Methamphetamine-related psychiatric hospitalizations on the rise
There has been recent rapid increase in methamphetamine use, which increases risk for substance-induced psychiatric symptoms such as acute psychosis, depression and anxiety, and suicidal ideation. This study characterized trends in US methamphetamine-involved psychiatric hospitalizations between 2015 and 2019 and associations with sociodemographic characteristics.
Methamphetamine is a synthetic central nervous system stimulant that, at low doses, generally causes a sense of euphoria and can increase wakefulness, heart rate, physical activity, and blood pressure. It is a Schedule II substance and is approved by the Food and Drug Administration to treat obesity and Attention Deficit/Hyperactivity Disorder. At high doses, however, methamphetamine use may result in high body temperatures, convulsions, and cardiovascular collapse, and death, and chronic use can lead to severe weight loss, memory loss, and damage to teeth and skin.
In recent years, there has been a rapid increase in methamphetamine use and harms. This has been particularly concerning among people reporting opioid use, fueling concerns of an emerging “twin epidemic ”, as rates of methamphetamine use increased from 9.0% in 2015 to 30.2% in 2017 among people who use heroin in a nationally representative sample. In addition to rates of use, the Drug Enforcement Agency has reported increases in the potency of methamphetamine, which can result in greater likelihood of acute harms. Amphetamine-involved hospitalizations, overall, increased more than 270% from 2008 to 2015, and deaths involving stimulants (i.e., including cocaine), increased more than 300% from 2013 to 2019. In some regions, such as West Virginia or the American West, these increases may be even greater.
Importantly, methamphetamine use also increases risk for substance-induced psychiatric symptoms, such as psychosis/delusions and paranoia, anxiety and depression, and suicidal ideation, yet little has been documented regarding rates of psychiatric hospitalization among this growing population. To this end, the current study examined trends in US methamphetamine-involved psychiatric hospitalizations.
HOW WAS THIS STUDY CONDUCTED?
This study was a population-based analysis of archival, publicly available data. The authors examined data on US psychiatric hospitalizations from the Healthcare Cost and Utilization Project National Inpatient Sample containing a 20% stratified sample of community hospitalizations from participating states. This means that the sample is drawn randomly from subpopulations that are representative of the sample, rather than a whole population, which decreases sampling errors. Collectively, this approach is representative of over 97% of the US population.
The authors examined rates of psychostimulant-involved psychiatric hospitalizations among US adults ages 18 or older from October 2015 to December 2019 and subdivided each year into quarters (Q1 to Q4). They defined “psychiatric hospitalization” as having an international Classification of Diseases 10 (ICD-10) diagnostic codes for anxiety, depressive, or bipolar disorders, schizophrenia, and other psychotic disorders listed in the first diagnostic position of the hospitalization. The authors also identified amphetamine/psychostimulant, cocaine, and opioid misuse or use disorder, poisoning, or adverse effects using their respective ICD-10 codes. Altogether, the authors grouped hospitalizations in 8 ways: (1) methamphetamine alone (no cocaine, no opioids); (2) methamphetamine and cocaine (no opioids); (3) methamphetamine and opioids (no cocaine); (4) methamphetamine and cocaine and opioids; (5) all methamphetamine-involved psychiatric hospitalizations; regardless of other drug use); (6) psychiatric hospitalizations involving opioids and/or cocaine (no methamphetamine); (7) nonsubstance-involved psychiatric hospitalizations (no cocaine, no opioids, no methamphetamine), and (8) all psychiatric hospitalizations in the dataset (substance-involved and nonsubstance involved). The researchers first examined trends in psychiatric hospitalization by groups. They then examined whether prevalence rates of hospitalizations that were categorized into each group differed by age groups (18-30, 31-40, 41-50, 51-60, >60), gender (male/female), race (White, Black, Hispanic, Asian/Pacific Islander/Native American/Other, missing), insurance status (Medicare, Medicaid, Private Pay/No Charge/Other, missing), or region (Northeast, Midwest, South, West).
Of note, the Healthcare Cost and Utilization Project National Inpatient Sample includes most US hospitals but excludes short-term rehabilitation hospitals, long-term acute care hospitals, psychiatric-specific hospitals, psychiatric residential treatment centers, psychiatric partial hospitalization treatment, and substance use treatment facilities. As a result, some hospitalizations at substance-specific and stand-alone psychiatric facilities may not have been included, even if they involved methamphetamine use. Diagnostic codes did not distinguish between methamphetamine use and the non-medical use of prescription amphetamines, and therefore all amphetamines were included though the study team “assumed that most psychostimulant-involved or amphetamine-involved hospitalizations were attributable to methamphetamine”.
WHAT DID THIS STUDY FIND?
Methamphetamine-related Psychiatric Hospitalizations Increased Between 2015 and 2019
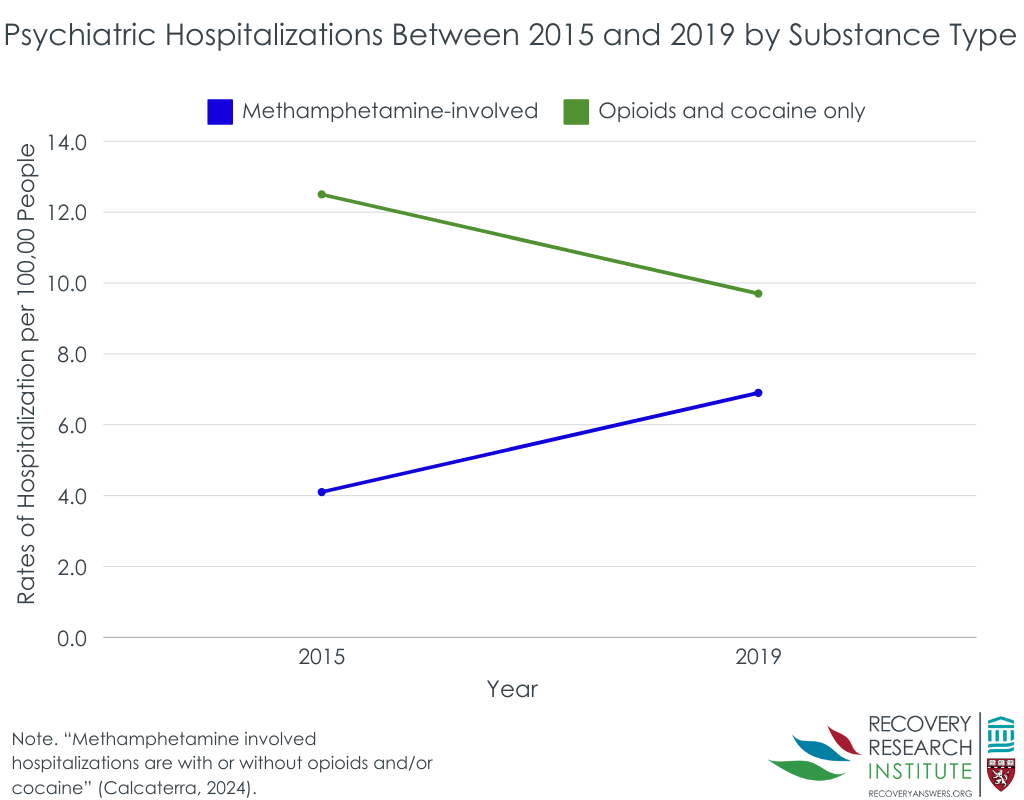
Between October 2015 and December 2019, there were 963,202 psychiatric hospitalizations. Whereas most did not involve substances (84.1%), 5.2% involved methamphetamine with or without opioids and/or cocaine and 10.7% involved opioids and/or cocaine without methamphetamine.
Rates of nonsubstance-involved psychiatric hospitalization remained relatively stable between 2015 and 2019. As illustrated in the figure below, methamphetamine-involved hospitalization rates (including those that may have involved other drugs) increased by 68.3% from 2015 to 2019. Opioid- and cocaine-involved psychiatric hospitalizations (not involving methamphetamine) decreased by 22.4%.
Methamphetamine hospitalizations was highest for younger adults and White individuals, but on the rise for older adults and Black individuals
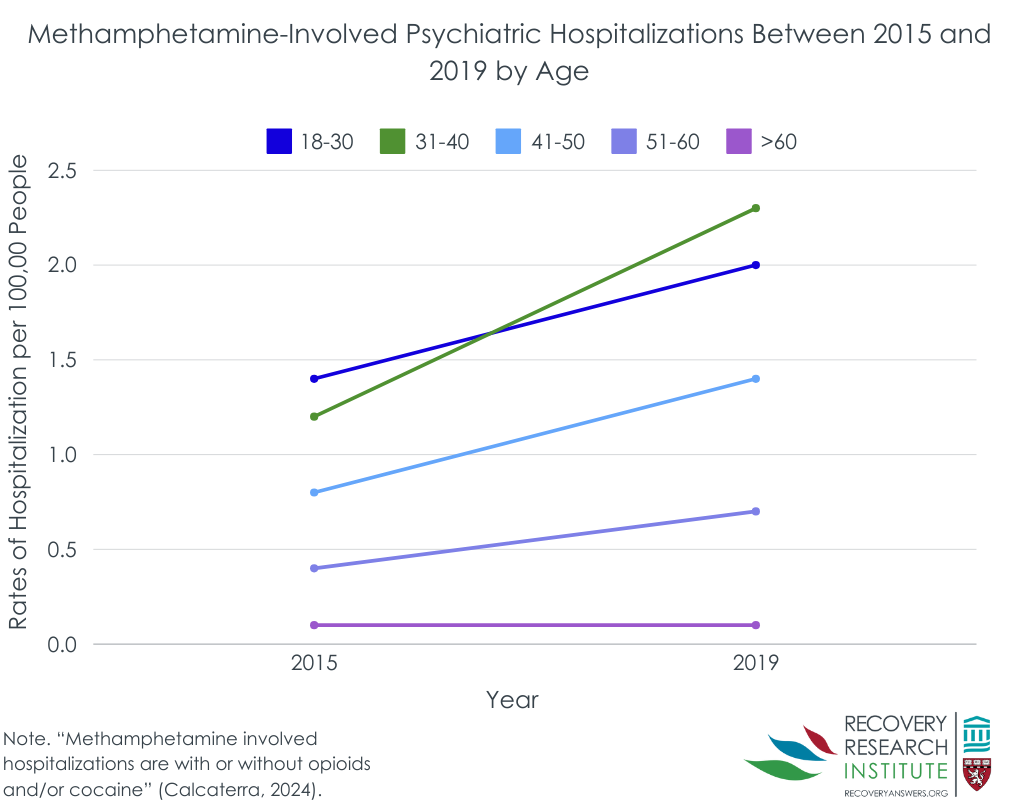
From 2015 to 2019, patients aged 18–30 and aged 31-40 accounted for 33.7% and 32.9% of methamphetamine-related psychiatric hospitalizations. Further, methamphetamine use was more frequent among male (61.9%) and White (63.2%) sub-groups as well as Medicaid beneficiaries (relative to all other categories, 52.8%), and those living in the West (40.5%).
In terms of changing trends, different patterns emerged. As shown in the figure below, whereas patients aged 18-40 accounted for most methamphetamine-involved hospitalizations overall, those aged 61 or older saw the largest increase between 2015 to 2019 (129% increase) , though the absolute rates for those 61+ was quite low (from 0.07 to 0.15 per 100,000 people). Further, Black patients saw a 100% increase in methamphetamine-involved hospitalizations, and those living in the Midwest saw a 145% increase in methamphetamine-involved hospitalizations. Medicaid beneficiaries, relative to other insurance groups, and men (relative to women) also saw greater increases from 2015 to 2019.
Methamphetamine-involved psychiatric hospitalizations were most common in the West, but rose at the greatest rate in the Midwest
When examining results by US region, methamphetamine-involved psychiatric hospitalizations increased quarterly at a rate of 4.6% in the Northeast, though the Northeast had the lowest overall rates of methamphetamine-involved hospitalizations relative to the South, Midwest, and the West. Methamphetamine-involved psychiatric hospitalizations increased at a rate of 10.1% per quarter in the Midwest from 2015 to mid-2017, but slowed to increases of 3.7% from mid-2017 through 2019. In the South, methamphetamine-involved psychiatric hospitalizations increased from end-2015 to mid-2018 at a rate of 0.8% per quarter, but picked up to 2.3% from end-2018 through 2019. Rates of methamphetamine-involved psychiatric hospitalizations initially increased in the West but then decreased at a rate of 0.5% from mid-2017 through 2019.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
These results document an emerging and disconcerting trend of rising rates of methamphetamine use and harms associated with such use. Yet, rates of methamphetamine use, and methamphetamine-involved psychiatric hospitalizations, remain much lower than the rate from opioids. The public health burden of methamphetamine may continue to increase without measures to adequately address these harms. Even as opioid mortality rates appear to decline, methamphetamine use is rising rapidly, particularly among people who also use opioids. This is concerning given joint effects but also because many people continue to use stimulants after discontinuing opioid use, and stimulant use during early opioid use disorder recovery may result in poorer recovery outcomes.
Importantly, we do not know whether these increases are attributable to increased potency of methamphetamine, simply to rising rates of use overall, or to some other reason. Regardless, the findings highlight the need for the deployment of effective treatment and recovery support services for methamphetamine use disorder. There are currently no FDA-approved medications for methamphetamine (though combination bupropion and extended-release naltrexone shows promise). Evidence-based care, such as outpatient programs and recovery support services, may be critical to providing support as methamphetamine use rates rise nationally. While more treatments are needed to engage the breadth of individuals with methamphetamine and other stimulant use disorders in care, there are several psychosocial interventions that can help (e.g., the Matrix Model a comprehensive 16-week group outpatient program). As such, keeping current on trends related to these harms may lead to expansion of timely strategies to engage individuals with these disorders in treatment and recovery support services that may help address these life-altering consequences.
This study also highlights the significant burden that psychiatric symptoms can create for people who use methamphetamine or who are attempting recovery from methamphetamine use disorder. It may be important to treat psychiatric symptoms during early recovery, and activities such as exercise have also been shown to help decrease psychiatric symptoms like depression among people who are in recovery from methamphetamine.
The results also highlighted particularly vulnerable populations that may be experiencing the greatest amount of harms from methamphetamine. Although men have higher rates of psychiatric hospitalizations, it is important to note that previous research has found that women seeking treatment for methamphetamine use tend to have worse psychiatric symptoms compared to men thus may be a uniquely vulnerable population among those being hospitalized for psychiatric reasons . Other populations such as those who are Black and those over the age of 60, are experiencing rapidly increasing rates of harm. These disparities may be partially attributable to disparities in access to care in the US healthcare system, though this may not explain why these effects appear to be increasing now as opposed to during other periods. It is unclear why rates of psychiatric hospitalizations are rising at a faster rate among those aged 60 or older relative to other age groups. Older adults are more sensitive to substance use effects and increases in potency of methamphetamine in the midst of an aging population may account for this increase. Finally, although there are higher rates of methamphetamine-involved psychiatric hospitalizations in the West, rates are increasing in other parts of the United States, highlighting a national, rather than regional, public health concern. As noted above, it should be remembered that these results excluded dedicated psychiatric-specific hospitals and specialty substance use treatment settings, likely leading to underestimates of both substance-involved and nonsubstance-involved psychiatric hospitalizations. Great knowledge about these psychiatric venues may help provide further explanations and better all round estimates of psychiatric harm increases related to methamphetamine.
Clinical diagnoses like those used here are dependent upon the information available to the provider and prone to the providers impressions and biases, which may influence diagnosis.
These data excluded dedicated psychiatric-specific hospitals and specialty substance use treatment settings, likely leading to underestimates of both substance-involved and nonsubstance-involved psychiatric hospitalizations.
BOTTOM LINE
Methamphetamine use is on the rise, and methamphetamine-involved psychiatric hospitalizations are rising at a faster rate relative to hospitalizations involving other drugs like cocaine and opioids. While younger adults, White individuals, and those living in the Western US had the highest overall rates, rates for older adults, Black individuals, and those in the Midwest may be on the rise.
For individuals and families seeking recovery: If you or a loved one are using methamphetamine, it is important to know that the potency has increased in recent years and that there appears to be an increased risk of experiencing severe psychiatric symptoms associated with methamphetamine use that may result in psychiatric hospitalization. Engaging in mutual support groups (e.g., Crystal Meth Anonymous; Narcotics Anonymous) or other recovery support services, or in outpatient therapy, may be useful for those attempting to stop using methamphetamine.
For treatment professionals and treatment systems: Rates of methamphetamine use are increasing in the United States and may induce or exacerbate psychiatric symptoms. Clinicians and treatment systems that are able to deliver person-centered care that is sensitive to the needs of people with substance use disorder may be able to prevent methamphetamine-involved psychiatric hospitalizations while also improving psychiatric care more broadly.
For scientists: There is a clear trend demonstrating increases in methamphetamine use and harm in the United States over the past few decades. However, it is unclear why this is happening, and how to best prevent continued rising rates of use and affiliated harms. More research to understand the intersection between methamphetamine use and psychiatric symptoms like depression and anxiety may also help lead to solutions in treatment.
For policy makers: Measuring trends in rates of substance use and mortality is critical for detecting emerging substance epidemics and their nature. Funding to maintain and support critical early detection infrastructure can help increase the response rate of systems of care. Additional funding for scientists to continue to study effective treatments may also help to alleviate the burden of substance use in the United States.
Methamphetamine is a synthetic central nervous system stimulant that, at low doses, generally causes a sense of euphoria and can increase wakefulness, heart rate, physical activity, and blood pressure. It is a Schedule II substance and is approved by the Food and Drug Administration to treat obesity and Attention Deficit/Hyperactivity Disorder. At high doses, however, methamphetamine use may result in high body temperatures, convulsions, and cardiovascular collapse, and death, and chronic use can lead to severe weight loss, memory loss, and damage to teeth and skin.
In recent years, there has been a rapid increase in methamphetamine use and harms. This has been particularly concerning among people reporting opioid use, fueling concerns of an emerging “twin epidemic ”, as rates of methamphetamine use increased from 9.0% in 2015 to 30.2% in 2017 among people who use heroin in a nationally representative sample. In addition to rates of use, the Drug Enforcement Agency has reported increases in the potency of methamphetamine, which can result in greater likelihood of acute harms. Amphetamine-involved hospitalizations, overall, increased more than 270% from 2008 to 2015, and deaths involving stimulants (i.e., including cocaine), increased more than 300% from 2013 to 2019. In some regions, such as West Virginia or the American West, these increases may be even greater.
Importantly, methamphetamine use also increases risk for substance-induced psychiatric symptoms, such as psychosis/delusions and paranoia, anxiety and depression, and suicidal ideation, yet little has been documented regarding rates of psychiatric hospitalization among this growing population. To this end, the current study examined trends in US methamphetamine-involved psychiatric hospitalizations.
HOW WAS THIS STUDY CONDUCTED?
This study was a population-based analysis of archival, publicly available data. The authors examined data on US psychiatric hospitalizations from the Healthcare Cost and Utilization Project National Inpatient Sample containing a 20% stratified sample of community hospitalizations from participating states. This means that the sample is drawn randomly from subpopulations that are representative of the sample, rather than a whole population, which decreases sampling errors. Collectively, this approach is representative of over 97% of the US population.
The authors examined rates of psychostimulant-involved psychiatric hospitalizations among US adults ages 18 or older from October 2015 to December 2019 and subdivided each year into quarters (Q1 to Q4). They defined “psychiatric hospitalization” as having an international Classification of Diseases 10 (ICD-10) diagnostic codes for anxiety, depressive, or bipolar disorders, schizophrenia, and other psychotic disorders listed in the first diagnostic position of the hospitalization. The authors also identified amphetamine/psychostimulant, cocaine, and opioid misuse or use disorder, poisoning, or adverse effects using their respective ICD-10 codes. Altogether, the authors grouped hospitalizations in 8 ways: (1) methamphetamine alone (no cocaine, no opioids); (2) methamphetamine and cocaine (no opioids); (3) methamphetamine and opioids (no cocaine); (4) methamphetamine and cocaine and opioids; (5) all methamphetamine-involved psychiatric hospitalizations; regardless of other drug use); (6) psychiatric hospitalizations involving opioids and/or cocaine (no methamphetamine); (7) nonsubstance-involved psychiatric hospitalizations (no cocaine, no opioids, no methamphetamine), and (8) all psychiatric hospitalizations in the dataset (substance-involved and nonsubstance involved). The researchers first examined trends in psychiatric hospitalization by groups. They then examined whether prevalence rates of hospitalizations that were categorized into each group differed by age groups (18-30, 31-40, 41-50, 51-60, >60), gender (male/female), race (White, Black, Hispanic, Asian/Pacific Islander/Native American/Other, missing), insurance status (Medicare, Medicaid, Private Pay/No Charge/Other, missing), or region (Northeast, Midwest, South, West).
Of note, the Healthcare Cost and Utilization Project National Inpatient Sample includes most US hospitals but excludes short-term rehabilitation hospitals, long-term acute care hospitals, psychiatric-specific hospitals, psychiatric residential treatment centers, psychiatric partial hospitalization treatment, and substance use treatment facilities. As a result, some hospitalizations at substance-specific and stand-alone psychiatric facilities may not have been included, even if they involved methamphetamine use. Diagnostic codes did not distinguish between methamphetamine use and the non-medical use of prescription amphetamines, and therefore all amphetamines were included though the study team “assumed that most psychostimulant-involved or amphetamine-involved hospitalizations were attributable to methamphetamine”.
WHAT DID THIS STUDY FIND?
Methamphetamine-related Psychiatric Hospitalizations Increased Between 2015 and 2019
Between October 2015 and December 2019, there were 963,202 psychiatric hospitalizations. Whereas most did not involve substances (84.1%), 5.2% involved methamphetamine with or without opioids and/or cocaine and 10.7% involved opioids and/or cocaine without methamphetamine.
Rates of nonsubstance-involved psychiatric hospitalization remained relatively stable between 2015 and 2019. As illustrated in the figure below, methamphetamine-involved hospitalization rates (including those that may have involved other drugs) increased by 68.3% from 2015 to 2019. Opioid- and cocaine-involved psychiatric hospitalizations (not involving methamphetamine) decreased by 22.4%.
Methamphetamine hospitalizations was highest for younger adults and White individuals, but on the rise for older adults and Black individuals
From 2015 to 2019, patients aged 18–30 and aged 31-40 accounted for 33.7% and 32.9% of methamphetamine-related psychiatric hospitalizations. Further, methamphetamine use was more frequent among male (61.9%) and White (63.2%) sub-groups as well as Medicaid beneficiaries (relative to all other categories, 52.8%), and those living in the West (40.5%).
In terms of changing trends, different patterns emerged. As shown in the figure below, whereas patients aged 18-40 accounted for most methamphetamine-involved hospitalizations overall, those aged 61 or older saw the largest increase between 2015 to 2019 (129% increase) , though the absolute rates for those 61+ was quite low (from 0.07 to 0.15 per 100,000 people). Further, Black patients saw a 100% increase in methamphetamine-involved hospitalizations, and those living in the Midwest saw a 145% increase in methamphetamine-involved hospitalizations. Medicaid beneficiaries, relative to other insurance groups, and men (relative to women) also saw greater increases from 2015 to 2019.
Methamphetamine-involved psychiatric hospitalizations were most common in the West, but rose at the greatest rate in the Midwest
When examining results by US region, methamphetamine-involved psychiatric hospitalizations increased quarterly at a rate of 4.6% in the Northeast, though the Northeast had the lowest overall rates of methamphetamine-involved hospitalizations relative to the South, Midwest, and the West. Methamphetamine-involved psychiatric hospitalizations increased at a rate of 10.1% per quarter in the Midwest from 2015 to mid-2017, but slowed to increases of 3.7% from mid-2017 through 2019. In the South, methamphetamine-involved psychiatric hospitalizations increased from end-2015 to mid-2018 at a rate of 0.8% per quarter, but picked up to 2.3% from end-2018 through 2019. Rates of methamphetamine-involved psychiatric hospitalizations initially increased in the West but then decreased at a rate of 0.5% from mid-2017 through 2019.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
These results document an emerging and disconcerting trend of rising rates of methamphetamine use and harms associated with such use. Yet, rates of methamphetamine use, and methamphetamine-involved psychiatric hospitalizations, remain much lower than the rate from opioids. The public health burden of methamphetamine may continue to increase without measures to adequately address these harms. Even as opioid mortality rates appear to decline, methamphetamine use is rising rapidly, particularly among people who also use opioids. This is concerning given joint effects but also because many people continue to use stimulants after discontinuing opioid use, and stimulant use during early opioid use disorder recovery may result in poorer recovery outcomes.
Importantly, we do not know whether these increases are attributable to increased potency of methamphetamine, simply to rising rates of use overall, or to some other reason. Regardless, the findings highlight the need for the deployment of effective treatment and recovery support services for methamphetamine use disorder. There are currently no FDA-approved medications for methamphetamine (though combination bupropion and extended-release naltrexone shows promise). Evidence-based care, such as outpatient programs and recovery support services, may be critical to providing support as methamphetamine use rates rise nationally. While more treatments are needed to engage the breadth of individuals with methamphetamine and other stimulant use disorders in care, there are several psychosocial interventions that can help (e.g., the Matrix Model a comprehensive 16-week group outpatient program). As such, keeping current on trends related to these harms may lead to expansion of timely strategies to engage individuals with these disorders in treatment and recovery support services that may help address these life-altering consequences.
This study also highlights the significant burden that psychiatric symptoms can create for people who use methamphetamine or who are attempting recovery from methamphetamine use disorder. It may be important to treat psychiatric symptoms during early recovery, and activities such as exercise have also been shown to help decrease psychiatric symptoms like depression among people who are in recovery from methamphetamine.
The results also highlighted particularly vulnerable populations that may be experiencing the greatest amount of harms from methamphetamine. Although men have higher rates of psychiatric hospitalizations, it is important to note that previous research has found that women seeking treatment for methamphetamine use tend to have worse psychiatric symptoms compared to men thus may be a uniquely vulnerable population among those being hospitalized for psychiatric reasons . Other populations such as those who are Black and those over the age of 60, are experiencing rapidly increasing rates of harm. These disparities may be partially attributable to disparities in access to care in the US healthcare system, though this may not explain why these effects appear to be increasing now as opposed to during other periods. It is unclear why rates of psychiatric hospitalizations are rising at a faster rate among those aged 60 or older relative to other age groups. Older adults are more sensitive to substance use effects and increases in potency of methamphetamine in the midst of an aging population may account for this increase. Finally, although there are higher rates of methamphetamine-involved psychiatric hospitalizations in the West, rates are increasing in other parts of the United States, highlighting a national, rather than regional, public health concern. As noted above, it should be remembered that these results excluded dedicated psychiatric-specific hospitals and specialty substance use treatment settings, likely leading to underestimates of both substance-involved and nonsubstance-involved psychiatric hospitalizations. Great knowledge about these psychiatric venues may help provide further explanations and better all round estimates of psychiatric harm increases related to methamphetamine.
Clinical diagnoses like those used here are dependent upon the information available to the provider and prone to the providers impressions and biases, which may influence diagnosis.
These data excluded dedicated psychiatric-specific hospitals and specialty substance use treatment settings, likely leading to underestimates of both substance-involved and nonsubstance-involved psychiatric hospitalizations.
BOTTOM LINE
Methamphetamine use is on the rise, and methamphetamine-involved psychiatric hospitalizations are rising at a faster rate relative to hospitalizations involving other drugs like cocaine and opioids. While younger adults, White individuals, and those living in the Western US had the highest overall rates, rates for older adults, Black individuals, and those in the Midwest may be on the rise.
For individuals and families seeking recovery: If you or a loved one are using methamphetamine, it is important to know that the potency has increased in recent years and that there appears to be an increased risk of experiencing severe psychiatric symptoms associated with methamphetamine use that may result in psychiatric hospitalization. Engaging in mutual support groups (e.g., Crystal Meth Anonymous; Narcotics Anonymous) or other recovery support services, or in outpatient therapy, may be useful for those attempting to stop using methamphetamine.
For treatment professionals and treatment systems: Rates of methamphetamine use are increasing in the United States and may induce or exacerbate psychiatric symptoms. Clinicians and treatment systems that are able to deliver person-centered care that is sensitive to the needs of people with substance use disorder may be able to prevent methamphetamine-involved psychiatric hospitalizations while also improving psychiatric care more broadly.
For scientists: There is a clear trend demonstrating increases in methamphetamine use and harm in the United States over the past few decades. However, it is unclear why this is happening, and how to best prevent continued rising rates of use and affiliated harms. More research to understand the intersection between methamphetamine use and psychiatric symptoms like depression and anxiety may also help lead to solutions in treatment.
For policy makers: Measuring trends in rates of substance use and mortality is critical for detecting emerging substance epidemics and their nature. Funding to maintain and support critical early detection infrastructure can help increase the response rate of systems of care. Additional funding for scientists to continue to study effective treatments may also help to alleviate the burden of substance use in the United States.
Methamphetamine is a synthetic central nervous system stimulant that, at low doses, generally causes a sense of euphoria and can increase wakefulness, heart rate, physical activity, and blood pressure. It is a Schedule II substance and is approved by the Food and Drug Administration to treat obesity and Attention Deficit/Hyperactivity Disorder. At high doses, however, methamphetamine use may result in high body temperatures, convulsions, and cardiovascular collapse, and death, and chronic use can lead to severe weight loss, memory loss, and damage to teeth and skin.
In recent years, there has been a rapid increase in methamphetamine use and harms. This has been particularly concerning among people reporting opioid use, fueling concerns of an emerging “twin epidemic ”, as rates of methamphetamine use increased from 9.0% in 2015 to 30.2% in 2017 among people who use heroin in a nationally representative sample. In addition to rates of use, the Drug Enforcement Agency has reported increases in the potency of methamphetamine, which can result in greater likelihood of acute harms. Amphetamine-involved hospitalizations, overall, increased more than 270% from 2008 to 2015, and deaths involving stimulants (i.e., including cocaine), increased more than 300% from 2013 to 2019. In some regions, such as West Virginia or the American West, these increases may be even greater.
Importantly, methamphetamine use also increases risk for substance-induced psychiatric symptoms, such as psychosis/delusions and paranoia, anxiety and depression, and suicidal ideation, yet little has been documented regarding rates of psychiatric hospitalization among this growing population. To this end, the current study examined trends in US methamphetamine-involved psychiatric hospitalizations.
HOW WAS THIS STUDY CONDUCTED?
This study was a population-based analysis of archival, publicly available data. The authors examined data on US psychiatric hospitalizations from the Healthcare Cost and Utilization Project National Inpatient Sample containing a 20% stratified sample of community hospitalizations from participating states. This means that the sample is drawn randomly from subpopulations that are representative of the sample, rather than a whole population, which decreases sampling errors. Collectively, this approach is representative of over 97% of the US population.
The authors examined rates of psychostimulant-involved psychiatric hospitalizations among US adults ages 18 or older from October 2015 to December 2019 and subdivided each year into quarters (Q1 to Q4). They defined “psychiatric hospitalization” as having an international Classification of Diseases 10 (ICD-10) diagnostic codes for anxiety, depressive, or bipolar disorders, schizophrenia, and other psychotic disorders listed in the first diagnostic position of the hospitalization. The authors also identified amphetamine/psychostimulant, cocaine, and opioid misuse or use disorder, poisoning, or adverse effects using their respective ICD-10 codes. Altogether, the authors grouped hospitalizations in 8 ways: (1) methamphetamine alone (no cocaine, no opioids); (2) methamphetamine and cocaine (no opioids); (3) methamphetamine and opioids (no cocaine); (4) methamphetamine and cocaine and opioids; (5) all methamphetamine-involved psychiatric hospitalizations; regardless of other drug use); (6) psychiatric hospitalizations involving opioids and/or cocaine (no methamphetamine); (7) nonsubstance-involved psychiatric hospitalizations (no cocaine, no opioids, no methamphetamine), and (8) all psychiatric hospitalizations in the dataset (substance-involved and nonsubstance involved). The researchers first examined trends in psychiatric hospitalization by groups. They then examined whether prevalence rates of hospitalizations that were categorized into each group differed by age groups (18-30, 31-40, 41-50, 51-60, >60), gender (male/female), race (White, Black, Hispanic, Asian/Pacific Islander/Native American/Other, missing), insurance status (Medicare, Medicaid, Private Pay/No Charge/Other, missing), or region (Northeast, Midwest, South, West).
Of note, the Healthcare Cost and Utilization Project National Inpatient Sample includes most US hospitals but excludes short-term rehabilitation hospitals, long-term acute care hospitals, psychiatric-specific hospitals, psychiatric residential treatment centers, psychiatric partial hospitalization treatment, and substance use treatment facilities. As a result, some hospitalizations at substance-specific and stand-alone psychiatric facilities may not have been included, even if they involved methamphetamine use. Diagnostic codes did not distinguish between methamphetamine use and the non-medical use of prescription amphetamines, and therefore all amphetamines were included though the study team “assumed that most psychostimulant-involved or amphetamine-involved hospitalizations were attributable to methamphetamine”.
WHAT DID THIS STUDY FIND?
Methamphetamine-related Psychiatric Hospitalizations Increased Between 2015 and 2019
Between October 2015 and December 2019, there were 963,202 psychiatric hospitalizations. Whereas most did not involve substances (84.1%), 5.2% involved methamphetamine with or without opioids and/or cocaine and 10.7% involved opioids and/or cocaine without methamphetamine.
Rates of nonsubstance-involved psychiatric hospitalization remained relatively stable between 2015 and 2019. As illustrated in the figure below, methamphetamine-involved hospitalization rates (including those that may have involved other drugs) increased by 68.3% from 2015 to 2019. Opioid- and cocaine-involved psychiatric hospitalizations (not involving methamphetamine) decreased by 22.4%.
Methamphetamine hospitalizations was highest for younger adults and White individuals, but on the rise for older adults and Black individuals
From 2015 to 2019, patients aged 18–30 and aged 31-40 accounted for 33.7% and 32.9% of methamphetamine-related psychiatric hospitalizations. Further, methamphetamine use was more frequent among male (61.9%) and White (63.2%) sub-groups as well as Medicaid beneficiaries (relative to all other categories, 52.8%), and those living in the West (40.5%).
In terms of changing trends, different patterns emerged. As shown in the figure below, whereas patients aged 18-40 accounted for most methamphetamine-involved hospitalizations overall, those aged 61 or older saw the largest increase between 2015 to 2019 (129% increase) , though the absolute rates for those 61+ was quite low (from 0.07 to 0.15 per 100,000 people). Further, Black patients saw a 100% increase in methamphetamine-involved hospitalizations, and those living in the Midwest saw a 145% increase in methamphetamine-involved hospitalizations. Medicaid beneficiaries, relative to other insurance groups, and men (relative to women) also saw greater increases from 2015 to 2019.
Methamphetamine-involved psychiatric hospitalizations were most common in the West, but rose at the greatest rate in the Midwest
When examining results by US region, methamphetamine-involved psychiatric hospitalizations increased quarterly at a rate of 4.6% in the Northeast, though the Northeast had the lowest overall rates of methamphetamine-involved hospitalizations relative to the South, Midwest, and the West. Methamphetamine-involved psychiatric hospitalizations increased at a rate of 10.1% per quarter in the Midwest from 2015 to mid-2017, but slowed to increases of 3.7% from mid-2017 through 2019. In the South, methamphetamine-involved psychiatric hospitalizations increased from end-2015 to mid-2018 at a rate of 0.8% per quarter, but picked up to 2.3% from end-2018 through 2019. Rates of methamphetamine-involved psychiatric hospitalizations initially increased in the West but then decreased at a rate of 0.5% from mid-2017 through 2019.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
These results document an emerging and disconcerting trend of rising rates of methamphetamine use and harms associated with such use. Yet, rates of methamphetamine use, and methamphetamine-involved psychiatric hospitalizations, remain much lower than the rate from opioids. The public health burden of methamphetamine may continue to increase without measures to adequately address these harms. Even as opioid mortality rates appear to decline, methamphetamine use is rising rapidly, particularly among people who also use opioids. This is concerning given joint effects but also because many people continue to use stimulants after discontinuing opioid use, and stimulant use during early opioid use disorder recovery may result in poorer recovery outcomes.
Importantly, we do not know whether these increases are attributable to increased potency of methamphetamine, simply to rising rates of use overall, or to some other reason. Regardless, the findings highlight the need for the deployment of effective treatment and recovery support services for methamphetamine use disorder. There are currently no FDA-approved medications for methamphetamine (though combination bupropion and extended-release naltrexone shows promise). Evidence-based care, such as outpatient programs and recovery support services, may be critical to providing support as methamphetamine use rates rise nationally. While more treatments are needed to engage the breadth of individuals with methamphetamine and other stimulant use disorders in care, there are several psychosocial interventions that can help (e.g., the Matrix Model a comprehensive 16-week group outpatient program). As such, keeping current on trends related to these harms may lead to expansion of timely strategies to engage individuals with these disorders in treatment and recovery support services that may help address these life-altering consequences.
This study also highlights the significant burden that psychiatric symptoms can create for people who use methamphetamine or who are attempting recovery from methamphetamine use disorder. It may be important to treat psychiatric symptoms during early recovery, and activities such as exercise have also been shown to help decrease psychiatric symptoms like depression among people who are in recovery from methamphetamine.
The results also highlighted particularly vulnerable populations that may be experiencing the greatest amount of harms from methamphetamine. Although men have higher rates of psychiatric hospitalizations, it is important to note that previous research has found that women seeking treatment for methamphetamine use tend to have worse psychiatric symptoms compared to men thus may be a uniquely vulnerable population among those being hospitalized for psychiatric reasons . Other populations such as those who are Black and those over the age of 60, are experiencing rapidly increasing rates of harm. These disparities may be partially attributable to disparities in access to care in the US healthcare system, though this may not explain why these effects appear to be increasing now as opposed to during other periods. It is unclear why rates of psychiatric hospitalizations are rising at a faster rate among those aged 60 or older relative to other age groups. Older adults are more sensitive to substance use effects and increases in potency of methamphetamine in the midst of an aging population may account for this increase. Finally, although there are higher rates of methamphetamine-involved psychiatric hospitalizations in the West, rates are increasing in other parts of the United States, highlighting a national, rather than regional, public health concern. As noted above, it should be remembered that these results excluded dedicated psychiatric-specific hospitals and specialty substance use treatment settings, likely leading to underestimates of both substance-involved and nonsubstance-involved psychiatric hospitalizations. Great knowledge about these psychiatric venues may help provide further explanations and better all round estimates of psychiatric harm increases related to methamphetamine.
Clinical diagnoses like those used here are dependent upon the information available to the provider and prone to the providers impressions and biases, which may influence diagnosis.
These data excluded dedicated psychiatric-specific hospitals and specialty substance use treatment settings, likely leading to underestimates of both substance-involved and nonsubstance-involved psychiatric hospitalizations.
BOTTOM LINE
Methamphetamine use is on the rise, and methamphetamine-involved psychiatric hospitalizations are rising at a faster rate relative to hospitalizations involving other drugs like cocaine and opioids. While younger adults, White individuals, and those living in the Western US had the highest overall rates, rates for older adults, Black individuals, and those in the Midwest may be on the rise.
For individuals and families seeking recovery: If you or a loved one are using methamphetamine, it is important to know that the potency has increased in recent years and that there appears to be an increased risk of experiencing severe psychiatric symptoms associated with methamphetamine use that may result in psychiatric hospitalization. Engaging in mutual support groups (e.g., Crystal Meth Anonymous; Narcotics Anonymous) or other recovery support services, or in outpatient therapy, may be useful for those attempting to stop using methamphetamine.
For treatment professionals and treatment systems: Rates of methamphetamine use are increasing in the United States and may induce or exacerbate psychiatric symptoms. Clinicians and treatment systems that are able to deliver person-centered care that is sensitive to the needs of people with substance use disorder may be able to prevent methamphetamine-involved psychiatric hospitalizations while also improving psychiatric care more broadly.
For scientists: There is a clear trend demonstrating increases in methamphetamine use and harm in the United States over the past few decades. However, it is unclear why this is happening, and how to best prevent continued rising rates of use and affiliated harms. More research to understand the intersection between methamphetamine use and psychiatric symptoms like depression and anxiety may also help lead to solutions in treatment.
For policy makers: Measuring trends in rates of substance use and mortality is critical for detecting emerging substance epidemics and their nature. Funding to maintain and support critical early detection infrastructure can help increase the response rate of systems of care. Additional funding for scientists to continue to study effective treatments may also help to alleviate the burden of substance use in the United States.