
Mounting Evidence of the Benefits of 12-step Sponsors
In 12-step groups like Alcoholics Anonymous, members are often encouraged to get a sponsor. What happens when scientists take a closer, empirical look at this bit of recovery wisdom?
WHAT PROBLEM DOES THIS STUDY ADDRESS?
In 12-step mutual-help groups like Alcoholics Anonymous (AA) and Narcotics Anonymous (NA), a sponsor is a volunteer who is currently practicing the 12-step program of recovery and who helps newer AA members by providing support, encouragement, & guidance to promote sustained long-term recovery. In a prior Recovery Research Institute Bulletin, we highlighted research that shows having a 12-step sponsor in mutual-help organizations like Alcoholics Anonymous (AA), is related to better alcohol and other drug abstinence rates over time.
Given that there are many factors that can influence whether or not one gets a sponsor, research is needed to learn how best to aid individuals in obtaining a sponsor, this study by Wendt and colleagues is an important contribution to the science on 12-step mutual-help-related treatment and recovery. They tested whether having a sponsor helped promote better outcomes in a sample of individuals with stimulant use disorders (e.g., cocaine), as well as whether a rigorous, outpatient 12-step facilitation approach led to greater likelihood of obtaining a sponsor compared to standard treatment.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of an original randomized control trial called Stimulant Abuser Groups to Engage in 12-Step (STAGE-12), which showed that 234 individuals with current stimulant use disorder (e.g., cocaine or methamphetamines) who received a 12-step facilitation intervention were more likely to be abstinent during treatment than the 237 individuals who received treatment-as-usual during. But after the treatment, both groups had roughly similar rates of stimulant use if they were not abstinent.
The 12-step facilitation approach integrated 8 hours of treatment – five group sessions and three individuals sessions – into an intensive outpatient treatment program (i.e., treatment as usual), substituting for existing sessions, so that both groups received the same amount of treatment sessions overall. The 12-step facilitation addressed patients’ efforts to obtain a 12-step sponsor during each of the specialized sessions, and one of the group sessions provided an in-depth focus on the topic of sponsorship. Also worth noting is that individual sessions comprised an active linkage to 12-step mutual-help organization groups, engaging patients with current members to actively facilitate their participation.
Study authors assessed participants when they:
- entered treatment (i.e., baseline)
- post/ended-treatment (i.e., 8 weeks later)
- 1-month post-treatment (4 weeks after the 8 week assessment)
They were interested in three overarching questions:
- Is it beneficial to have a sponsor in terms of substance use outcomes?
- What types of thoughts and other attitudes when entering treatment were related to obtaining a 12-step sponsor?
- Was the 12-step facilitation more effective at improving an individual’s chance of obtaining a sponsor compared to treatment-as-usual?
There are several key methodological details that help put the study in context. The sample was comprised of 338 individuals with cocaine dependence based on the diagnostic and statistical manual of mental disorders, 4th edition (DSM-IV), 170 with methamphetamine dependence, of which 45 were dually-diagnosed. Nearly half had a co-occurring alcohol use disorder. The two treatment groups were roughly equal in the percentage of individuals with different diagnoses. Authors assessed 12-step participation with the 12-step Experiences and Expectations Scale (the number of meetings attended in the past 30 days, meetings with other members outside of meetings, receiving phones call from other members, assisting with meeting duties, speaking during meetings, reading 12-step literature for at least 5 minutes, and, germane to this study especially, whether or not one had a 12-step sponsor). They used the Survey of Readiness for AA (with items modified for other 12-step meetings as well) to assess readiness and expectations regarding 12-step participation as well as perceived barriers to participation. They used the Etiology of Addiction subscale of the Short Understanding of Substance Abuse Scale to assess participants’ belief in the “disease model” of addiction; i.e., that addiction is a disease that can be treated and managed, but never cured.
Finally, authors used three measures of substance use:
- days of stimulant use in the past 30 days
- any illicit drug use or drug use problem from the Addiction Severity Index (including but not limited to stimulant use)
- any alcohol use or alcohol use problem from the Addiction Severity Index
WHAT DID THIS STUDY FIND?
Individuals with a sponsor at the end of treatment had 33 or 50% greater chances of no illicit drug use or problems, and no stimulant use, respectively, at 1-month post-treatment compared to those without a sponsor, after adjusting for their substance use when they entered the study. Those with a sponsor also had a slightly greater likelihood of alcohol abstinence (or the absence of alcohol-related problems) compared to patients without a sponsor, though this advantage was not statistically significant. These patterns held for individuals in both treatment groups – in other words, sponsorship was related to better outcomes whether one received the 12-step facilitation or treatment-as-usual.
Contrary to what might be expected, neither one’s belief in the disease model of addiction, nor one’s readiness and expectations regarding 12-step participation upon entering treatment was related to whether someone had a sponsor at the end of treatment, after adjusting for having a sponsor when entering the study and which treatment they received (12-step facilitation or treatment-as-usual).
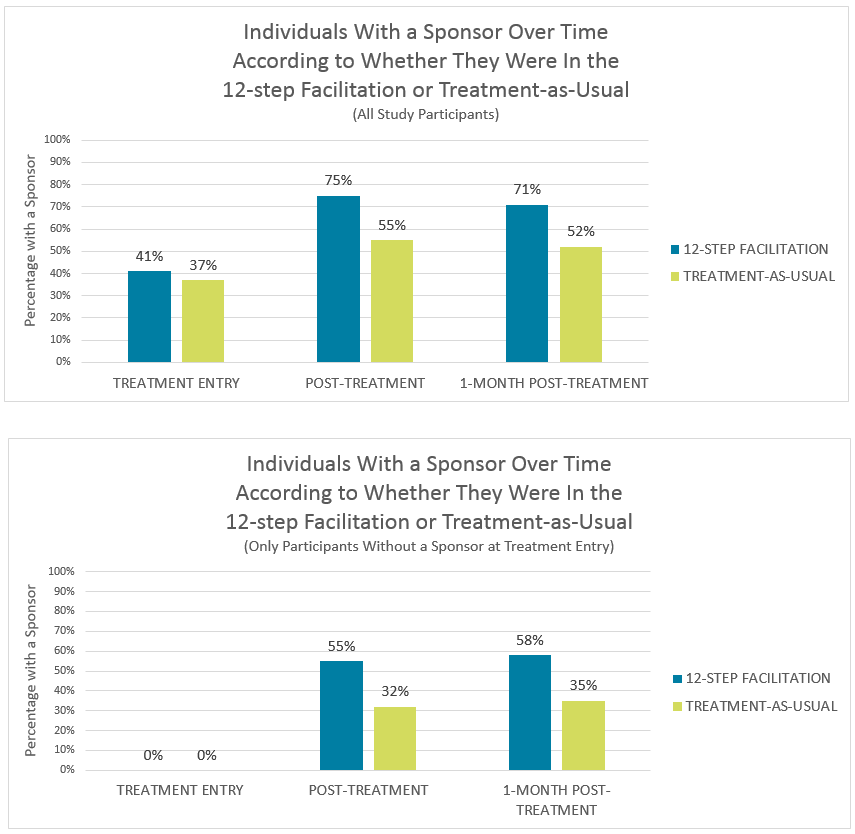
Finally, individuals who received the 12-step facilitation had odds two times higher of having a sponsor at the end of treatment, compared to treatment-as-usual. While this result may be expected given the greater focus in 12-step facilitation on attending 12-step groups (treatment-as-usual also strongly encouraged 12-step participation), its importance is magnified given that greater odds of having a sponsor was present in two separate models.
In one model, authors adjusted for an individual’s attitudes toward 12-step groups (readiness to attend, perceived barriers, etc.) and their disease model beliefs, and whether or not they had a sponsor at treatment entry. In the other model, authors adjusted for their other 12-step activities during treatment and whether or not they had a sponsor at treatment entry. Thus, some key ingredient of the 12-step facilitation treatment predicted obtaining a sponsor, beyond its ability to get patients to attend 12-step groups. The two times greater odds of having a sponsor in the 12-step facilitation compared to treatment-as-usual held up 1-month post-treatment as well.
These two figures show the percentage of individuals with a sponsor over time according to whether they received 12-step facilitation or treatment-as-usual. The figure on the top includes the total sample of 470 participants. The figure on the bottom includes only the 198 individuals who did not have a sponsor when they entered treatment.
WHY IS THIS STUDY IMPORTANT
The results from this study add to a growing body of other scientific studies that have also found that having a 12-step sponsor – and a better relationship with a sponsor – is related to better alcohol and other drug outcomes. In this case, the data also show that receiving 12-step facilitation can improve someone’s chances of obtaining a sponsor. With few exceptions, there is consensus in the scientific literature that having a 12-step sponsor helps improve substance use outcomes, and that psychosocial treatments that focus on helping individuals attend and actively participate in 12-step groups, with a special focus on obtaining a sponsor, can boost one’s likelihood of making this recovery-supportive personal connection.Although whether the 12-step facilitation worked by helping individuals obtain a sponsor was not tested in this study, in an investigation of another type of 12-step facilitation called Making AA Easy, results showed that the treatment led to better outcomes for those with prior 12-step experience, in part, by helping participants obtain 12-step sponsors.
This finding that interventions can boost likelihood of active 12-step involvement is particularly important given the many preconceived notions of what leads to success in 12-step groups (e.g., how religious one is or belief in the disease model of addiction) and may affect how likely one is to attend groups. For those who attend, it may be important to recognize the types of factors that increase likelihood of drop out.
A 12-step facilitation intervention like the one delivered in this study, may help overcome some of these attitudinal and practical barriers to 12-step participation. In turn, this increased 12-step participation can help boost alcohol and other drug outcomes over time irrespective of initial attitudes.
- LIMITATIONS
-
- The main limitation is that individuals were not randomized to receive or not receive a sponsor. In context of other sponsor related research with similar findings, though, it seems more likely than not that having sponsor is causally related to better alcohol and other drug outcomes.
- Also, the study only investigated outcomes 1-month post-treatment, a relatively short period of time. Again, though, other studies in this area mentioned earlier have found similar results when following individuals for 9-12 months.
- The goal of the study was to see whether “treatment-as-usual”, which also includes encouragement to attend 12-step organizations and to get a sponsor, could be improved upon by implementing a more focused, systematic, and rigorous 12-step facilitation. Consequently, because the “treatment-as-usual” comparison condition also strongly encouraged participants to actively participate in 12-step groups and to obtain a sponsor, this could have weakened the effect of the more rigorous 12-step facilitation intervention.
NEXT STEPS
The study cannot speak to why having a sponsor might be helpful to substance use disorder outcomes. For example, Kelly and colleagues showed that the quality of the relationship between an individual and his/her sponsor is related to better substance use outcomes. In another study, they showed that beneficial effects of having a sponsor are not explained by its ability to promote changes in an individual’s social network. From several theoretical standpoints, however, it is likely that the regular (often daily) monitoring, accountability, encouragement, imparting of recovery coping skills, and recovery role modeling, may help explain some of these beneficial effects of having a sponsor. In addition to studying these potential mechanisms, next steps might investigate whether sponsor benefits depend on individual factors (e.g., age, gender, and race/ethnicity) or clinical factors (e.g., the presence of a co-occurring psychiatric disorder in addition to substance is disorder).
Finally, there is not an obvious explanation for the finding that having a sponsor was related to better illicit drug, but not alcohol outcomes, especially given the strong emphasis on abstinence from all mood-altering psychoactive substances in 12-step organizations. Future studies might seek to replicate this particular finding and examine in more detail why it may be the case.
BOTTOM LINE
- For individuals & families seeking recovery: There is a good accumulation of evidence that obtaining a 12-step sponsor is likely to improve recovery rates over time. More research is needed, however, to understand exactly what is it about one’s relationship with a sponsor that helps support recovery.
- For scientists: There is a good accumulation of evidence that obtaining a 12-step sponsor is likely to improve recovery rates over time. More research is needed, however, to understand exactly what is it about one’s relationship with a sponsor that helps support recovery. Furthermore, research is needed to understand whether certain individuals benefit more from having a sponsor than others.
- For policy makers: There is a good accumulation of evidence that obtaining a 12-step sponsor is likely to improve recovery rates over time. Recovery-supportive services delivered in the community, such as recovery community centers, may benefit from policies that emphasize obtaining a 12-step sponsor if not already doing so.
- For treatment professionals and treatment systems: There is a good accumulation of evidence that obtaining a 12-step sponsor is likely to improve recovery rates over time. In addition, clinical interventions that emphasize obtaining a 12-step sponsor can improve one’s chances of doing so compared to interventions that do not have that explicit focus.
CITATIONS
Wendt, D. C., Hallgren, K. A., Daley, D. C., & Donovan, D. M. (2017). Predictors and Outcomes of Twelve-Step Sponsorship of Stimulant Users: Secondary Analyses of a Multisite Randomized Clinical Trial. Journal of Studies on Alcohol and Drugs, 78(2), 287-295.
