Patients visiting the emergency department benefit from specialized hospital-based addiction support
When people experience substance-related consequences, they may show up to emergency departments, providing an opportune time to help alter the future course of their substance use – not just provide acute care. This study compared outcomes for those presenting to the emergency room who received substance use disorder services to those who did not.
In particular, emergency departments are well positioned to meaningfully engage people with substance use disorder. For instance, deploying recovery coaches in emergency departments and initiating medications for the treatment of substance use disorders may be able to help engage people with substance use disorders in care. The researchers in this study examined the impact of hospital-based interventions for substance use disorders on the frequency of returning to the emergency department, an important marker of an individual’s level of functioning and financial burden to the health care system. This research can help test whether hospital-based interventions are effective in improving the health outcomes of people with substance use disorder.
HOW WAS THIS STUDY CONDUCTED?
The research team compared the frequency of returning to the emergency room between those who received 2 different hospital-based interventions for substance use disorder and those who presented to the emergency room but did not receive specialized addiction services. The researchers retrospectively examined administrative data from all patients with a substance use disorder presenting at the Health Sciences North hospital in Ontario, Canada between 2018 and 2022.
Administrative data included medical records from January 1, 2018 through August 31, 2022 and were obtained from the Discharge Abstract Database and the National Ambulatory Care Reporting System database. The Discharge Abstract Database provided information on all hospital admissions and discharges during the study period. The National Ambulatory Care Reporting System database provided information on emergency department visits, discharges, and diagnosis codes.
The two hospital-based interventions were (1) addiction medicine consult services and (2) the specialized addiction medicine unit (AMU group). The addiction medicine consult services were offered both to patients in the emergency department and to those who were hospitalized, which were considered separately in analyses.
The addiction medicine unit is a specialized inpatient medical unit designed to offer addiction support to stabilize patients. To be admitted to the unit, patients must have had an acute medical or psychiatric diagnosis and require ongoing care alongside active addiction concerns, or be in acute withdrawal that required medical monitoring. These 2 intervention groups were compared to people who visited the emergency department and were either discharged or admitted to an inpatient unit, but did not receive any addiction services.
The primary outcome was returning to the emergency department for any cause within 30 days of discharge from the hospital or emergency department with a primary or secondary diagnosis of a substance use disorder (i.e., an “index event”). The researchers were also interested in the first return to the emergency department across 1 year after the index discharge date. Additionally, the researchers collected information on patients’ age, biological sex, homelessness, and visits to the emergency department or hospital for mental health.
The researchers analyzed the data in 2 ways that allowed them to answer different questions. The first way allowed them to determine whether a return to the emergency department had occurred. The second way allowed them to determine the time until a return had occurred.
Participants across groups included a total of 5,267 patients, of which 62% were male and 19% were experiencing homeless. Among the 5,267 patients, there 10,871 index events (i.e., discharges from emergency department or hospital) and 2,127 returns to the emergency department, resulting in a return event rate of 19.6% – that is, overall, 1 in every 5 discharges where substance use disorder was a documented diagnosis resulted in another subsequent emergency department visit. The reason the majority of patients (over 50%) had a first index event was mental health or substance use-related.
WHAT DID THIS STUDY FIND?
Addiction Medicine Consult Services reduced the frequency of returning to the emergency department both short- and long-term
Patients receiving Addiction Medicine Consult Services in the emergency department (but not when hospitalized) were 47% less likely to return to the emergency department within the first 30 days following discharge and were 58% less likely to return within the first year after a discharge than those who presented to the emergency department but did not receive any addiction services.
Patients receiving these services also had a 42% decreased risk of returning to the emergency department within the first 30 days and a 55% decreased risk of a revisit within the first year after a discharge than those who presented to the emergency department but did not receive any addiction service.
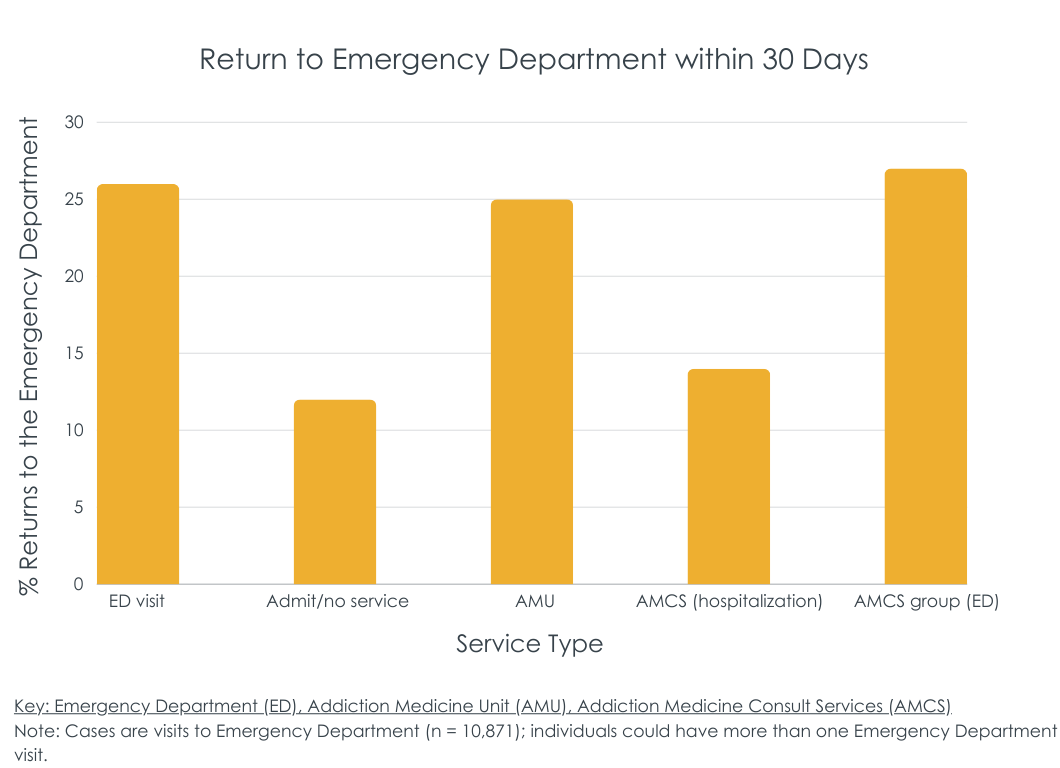
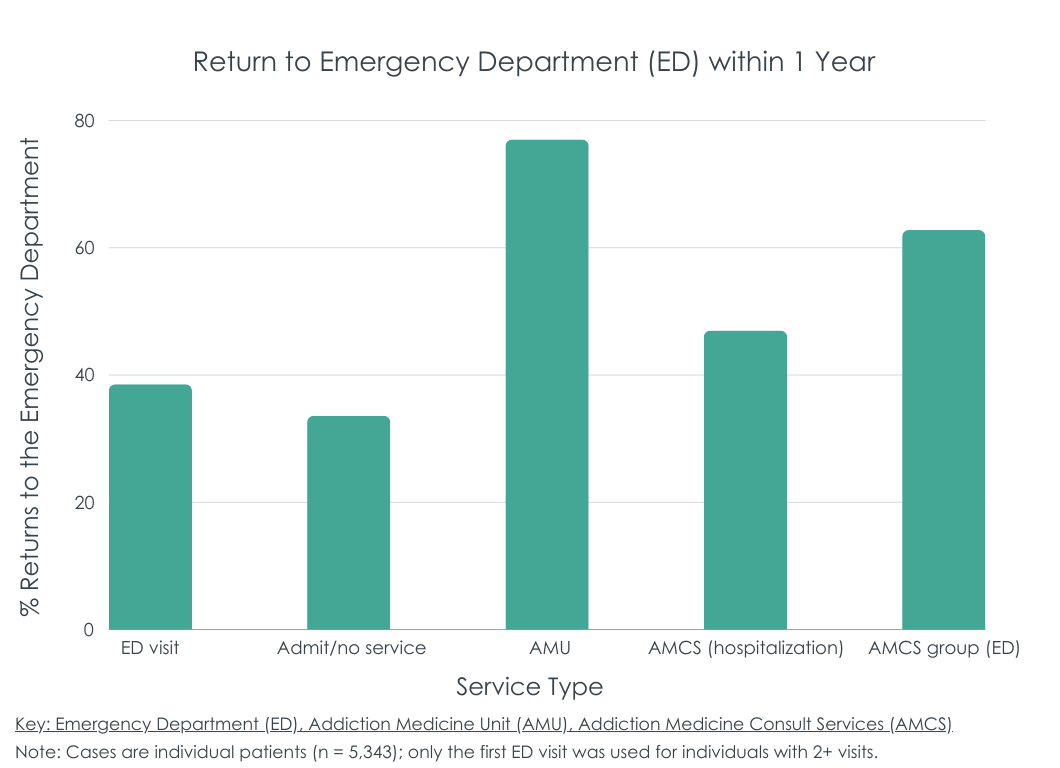
The figures below show raw rates of return to the emergency department by group within 30 days of discharge and within 1 year of discharge. Of note, these raw data do not control for any group differences like the analyses did – these covariates included age, biological sex, homelessness, and visits to the ED or hospital for mental health, as well as the presence of alcohol or opioid use disorder diagnoses in their medical chart at the time of admission to the emergency department.
Addiction Medical Unit patients had reductions in emergency department visits long-term, but not immediately
After accounting for variables like age, homelessness, and presence of alcohol or opioid use disorder in one’s chart when admitted, patients who were admitted to the specialty Addiction Medical Unit were 20% less likely to return to the emergency department within the first year after a discharge compared to those who presented to the emergency department but did not receive addiction services. However, there were no differences between these patients and patients who presented to the emergency department but did not receive addiction services during the first 30 days following discharge.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study examined whether hospital-based interventions for substance use disorder could decrease the frequency of returns to the emergency department, as compared to the standard of care, which does not involve specialized addiction services. They showed that Addiction Medicine Consult Services offered in the emergency department reduced the frequency of returning to the emergency department within the first 30 days of discharge and beyond that 30-day window, while the Addiction Medicine Unit reduced returns to the emergency department outside of the initial 30-day window following discharge. Accordingly, offering support to people with substance use disorder in a hospital-based setting, or in other words, “meeting people where they are” and adhering to the principles of harm reduction, seems to have beneficial health effects, as demonstrated by fewer returns to the emergency department.
Of note, however, is that researchers were not able to equate the study groups based on all variables that might have affected the results, making the study vulnerable to “selection biases”. While they were able to control for several influences, there are likely other factors that may be affecting the results. For example, patients who were admitted to the specialty treatment Addiction Medicine Unit had more severe clinical profiles, on average, than those who received the less intensive Consult Services. Any advantage for the consult services here are due, in part, to being less severe than those linked to the specialty inpatient treatment program. The research design also limits the extent to which the researchers can conclude the association between hospital-based interventions and reduced frequency of returning to the emergency department is causal – the study did not include information about patients’ health beyond returning to the emergency department.
Despite these limitations, the results still support the overall conclusion that offering addiction services to people with substance use disorders who present to the emergency department is likely to be beneficial. In a separate study, for each patient who receives an addiction consultation, the hospital saved an average of $203 per year. Another study found that patients receiving referrals to a hospital-based intervention program were twice as likely to engage in treatment after discharge than patients who were not referred. Taken together, these results add to the growing research base demonstrating that offering addiction consultations to people in the hospital can save costs and improve patients’ engagement in treatment.
The study was observational and used administrative data. This design limits the extent to which the researchers can conclude that the association between hospital-based interventions and revisit recurrence is causal.
Also because the study used observational data, the researchers were not able to entirely equate the study groups based on variables that can affect the results, which can result in selection bias effects. For example, patients who were admitted to the Addiction Medicine Unit had more severe clinical profiles, on average, than those who received the less intensive Consult Services. Any advantage for the consult services here are due, in part, to being less severe than those linked to the specialty inpatient treatment program.
One other note regarding the observational nature of the study were some issues with clarity both in terms of the measurement of certain variables – like the presence of alcohol and opioid use disorders – and in terms of the presentation of certain findings – like whether long-term effects were examined across 1 year or the entire 4 year study period. While an important study with major public health significance, these minor issues with study design clarity should be considered when interpreting the findings.
The study was conducted at one hospital in Ontario, Canada. Thus, the results may not generalize to other medical settings or locations.
BOTTOM LINE
For people with substance use disorder who show up to the emergency department, offering them support and linkage to services may protect against returning, both short- and long-term.
For individuals and families seeking recovery: This study showed that hospital-based interventions for substance use disorder can help reduce returns to the emergency department, thereby suggesting improved health outcomes. Accordingly, if individuals with substance use disorder are offered such services when presenting to the emergency department, those who take advantage of them may have a lower risk of a revisit.
For treatment professionals and treatment systems: Hospital-based interventions for substance use disorder have shown that they can help reduce the frequency of returning to the emergency department, in part by adhering to harm reduction principles and “meeting people where they are”. This clearly applies to treatment professionals who work in hospital settings, but professionals who work in other medical settings and engage in harm reduction principles may similarly see beneficial health outcomes.
For scientists: Because the current study was observational and not able to determine whether participation in addiction-based hospital services caused reductions in emergency department revisits, future research that uses different research designs (e.g., experimental and quasi-experimental longitudinal designs) may be able to help shed light on the extent to which hospital-based interventions were causally related to improved outcomes. Also, given that the different interventions yielded slightly different results, future research that examines differences between interventions will help uncover which interventions are likely to be the most beneficial and which aspects of each are accounting for any observed benefits (e.g., dismantling studies). Finally, studies that are conducted in different medical settings and in different locations can demonstrate whether the results from the current study generalize to other contexts. Sub-group analyses, will likely also help uncover for which type of patient, in particular, which types of interventions may be best suited.
For policy makers: This study showed receiving hospital-based interventions were associated with reductions in the frequency of returns to the emergency department, which supports the notion that harm reduction efforts can help improve health outcomes. Accordingly, supporting policies that promote harm reduction efforts can have beneficial public health effects. However, since the researchers in this study cannot determine the extent to which the association was causal, funding for additional research with more rigorous designs could help shed light on the causal effects of such interventions.
In particular, emergency departments are well positioned to meaningfully engage people with substance use disorder. For instance, deploying recovery coaches in emergency departments and initiating medications for the treatment of substance use disorders may be able to help engage people with substance use disorders in care. The researchers in this study examined the impact of hospital-based interventions for substance use disorders on the frequency of returning to the emergency department, an important marker of an individual’s level of functioning and financial burden to the health care system. This research can help test whether hospital-based interventions are effective in improving the health outcomes of people with substance use disorder.
HOW WAS THIS STUDY CONDUCTED?
The research team compared the frequency of returning to the emergency room between those who received 2 different hospital-based interventions for substance use disorder and those who presented to the emergency room but did not receive specialized addiction services. The researchers retrospectively examined administrative data from all patients with a substance use disorder presenting at the Health Sciences North hospital in Ontario, Canada between 2018 and 2022.
Administrative data included medical records from January 1, 2018 through August 31, 2022 and were obtained from the Discharge Abstract Database and the National Ambulatory Care Reporting System database. The Discharge Abstract Database provided information on all hospital admissions and discharges during the study period. The National Ambulatory Care Reporting System database provided information on emergency department visits, discharges, and diagnosis codes.
The two hospital-based interventions were (1) addiction medicine consult services and (2) the specialized addiction medicine unit (AMU group). The addiction medicine consult services were offered both to patients in the emergency department and to those who were hospitalized, which were considered separately in analyses.
The addiction medicine unit is a specialized inpatient medical unit designed to offer addiction support to stabilize patients. To be admitted to the unit, patients must have had an acute medical or psychiatric diagnosis and require ongoing care alongside active addiction concerns, or be in acute withdrawal that required medical monitoring. These 2 intervention groups were compared to people who visited the emergency department and were either discharged or admitted to an inpatient unit, but did not receive any addiction services.
The primary outcome was returning to the emergency department for any cause within 30 days of discharge from the hospital or emergency department with a primary or secondary diagnosis of a substance use disorder (i.e., an “index event”). The researchers were also interested in the first return to the emergency department across 1 year after the index discharge date. Additionally, the researchers collected information on patients’ age, biological sex, homelessness, and visits to the emergency department or hospital for mental health.
The researchers analyzed the data in 2 ways that allowed them to answer different questions. The first way allowed them to determine whether a return to the emergency department had occurred. The second way allowed them to determine the time until a return had occurred.
Participants across groups included a total of 5,267 patients, of which 62% were male and 19% were experiencing homeless. Among the 5,267 patients, there 10,871 index events (i.e., discharges from emergency department or hospital) and 2,127 returns to the emergency department, resulting in a return event rate of 19.6% – that is, overall, 1 in every 5 discharges where substance use disorder was a documented diagnosis resulted in another subsequent emergency department visit. The reason the majority of patients (over 50%) had a first index event was mental health or substance use-related.
WHAT DID THIS STUDY FIND?
Addiction Medicine Consult Services reduced the frequency of returning to the emergency department both short- and long-term
Patients receiving Addiction Medicine Consult Services in the emergency department (but not when hospitalized) were 47% less likely to return to the emergency department within the first 30 days following discharge and were 58% less likely to return within the first year after a discharge than those who presented to the emergency department but did not receive any addiction services.
Patients receiving these services also had a 42% decreased risk of returning to the emergency department within the first 30 days and a 55% decreased risk of a revisit within the first year after a discharge than those who presented to the emergency department but did not receive any addiction service.
The figures below show raw rates of return to the emergency department by group within 30 days of discharge and within 1 year of discharge. Of note, these raw data do not control for any group differences like the analyses did – these covariates included age, biological sex, homelessness, and visits to the ED or hospital for mental health, as well as the presence of alcohol or opioid use disorder diagnoses in their medical chart at the time of admission to the emergency department.
Addiction Medical Unit patients had reductions in emergency department visits long-term, but not immediately
After accounting for variables like age, homelessness, and presence of alcohol or opioid use disorder in one’s chart when admitted, patients who were admitted to the specialty Addiction Medical Unit were 20% less likely to return to the emergency department within the first year after a discharge compared to those who presented to the emergency department but did not receive addiction services. However, there were no differences between these patients and patients who presented to the emergency department but did not receive addiction services during the first 30 days following discharge.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study examined whether hospital-based interventions for substance use disorder could decrease the frequency of returns to the emergency department, as compared to the standard of care, which does not involve specialized addiction services. They showed that Addiction Medicine Consult Services offered in the emergency department reduced the frequency of returning to the emergency department within the first 30 days of discharge and beyond that 30-day window, while the Addiction Medicine Unit reduced returns to the emergency department outside of the initial 30-day window following discharge. Accordingly, offering support to people with substance use disorder in a hospital-based setting, or in other words, “meeting people where they are” and adhering to the principles of harm reduction, seems to have beneficial health effects, as demonstrated by fewer returns to the emergency department.
Of note, however, is that researchers were not able to equate the study groups based on all variables that might have affected the results, making the study vulnerable to “selection biases”. While they were able to control for several influences, there are likely other factors that may be affecting the results. For example, patients who were admitted to the specialty treatment Addiction Medicine Unit had more severe clinical profiles, on average, than those who received the less intensive Consult Services. Any advantage for the consult services here are due, in part, to being less severe than those linked to the specialty inpatient treatment program. The research design also limits the extent to which the researchers can conclude the association between hospital-based interventions and reduced frequency of returning to the emergency department is causal – the study did not include information about patients’ health beyond returning to the emergency department.
Despite these limitations, the results still support the overall conclusion that offering addiction services to people with substance use disorders who present to the emergency department is likely to be beneficial. In a separate study, for each patient who receives an addiction consultation, the hospital saved an average of $203 per year. Another study found that patients receiving referrals to a hospital-based intervention program were twice as likely to engage in treatment after discharge than patients who were not referred. Taken together, these results add to the growing research base demonstrating that offering addiction consultations to people in the hospital can save costs and improve patients’ engagement in treatment.
The study was observational and used administrative data. This design limits the extent to which the researchers can conclude that the association between hospital-based interventions and revisit recurrence is causal.
Also because the study used observational data, the researchers were not able to entirely equate the study groups based on variables that can affect the results, which can result in selection bias effects. For example, patients who were admitted to the Addiction Medicine Unit had more severe clinical profiles, on average, than those who received the less intensive Consult Services. Any advantage for the consult services here are due, in part, to being less severe than those linked to the specialty inpatient treatment program.
One other note regarding the observational nature of the study were some issues with clarity both in terms of the measurement of certain variables – like the presence of alcohol and opioid use disorders – and in terms of the presentation of certain findings – like whether long-term effects were examined across 1 year or the entire 4 year study period. While an important study with major public health significance, these minor issues with study design clarity should be considered when interpreting the findings.
The study was conducted at one hospital in Ontario, Canada. Thus, the results may not generalize to other medical settings or locations.
BOTTOM LINE
For people with substance use disorder who show up to the emergency department, offering them support and linkage to services may protect against returning, both short- and long-term.
For individuals and families seeking recovery: This study showed that hospital-based interventions for substance use disorder can help reduce returns to the emergency department, thereby suggesting improved health outcomes. Accordingly, if individuals with substance use disorder are offered such services when presenting to the emergency department, those who take advantage of them may have a lower risk of a revisit.
For treatment professionals and treatment systems: Hospital-based interventions for substance use disorder have shown that they can help reduce the frequency of returning to the emergency department, in part by adhering to harm reduction principles and “meeting people where they are”. This clearly applies to treatment professionals who work in hospital settings, but professionals who work in other medical settings and engage in harm reduction principles may similarly see beneficial health outcomes.
For scientists: Because the current study was observational and not able to determine whether participation in addiction-based hospital services caused reductions in emergency department revisits, future research that uses different research designs (e.g., experimental and quasi-experimental longitudinal designs) may be able to help shed light on the extent to which hospital-based interventions were causally related to improved outcomes. Also, given that the different interventions yielded slightly different results, future research that examines differences between interventions will help uncover which interventions are likely to be the most beneficial and which aspects of each are accounting for any observed benefits (e.g., dismantling studies). Finally, studies that are conducted in different medical settings and in different locations can demonstrate whether the results from the current study generalize to other contexts. Sub-group analyses, will likely also help uncover for which type of patient, in particular, which types of interventions may be best suited.
For policy makers: This study showed receiving hospital-based interventions were associated with reductions in the frequency of returns to the emergency department, which supports the notion that harm reduction efforts can help improve health outcomes. Accordingly, supporting policies that promote harm reduction efforts can have beneficial public health effects. However, since the researchers in this study cannot determine the extent to which the association was causal, funding for additional research with more rigorous designs could help shed light on the causal effects of such interventions.
In particular, emergency departments are well positioned to meaningfully engage people with substance use disorder. For instance, deploying recovery coaches in emergency departments and initiating medications for the treatment of substance use disorders may be able to help engage people with substance use disorders in care. The researchers in this study examined the impact of hospital-based interventions for substance use disorders on the frequency of returning to the emergency department, an important marker of an individual’s level of functioning and financial burden to the health care system. This research can help test whether hospital-based interventions are effective in improving the health outcomes of people with substance use disorder.
HOW WAS THIS STUDY CONDUCTED?
The research team compared the frequency of returning to the emergency room between those who received 2 different hospital-based interventions for substance use disorder and those who presented to the emergency room but did not receive specialized addiction services. The researchers retrospectively examined administrative data from all patients with a substance use disorder presenting at the Health Sciences North hospital in Ontario, Canada between 2018 and 2022.
Administrative data included medical records from January 1, 2018 through August 31, 2022 and were obtained from the Discharge Abstract Database and the National Ambulatory Care Reporting System database. The Discharge Abstract Database provided information on all hospital admissions and discharges during the study period. The National Ambulatory Care Reporting System database provided information on emergency department visits, discharges, and diagnosis codes.
The two hospital-based interventions were (1) addiction medicine consult services and (2) the specialized addiction medicine unit (AMU group). The addiction medicine consult services were offered both to patients in the emergency department and to those who were hospitalized, which were considered separately in analyses.
The addiction medicine unit is a specialized inpatient medical unit designed to offer addiction support to stabilize patients. To be admitted to the unit, patients must have had an acute medical or psychiatric diagnosis and require ongoing care alongside active addiction concerns, or be in acute withdrawal that required medical monitoring. These 2 intervention groups were compared to people who visited the emergency department and were either discharged or admitted to an inpatient unit, but did not receive any addiction services.
The primary outcome was returning to the emergency department for any cause within 30 days of discharge from the hospital or emergency department with a primary or secondary diagnosis of a substance use disorder (i.e., an “index event”). The researchers were also interested in the first return to the emergency department across 1 year after the index discharge date. Additionally, the researchers collected information on patients’ age, biological sex, homelessness, and visits to the emergency department or hospital for mental health.
The researchers analyzed the data in 2 ways that allowed them to answer different questions. The first way allowed them to determine whether a return to the emergency department had occurred. The second way allowed them to determine the time until a return had occurred.
Participants across groups included a total of 5,267 patients, of which 62% were male and 19% were experiencing homeless. Among the 5,267 patients, there 10,871 index events (i.e., discharges from emergency department or hospital) and 2,127 returns to the emergency department, resulting in a return event rate of 19.6% – that is, overall, 1 in every 5 discharges where substance use disorder was a documented diagnosis resulted in another subsequent emergency department visit. The reason the majority of patients (over 50%) had a first index event was mental health or substance use-related.
WHAT DID THIS STUDY FIND?
Addiction Medicine Consult Services reduced the frequency of returning to the emergency department both short- and long-term
Patients receiving Addiction Medicine Consult Services in the emergency department (but not when hospitalized) were 47% less likely to return to the emergency department within the first 30 days following discharge and were 58% less likely to return within the first year after a discharge than those who presented to the emergency department but did not receive any addiction services.
Patients receiving these services also had a 42% decreased risk of returning to the emergency department within the first 30 days and a 55% decreased risk of a revisit within the first year after a discharge than those who presented to the emergency department but did not receive any addiction service.
The figures below show raw rates of return to the emergency department by group within 30 days of discharge and within 1 year of discharge. Of note, these raw data do not control for any group differences like the analyses did – these covariates included age, biological sex, homelessness, and visits to the ED or hospital for mental health, as well as the presence of alcohol or opioid use disorder diagnoses in their medical chart at the time of admission to the emergency department.
Addiction Medical Unit patients had reductions in emergency department visits long-term, but not immediately
After accounting for variables like age, homelessness, and presence of alcohol or opioid use disorder in one’s chart when admitted, patients who were admitted to the specialty Addiction Medical Unit were 20% less likely to return to the emergency department within the first year after a discharge compared to those who presented to the emergency department but did not receive addiction services. However, there were no differences between these patients and patients who presented to the emergency department but did not receive addiction services during the first 30 days following discharge.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study examined whether hospital-based interventions for substance use disorder could decrease the frequency of returns to the emergency department, as compared to the standard of care, which does not involve specialized addiction services. They showed that Addiction Medicine Consult Services offered in the emergency department reduced the frequency of returning to the emergency department within the first 30 days of discharge and beyond that 30-day window, while the Addiction Medicine Unit reduced returns to the emergency department outside of the initial 30-day window following discharge. Accordingly, offering support to people with substance use disorder in a hospital-based setting, or in other words, “meeting people where they are” and adhering to the principles of harm reduction, seems to have beneficial health effects, as demonstrated by fewer returns to the emergency department.
Of note, however, is that researchers were not able to equate the study groups based on all variables that might have affected the results, making the study vulnerable to “selection biases”. While they were able to control for several influences, there are likely other factors that may be affecting the results. For example, patients who were admitted to the specialty treatment Addiction Medicine Unit had more severe clinical profiles, on average, than those who received the less intensive Consult Services. Any advantage for the consult services here are due, in part, to being less severe than those linked to the specialty inpatient treatment program. The research design also limits the extent to which the researchers can conclude the association between hospital-based interventions and reduced frequency of returning to the emergency department is causal – the study did not include information about patients’ health beyond returning to the emergency department.
Despite these limitations, the results still support the overall conclusion that offering addiction services to people with substance use disorders who present to the emergency department is likely to be beneficial. In a separate study, for each patient who receives an addiction consultation, the hospital saved an average of $203 per year. Another study found that patients receiving referrals to a hospital-based intervention program were twice as likely to engage in treatment after discharge than patients who were not referred. Taken together, these results add to the growing research base demonstrating that offering addiction consultations to people in the hospital can save costs and improve patients’ engagement in treatment.
The study was observational and used administrative data. This design limits the extent to which the researchers can conclude that the association between hospital-based interventions and revisit recurrence is causal.
Also because the study used observational data, the researchers were not able to entirely equate the study groups based on variables that can affect the results, which can result in selection bias effects. For example, patients who were admitted to the Addiction Medicine Unit had more severe clinical profiles, on average, than those who received the less intensive Consult Services. Any advantage for the consult services here are due, in part, to being less severe than those linked to the specialty inpatient treatment program.
One other note regarding the observational nature of the study were some issues with clarity both in terms of the measurement of certain variables – like the presence of alcohol and opioid use disorders – and in terms of the presentation of certain findings – like whether long-term effects were examined across 1 year or the entire 4 year study period. While an important study with major public health significance, these minor issues with study design clarity should be considered when interpreting the findings.
The study was conducted at one hospital in Ontario, Canada. Thus, the results may not generalize to other medical settings or locations.
BOTTOM LINE
For people with substance use disorder who show up to the emergency department, offering them support and linkage to services may protect against returning, both short- and long-term.
For individuals and families seeking recovery: This study showed that hospital-based interventions for substance use disorder can help reduce returns to the emergency department, thereby suggesting improved health outcomes. Accordingly, if individuals with substance use disorder are offered such services when presenting to the emergency department, those who take advantage of them may have a lower risk of a revisit.
For treatment professionals and treatment systems: Hospital-based interventions for substance use disorder have shown that they can help reduce the frequency of returning to the emergency department, in part by adhering to harm reduction principles and “meeting people where they are”. This clearly applies to treatment professionals who work in hospital settings, but professionals who work in other medical settings and engage in harm reduction principles may similarly see beneficial health outcomes.
For scientists: Because the current study was observational and not able to determine whether participation in addiction-based hospital services caused reductions in emergency department revisits, future research that uses different research designs (e.g., experimental and quasi-experimental longitudinal designs) may be able to help shed light on the extent to which hospital-based interventions were causally related to improved outcomes. Also, given that the different interventions yielded slightly different results, future research that examines differences between interventions will help uncover which interventions are likely to be the most beneficial and which aspects of each are accounting for any observed benefits (e.g., dismantling studies). Finally, studies that are conducted in different medical settings and in different locations can demonstrate whether the results from the current study generalize to other contexts. Sub-group analyses, will likely also help uncover for which type of patient, in particular, which types of interventions may be best suited.
For policy makers: This study showed receiving hospital-based interventions were associated with reductions in the frequency of returns to the emergency department, which supports the notion that harm reduction efforts can help improve health outcomes. Accordingly, supporting policies that promote harm reduction efforts can have beneficial public health effects. However, since the researchers in this study cannot determine the extent to which the association was causal, funding for additional research with more rigorous designs could help shed light on the causal effects of such interventions.