
For Opioid Use Disorder, Does Cannabis Produce Harm or Reduce Harm?
Theories abound that cannabis use can help individuals recover from opioid use disorder or may serve as a less-risky pain management approach to pharmaceutical opioids. In this study scientists took an empirical, prospective look at the relationship between cannabis and opioid use disorder.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Opioid overdose deaths have continued to climb from 33,000 in 2015 to 42,000 in 2016. It is critical to identify as many strategies as possible to curb this public health trend. Due to research showing that passing medical marijuana laws is associated with a decrease in opioid overdose deaths and hospitalizations, some speculate marijuana could reduce the chances of overdose death.
One theory is that marijuana can be an alternative to opioid medications for individuals who are coping with chronic pain. It is difficult, however, to draw conclusions from research on which advocates of medical marijuana as an antidote to opioid overdose have based their claims. These studies, while certainly important, speak to trends at population levels (e.g., by state) not for a given individual. That is, while the availability of medical marijuana at a state level might be associated with decreased rates of opioid overdose in that population of individuals (e.g., all the residents in a state), that does not necessarily mean that, for any given individual, marijuana helps decrease opioid use and subsequent increased chances of overdose.
Another theory is that using cannabis to get high may serve similar functions as opioid use (e.g., producing euphoria, reducing stress, etc.) in a less intense way and without an overdose risk. Epidemiological research where individuals are followed over time, however, suggests marijuana use might actually predispose someone to develop a drug use disorder, including but not limited to opioid use disorder. This study by Olfson and colleagues helped shed some light on this issue by investigating how cannabis use at one point in time relates to nonmedical use of pharmaceutical opioids (i.e., prescription painkillers) and opioid use disorder in US adults 3 years later.
HOW WAS THIS STUDY CONDUCTED?
This study used data from two measurement periods (i.e., “waves”) of the National Epidemiological Study on Alcohol and Related Conditions (NESARC) collected in 2001-2002 (called Wave 1) and 2004-2005 (Wave 2). Authors investigated whether cannabis use at Wave 1 predicted opioid use and opioid use disorder at Wave 2.
- MORE ON STUDY METHODS
-
To control for some (but not all) potential alternative explanations – thus increasing confidence that cannabis use is causing increases or decreases in opioid outcomes – authors controlled statistically for the effects of age, race/ethnicity, having first degree relatives with substance use and other psychiatric disorders, antisocial personality disorder, substance use disorders, and mood and anxiety disorders.
They assessed for substance use and other psychiatric disorder with a structured interview for the diagnostic and statistical manual of mental disorders, 4th edition (DSM-IV). In their analyses, they examined not only prevalence of opioid use and opioid use disorder (“Is it there?”) but also the incidence, which we refer to as new-onset (“Is it there for the first time?”). Furthermore they examined a number of factors that might alter the strength of the relationship between cannabis and opioid use, such as whether or not someone had a cannabis use disorder or whether they were in physical pain.
Here are some key definitions and measurements from the study:
- Nonmedical use of pharmaceutical opioids (i.e., non-heroin): Use “without a prescription, in greater amounts, more often, or longer than prescribed, or for a reason other than the doctor said you should use them”
- Cannabis use and opioid use in the past 12 months (In most analyses the three use categories were combined into any use (Yes) compared to no use).:
- No use
- Occasional use = less than once a month
- Frequent use = once a month to twice a week
- Very frequent use = Three times per week to everyday.
- Pain: Measured with the Short Form Health Survey (SF-12), where no or little interference from pain during the past month was categorized as No pain and moderate to extreme interference with pain during the past month was categorized as Pain
WHAT DID THIS STUDY FIND?
First it is worth noting that cannabis users were more severe than non-users including greater rates of substance use disorder and mood and anxiety disorders. Cannabis users and non-users, however, had similar rates of pain.
THE EFFECTS OF CANNABIS ON OPIOID USE
Cannabis users had 3.5 times greater odds of any opioid use and 2.6 times greater odds of new-onset opioid use 3 years later. These odds were essentially the same when excluding people that had cannabis use disorder, suggesting these rates applied both to individuals using cannabis “recreationally” and those for whom it caused problems in their life. For individuals with pain, odds of subsequent opioid use and new-onset opioid use in cannabis users compared to non-users were even higher. For individuals who used opioids in the year before entering the study, cannabis use was related to significantly increased opioid use. This was also true for those both with pain and opioid use when entering the study, but because of the smaller number of individuals to analyze, the effects were not statistically significant.
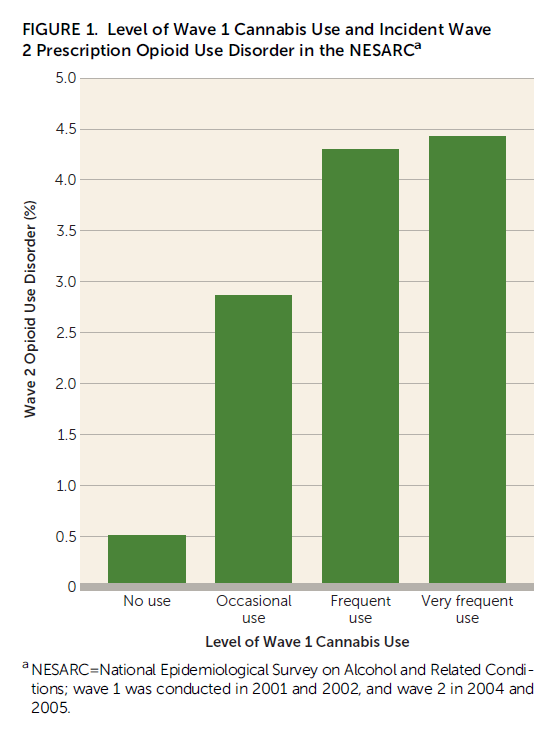
THE EFFECT OF CANNABIS ON OPIOID USE DISORDER
Looking at the raw percentages as shown in the figure below, cannabis users were more likely than non-users to experience new-onset opioid use disorder 3 years later. For example, frequent users (ranging from once a month to twice a week) had an 8-fold greater chance of subsequent, new-onset opioid use disorder compared to non-users. Even after adjusting for all the demographic and clinical variables listed in “How was this study conducted?” – cannabis users had 2.2 times greater odds of new-onset opioid use disorder than non-users (a significant relationship). Taking those with cannabis use disorder out of analyses, however, and the relationship between cannabis use and new-onset opioid use disorder is no longer significant. Similarly, when examining only the individuals with pain, there is no relationship between cannabis use and new-onset opioid use disorder.
WHY IS THIS STUDY IMPORTANT?
This study uses individual data such that someone’s cannabis use can be tied directly to their opioid use and opioid use disorder. On the other hand, studies that have found medical marijuana laws are related to reduced opioid overdose use group-level data. Using these kinds of group level data to understand individuals is called the ecological fallacy, and while they can be very informative in terms of overall trends in a population, caution should be made when extrapolating from these group-level data to individuals.
The most important finding in this study is that cannabis use is related to greater odds of both new-onset opioid use and opioid use disorder 3 years later, even when adjusting for many potential factors that could explain this relationship.
For example, the analyses adjusted for mood and anxiety disorders, so that the findings are not readily explained by the greater presence of depression in cannabis users, which could lead to greater use of substances, overall, in order to cope with unpleasant feelings and experiences. It is also important that, when looking at opioid use disorder, authors accounted for whether participants were initially using any opioids. So it is unlikely that greater access to substances more generally among the cannabis users is what is explaining the greater likelihood of opioid use disorder.
Overall, this study is important because it focuses on an important public health problem – the opioid overdose crisis – and addresses a question in the field – how cannabis use affects opioid use. While presenting stronger evidence of an association between cannabis use and greater chances of subsequent opioid use and opioid use disorder, the design of the study prevents strong causal conclusions. More tightly controlled research is needed to arrive at more definitive conclusions about the impact of cannabis use on opioid use for everyone, but especially for individuals with chronic pain.
- LIMITATIONS
-
- Substance use in this study – cannabis and opioid use – was measured with yes/no response items in analyses. These findings do not speak to frequency of opioid use and/or the severity of the opioid use disorder.
- While opioid use and opioid use disorder are clear risk factors for opioid overdose, they are not perfect substitutes. The study does not include information about the impact of cannabis on opioid overdose.
- As authors mention, the study was conducted several years ago. The changing social context of cannabis use (i.e., less stigmatized and reduced perception of harm) could counter effects seen here, while on the other hand, increased THC content in marijuana since that time could magnify any risks of cannabis use on later opioid use.
NEXT STEPS
There is a critical need for controlled studies in this area. Randomized controlled trials are gold standards for determining whether one factor causes, at least in part, a particular outcome. Some point to potential ethical problems of randomizing individuals to consume cannabis, though, as with all studies, we must weigh the potential benefits of gaining knowledge against the risks of conducting such a study. The potential benefits of knowledge regarding fatal opioid overdose and its relationship to cannabis use, the consumption of which is not known directly to cause death, appear to outweigh the risks.
For adolescents, however, there are greater risks of cannabis use on the brain compared to adults. Animal studies have shown that cannabis exposure in adolescence predisposes adults to greater self-administration of heroin. Such studies in humans, however, would be unethical. Thus it is important to mention there are also more technical ways to try and equate cannabis and non-cannabis users than was done here, such as propensity score matching, which would find a statistical non-cannabis using “match” for each cannabis user based on a series of individual characteristics. In that case, theoretically, the groups would be similar and group differences between individuals who use cannabis and those who do not use cannabis could be more readily attributed to the cannabis use, rather than some other factor.
BOTTOM LINE
- For individuals & families seeking recovery: Cannabis use is related prospectively to using opioids as well as developing opioid use disorder for the first time. While definitive conclusions cannot be made from this single study, its finding in a large, representative sample of US adults that ties individuals’ cannabis use to their subsequent opioid use runs counter to theories that marijuana is a potential harm-reduction option for individuals recovering from opioid use disorder or may be an alternative to opioids for individuals coping with pain.
- For scientists: This secondary analysis of a widely-utilized epidemiological dataset showed cannabis use is related prospectively to new-onset opioid use and opioid use disorder. While these findings do not support the use of marijuana as a harm reduction strategy or as an alternative chronic pain management strategy, more rigorous studies are needed to determine whether marijuana is a risk factor for opioid use and opioid use disorder as suggested by these conclusions (see “What are the next steps in this line of research” for more detail), or if it may provide benefit in more controlled studies.
- For policy makers: Cannabis use is related prospectively to using opioids as well as developing opioid use disorder for the first time. While definitive conclusions cannot be made from this single study, its finding in a large, representative sample of US adults that ties individuals’ cannabis use to their subsequent opioid use runs counter to theories that marijuana is a potential harm-reduction option for individuals recovering from opioid use disorder or may be an alternative to opioids for individuals coping with pain. Given the widely increasing discourse that marijuana may be helpful in addressing the opioid overdose crisis, as well as the changing legal landscape of marijuana leading to increased availability, policies and funding that facilitate research on the effects of cannabis use – both its potential benefits and harms – are needed.
- For treatment professionals and treatment systems: Cannabis use is related prospectively to using opioids as well as developing opioid use disorder for the first time. Individuals with a history of cannabis use disorder may be particularly vulnerable to cannabis use as a risk factor for later opioid use. Those with prior opioid use tend to experience an increase in their opioid use if they use cannabis. While definitive conclusions cannot be made from this single study, its finding in a large, representative sample of US adults that ties individuals’ cannabis use to their subsequent opioid use runs counter to theories that marijuana is a potential harm-reduction option for individuals recovering from opioid use disorder or may be an alternative to opioids for individuals coping with pain. Treatment providers may wish to consider these data to inform discussions with patients who are using cannabis to reduce opioid-related harms.
CITATIONS
Olfson, M., Wall, M. M., Liu, S. M., & Blanco, C. (2017). Cannabis use and risk of prescription opioid use disorder in the United States. American Journal of Psychiatry, 175(1), 47-53.
