Perceived stigma among people receiving opioid use disorder medication
Stigma toward opioid use disorder and its treatment is a potential barrier to engaging in care, but little is known about experiences of internalization of stigma, called self-stigma, during opioid use disorder medication treatment. This study examined perceived stigma and self-stigma among individuals who have received buprenorphine or methadone treatment.
Medication treatments like buprenorphine and methadone (i.e. opioid agonist treatments) are helpful gold-standard treatments for opioid use disorder that ultimately help to support positive recovery outcomes. In France, nearly 90% of individuals with opioid use disorder that get treatment receive an opioid agonist medication, significantly more common than in the United States (~20%).
Though 3/4 of French patients receive opioid agonist treatment from non-specialty providers (e.g., primary care), these patients are treated by a group constituting only 1/4 of all physicians that have the ability to prescribe opioid agonist treatments – of the physicians eligible to prescribe these medications, 75% choose not to do so. Primary care providers offering initial prescriptions of buprenorphine for opioid use disorder in France declined 44% between 2009 and 2015, and have remained stagnant since 2011, whereas methadone initiations have increased. Similar issues have been observed in the United States, with only about 8% of primary care physicians having prescribed buprenorphine. With rates of opioid use disorder continuing to increase in Europe, the declining involvement of primary care physicians in opioid use disorder medication treatment could reduce buprenorphine availability and threaten the success that France has had with medication treatment uptake.
To address these issues, studies have begun to evaluate the barriers to prescribing medication treatment in primary care, with provider attitudes toward opioid use disorder and its treatment being noted as one potential barrier. Treatment providers’ misconceptions about medication treatment can lead to discriminatory attitudes toward individuals with opioid use disorder. These misconceptions contribute to the negative stereotypes that people hold about individuals with opioid use disorder, perpetuating social stigma and discrimination. This social stigma can lead to discriminatory acts toward individuals with opioid use disorder, contributing to housing, employment, and legal challenges amongst those who are stigmatized. It can also cause individuals with opioid use disorder to believe that others have negative attitudes about them due to their disorder (i.e. perceived stigma). Individuals with opioid use disorder might also internalize the negative attitudes held by the public, impacting identity, self-esteem, and self-worth (i.e. self-stigma). Self-stigma can thereby hinder treatment and recovery, reducing patient hope, empowerment, and treatment initiation/adherence, while increasing risk for other psychiatric symptoms (e.g., depression, anxiety, etc.). Public and perceived stigma towards individuals receiving opioid use disorder medication treatment often persist beyond cessation of illicit opioid use, and exist across multiple life domains (e.g., medical, social, family, professional). This stigma can also reduce providers’ willingness to prescribe medication treatments for opioid use disorder.
Given the impact of stigma on treatment and recovery, increased efforts are needed to better understand experiences of stigma among patients with opioid use disorder. To address this gap, this study assessed perceived-stigma, self-stigma and its relationship to treatment seeking among individuals receiving opioid use disorder medication treatment in France, a country with particularly high rates of medication treatment.
HOW WAS THIS STUDY CONDUCTED?
This was an observational cross-sectional study of perceived- and self-stigma, conducted 2022-2023 among 73 adults who received outpatient medication treatment (i.e. buprenorphine or methadone) from an addiction medicine department at a single hospital in France any time since 2012 (i.e., recruited individuals were both current and past patients). In France, buprenorphine treatment is accessible in a primary care setting, whereas methadone treatment is available via specialized centers. Unlike treatment in the United States, patients receiving methadone from specialized treatment facilities in France have the ability to continue methadone in primary care settings after they reach a stable dose, with methadone prescribed and dispensed at community pharmacies.
The authors evaluated the prevalence of perceived stigma and self-stigma, as well as the relationship between self-stigma and delays in treatment seeking. Patients who had previously received or were currently receiving opioid agonist treatment (i.e. methadone or buprenorphine) for a past or current opioid use disorder at the hospital’s addiction medicine department were invited to participate. Those who enrolled in the study (32% of eligible patients) completed self-report questionnaires concerning demographics, clinical characteristics, perceived stigma, and self-stigma.
Perceived stigma was defined as the belief that others hold negative attitudes or have behaved in discriminatory ways toward them due to their opioid use disorder or status as a patient taking buprenorphine/methadone, and was assessed with a 6-item questionnaire with yes/no responses that was designed for this study. Questionnaire items addressed the quality of the patient’s relationship with their primary care provider, experiences of stigma around opioid use disorder and medication treatment from a medical professional, and avoidance of care seeking due to fear of stigma.
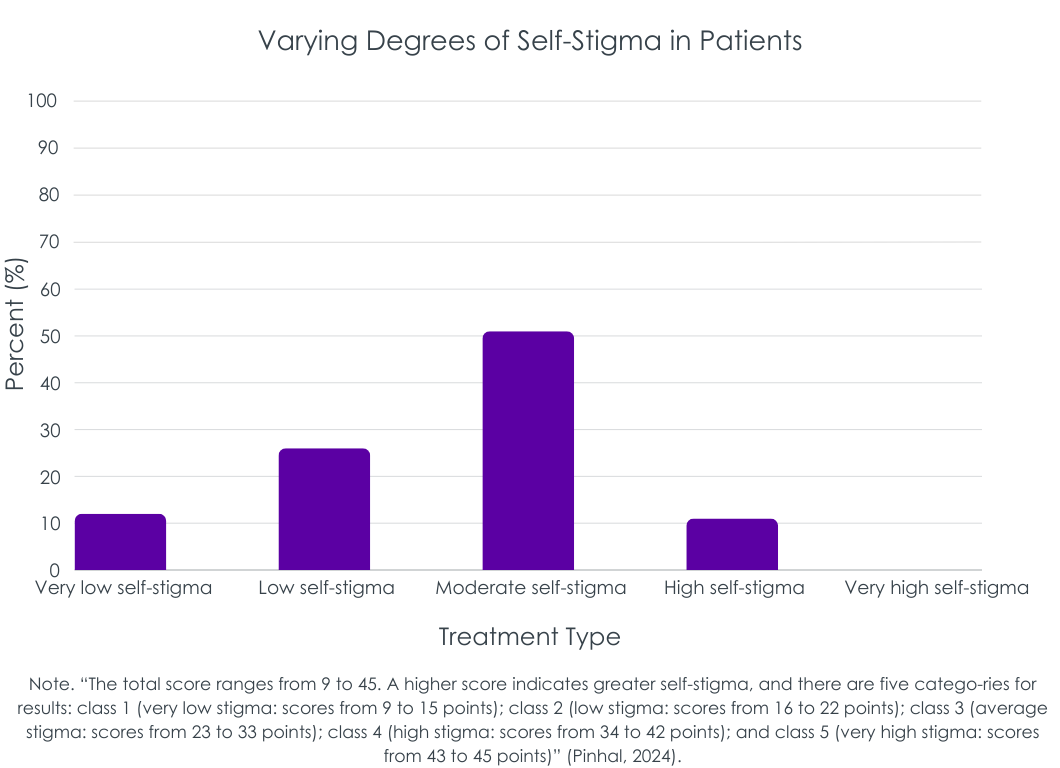
Self-stigma was defined as having stigmatizing attitudes towards oneself, due to the internalization of negative societal attitudes and stereotypes, and was measured with the Self-Stigma Scale-Short inventory, modified to address stigma related to patients receiving opioid agonist treatment. Participants rated their level of agreement with 9 statements about self-stigma. See the figure below for examples of self-stigma items. The total scale score ranged from 9 (low stigma) to 45 (high stigma), and was categorized into 1 of 5 self-stigma severity categories: (1) 9 – 15 points = very low stigma; (2) 16 – 22 = low stigma; (3) 23 – 33 = moderate stigma; (4) 34 – 42 = high stigma; (5) 43 – 45 = very high stigma.
Delays in care seeking were assessed as the time between a patient’s opioid use disorder onset and the start of their first treatment episode. Though participants needed to be current or past patients at a particular university-affiliated addiction treatment program with any history of taking methadone/buprenorphine, the study does not specify whether the treatment onset examined here in relation to self-stigma is receipt of methadone/buprenorphine (or any treatment), or whether the treatment needed to be in their addiction treatment program (or any program). Importantly, it is also unclear how the delay in treatment seeking – from opioid use disorder onset – would be determined if participants entered their system to begin receiving medication – e.g., patients may have provided information to help determine onset of opioid use disorder symptoms or self-reported this information, etc. but the details of how these values were determined is not clear from the study.
The researchers analyzed the percentage of patients who experienced perceived stigma due to their opioid use disorder and medication treatment. The authors then examined mean self-stigma scores, as well as the percentage of patients whose scores fell within each of the 5 self-stigma severity categories. Thereafter, the relationship between self-stigma scores (low vs. high) and patient factors was assessed.
The majority of participants were unemployed (62%) men (73%) in their early forties. Eighty eight percent of participants were currently receiving opioid agonist treatment (63% methadone, 25% buprenorphine), whereas 12% had received opioid agonist treatment in the past but were no longer taking it at the time of the survey. Thirty-two percent of participants had misused opioids in the past 60 days.
WHAT DID THIS STUDY FIND?
Half reported experiencing stigma from healthcare professionals
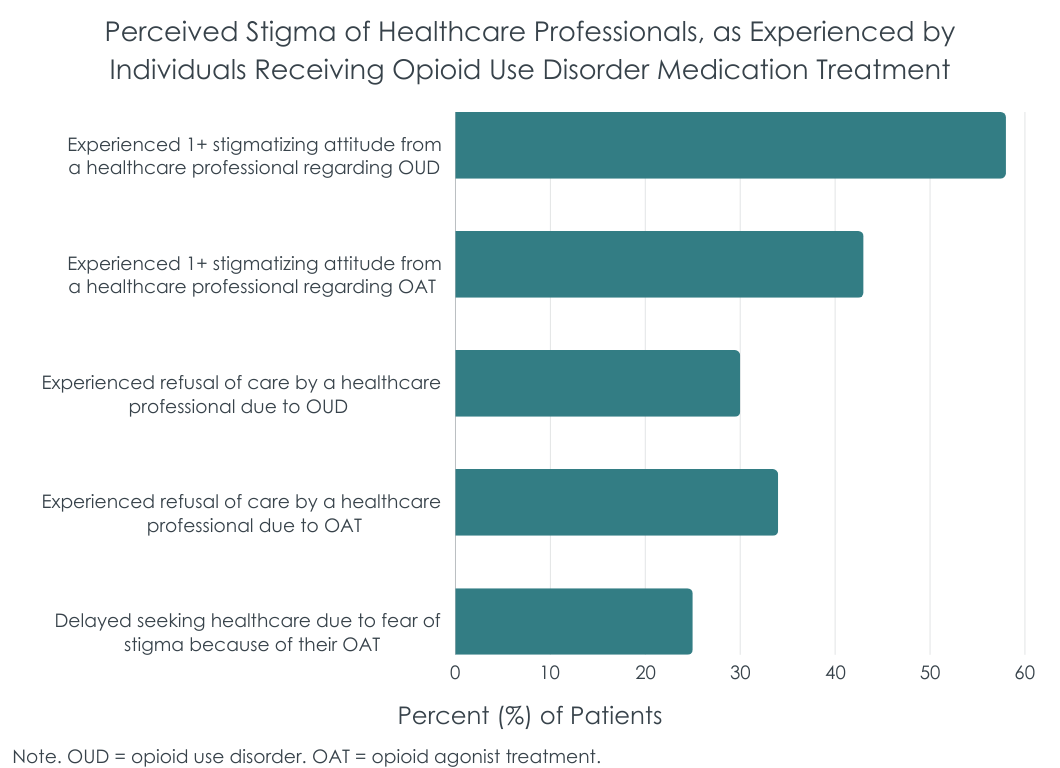
Nearly 50% of patients perceived stigmatizing attitudes from healthcare professionals and about 1/3 were denied care by a healthcare provider due to their opioid use disorder and/or their medication treatment. In addition, about 25% of patients reported that they delayed seeking healthcare due to fear that they would be stigmatized because of their medication treatment. Despite this, 85% of participants reported having a good to moderate quality relationship with their primary care provider.
On average, patients reported a moderate degree of self-stigma
The average self-stigma scale score among patients was 24.7 out of 45 points, reflective of a moderate degree of self-stigma around one’s current/past medication treatment. When self-stigma scores were categorized, 38% of patients had a ‘very low’ or ‘low’ degree of self-stigma, 51% had a ‘moderate’ degree of self-stigma, and 11% had a ‘high’ degree of self-stigma. None of the patients had scores higher than 42 (i.e. ‘very high’ stigma).
Self-stigma was not related to delays in treatment seeking
Self-stigma scores were not significantly related to the amount of time between when the patient’s opioid use disorder onset and when they sought addiction treatment. In addition to not meeting the threshold for statistical significance, the correlation was very small and unlikely to have real world significance as well.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
TIn this study, individuals with a current or past history of opioid agonist medication treatment (i.e. buprenorphine or methadone) in France experienced high rates of self-stigma mostly in the moderate range or below, as well as perceived stigma from healthcare workers, due to their opioid use disorder and medication treatment. Despite this, this self-stigma did not appear to delay treatment-seeking. Given the low response rate of eligible patients (only 32% agreed to participate), that some individuals were reporting on their experience from several years earlier, and differences between the French and U.S. health care systems, it is unclear how representative these findings may be of patients currently treated in France, or how findings may generalize to the United States.
Despite some substantial limitations of this study, findings are, nevertheless somewhat consistent with studies of stigma conducted in other countries and healthcare settings, showing associations between self-stigma and perceived stigma among individuals receiving medication treatment. In addition to healthcare providers being perceived as stigmatizing by individuals receiving medication treatment, prior studies have demonstrated these stigmatizing beliefs among healthcare workers, suggesting that this stigma may not merely be a misperception of patients but potentially actual experiences of enacted stigma. Indeed, about 1/3 of patients in this study reported that they were refused care by a healthcare professional due to their opioid use disorder and medication treatment. Even though France has one of the highest rates of opioid use disorder medication treatment receipt, stigma toward these medication treatments still exists; exposure to and knowledge about medication treatment and patients receiving it may therefore not be enough to combat the stigmatizing beliefs and discriminatory behaviors that have been deeply ingrained in society over the past several decades. This stigma is so prevalent, socioculturally, that individuals who receive medication treatment can internalize these beliefs and may see themselves in ways that reflect these stigmatizing attitudes, which can hinder treatment and recovery progress.
As noted above, one important caveat is that only 32% of eligible patients completed the survey. As such, the findings here may not be representative of all opioid agonist patients in France – it is possible for example, that individuals with especially negative experiences may have taken the opportunity to express those experiences. Financial incentives for participation can protect against these types of selection biases, though the study did not report whether or not financial incentives were offered. That said, given that stigma can reduce providers’ willingness to prescribe and patients’ willingness to receive these medication treatments, novel public health campaigns and efforts within and outside of healthcare institutions are needed to combat stigma toward opioid use disorder and its treatment. The long period over which participants may have been taking the agonist medication – since 2012 – also presents some opportunities to see whether there may be changes in self-stigma over time that could have been related to different types of system changes during that period but such analyses were not reported and, again, the small sample size also would not lend itself well to those kinds of analyses.
However, the literature is still mixed, suggesting that the impact that stigma has on healthcare behaviors and treatment seeking can vary widely. This means other factors can often influence stigma’s effect on actual treatment seeking behaviors. Though this study found no correlation between self-stigma and delayed treatment seeking with respect to a patient’s first opioid use disorder treatment episode, about 25% of medication-treated patients reported that they delayed seeking healthcare more broadly, due to fear that they would be stigmatized because of their current/past use of medication treatment. Thus, for at least a subset of individuals with a history of medication treatment self-stigma may negatively influence healthcare utilization.
Finally, it is worth reiterating that this study was conducted in France where opioid agonist medications are very common. In the US, rates of opioid agonist medication use are much lower. How policy changes that may help mainstream these medications in US healthcare – like ending the requirement for 8 hours of specialized training (i.e., the Drug Enforcement Administration, or DEA, “X waiver”) – will impact prescription rates and patients’ perceived stigma are not yet clear. Overall, this study’s findings warrant additional efforts to better understand recent experiences of stigma and their effects on health-related behaviors and use of healthcare resources across the globe.
Data were collected from a single hospital in France and the study population did not differentiate between patients with current or past opioid use disorder. Stigma may differ in other medical facilities, countries, and at different stages and severity of opioid use disorder.
Only 32% of eligible patients decided to participate in this study. Thus, how representative this select sample may be of patients treated at that hospital (or any other) is unclear and could be biased in some way.
This study was based on self-reported data and information about disorder diagnoses and treatment episodes are therefore subject to self-report bias. Perceived- and self-stigma questions did not ask about stigmatizing beliefs/experiences within a given time frame and rates of stigma may therefore reflect past experiences combined with more recent experiences, demanding additional research.
BOTTOM LINE
About half of the French adults in this study experienced perceived stigma from healthcare professionals due to their opioid use disorder and medication treatment. Self-stigma was also common, with 85% reporting low-moderate degrees of self-stigma and 62% reporting moderate to high degrees of self-stigma around their identity as a person who has received opioid use disorder medication treatment. No one, however, reported very-high self-stigma. Though self-stigma was not significantly related to delays in seeking a first treatment episode for opioid use disorder, about 1/4 of patients reported delaying healthcare seeking more broadly, due to fear that they would be stigmatized because of their medication treatment. Thus, this study also suggests that a subset of people may be delaying general healthcare seeking due to self-stigma, warranting additional research to identify novel methods that help reduce self-stigma in medication treated patients, and that address discrimination and stigmatizing attitudes among the healthcare workforce.
For individuals and families seeking recovery: Amid ongoing efforts to combat stigma and discrimination toward opioid use disorder and its treatment, individuals and families seeking medication treatment are encouraged to find a healthcare team that has experience treating individuals with medication treatment and that uses this experience to provide patient-centered empathetic care. Individuals who feel stigmatized by their healthcare providers are encouraged to find another doctor who better understands medication treatment and that they feel comfortable discussing their opioid use disorder and treatment history with, sans judgement. Individuals experiencing self-stigma might consider joining a support group of peers with lived experience of medication treatment (such as Medication Assisted Recovery Anonymous, or MARA) and/or seeking individual therapy to help address shame and stigma and to develop better self-talk and adaptive behaviors that improve self-image.
For treatment professionals and treatment systems: It is essential for treatment professionals and systems to obtain ongoing training about medication treatment for opioid use disorder to ensure stigmatizing attitudes toward opioid use disorder and its treatment, driven by misconceptions and past personal experiences, do not perpetuate stigma towards individuals who are seeking and receiving treatment for opioid use disorder. These stigmatizing beliefs can lead patients to see themselves in negative ways, and some may even avoid seeking essential healthcare due to fear of being stigmatized by healthcare providers and systems. Challenging stigmatizing beliefs through professional education and exposure, and enacting policy and regulatory changes in healthcare systems around medication treatment may help reduce stigma within healthcare systems, as well as the harm it can cause to the patients these systems treatment.
For scientists: Naturalistic longitudinal investigations are needed to determine the extent to which self-stigma and perceived stigma influence uptake of opioid use disorder medication treatments, and how use of these treatments in turn affect self-stigma and perceived stigma from healthcare professionals and the general public. Studies are needed to determine the factors that moderate – i.e., protect against – the influence of stigma on treatment seeking and healthcare decision making at a micro-, meso-, and macro-level. Examining the relationship between stigma and additional health-related behaviors is warranted to better understand the impact of stigma on treatment seeking, uptake, and retention, as well as patient well-being.
For policy makers: Studies like this help us better understand how beliefs and attitudes toward medication treatment for opioid use disorder affect individuals who receive it, including their beliefs about themselves and their health behaviors. By characterizing patient experiences of stigma and their relationship to treatment and other healthcare seeking behaviors, we can better address the opioid epidemic through an understanding of stigma as a barrier to medication treatment receipt and prescribing, as well as it’s secondary downstream effects on patient healthcare utilization and treatment/recovery outcomes. Healthcare-provider exposure to and knowledge about medication treatment and opioid use disorder may not be enough to combat the deeply ingrained, stigmatizing beliefs held by society and many healthcare professionals. Ongoing funding for research on the ways that medication treatment laws and healthcare regulations impact stigma are essential to inform policy reform that can help combat stigma and discrimination to ultimately better address the opioid epidemic.
Medication treatments like buprenorphine and methadone (i.e. opioid agonist treatments) are helpful gold-standard treatments for opioid use disorder that ultimately help to support positive recovery outcomes. In France, nearly 90% of individuals with opioid use disorder that get treatment receive an opioid agonist medication, significantly more common than in the United States (~20%).
Though 3/4 of French patients receive opioid agonist treatment from non-specialty providers (e.g., primary care), these patients are treated by a group constituting only 1/4 of all physicians that have the ability to prescribe opioid agonist treatments – of the physicians eligible to prescribe these medications, 75% choose not to do so. Primary care providers offering initial prescriptions of buprenorphine for opioid use disorder in France declined 44% between 2009 and 2015, and have remained stagnant since 2011, whereas methadone initiations have increased. Similar issues have been observed in the United States, with only about 8% of primary care physicians having prescribed buprenorphine. With rates of opioid use disorder continuing to increase in Europe, the declining involvement of primary care physicians in opioid use disorder medication treatment could reduce buprenorphine availability and threaten the success that France has had with medication treatment uptake.
To address these issues, studies have begun to evaluate the barriers to prescribing medication treatment in primary care, with provider attitudes toward opioid use disorder and its treatment being noted as one potential barrier. Treatment providers’ misconceptions about medication treatment can lead to discriminatory attitudes toward individuals with opioid use disorder. These misconceptions contribute to the negative stereotypes that people hold about individuals with opioid use disorder, perpetuating social stigma and discrimination. This social stigma can lead to discriminatory acts toward individuals with opioid use disorder, contributing to housing, employment, and legal challenges amongst those who are stigmatized. It can also cause individuals with opioid use disorder to believe that others have negative attitudes about them due to their disorder (i.e. perceived stigma). Individuals with opioid use disorder might also internalize the negative attitudes held by the public, impacting identity, self-esteem, and self-worth (i.e. self-stigma). Self-stigma can thereby hinder treatment and recovery, reducing patient hope, empowerment, and treatment initiation/adherence, while increasing risk for other psychiatric symptoms (e.g., depression, anxiety, etc.). Public and perceived stigma towards individuals receiving opioid use disorder medication treatment often persist beyond cessation of illicit opioid use, and exist across multiple life domains (e.g., medical, social, family, professional). This stigma can also reduce providers’ willingness to prescribe medication treatments for opioid use disorder.
Given the impact of stigma on treatment and recovery, increased efforts are needed to better understand experiences of stigma among patients with opioid use disorder. To address this gap, this study assessed perceived-stigma, self-stigma and its relationship to treatment seeking among individuals receiving opioid use disorder medication treatment in France, a country with particularly high rates of medication treatment.
HOW WAS THIS STUDY CONDUCTED?
This was an observational cross-sectional study of perceived- and self-stigma, conducted 2022-2023 among 73 adults who received outpatient medication treatment (i.e. buprenorphine or methadone) from an addiction medicine department at a single hospital in France any time since 2012 (i.e., recruited individuals were both current and past patients). In France, buprenorphine treatment is accessible in a primary care setting, whereas methadone treatment is available via specialized centers. Unlike treatment in the United States, patients receiving methadone from specialized treatment facilities in France have the ability to continue methadone in primary care settings after they reach a stable dose, with methadone prescribed and dispensed at community pharmacies.
The authors evaluated the prevalence of perceived stigma and self-stigma, as well as the relationship between self-stigma and delays in treatment seeking. Patients who had previously received or were currently receiving opioid agonist treatment (i.e. methadone or buprenorphine) for a past or current opioid use disorder at the hospital’s addiction medicine department were invited to participate. Those who enrolled in the study (32% of eligible patients) completed self-report questionnaires concerning demographics, clinical characteristics, perceived stigma, and self-stigma.
Perceived stigma was defined as the belief that others hold negative attitudes or have behaved in discriminatory ways toward them due to their opioid use disorder or status as a patient taking buprenorphine/methadone, and was assessed with a 6-item questionnaire with yes/no responses that was designed for this study. Questionnaire items addressed the quality of the patient’s relationship with their primary care provider, experiences of stigma around opioid use disorder and medication treatment from a medical professional, and avoidance of care seeking due to fear of stigma.
Self-stigma was defined as having stigmatizing attitudes towards oneself, due to the internalization of negative societal attitudes and stereotypes, and was measured with the Self-Stigma Scale-Short inventory, modified to address stigma related to patients receiving opioid agonist treatment. Participants rated their level of agreement with 9 statements about self-stigma. See the figure below for examples of self-stigma items. The total scale score ranged from 9 (low stigma) to 45 (high stigma), and was categorized into 1 of 5 self-stigma severity categories: (1) 9 – 15 points = very low stigma; (2) 16 – 22 = low stigma; (3) 23 – 33 = moderate stigma; (4) 34 – 42 = high stigma; (5) 43 – 45 = very high stigma.
Delays in care seeking were assessed as the time between a patient’s opioid use disorder onset and the start of their first treatment episode. Though participants needed to be current or past patients at a particular university-affiliated addiction treatment program with any history of taking methadone/buprenorphine, the study does not specify whether the treatment onset examined here in relation to self-stigma is receipt of methadone/buprenorphine (or any treatment), or whether the treatment needed to be in their addiction treatment program (or any program). Importantly, it is also unclear how the delay in treatment seeking – from opioid use disorder onset – would be determined if participants entered their system to begin receiving medication – e.g., patients may have provided information to help determine onset of opioid use disorder symptoms or self-reported this information, etc. but the details of how these values were determined is not clear from the study.
The researchers analyzed the percentage of patients who experienced perceived stigma due to their opioid use disorder and medication treatment. The authors then examined mean self-stigma scores, as well as the percentage of patients whose scores fell within each of the 5 self-stigma severity categories. Thereafter, the relationship between self-stigma scores (low vs. high) and patient factors was assessed.
The majority of participants were unemployed (62%) men (73%) in their early forties. Eighty eight percent of participants were currently receiving opioid agonist treatment (63% methadone, 25% buprenorphine), whereas 12% had received opioid agonist treatment in the past but were no longer taking it at the time of the survey. Thirty-two percent of participants had misused opioids in the past 60 days.
WHAT DID THIS STUDY FIND?
Half reported experiencing stigma from healthcare professionals
Nearly 50% of patients perceived stigmatizing attitudes from healthcare professionals and about 1/3 were denied care by a healthcare provider due to their opioid use disorder and/or their medication treatment. In addition, about 25% of patients reported that they delayed seeking healthcare due to fear that they would be stigmatized because of their medication treatment. Despite this, 85% of participants reported having a good to moderate quality relationship with their primary care provider.
On average, patients reported a moderate degree of self-stigma
The average self-stigma scale score among patients was 24.7 out of 45 points, reflective of a moderate degree of self-stigma around one’s current/past medication treatment. When self-stigma scores were categorized, 38% of patients had a ‘very low’ or ‘low’ degree of self-stigma, 51% had a ‘moderate’ degree of self-stigma, and 11% had a ‘high’ degree of self-stigma. None of the patients had scores higher than 42 (i.e. ‘very high’ stigma).
Self-stigma was not related to delays in treatment seeking
Self-stigma scores were not significantly related to the amount of time between when the patient’s opioid use disorder onset and when they sought addiction treatment. In addition to not meeting the threshold for statistical significance, the correlation was very small and unlikely to have real world significance as well.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
TIn this study, individuals with a current or past history of opioid agonist medication treatment (i.e. buprenorphine or methadone) in France experienced high rates of self-stigma mostly in the moderate range or below, as well as perceived stigma from healthcare workers, due to their opioid use disorder and medication treatment. Despite this, this self-stigma did not appear to delay treatment-seeking. Given the low response rate of eligible patients (only 32% agreed to participate), that some individuals were reporting on their experience from several years earlier, and differences between the French and U.S. health care systems, it is unclear how representative these findings may be of patients currently treated in France, or how findings may generalize to the United States.
Despite some substantial limitations of this study, findings are, nevertheless somewhat consistent with studies of stigma conducted in other countries and healthcare settings, showing associations between self-stigma and perceived stigma among individuals receiving medication treatment. In addition to healthcare providers being perceived as stigmatizing by individuals receiving medication treatment, prior studies have demonstrated these stigmatizing beliefs among healthcare workers, suggesting that this stigma may not merely be a misperception of patients but potentially actual experiences of enacted stigma. Indeed, about 1/3 of patients in this study reported that they were refused care by a healthcare professional due to their opioid use disorder and medication treatment. Even though France has one of the highest rates of opioid use disorder medication treatment receipt, stigma toward these medication treatments still exists; exposure to and knowledge about medication treatment and patients receiving it may therefore not be enough to combat the stigmatizing beliefs and discriminatory behaviors that have been deeply ingrained in society over the past several decades. This stigma is so prevalent, socioculturally, that individuals who receive medication treatment can internalize these beliefs and may see themselves in ways that reflect these stigmatizing attitudes, which can hinder treatment and recovery progress.
As noted above, one important caveat is that only 32% of eligible patients completed the survey. As such, the findings here may not be representative of all opioid agonist patients in France – it is possible for example, that individuals with especially negative experiences may have taken the opportunity to express those experiences. Financial incentives for participation can protect against these types of selection biases, though the study did not report whether or not financial incentives were offered. That said, given that stigma can reduce providers’ willingness to prescribe and patients’ willingness to receive these medication treatments, novel public health campaigns and efforts within and outside of healthcare institutions are needed to combat stigma toward opioid use disorder and its treatment. The long period over which participants may have been taking the agonist medication – since 2012 – also presents some opportunities to see whether there may be changes in self-stigma over time that could have been related to different types of system changes during that period but such analyses were not reported and, again, the small sample size also would not lend itself well to those kinds of analyses.
However, the literature is still mixed, suggesting that the impact that stigma has on healthcare behaviors and treatment seeking can vary widely. This means other factors can often influence stigma’s effect on actual treatment seeking behaviors. Though this study found no correlation between self-stigma and delayed treatment seeking with respect to a patient’s first opioid use disorder treatment episode, about 25% of medication-treated patients reported that they delayed seeking healthcare more broadly, due to fear that they would be stigmatized because of their current/past use of medication treatment. Thus, for at least a subset of individuals with a history of medication treatment self-stigma may negatively influence healthcare utilization.
Finally, it is worth reiterating that this study was conducted in France where opioid agonist medications are very common. In the US, rates of opioid agonist medication use are much lower. How policy changes that may help mainstream these medications in US healthcare – like ending the requirement for 8 hours of specialized training (i.e., the Drug Enforcement Administration, or DEA, “X waiver”) – will impact prescription rates and patients’ perceived stigma are not yet clear. Overall, this study’s findings warrant additional efforts to better understand recent experiences of stigma and their effects on health-related behaviors and use of healthcare resources across the globe.
Data were collected from a single hospital in France and the study population did not differentiate between patients with current or past opioid use disorder. Stigma may differ in other medical facilities, countries, and at different stages and severity of opioid use disorder.
Only 32% of eligible patients decided to participate in this study. Thus, how representative this select sample may be of patients treated at that hospital (or any other) is unclear and could be biased in some way.
This study was based on self-reported data and information about disorder diagnoses and treatment episodes are therefore subject to self-report bias. Perceived- and self-stigma questions did not ask about stigmatizing beliefs/experiences within a given time frame and rates of stigma may therefore reflect past experiences combined with more recent experiences, demanding additional research.
BOTTOM LINE
About half of the French adults in this study experienced perceived stigma from healthcare professionals due to their opioid use disorder and medication treatment. Self-stigma was also common, with 85% reporting low-moderate degrees of self-stigma and 62% reporting moderate to high degrees of self-stigma around their identity as a person who has received opioid use disorder medication treatment. No one, however, reported very-high self-stigma. Though self-stigma was not significantly related to delays in seeking a first treatment episode for opioid use disorder, about 1/4 of patients reported delaying healthcare seeking more broadly, due to fear that they would be stigmatized because of their medication treatment. Thus, this study also suggests that a subset of people may be delaying general healthcare seeking due to self-stigma, warranting additional research to identify novel methods that help reduce self-stigma in medication treated patients, and that address discrimination and stigmatizing attitudes among the healthcare workforce.
For individuals and families seeking recovery: Amid ongoing efforts to combat stigma and discrimination toward opioid use disorder and its treatment, individuals and families seeking medication treatment are encouraged to find a healthcare team that has experience treating individuals with medication treatment and that uses this experience to provide patient-centered empathetic care. Individuals who feel stigmatized by their healthcare providers are encouraged to find another doctor who better understands medication treatment and that they feel comfortable discussing their opioid use disorder and treatment history with, sans judgement. Individuals experiencing self-stigma might consider joining a support group of peers with lived experience of medication treatment (such as Medication Assisted Recovery Anonymous, or MARA) and/or seeking individual therapy to help address shame and stigma and to develop better self-talk and adaptive behaviors that improve self-image.
For treatment professionals and treatment systems: It is essential for treatment professionals and systems to obtain ongoing training about medication treatment for opioid use disorder to ensure stigmatizing attitudes toward opioid use disorder and its treatment, driven by misconceptions and past personal experiences, do not perpetuate stigma towards individuals who are seeking and receiving treatment for opioid use disorder. These stigmatizing beliefs can lead patients to see themselves in negative ways, and some may even avoid seeking essential healthcare due to fear of being stigmatized by healthcare providers and systems. Challenging stigmatizing beliefs through professional education and exposure, and enacting policy and regulatory changes in healthcare systems around medication treatment may help reduce stigma within healthcare systems, as well as the harm it can cause to the patients these systems treatment.
For scientists: Naturalistic longitudinal investigations are needed to determine the extent to which self-stigma and perceived stigma influence uptake of opioid use disorder medication treatments, and how use of these treatments in turn affect self-stigma and perceived stigma from healthcare professionals and the general public. Studies are needed to determine the factors that moderate – i.e., protect against – the influence of stigma on treatment seeking and healthcare decision making at a micro-, meso-, and macro-level. Examining the relationship between stigma and additional health-related behaviors is warranted to better understand the impact of stigma on treatment seeking, uptake, and retention, as well as patient well-being.
For policy makers: Studies like this help us better understand how beliefs and attitudes toward medication treatment for opioid use disorder affect individuals who receive it, including their beliefs about themselves and their health behaviors. By characterizing patient experiences of stigma and their relationship to treatment and other healthcare seeking behaviors, we can better address the opioid epidemic through an understanding of stigma as a barrier to medication treatment receipt and prescribing, as well as it’s secondary downstream effects on patient healthcare utilization and treatment/recovery outcomes. Healthcare-provider exposure to and knowledge about medication treatment and opioid use disorder may not be enough to combat the deeply ingrained, stigmatizing beliefs held by society and many healthcare professionals. Ongoing funding for research on the ways that medication treatment laws and healthcare regulations impact stigma are essential to inform policy reform that can help combat stigma and discrimination to ultimately better address the opioid epidemic.
Medication treatments like buprenorphine and methadone (i.e. opioid agonist treatments) are helpful gold-standard treatments for opioid use disorder that ultimately help to support positive recovery outcomes. In France, nearly 90% of individuals with opioid use disorder that get treatment receive an opioid agonist medication, significantly more common than in the United States (~20%).
Though 3/4 of French patients receive opioid agonist treatment from non-specialty providers (e.g., primary care), these patients are treated by a group constituting only 1/4 of all physicians that have the ability to prescribe opioid agonist treatments – of the physicians eligible to prescribe these medications, 75% choose not to do so. Primary care providers offering initial prescriptions of buprenorphine for opioid use disorder in France declined 44% between 2009 and 2015, and have remained stagnant since 2011, whereas methadone initiations have increased. Similar issues have been observed in the United States, with only about 8% of primary care physicians having prescribed buprenorphine. With rates of opioid use disorder continuing to increase in Europe, the declining involvement of primary care physicians in opioid use disorder medication treatment could reduce buprenorphine availability and threaten the success that France has had with medication treatment uptake.
To address these issues, studies have begun to evaluate the barriers to prescribing medication treatment in primary care, with provider attitudes toward opioid use disorder and its treatment being noted as one potential barrier. Treatment providers’ misconceptions about medication treatment can lead to discriminatory attitudes toward individuals with opioid use disorder. These misconceptions contribute to the negative stereotypes that people hold about individuals with opioid use disorder, perpetuating social stigma and discrimination. This social stigma can lead to discriminatory acts toward individuals with opioid use disorder, contributing to housing, employment, and legal challenges amongst those who are stigmatized. It can also cause individuals with opioid use disorder to believe that others have negative attitudes about them due to their disorder (i.e. perceived stigma). Individuals with opioid use disorder might also internalize the negative attitudes held by the public, impacting identity, self-esteem, and self-worth (i.e. self-stigma). Self-stigma can thereby hinder treatment and recovery, reducing patient hope, empowerment, and treatment initiation/adherence, while increasing risk for other psychiatric symptoms (e.g., depression, anxiety, etc.). Public and perceived stigma towards individuals receiving opioid use disorder medication treatment often persist beyond cessation of illicit opioid use, and exist across multiple life domains (e.g., medical, social, family, professional). This stigma can also reduce providers’ willingness to prescribe medication treatments for opioid use disorder.
Given the impact of stigma on treatment and recovery, increased efforts are needed to better understand experiences of stigma among patients with opioid use disorder. To address this gap, this study assessed perceived-stigma, self-stigma and its relationship to treatment seeking among individuals receiving opioid use disorder medication treatment in France, a country with particularly high rates of medication treatment.
HOW WAS THIS STUDY CONDUCTED?
This was an observational cross-sectional study of perceived- and self-stigma, conducted 2022-2023 among 73 adults who received outpatient medication treatment (i.e. buprenorphine or methadone) from an addiction medicine department at a single hospital in France any time since 2012 (i.e., recruited individuals were both current and past patients). In France, buprenorphine treatment is accessible in a primary care setting, whereas methadone treatment is available via specialized centers. Unlike treatment in the United States, patients receiving methadone from specialized treatment facilities in France have the ability to continue methadone in primary care settings after they reach a stable dose, with methadone prescribed and dispensed at community pharmacies.
The authors evaluated the prevalence of perceived stigma and self-stigma, as well as the relationship between self-stigma and delays in treatment seeking. Patients who had previously received or were currently receiving opioid agonist treatment (i.e. methadone or buprenorphine) for a past or current opioid use disorder at the hospital’s addiction medicine department were invited to participate. Those who enrolled in the study (32% of eligible patients) completed self-report questionnaires concerning demographics, clinical characteristics, perceived stigma, and self-stigma.
Perceived stigma was defined as the belief that others hold negative attitudes or have behaved in discriminatory ways toward them due to their opioid use disorder or status as a patient taking buprenorphine/methadone, and was assessed with a 6-item questionnaire with yes/no responses that was designed for this study. Questionnaire items addressed the quality of the patient’s relationship with their primary care provider, experiences of stigma around opioid use disorder and medication treatment from a medical professional, and avoidance of care seeking due to fear of stigma.
Self-stigma was defined as having stigmatizing attitudes towards oneself, due to the internalization of negative societal attitudes and stereotypes, and was measured with the Self-Stigma Scale-Short inventory, modified to address stigma related to patients receiving opioid agonist treatment. Participants rated their level of agreement with 9 statements about self-stigma. See the figure below for examples of self-stigma items. The total scale score ranged from 9 (low stigma) to 45 (high stigma), and was categorized into 1 of 5 self-stigma severity categories: (1) 9 – 15 points = very low stigma; (2) 16 – 22 = low stigma; (3) 23 – 33 = moderate stigma; (4) 34 – 42 = high stigma; (5) 43 – 45 = very high stigma.
Delays in care seeking were assessed as the time between a patient’s opioid use disorder onset and the start of their first treatment episode. Though participants needed to be current or past patients at a particular university-affiliated addiction treatment program with any history of taking methadone/buprenorphine, the study does not specify whether the treatment onset examined here in relation to self-stigma is receipt of methadone/buprenorphine (or any treatment), or whether the treatment needed to be in their addiction treatment program (or any program). Importantly, it is also unclear how the delay in treatment seeking – from opioid use disorder onset – would be determined if participants entered their system to begin receiving medication – e.g., patients may have provided information to help determine onset of opioid use disorder symptoms or self-reported this information, etc. but the details of how these values were determined is not clear from the study.
The researchers analyzed the percentage of patients who experienced perceived stigma due to their opioid use disorder and medication treatment. The authors then examined mean self-stigma scores, as well as the percentage of patients whose scores fell within each of the 5 self-stigma severity categories. Thereafter, the relationship between self-stigma scores (low vs. high) and patient factors was assessed.
The majority of participants were unemployed (62%) men (73%) in their early forties. Eighty eight percent of participants were currently receiving opioid agonist treatment (63% methadone, 25% buprenorphine), whereas 12% had received opioid agonist treatment in the past but were no longer taking it at the time of the survey. Thirty-two percent of participants had misused opioids in the past 60 days.
WHAT DID THIS STUDY FIND?
Half reported experiencing stigma from healthcare professionals
Nearly 50% of patients perceived stigmatizing attitudes from healthcare professionals and about 1/3 were denied care by a healthcare provider due to their opioid use disorder and/or their medication treatment. In addition, about 25% of patients reported that they delayed seeking healthcare due to fear that they would be stigmatized because of their medication treatment. Despite this, 85% of participants reported having a good to moderate quality relationship with their primary care provider.
On average, patients reported a moderate degree of self-stigma
The average self-stigma scale score among patients was 24.7 out of 45 points, reflective of a moderate degree of self-stigma around one’s current/past medication treatment. When self-stigma scores were categorized, 38% of patients had a ‘very low’ or ‘low’ degree of self-stigma, 51% had a ‘moderate’ degree of self-stigma, and 11% had a ‘high’ degree of self-stigma. None of the patients had scores higher than 42 (i.e. ‘very high’ stigma).
Self-stigma was not related to delays in treatment seeking
Self-stigma scores were not significantly related to the amount of time between when the patient’s opioid use disorder onset and when they sought addiction treatment. In addition to not meeting the threshold for statistical significance, the correlation was very small and unlikely to have real world significance as well.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
TIn this study, individuals with a current or past history of opioid agonist medication treatment (i.e. buprenorphine or methadone) in France experienced high rates of self-stigma mostly in the moderate range or below, as well as perceived stigma from healthcare workers, due to their opioid use disorder and medication treatment. Despite this, this self-stigma did not appear to delay treatment-seeking. Given the low response rate of eligible patients (only 32% agreed to participate), that some individuals were reporting on their experience from several years earlier, and differences between the French and U.S. health care systems, it is unclear how representative these findings may be of patients currently treated in France, or how findings may generalize to the United States.
Despite some substantial limitations of this study, findings are, nevertheless somewhat consistent with studies of stigma conducted in other countries and healthcare settings, showing associations between self-stigma and perceived stigma among individuals receiving medication treatment. In addition to healthcare providers being perceived as stigmatizing by individuals receiving medication treatment, prior studies have demonstrated these stigmatizing beliefs among healthcare workers, suggesting that this stigma may not merely be a misperception of patients but potentially actual experiences of enacted stigma. Indeed, about 1/3 of patients in this study reported that they were refused care by a healthcare professional due to their opioid use disorder and medication treatment. Even though France has one of the highest rates of opioid use disorder medication treatment receipt, stigma toward these medication treatments still exists; exposure to and knowledge about medication treatment and patients receiving it may therefore not be enough to combat the stigmatizing beliefs and discriminatory behaviors that have been deeply ingrained in society over the past several decades. This stigma is so prevalent, socioculturally, that individuals who receive medication treatment can internalize these beliefs and may see themselves in ways that reflect these stigmatizing attitudes, which can hinder treatment and recovery progress.
As noted above, one important caveat is that only 32% of eligible patients completed the survey. As such, the findings here may not be representative of all opioid agonist patients in France – it is possible for example, that individuals with especially negative experiences may have taken the opportunity to express those experiences. Financial incentives for participation can protect against these types of selection biases, though the study did not report whether or not financial incentives were offered. That said, given that stigma can reduce providers’ willingness to prescribe and patients’ willingness to receive these medication treatments, novel public health campaigns and efforts within and outside of healthcare institutions are needed to combat stigma toward opioid use disorder and its treatment. The long period over which participants may have been taking the agonist medication – since 2012 – also presents some opportunities to see whether there may be changes in self-stigma over time that could have been related to different types of system changes during that period but such analyses were not reported and, again, the small sample size also would not lend itself well to those kinds of analyses.
However, the literature is still mixed, suggesting that the impact that stigma has on healthcare behaviors and treatment seeking can vary widely. This means other factors can often influence stigma’s effect on actual treatment seeking behaviors. Though this study found no correlation between self-stigma and delayed treatment seeking with respect to a patient’s first opioid use disorder treatment episode, about 25% of medication-treated patients reported that they delayed seeking healthcare more broadly, due to fear that they would be stigmatized because of their current/past use of medication treatment. Thus, for at least a subset of individuals with a history of medication treatment self-stigma may negatively influence healthcare utilization.
Finally, it is worth reiterating that this study was conducted in France where opioid agonist medications are very common. In the US, rates of opioid agonist medication use are much lower. How policy changes that may help mainstream these medications in US healthcare – like ending the requirement for 8 hours of specialized training (i.e., the Drug Enforcement Administration, or DEA, “X waiver”) – will impact prescription rates and patients’ perceived stigma are not yet clear. Overall, this study’s findings warrant additional efforts to better understand recent experiences of stigma and their effects on health-related behaviors and use of healthcare resources across the globe.
Data were collected from a single hospital in France and the study population did not differentiate between patients with current or past opioid use disorder. Stigma may differ in other medical facilities, countries, and at different stages and severity of opioid use disorder.
Only 32% of eligible patients decided to participate in this study. Thus, how representative this select sample may be of patients treated at that hospital (or any other) is unclear and could be biased in some way.
This study was based on self-reported data and information about disorder diagnoses and treatment episodes are therefore subject to self-report bias. Perceived- and self-stigma questions did not ask about stigmatizing beliefs/experiences within a given time frame and rates of stigma may therefore reflect past experiences combined with more recent experiences, demanding additional research.
BOTTOM LINE
About half of the French adults in this study experienced perceived stigma from healthcare professionals due to their opioid use disorder and medication treatment. Self-stigma was also common, with 85% reporting low-moderate degrees of self-stigma and 62% reporting moderate to high degrees of self-stigma around their identity as a person who has received opioid use disorder medication treatment. No one, however, reported very-high self-stigma. Though self-stigma was not significantly related to delays in seeking a first treatment episode for opioid use disorder, about 1/4 of patients reported delaying healthcare seeking more broadly, due to fear that they would be stigmatized because of their medication treatment. Thus, this study also suggests that a subset of people may be delaying general healthcare seeking due to self-stigma, warranting additional research to identify novel methods that help reduce self-stigma in medication treated patients, and that address discrimination and stigmatizing attitudes among the healthcare workforce.
For individuals and families seeking recovery: Amid ongoing efforts to combat stigma and discrimination toward opioid use disorder and its treatment, individuals and families seeking medication treatment are encouraged to find a healthcare team that has experience treating individuals with medication treatment and that uses this experience to provide patient-centered empathetic care. Individuals who feel stigmatized by their healthcare providers are encouraged to find another doctor who better understands medication treatment and that they feel comfortable discussing their opioid use disorder and treatment history with, sans judgement. Individuals experiencing self-stigma might consider joining a support group of peers with lived experience of medication treatment (such as Medication Assisted Recovery Anonymous, or MARA) and/or seeking individual therapy to help address shame and stigma and to develop better self-talk and adaptive behaviors that improve self-image.
For treatment professionals and treatment systems: It is essential for treatment professionals and systems to obtain ongoing training about medication treatment for opioid use disorder to ensure stigmatizing attitudes toward opioid use disorder and its treatment, driven by misconceptions and past personal experiences, do not perpetuate stigma towards individuals who are seeking and receiving treatment for opioid use disorder. These stigmatizing beliefs can lead patients to see themselves in negative ways, and some may even avoid seeking essential healthcare due to fear of being stigmatized by healthcare providers and systems. Challenging stigmatizing beliefs through professional education and exposure, and enacting policy and regulatory changes in healthcare systems around medication treatment may help reduce stigma within healthcare systems, as well as the harm it can cause to the patients these systems treatment.
For scientists: Naturalistic longitudinal investigations are needed to determine the extent to which self-stigma and perceived stigma influence uptake of opioid use disorder medication treatments, and how use of these treatments in turn affect self-stigma and perceived stigma from healthcare professionals and the general public. Studies are needed to determine the factors that moderate – i.e., protect against – the influence of stigma on treatment seeking and healthcare decision making at a micro-, meso-, and macro-level. Examining the relationship between stigma and additional health-related behaviors is warranted to better understand the impact of stigma on treatment seeking, uptake, and retention, as well as patient well-being.
For policy makers: Studies like this help us better understand how beliefs and attitudes toward medication treatment for opioid use disorder affect individuals who receive it, including their beliefs about themselves and their health behaviors. By characterizing patient experiences of stigma and their relationship to treatment and other healthcare seeking behaviors, we can better address the opioid epidemic through an understanding of stigma as a barrier to medication treatment receipt and prescribing, as well as it’s secondary downstream effects on patient healthcare utilization and treatment/recovery outcomes. Healthcare-provider exposure to and knowledge about medication treatment and opioid use disorder may not be enough to combat the deeply ingrained, stigmatizing beliefs held by society and many healthcare professionals. Ongoing funding for research on the ways that medication treatment laws and healthcare regulations impact stigma are essential to inform policy reform that can help combat stigma and discrimination to ultimately better address the opioid epidemic.