
Do Reasons For NOT Seeking Treatment Depend on the Severity of the Alcohol Use Disorder?
Among individuals with an alcohol use disorder, treatment rates remain relatively low.
This study of six countries in the European Union investigated why primary care patients with an alcohol use disorder choose not to seek treatment and if their reasons vary according to level of severity.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Alcohol use disorder is among the most prevalent mental disorders in United States and other countries. For example, there were 23 million people who met criteria for an alcohol use disorder in 2010 in the European Union. Despite the high prevalence of alcohol use disorder, treatment rates have been the lowest of all major mental disorders averaging about 10% in Europe during the past decade; a figure similar to the US.
Yet, despite the fact that most individuals who meet criteria for alcohol use disorder do not seek specialty care for it, these individuals often do access primary care settings making it an ideal place to screen and intervene on this debilitating disorder. Increasing the treatment rates requires greater understanding of the reasons why patients do not seek treatment and whether these reasons vary according to severity of the illness.
Consequently, this study examined self-reported reasons for not seeking treatment and their association with alcohol use disorder severity among primary health care patients diagnosed with an alcohol use disorder.
HOW WAS THIS STUDY CONDUCTED?
As part of the Alcohol Dependence in Primary Care Study, alcohol use disorders and reasons for not seeking treatment were assessed using interviews on regionally representative samples of primary care patients from 6 European countries (Italy, Germany, Hungary, Latvia, Poland and Spain). General practitioners and study personnel completed questionnaires assessing their patients’ alcohol use. Study refusal rate was 56.4%.
Although the authors started with sample of 9,098 primary care patients (3,715 males and 5,383 females), 1,008 were diagnosed with a current alcohol use disorder (past 12 months) and an additional 1,774 had a past alcohol use disorder at some point in their life (excluding the past 12 months). The majority of patients did not receive treatment who had a current (810) or lifetime diagnosis (1,372). Of the patients with a current diagnosis, 251 (25%) provided a reason for not receiving treatment compared to 664 (37%) patients with a lifetime diagnosis.
A theoretical framework proposed by Saunders was used to test the theory that reasons for not seeking treatment are related to alcohol use disorder severity. The theory states that at low levels of alcohol use disorder severity ‘a lack of problem awareness/denial’ is the primary reason; however, as severity increases, denial becomes challenged and individuals are more likely to consider treatment and encounter barriers in the process.
WHAT DID THIS STUDY FIND?
Across All Levels of Alcohol Use Disorder Severity:
-
The most frequent reason for not seeking treatment was ‘lack of problem awareness’ given by 55.3% of patients with a current alcohol use disorder who responded (compared to 78.3% of lifetime)
-
The second most common response was ‘stigma or shame’ given by 28.6 % (compared to 2.4% of lifetime),
-
The third most common response was ‘encounter barriers’ provided by 22.8 % (compared to 4.6% of lifetime). Notably, the most frequently endorsed ‘barrier’ reported by patients with a current alcohol use disorder was a wish to not stop drinking at 72.9% (compared to 10% lifetime).
-
Fourth, a preference to ‘cope alone’ provided by 20.9% (compared to 17.2% of lifetime).
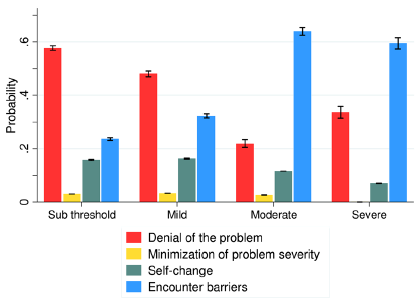
Further analysis was conducted to investigate the association between reasons for not seeking treatment and alcohol use disorder severity. The results indicated lower probabilities of reporting ‘lack of awareness/denial of problem’ and higher probabilities to report ‘encounter barriers’ as alcohol use disorders severity increases.
WHY IS THIS STUDY IMPORTANT?
Overall, among primary care patients with a diagnosable alcohol use disorder, this study found that the most frequently reported reason for not seeking treatment was ‘lack of problem awareness/denial’. This was especially true at low levels of alcohol use disorder severity.
This shows that many patients are unable to recognize and acknowledge problems related to their alcohol use when severity is low. Continuous monitoring of patients’ alcohol use in primary care settings could be useful not only for the prevention of health and social consequences, but the prevention of alcohol use disorders.
Alcohol use disorder is a major contributor to premature death, disease, and disability in Europe, the US, and in nearly all high-income countries.
As alcohol use disorder severity increases, individuals are more likely to consider and seek alcohol use disorder treatment and to encounter actual barriers associated with the treatment seeking process. The desire not to stop drinking completely was the barrier reported most frequently among patients with a current alcohol use disorder.
Local communities and national policies can create natural reinforcers in various community entities as a way of incentivizing longer-term recoveries.
Treatment providers should link clients to natural reinforcers that will make long-term abstinence more appealing.
Treatment approaches that focus on helping patients to initially try reductions in drinking, instead of complete abstinence, may help attract and engage more of these individuals into treatment and help reduce harm whether or not these same individuals choose to abstain at a later time.
Many treatment programs in Europe these days often incorporate client-centered and harm reduction approaches to alcohol and other drug problems, so the perceived barrier of treatment being abstinence-only may be outdated.
- LIMITATIONS
-
- The study had a very high refusal rate. Thus, the generalizability of the study findings are unknown.
NEXT STEPS
Methods by which general practitioners can provide routine assessment of patients alcohol use deserve further exploration. For example, the screening and monitoring of patients’ blood pressure could serve as a model for routine alcohol use assessment in primary care.
Furthermore, blood pressure monitoring itself may offer a destigmatized approach to screening for alcohol use disorder since it is correlated with alcohol use and is standard in yearly checkups.
BOTTOM LINE
- For individuals & families seeking recovery: This study showed that most primary care patients with an alcohol use disorder do not seek treatment. The reasons vary according to the severity of the alcohol use disorder. At lower levels of severity (i.e., subthreshold or mild) it is difficult for people to acknowledge or agree that they have a problem with alcohol. At higher levels of severity (i.e., moderate or severe) some people with alcohol use disorder appear to seek specialty treatment but may encounter other obstacles such as a mismatch between their own desire to not quit drinking completely and a perceived abstinence-orientation of the treatment program. Many programs, however, typically use client-centered/motivational interviewing techniques to engage patients in care and agree to treatment goals with the patient, so complete abstinence from alcohol may not be as big of a barrier as previously perceived.
- For Scientists: The overall message is that reasons for not seeking treatment may vary depending on the severity of alcohol use disorder. Given that 56% of general practitioners refused to participate in the study, and some practitioners reported they did not want to share sensitive patient data such as alcohol use, however, means that findings here should be viewed cautiously regarding their generalizability.
- For Policy makers: This study suggests many individuals who have had a past or current alcohol use disorder still check-in with a general practitioner, even if they do not seek treatment for their alcohol use disorder. Previous research has shown that brief interventions delivered in primary care setting can be highly useful in prevention of progression into more severe stages of alcohol use disorders, alcohol related mortality, and societal harms. Prioritization of research and policies designed to bridge the gap between patients with alcohol use disorder and interventions in primary care may help to raise early detection and prevent health and social consequences of alcohol use disorder.
- For Treatment professionals and treatment systems: Among primary care patients with the most severe alcohol use disorder, the wish not to stop drinking completely was the most frequent treatment barrier reported in this study. For some of these individuals, using a client-centered/motivational interviewing approach and ensuring prospective patients understand that this approach exists may be a helpful way to engage them in care.
CITATIONS
Probst, C. Manthey, J., Martinez, A., & Rehm, J. (2015). Alcohol use disorder severity and reported reasons not to seek treatment: A cross-sectional study in European primary care practices. Substance Abuse Treatment, Prevention, and Policy, 10:32. DOI 10.1186/s13011-015-0028-z
