into and out of use and treatment and the state also showed that initiating medications for the treatment of opioid use disorder during detox and linking patients to outpatient medication treatment is helpful. Specifically, in comparison to no initiation or linkage, the simulation with 100% linkage resulted in a 2.4% decrease in active opioid use, a 26.0% increase in outpatient medication treatment, and prevented 4.5% of fatal overdoses over the course of 10 years.
The 50% linkage simulation resulted 1.2% decrease in active opioid use, a 15.2% increase in outpatient medication treatment, and a 2.3% decrease in fatal overdoses over a 10-year period.
Initiating medication in detox and linkages to community treatment is cost-effective.
In comparison to no initiation or linkage, the simulation with 100% linkage showed that the undiscounted cost of medication initiation and linkage was $629 million dollars over 10 years (i.e., not accounting for inflation). The discounted, incremental cost was $306 million (i.e., accounting for inflation). The incremental cost-effectiveness ratio was $67,600 per life year saved and $55,600 per quality adjusted life year saved.
In comparison to no initiation or linkage, the simulation with 50% linkage showed that the undiscounted cost of medication initiation and linkage was $323 million dollars over 10 years. The discounted, incremental cost was $225 million. The incremental cost-effectiveness ratio was $97,300 per life-years saved and $78,500 per quality adjusted life year saved.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study used simulation modeling to estimate the effectiveness and cost-effectiveness of initiating medications for the treatment of opioid use disorder during detox and linking patients to outpatient medication treatment. In comparison to no medication initiation or linkage, results showed that medication initiation and linkage was helpful at preventing return to drug use and overdose deaths and increasing outpatient treatment.
Medication initiation and linkage through detox centers was also shown to be cost-effective, costing the healthcare sector in Massachusetts approximately $100-$400 per person. This would only require a 0.5-1% increase in the state budget above current spending. This benefit is maximized by delivering the intervention to all eligible detox patients – the cost savings from rationing funding so that only a subset receive the linkage is negligible while the outcomes are half as good.
While the benefits from the population models are more modest, and call into question whether the intervention is worth additional funding, cost-effectiveness analyses like these are important for demonstrating that the ultimate savings from the intervention come from reduced health care and overdose costs. These reductions help to offset the increased costs from funding the medications in the intervention.
Although the study used simulations to estimate the potential impact of medication initiation and linkage, data for the models was drawn from real-world sources and contributes to the growing research base on effective strategies for addressing the opioid epidemic. The results suggest that detox centers can provide a cost-effective place for initiating medications and connecting patients to outpatient medication treatment, which is one strategy that can be an effective part of a larger, comprehensive overdose prevention effort.
The simulation models do not adjust the estimates provided when patients drop out of treatment or die, both of which are likely to occur in real-world scenarios. This could result in the model overestimating the strategy’s effectiveness.
The data used in the simulation models were based on current estimates from Massachusetts. Changes in these trends in the future could affect the estimates of effectiveness and cost-effectiveness, as could using data from other states.
The research team did not have access to data regarding transitions between different medications, so it is unclear if switching medications would affect outcomes.
Because this study involved a simulation, the researchers needed to make several assumptions. For example, they assumed that patients entering detox programs have a high level of interest in medications for treatment, which may or may not be the case. Making different assumptions for the simulations may have resulted in different findings.
This study focused on medication treatment only and did not consider the impact of additional strategies that have been shown to prevent return to drug use, such as harm reduction and recovery support services.
BOTTOM LINE
Results suggest that initiating medications for the treatment of opioid use disorder during detox and linking patients to outpatient medication treatment is a cost-effective strategy for improving and saving lives. It can help reduce overdoses for individuals with opioid use disorder while adding only marginal costs to a state’s substance use budget.
For individuals and families seeking recovery: Initiating medications for the treatment of opioid use disorder during detox and linking patients to outpatient medication treatment may help prevent return to drug use and overdose deaths and increase outpatient treatment engagement that facilitates ongoing use of medications. Accordingly, if individuals with opioid use disorder enter detox and accept medication as part of their treatment, as well as following up with outpatient treatment, they are likely to have better opioid outcomes while reducing risk of overdose. Likewise, families of these individuals are encouraged to support medication treatment during detox and facilitate outpatient treatment following detox.
For treatment professionals and treatment systems: Treatment professionals who work in detox settings may improve patient outcomes by actively linking individuals to community-based treatment that provides FDA-approved opioid use disorder medications. Beyond this, however, return to use and overdose are likely to be further prevented when this strategy is implemented in combination with other efforts, such as connecting patients with recovery peer support and harm reduction.
For scientists: Given that the current study used simulation modeling to estimate the public health benefit of initiating opioid use disorder medication and linkages to community treatment in detox, future research is needed that examines the real-world public health impacts of these interventions. Such research would add to the current findings and shed light on these strategy’s effectiveness and cost-effectiveness when implemented in practice. Further, since the study used data from Massachusetts, future research can also extend the generalizability of the findings to patients in other states.
For policy makers: Supporting policies that promote the availability of medication initiation and linkage as a routine practice could improve and save lives of patients with opioid use disorderwhile adding only modest costs. If such policies were implemented as part of a comprehensive overdose prevention effort, there is likely to be a larger impact with more lives and money saved.
In the United States, the opioid epidemic continues to be deadly, with approximately 128 people dying every day of a related overdose, and economically costly, with an estimated cost of more than $600 billion between 2015 and 2018. Medically supervised detoxification programs (often referred to simply as “detox”) can help address physical and psychological difficulties associated with opioid withdrawal, yet detox alone is not very effective in preventing a return to opioid use or overdose. Nearly 65% of people return to use within 1 month following detox. Further, although the time immediately after detox is associated with increased overdose risk because of a reduced opioid tolerance, only 3% of people follow up with outpatient treatment.
Initiating helpful medications, such as methadone and buprenorphine (i.e., the active ingredient in the more commonly known drug, Suboxone), during detox and linking patients to outpatient medication treatment following detox could reduce the number of patients who return to use or overdose. Further, because detox programs are often one of the first treatment choices for people with opioid use disorder, detox centers can provide a cost-effective means of initiating medication treatment. Few detox centers, however, report offering medications to patients.
This study used computer simulation making use of existing opioid use disorder research to evaluate the long-term effectiveness and cost-effectiveness of initiating medications for opioid use disorder during inpatient detox programs and linking patients to outpatient medication treatment. Studies like these can shed light on the impact of offering medication to patients during detox.
HOW WAS THIS STUDY CONDUCTED?
The research team used simulation modeling to estimate the impact of medication initiation during detox and linkage to outpatient medication treatment on returning to drug use and fatal overdoses, as well as its cost-effectiveness, in Massachusetts. The type of model used allowed the researchers to account for the movement of people with opioid use disorder into the state as well as the development of new cases and people entering treatment, referred to as the “population model.” However, they also modeled it while not allowing for such movement, referred to as the “detox-only model.” More detail on this type of modeling can be found on the study’s website.
The detox-only models simulated 40,000 people admitted to detox, which they followed for 1 year. That is approximately the number of people who enter detox each year in Massachusetts. The population models simulated all people with opioid use disorder in Massachusetts over a ten-year period, where some accessed detox at different times and others never did. In these simulation models, they compared the “standard of care,” where no patients initiated medications during detox or were linked to outpatient medication providers, to offering medications during detox and linking to outpatient medication treatment.
In the models where patients were offered medications during detox, the researchers simulated all patients who entered detox being offered methadone, buprenorphine, or naltrexone, and 78% accepting the offer. Of these, they simulated that 28% chose buprenorphine, 18% chose methadone, and 32% chose naltrexone injection, based on recent research examining patients’ beliefs and preference for each. The researchers also simulated 2 levels of linking to outpatient medication treatment: (1) perfect linkage with 100% of those who initiated medications during detox being linked to outpatient medication treatment, and (2) moderate-linkage where 50% of those who initiated medications during detox being linked to outpatient medication treatment.
Cost-effectiveness was analyzed in the population models only. For these analyses, costs were estimated in 2019 US dollars and were discounted annually at 3% (which is similar to accounting for inflation). Three sources of costs were included: 1) costs of health-care utilization for all services other than opioid use disorder treatment, (2) costs of opioid use disorder treatment, and (3) costs related to overdose. Researchers also estimated the incremental cost-effectiveness ratio, which estimates costs per life-year saved and quality adjusted life-year saved, which adjusts for the burden of an illness or disorder, where one quality adjusted life year equates to one year in good health.
Data for the models were obtained from the Massachusetts Public Health Data Warehouse, which includes administrative records from over 16 agencies across Massachusetts. The researchers also used data from previous studies to obtain information about the natural course of opioid use disorder and quality of life indicators.
WHAT DID THIS STUDY FIND?
Initiating medication in detox and linkages to community treatment improve opioid outcomes for 1 year.
The detox-only models that did not allow for movement into and out of use and treatment and the state showed that initiating medications for the treatment of opioid use disorder during detox and linking patients to outpatient medication treatment is helpful. Specifically, in comparison to no initiation or linkage, the simulation with 100% linkage resulted in a 21.4% decrease in active opioid use, a 334% (i.e., three-fold) increase in outpatient medication treatment, and a 25.1% reduction in fatal overdoses over the course of 1 year.
The 50% linkage simulation resulted in an 11.0% decrease in active use, a 172% increase in outpatient medication treatment, and a 13.1% reduction in fatal overdoses over the course of 1 year.
Among the population, initiating medication in detox and linkages to community treatment improve opioid outcomes for 10 years.
The population models that allowed for movement into and out of use and treatment and the state also showed that initiating medications for the treatment of opioid use disorder during detox and linking patients to outpatient medication treatment is helpful. Specifically, in comparison to no initiation or linkage, the simulation with 100% linkage resulted in a 2.4% decrease in active opioid use, a 26.0% increase in outpatient medication treatment, and prevented 4.5% of fatal overdoses over the course of 10 years.
The 50% linkage simulation resulted 1.2% decrease in active opioid use, a 15.2% increase in outpatient medication treatment, and a 2.3% decrease in fatal overdoses over a 10-year period.
Initiating medication in detox and linkages to community treatment is cost-effective.
In comparison to no initiation or linkage, the simulation with 100% linkage showed that the undiscounted cost of medication initiation and linkage was $629 million dollars over 10 years (i.e., not accounting for inflation). The discounted, incremental cost was $306 million (i.e., accounting for inflation). The incremental cost-effectiveness ratio was $67,600 per life year saved and $55,600 per quality adjusted life year saved.
In comparison to no initiation or linkage, the simulation with 50% linkage showed that the undiscounted cost of medication initiation and linkage was $323 million dollars over 10 years. The discounted, incremental cost was $225 million. The incremental cost-effectiveness ratio was $97,300 per life-years saved and $78,500 per quality adjusted life year saved.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study used simulation modeling to estimate the effectiveness and cost-effectiveness of initiating medications for the treatment of opioid use disorder during detox and linking patients to outpatient medication treatment. In comparison to no medication initiation or linkage, results showed that medication initiation and linkage was helpful at preventing return to drug use and overdose deaths and increasing outpatient treatment.
Medication initiation and linkage through detox centers was also shown to be cost-effective, costing the healthcare sector in Massachusetts approximately $100-$400 per person. This would only require a 0.5-1% increase in the state budget above current spending. This benefit is maximized by delivering the intervention to all eligible detox patients – the cost savings from rationing funding so that only a subset receive the linkage is negligible while the outcomes are half as good.
While the benefits from the population models are more modest, and call into question whether the intervention is worth additional funding, cost-effectiveness analyses like these are important for demonstrating that the ultimate savings from the intervention come from reduced health care and overdose costs. These reductions help to offset the increased costs from funding the medications in the intervention.
Although the study used simulations to estimate the potential impact of medication initiation and linkage, data for the models was drawn from real-world sources and contributes to the growing research base on effective strategies for addressing the opioid epidemic. The results suggest that detox centers can provide a cost-effective place for initiating medications and connecting patients to outpatient medication treatment, which is one strategy that can be an effective part of a larger, comprehensive overdose prevention effort.
The simulation models do not adjust the estimates provided when patients drop out of treatment or die, both of which are likely to occur in real-world scenarios. This could result in the model overestimating the strategy’s effectiveness.
The data used in the simulation models were based on current estimates from Massachusetts. Changes in these trends in the future could affect the estimates of effectiveness and cost-effectiveness, as could using data from other states.
The research team did not have access to data regarding transitions between different medications, so it is unclear if switching medications would affect outcomes.
Because this study involved a simulation, the researchers needed to make several assumptions. For example, they assumed that patients entering detox programs have a high level of interest in medications for treatment, which may or may not be the case. Making different assumptions for the simulations may have resulted in different findings.
This study focused on medication treatment only and did not consider the impact of additional strategies that have been shown to prevent return to drug use, such as harm reduction and recovery support services.
BOTTOM LINE
Results suggest that initiating medications for the treatment of opioid use disorder during detox and linking patients to outpatient medication treatment is a cost-effective strategy for improving and saving lives. It can help reduce overdoses for individuals with opioid use disorder while adding only marginal costs to a state’s substance use budget.
For individuals and families seeking recovery: Initiating medications for the treatment of opioid use disorder during detox and linking patients to outpatient medication treatment may help prevent return to drug use and overdose deaths and increase outpatient treatment engagement that facilitates ongoing use of medications. Accordingly, if individuals with opioid use disorder enter detox and accept medication as part of their treatment, as well as following up with outpatient treatment, they are likely to have better opioid outcomes while reducing risk of overdose. Likewise, families of these individuals are encouraged to support medication treatment during detox and facilitate outpatient treatment following detox.
For treatment professionals and treatment systems: Treatment professionals who work in detox settings may improve patient outcomes by actively linking individuals to community-based treatment that provides FDA-approved opioid use disorder medications. Beyond this, however, return to use and overdose are likely to be further prevented when this strategy is implemented in combination with other efforts, such as connecting patients with recovery peer support and harm reduction.
For scientists: Given that the current study used simulation modeling to estimate the public health benefit of initiating opioid use disorder medication and linkages to community treatment in detox, future research is needed that examines the real-world public health impacts of these interventions. Such research would add to the current findings and shed light on these strategy’s effectiveness and cost-effectiveness when implemented in practice. Further, since the study used data from Massachusetts, future research can also extend the generalizability of the findings to patients in other states.
For policy makers: Supporting policies that promote the availability of medication initiation and linkage as a routine practice could improve and save lives of patients with opioid use disorderwhile adding only modest costs. If such policies were implemented as part of a comprehensive overdose prevention effort, there is likely to be a larger impact with more lives and money saved.