Racially segregated counties are more likely to have a syringe service program, but have more difficulty disseminating resources
Research examining access to resources in areas with more racial segregation – where individuals of similar races are more clustered than expected – can highlight inequities for minority groups. This study examined whether racial segregation is associated with syringe service program operation and distribution of syringes and naloxone doses.
The United States is currently experiencing not only an opioid overdose epidemic, but also epidemics of Hepatitis C and infections of the skin, soft tissues, and heart, as well as HIV outbreaks. These multiple epidemics disproportionately impact racial minorities, with the highest increases of overdose deaths being observed among people who are American Indian, Alaskan Native, and Black. HIV diagnoses are also higher among Black and Hispanic people than would be expected given their share of the general population.
Harm reduction strategies, such as syringe service programs and broad access to naloxone, can help prevent overdoses and infectious diseases. However, racial minorities often have unequal access to such services. Further, even in areas where there may be equal or higher access, the full impact of services may not be realized. For example, in one recent study, municipalities in Massachusetts with greater proportions of Black people had higher rates of naloxone coverage, but this increased naloxone presence did not decrease overdose deaths during the pandemic in this group.
These inequities can be explained, in part, by structural racism. For example, practices such as redlining for home mortgages and exclusionary real estate practices have created racial residential segregation and economic inequality. In these “racialized environments”, residents have fewer opportunities to advance economically and experience more social and health disadvantages. This study examined whether there is differential access to syringe service programs and harm reduction supplies because of racial segregation. This research can help address health inequities that disproportionately impact racial minorities.
HOW WAS THIS STUDY CONDUCTED?
The research team explored the associations of racial segregation with syringe service program operation and distribution of syringes and naloxone doses by collecting information from program directors about their program operations in 2021. Covariates that were controlled for included, urbanicity, political orientation, and 2019 overdose mortality. Information was collected as part of the National Survey of Syringe Service Programs. For this survey, the research team recruited syringe service programs in the US from a variety of sources, including various networks, social media, and conferences, from February to June 2021. Program directors were emailed up to 3 times asking for their participation in the online survey and then non-responders were called. The survey asked participants what county their program operated in during 2020 and how many syringes and naloxone doses were distributed by their program. Out of 412 programs that were contacted, 295 program directors participated. Participants were compensated for $75 for their time completing the survey.
The primary outcomes of interest were 3 county-level measures that were constructed using geocoding. The first measure was whether or not a syringe service program operated in the county (yes/no). The second measure was county-level per capita syringe distribution, which was calculated by dividing the total number of syringes distributed across programs, as reported by program directors in the survey, by the population size of the county. The third measure was county-level per capita naloxone distribution, which was similarly calculated by dividing the total number of naloxone doses distributed across programs, as reported by program directors in the survey, by the population size of the county.
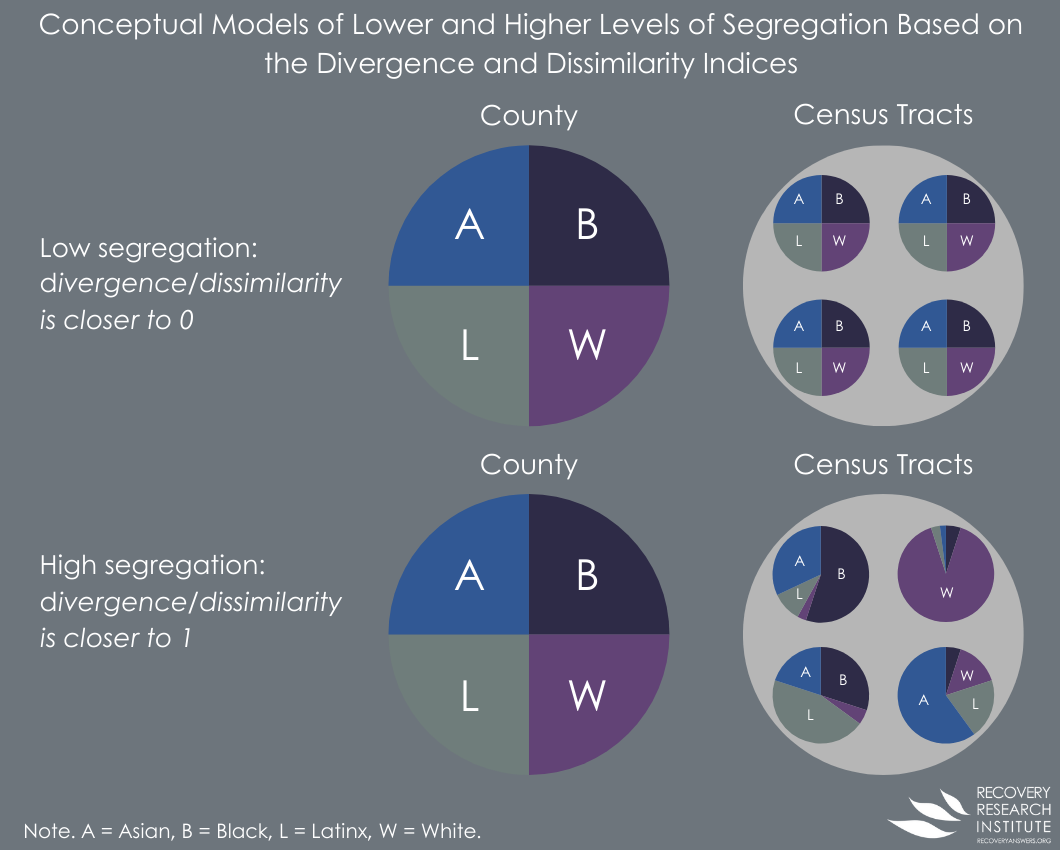
The primary predictor was racial residential segregation, measured in this study by 2 commonly used indexes of segregation, the Divergence and Dissimilarity Indexes. These indices measure how divergent and dissimilar a given area is in comparison to the entire county and range from 0 to 1, where higher values indicate higher levels of segregation. In brief, the Divergence index measures the degree to which race breakdowns in census tracts within counties match the overall county race breakdown. The Dissimilarity Index measures the percent of individuals from the minority group that would need to move relative to White individuals such that census tracts were equally distributed by race. See below for a conceptual figure explaining how these measures of segregation are calculated.
The research team was also interested in racial and ethnic composition in a county and the following covariates: urbanicity, political orientation, and 2019 overdose mortality. Data for racial and ethnic composition was obtained from the American Community Survey, conducted by the US Census Bureau, for the 5-year period between 2016 and 2020. Urbanicity was determined by the NCHS Urban-Rural Classification Scheme. Political orientation was assessed by calculating the percent of votes within the county for the Republican presidential candidate in 2020, as this may serve as a proxy for opposition to harm reduction methods. Overdose mortality was calculated for the year 2019 per 100,000 people in a county. All deaths involving opioids in 2019 were included.
A total of 3106 counties in the contiguous US were analyzed – each “case” was a county, agnostic to its overall population – i.e., there was no weighting by the number of people living in a given county such that more populous and less populous counties were both counted as 1 county. Analyses were first conducted to examine whether the Divergence and Dissimilarity indices are predictive of the presence or absence of a syringe service program operating in the county. Separate analyses were then conducted to examine whether the Divergence and Dissimilarity indices are predictive of the rates of syringe and naloxone distribution per 100,000 people in a county. Covariates were also included in all models. The proportion of non-Hispanic Black, non-Hispanic Asian, non-Hispanic Other, and Hispanic people within a county were further compared to the proportion of non-Hispanic White people. Finally, analyses were conducted to examine whether missingness biased the results.
Syringe service programs were reported to be operating in 9% of counties. On average, there were 10,099 syringes and 112 naloxone doses distributed per 100,000 people. Levels of segregation varied from no segregation to almost total segregation. In an average county (irrespective of population size), the percent of votes for the Republican presidential candidate was 56% and the mean opioid overdose mortality rate was 13.07 per 100,000 people. Counties had a mean percentage of 76% non-Hispanic White people, 9% non-Hispanic Black people, 1.3% non-Hispanic Asian people, 4% people identifying as non-Hispanic Other, and 9.6% Hispanic people. For urbanicity, counties were 63% rural, 35% suburban, and 2% urban.
WHAT DID THIS STUDY FIND?
Counties with higher levels of racial segregation had more syringe service programs
Higher levels of racial segregation were associated with greater chances of a syringe service program operating in the county. As the Divergence Index increased, the chances of a program operating in the county increased by 33%. As the Black-White and Hispanic-White Dissimilarity Indices increased, the chances of a program operating in the county increased by 66% and 78%, respectively. However, no differences were found when comparing the chances of a program operating in counties with greater raw proportions of Black, Asian, and Hispanic people to counties with greater proportions of non-Hispanic White people. Missing data was not found to bias these results.
Counties with higher levels of racial segregation distributed fewer syringes and naloxone doses
Higher levels of racial segregation were associated with lower rates of syringe distribution per capita (e.g., controlling for the number of people). As the Divergence Index increased, the rate of syringe distribution decreased by 33%. As the Hispanic-White Dissimilarity Index increased, the rate of syringe distribution decreased by 35%. Additionally, counties with higher proportions of Black individuals distributed 31% fewer syringes than counties with higher proportions of non-Hispanic White individuals. Missing data was not found to bias these results.
Higher levels of racial segregation were not associated with rates of naloxone distribution, as measured by the Divergence and Dissimilarity Indices, but there were differences in the racial compositions of the counties. Counties with higher proportions of people who identified as Other race and Hispanic distributed 40% and 3% fewer naloxone doses, respectively, than counties with higher proportions of non-Hispanic White people. Missing data was not found to bias these results.
County characteristics were associated with chances of syringe service program operation and syringe and naloxone distribution
Urbanicity was associated with greater likelihood of a syringe service program operating in the county and lower rates of syringe and naloxone distribution. Urban counties had an almost 17-fold greater chance of a syringe service program operating than rural counties, and suburban counties were almost twice as likely as rural counties. However, urban and suburban counties distributed 3% and 10% fewer syringes and 1% and 5% fewer naloxone doses per capita than rural counties, respectively.
Republican political orientation was associated with a decreased chance of a syringe service program operating in the county but was not associated with rates of syringe and naloxone distribution. Counties with a higher proportion of Republican votes in the 2020 presidential election were 49% less likely to have a syringe service program operating.
Opioid overdose mortality rates were also associated with the chances of a syringe service program operating in the county but were not associated with rates of syringe and naloxone distribution. Counties with higher overdose mortality rates were 60% more likely to have a syringe service program operating.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team examined the associations of racial residential segregation with syringe service program operation and distribution of syringes and naloxone doses in counties across the United States. Results showed that counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses per capita. Likewise, urban and suburban counties were more likely to have a program in operation than rural counties but distributed fewer syringes and naloxone doses per capita. Finally, the percentage of Republican votes in a county was associated with a decreased chance of a syringe service program operating and opioid overdose mortality rates were associated with an increased chance, but neither were associated with rates of syringe and naloxone distributions.
These results suggest that racially segregated counties, and those with a greater need for harm reduction services, are aiming to meet the needs of the community by implementing a syringe service program. This is consistent with prior studies that have shown that higher levels of racial segregation are associated with higher levels of resilience and cultures of care for others, which may be explained by people in these communities feeling they are best positioned to rely on peers and community leaders, rather than federal and state governments, to meet their needs.
However, the finding that these racially segregated counties also distributed fewer syringes and naloxone doses suggests that these communities may lack the resources to be able to adequately staff their programs and scale harm reduction distribution efforts for successful implementation. These deficits in resources may be explained by long-standing structural inequities. Also of note, many of these programs operate in brick-and-mortar physical locations, limiting their capacity to scale. Then, when examining per capita distribution, syringe programs reach a smaller proportion of these more populous counties compared to programs in rural areas which may reach a larger proportion simply because they have fewer overall people to serve. Future studies can examine whether strategies to extend access beyond physical locations – e.g., mobile syringe distribution vans, etc. – can help to redress these difficulties with distribution. Overall, addressing these community level factors may help to improve the ability of syringe service programs to achieve greater levels of syringe and naloxone distribution, thereby helping to prevent overdoses and infectious diseases.
There may have been syringe service programs operating in the United States that were not included in the analyses. The impact this could have had on the results is unclear and may have depended on the area the programs were operating in.
Data on harm reduction services was collected by self-report, which is known to be subject to response biases, such as recall or social desirability. People may, for example, be more likely to report higher rates of syringe and naloxone distributions because they think it is a desirable outcome for the researchers. Of note, however, county level data were derived from US census and related rigorously collected, publicly available data.
Most of the counties in the US, and thus in the study, are not urban, which is where the racial segregation measures are more precise given larger populations.
BOTTOM LINE
Counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses. This suggests that racially segregated counties are aiming to meet the needs of the community by implementing a syringe service program but may lack the resources to be able to adequately scale harm reduction distribution efforts.
For individuals and families seeking recovery: This study found that counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses. The presence of a syringe service program reflects the resilience and culture of care for others that racially segregated communities display, while the low distribution rates may reflect a lack of resources for successful implementation. Accordingly, people in these communities may similarly rely on grassroots efforts for fundraising to improve the distribution rates of harm reduction supplies. Individuals may also advocate for local and federal policymakers to address structural inequities and provide greater investments in these communities.
For treatment professionals and treatment systems: This study showed that counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses. Low distribution rates may reflect a lack of resources for successful implementation due to structural barriers and disinvestment, but the presence of syringe service programs reflects the communities’ ability and willingness meet its needs as a grassroots level. Treatment professionals may help to boost these programs’ resources by holding fundraisers or advocating at the local and federal levels. Such efforts may improve the distribution rates of harm reduction supplies, thereby preventing overdoses and infectious disease.
For scientists: This study showed that counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses. Future studies might test whether strategies can help extend the reach of brick-and-mortar harm reduction programs – e.g., mobile vans to distribute syringes – to improve distribution.
For policy makers: This study demonstrated that counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses. These results reflect the desire and willingness of communities to implement a syringe service program, but also suggest that they may lack the necessary resources to scale such efforts across their respective counties. Such challenges to scaling harm reduction may be explained by structural inequities; thus, policies that help address these barriers and invest in disadvantaged communities may improve these programs’ ability to achieve greater rates of harm reduction supply distribution, which can lead to fewer overdoses and reduced rates of infectious disease.
The United States is currently experiencing not only an opioid overdose epidemic, but also epidemics of Hepatitis C and infections of the skin, soft tissues, and heart, as well as HIV outbreaks. These multiple epidemics disproportionately impact racial minorities, with the highest increases of overdose deaths being observed among people who are American Indian, Alaskan Native, and Black. HIV diagnoses are also higher among Black and Hispanic people than would be expected given their share of the general population.
Harm reduction strategies, such as syringe service programs and broad access to naloxone, can help prevent overdoses and infectious diseases. However, racial minorities often have unequal access to such services. Further, even in areas where there may be equal or higher access, the full impact of services may not be realized. For example, in one recent study, municipalities in Massachusetts with greater proportions of Black people had higher rates of naloxone coverage, but this increased naloxone presence did not decrease overdose deaths during the pandemic in this group.
These inequities can be explained, in part, by structural racism. For example, practices such as redlining for home mortgages and exclusionary real estate practices have created racial residential segregation and economic inequality. In these “racialized environments”, residents have fewer opportunities to advance economically and experience more social and health disadvantages. This study examined whether there is differential access to syringe service programs and harm reduction supplies because of racial segregation. This research can help address health inequities that disproportionately impact racial minorities.
HOW WAS THIS STUDY CONDUCTED?
The research team explored the associations of racial segregation with syringe service program operation and distribution of syringes and naloxone doses by collecting information from program directors about their program operations in 2021. Covariates that were controlled for included, urbanicity, political orientation, and 2019 overdose mortality. Information was collected as part of the National Survey of Syringe Service Programs. For this survey, the research team recruited syringe service programs in the US from a variety of sources, including various networks, social media, and conferences, from February to June 2021. Program directors were emailed up to 3 times asking for their participation in the online survey and then non-responders were called. The survey asked participants what county their program operated in during 2020 and how many syringes and naloxone doses were distributed by their program. Out of 412 programs that were contacted, 295 program directors participated. Participants were compensated for $75 for their time completing the survey.
The primary outcomes of interest were 3 county-level measures that were constructed using geocoding. The first measure was whether or not a syringe service program operated in the county (yes/no). The second measure was county-level per capita syringe distribution, which was calculated by dividing the total number of syringes distributed across programs, as reported by program directors in the survey, by the population size of the county. The third measure was county-level per capita naloxone distribution, which was similarly calculated by dividing the total number of naloxone doses distributed across programs, as reported by program directors in the survey, by the population size of the county.
The primary predictor was racial residential segregation, measured in this study by 2 commonly used indexes of segregation, the Divergence and Dissimilarity Indexes. These indices measure how divergent and dissimilar a given area is in comparison to the entire county and range from 0 to 1, where higher values indicate higher levels of segregation. In brief, the Divergence index measures the degree to which race breakdowns in census tracts within counties match the overall county race breakdown. The Dissimilarity Index measures the percent of individuals from the minority group that would need to move relative to White individuals such that census tracts were equally distributed by race. See below for a conceptual figure explaining how these measures of segregation are calculated.
The research team was also interested in racial and ethnic composition in a county and the following covariates: urbanicity, political orientation, and 2019 overdose mortality. Data for racial and ethnic composition was obtained from the American Community Survey, conducted by the US Census Bureau, for the 5-year period between 2016 and 2020. Urbanicity was determined by the NCHS Urban-Rural Classification Scheme. Political orientation was assessed by calculating the percent of votes within the county for the Republican presidential candidate in 2020, as this may serve as a proxy for opposition to harm reduction methods. Overdose mortality was calculated for the year 2019 per 100,000 people in a county. All deaths involving opioids in 2019 were included.
A total of 3106 counties in the contiguous US were analyzed – each “case” was a county, agnostic to its overall population – i.e., there was no weighting by the number of people living in a given county such that more populous and less populous counties were both counted as 1 county. Analyses were first conducted to examine whether the Divergence and Dissimilarity indices are predictive of the presence or absence of a syringe service program operating in the county. Separate analyses were then conducted to examine whether the Divergence and Dissimilarity indices are predictive of the rates of syringe and naloxone distribution per 100,000 people in a county. Covariates were also included in all models. The proportion of non-Hispanic Black, non-Hispanic Asian, non-Hispanic Other, and Hispanic people within a county were further compared to the proportion of non-Hispanic White people. Finally, analyses were conducted to examine whether missingness biased the results.
Syringe service programs were reported to be operating in 9% of counties. On average, there were 10,099 syringes and 112 naloxone doses distributed per 100,000 people. Levels of segregation varied from no segregation to almost total segregation. In an average county (irrespective of population size), the percent of votes for the Republican presidential candidate was 56% and the mean opioid overdose mortality rate was 13.07 per 100,000 people. Counties had a mean percentage of 76% non-Hispanic White people, 9% non-Hispanic Black people, 1.3% non-Hispanic Asian people, 4% people identifying as non-Hispanic Other, and 9.6% Hispanic people. For urbanicity, counties were 63% rural, 35% suburban, and 2% urban.
WHAT DID THIS STUDY FIND?
Counties with higher levels of racial segregation had more syringe service programs
Higher levels of racial segregation were associated with greater chances of a syringe service program operating in the county. As the Divergence Index increased, the chances of a program operating in the county increased by 33%. As the Black-White and Hispanic-White Dissimilarity Indices increased, the chances of a program operating in the county increased by 66% and 78%, respectively. However, no differences were found when comparing the chances of a program operating in counties with greater raw proportions of Black, Asian, and Hispanic people to counties with greater proportions of non-Hispanic White people. Missing data was not found to bias these results.
Counties with higher levels of racial segregation distributed fewer syringes and naloxone doses
Higher levels of racial segregation were associated with lower rates of syringe distribution per capita (e.g., controlling for the number of people). As the Divergence Index increased, the rate of syringe distribution decreased by 33%. As the Hispanic-White Dissimilarity Index increased, the rate of syringe distribution decreased by 35%. Additionally, counties with higher proportions of Black individuals distributed 31% fewer syringes than counties with higher proportions of non-Hispanic White individuals. Missing data was not found to bias these results.
Higher levels of racial segregation were not associated with rates of naloxone distribution, as measured by the Divergence and Dissimilarity Indices, but there were differences in the racial compositions of the counties. Counties with higher proportions of people who identified as Other race and Hispanic distributed 40% and 3% fewer naloxone doses, respectively, than counties with higher proportions of non-Hispanic White people. Missing data was not found to bias these results.
County characteristics were associated with chances of syringe service program operation and syringe and naloxone distribution
Urbanicity was associated with greater likelihood of a syringe service program operating in the county and lower rates of syringe and naloxone distribution. Urban counties had an almost 17-fold greater chance of a syringe service program operating than rural counties, and suburban counties were almost twice as likely as rural counties. However, urban and suburban counties distributed 3% and 10% fewer syringes and 1% and 5% fewer naloxone doses per capita than rural counties, respectively.
Republican political orientation was associated with a decreased chance of a syringe service program operating in the county but was not associated with rates of syringe and naloxone distribution. Counties with a higher proportion of Republican votes in the 2020 presidential election were 49% less likely to have a syringe service program operating.
Opioid overdose mortality rates were also associated with the chances of a syringe service program operating in the county but were not associated with rates of syringe and naloxone distribution. Counties with higher overdose mortality rates were 60% more likely to have a syringe service program operating.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team examined the associations of racial residential segregation with syringe service program operation and distribution of syringes and naloxone doses in counties across the United States. Results showed that counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses per capita. Likewise, urban and suburban counties were more likely to have a program in operation than rural counties but distributed fewer syringes and naloxone doses per capita. Finally, the percentage of Republican votes in a county was associated with a decreased chance of a syringe service program operating and opioid overdose mortality rates were associated with an increased chance, but neither were associated with rates of syringe and naloxone distributions.
These results suggest that racially segregated counties, and those with a greater need for harm reduction services, are aiming to meet the needs of the community by implementing a syringe service program. This is consistent with prior studies that have shown that higher levels of racial segregation are associated with higher levels of resilience and cultures of care for others, which may be explained by people in these communities feeling they are best positioned to rely on peers and community leaders, rather than federal and state governments, to meet their needs.
However, the finding that these racially segregated counties also distributed fewer syringes and naloxone doses suggests that these communities may lack the resources to be able to adequately staff their programs and scale harm reduction distribution efforts for successful implementation. These deficits in resources may be explained by long-standing structural inequities. Also of note, many of these programs operate in brick-and-mortar physical locations, limiting their capacity to scale. Then, when examining per capita distribution, syringe programs reach a smaller proportion of these more populous counties compared to programs in rural areas which may reach a larger proportion simply because they have fewer overall people to serve. Future studies can examine whether strategies to extend access beyond physical locations – e.g., mobile syringe distribution vans, etc. – can help to redress these difficulties with distribution. Overall, addressing these community level factors may help to improve the ability of syringe service programs to achieve greater levels of syringe and naloxone distribution, thereby helping to prevent overdoses and infectious diseases.
There may have been syringe service programs operating in the United States that were not included in the analyses. The impact this could have had on the results is unclear and may have depended on the area the programs were operating in.
Data on harm reduction services was collected by self-report, which is known to be subject to response biases, such as recall or social desirability. People may, for example, be more likely to report higher rates of syringe and naloxone distributions because they think it is a desirable outcome for the researchers. Of note, however, county level data were derived from US census and related rigorously collected, publicly available data.
Most of the counties in the US, and thus in the study, are not urban, which is where the racial segregation measures are more precise given larger populations.
BOTTOM LINE
Counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses. This suggests that racially segregated counties are aiming to meet the needs of the community by implementing a syringe service program but may lack the resources to be able to adequately scale harm reduction distribution efforts.
For individuals and families seeking recovery: This study found that counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses. The presence of a syringe service program reflects the resilience and culture of care for others that racially segregated communities display, while the low distribution rates may reflect a lack of resources for successful implementation. Accordingly, people in these communities may similarly rely on grassroots efforts for fundraising to improve the distribution rates of harm reduction supplies. Individuals may also advocate for local and federal policymakers to address structural inequities and provide greater investments in these communities.
For treatment professionals and treatment systems: This study showed that counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses. Low distribution rates may reflect a lack of resources for successful implementation due to structural barriers and disinvestment, but the presence of syringe service programs reflects the communities’ ability and willingness meet its needs as a grassroots level. Treatment professionals may help to boost these programs’ resources by holding fundraisers or advocating at the local and federal levels. Such efforts may improve the distribution rates of harm reduction supplies, thereby preventing overdoses and infectious disease.
For scientists: This study showed that counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses. Future studies might test whether strategies can help extend the reach of brick-and-mortar harm reduction programs – e.g., mobile vans to distribute syringes – to improve distribution.
For policy makers: This study demonstrated that counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses. These results reflect the desire and willingness of communities to implement a syringe service program, but also suggest that they may lack the necessary resources to scale such efforts across their respective counties. Such challenges to scaling harm reduction may be explained by structural inequities; thus, policies that help address these barriers and invest in disadvantaged communities may improve these programs’ ability to achieve greater rates of harm reduction supply distribution, which can lead to fewer overdoses and reduced rates of infectious disease.
The United States is currently experiencing not only an opioid overdose epidemic, but also epidemics of Hepatitis C and infections of the skin, soft tissues, and heart, as well as HIV outbreaks. These multiple epidemics disproportionately impact racial minorities, with the highest increases of overdose deaths being observed among people who are American Indian, Alaskan Native, and Black. HIV diagnoses are also higher among Black and Hispanic people than would be expected given their share of the general population.
Harm reduction strategies, such as syringe service programs and broad access to naloxone, can help prevent overdoses and infectious diseases. However, racial minorities often have unequal access to such services. Further, even in areas where there may be equal or higher access, the full impact of services may not be realized. For example, in one recent study, municipalities in Massachusetts with greater proportions of Black people had higher rates of naloxone coverage, but this increased naloxone presence did not decrease overdose deaths during the pandemic in this group.
These inequities can be explained, in part, by structural racism. For example, practices such as redlining for home mortgages and exclusionary real estate practices have created racial residential segregation and economic inequality. In these “racialized environments”, residents have fewer opportunities to advance economically and experience more social and health disadvantages. This study examined whether there is differential access to syringe service programs and harm reduction supplies because of racial segregation. This research can help address health inequities that disproportionately impact racial minorities.
HOW WAS THIS STUDY CONDUCTED?
The research team explored the associations of racial segregation with syringe service program operation and distribution of syringes and naloxone doses by collecting information from program directors about their program operations in 2021. Covariates that were controlled for included, urbanicity, political orientation, and 2019 overdose mortality. Information was collected as part of the National Survey of Syringe Service Programs. For this survey, the research team recruited syringe service programs in the US from a variety of sources, including various networks, social media, and conferences, from February to June 2021. Program directors were emailed up to 3 times asking for their participation in the online survey and then non-responders were called. The survey asked participants what county their program operated in during 2020 and how many syringes and naloxone doses were distributed by their program. Out of 412 programs that were contacted, 295 program directors participated. Participants were compensated for $75 for their time completing the survey.
The primary outcomes of interest were 3 county-level measures that were constructed using geocoding. The first measure was whether or not a syringe service program operated in the county (yes/no). The second measure was county-level per capita syringe distribution, which was calculated by dividing the total number of syringes distributed across programs, as reported by program directors in the survey, by the population size of the county. The third measure was county-level per capita naloxone distribution, which was similarly calculated by dividing the total number of naloxone doses distributed across programs, as reported by program directors in the survey, by the population size of the county.
The primary predictor was racial residential segregation, measured in this study by 2 commonly used indexes of segregation, the Divergence and Dissimilarity Indexes. These indices measure how divergent and dissimilar a given area is in comparison to the entire county and range from 0 to 1, where higher values indicate higher levels of segregation. In brief, the Divergence index measures the degree to which race breakdowns in census tracts within counties match the overall county race breakdown. The Dissimilarity Index measures the percent of individuals from the minority group that would need to move relative to White individuals such that census tracts were equally distributed by race. See below for a conceptual figure explaining how these measures of segregation are calculated.
The research team was also interested in racial and ethnic composition in a county and the following covariates: urbanicity, political orientation, and 2019 overdose mortality. Data for racial and ethnic composition was obtained from the American Community Survey, conducted by the US Census Bureau, for the 5-year period between 2016 and 2020. Urbanicity was determined by the NCHS Urban-Rural Classification Scheme. Political orientation was assessed by calculating the percent of votes within the county for the Republican presidential candidate in 2020, as this may serve as a proxy for opposition to harm reduction methods. Overdose mortality was calculated for the year 2019 per 100,000 people in a county. All deaths involving opioids in 2019 were included.
A total of 3106 counties in the contiguous US were analyzed – each “case” was a county, agnostic to its overall population – i.e., there was no weighting by the number of people living in a given county such that more populous and less populous counties were both counted as 1 county. Analyses were first conducted to examine whether the Divergence and Dissimilarity indices are predictive of the presence or absence of a syringe service program operating in the county. Separate analyses were then conducted to examine whether the Divergence and Dissimilarity indices are predictive of the rates of syringe and naloxone distribution per 100,000 people in a county. Covariates were also included in all models. The proportion of non-Hispanic Black, non-Hispanic Asian, non-Hispanic Other, and Hispanic people within a county were further compared to the proportion of non-Hispanic White people. Finally, analyses were conducted to examine whether missingness biased the results.
Syringe service programs were reported to be operating in 9% of counties. On average, there were 10,099 syringes and 112 naloxone doses distributed per 100,000 people. Levels of segregation varied from no segregation to almost total segregation. In an average county (irrespective of population size), the percent of votes for the Republican presidential candidate was 56% and the mean opioid overdose mortality rate was 13.07 per 100,000 people. Counties had a mean percentage of 76% non-Hispanic White people, 9% non-Hispanic Black people, 1.3% non-Hispanic Asian people, 4% people identifying as non-Hispanic Other, and 9.6% Hispanic people. For urbanicity, counties were 63% rural, 35% suburban, and 2% urban.
WHAT DID THIS STUDY FIND?
Counties with higher levels of racial segregation had more syringe service programs
Higher levels of racial segregation were associated with greater chances of a syringe service program operating in the county. As the Divergence Index increased, the chances of a program operating in the county increased by 33%. As the Black-White and Hispanic-White Dissimilarity Indices increased, the chances of a program operating in the county increased by 66% and 78%, respectively. However, no differences were found when comparing the chances of a program operating in counties with greater raw proportions of Black, Asian, and Hispanic people to counties with greater proportions of non-Hispanic White people. Missing data was not found to bias these results.
Counties with higher levels of racial segregation distributed fewer syringes and naloxone doses
Higher levels of racial segregation were associated with lower rates of syringe distribution per capita (e.g., controlling for the number of people). As the Divergence Index increased, the rate of syringe distribution decreased by 33%. As the Hispanic-White Dissimilarity Index increased, the rate of syringe distribution decreased by 35%. Additionally, counties with higher proportions of Black individuals distributed 31% fewer syringes than counties with higher proportions of non-Hispanic White individuals. Missing data was not found to bias these results.
Higher levels of racial segregation were not associated with rates of naloxone distribution, as measured by the Divergence and Dissimilarity Indices, but there were differences in the racial compositions of the counties. Counties with higher proportions of people who identified as Other race and Hispanic distributed 40% and 3% fewer naloxone doses, respectively, than counties with higher proportions of non-Hispanic White people. Missing data was not found to bias these results.
County characteristics were associated with chances of syringe service program operation and syringe and naloxone distribution
Urbanicity was associated with greater likelihood of a syringe service program operating in the county and lower rates of syringe and naloxone distribution. Urban counties had an almost 17-fold greater chance of a syringe service program operating than rural counties, and suburban counties were almost twice as likely as rural counties. However, urban and suburban counties distributed 3% and 10% fewer syringes and 1% and 5% fewer naloxone doses per capita than rural counties, respectively.
Republican political orientation was associated with a decreased chance of a syringe service program operating in the county but was not associated with rates of syringe and naloxone distribution. Counties with a higher proportion of Republican votes in the 2020 presidential election were 49% less likely to have a syringe service program operating.
Opioid overdose mortality rates were also associated with the chances of a syringe service program operating in the county but were not associated with rates of syringe and naloxone distribution. Counties with higher overdose mortality rates were 60% more likely to have a syringe service program operating.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team examined the associations of racial residential segregation with syringe service program operation and distribution of syringes and naloxone doses in counties across the United States. Results showed that counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses per capita. Likewise, urban and suburban counties were more likely to have a program in operation than rural counties but distributed fewer syringes and naloxone doses per capita. Finally, the percentage of Republican votes in a county was associated with a decreased chance of a syringe service program operating and opioid overdose mortality rates were associated with an increased chance, but neither were associated with rates of syringe and naloxone distributions.
These results suggest that racially segregated counties, and those with a greater need for harm reduction services, are aiming to meet the needs of the community by implementing a syringe service program. This is consistent with prior studies that have shown that higher levels of racial segregation are associated with higher levels of resilience and cultures of care for others, which may be explained by people in these communities feeling they are best positioned to rely on peers and community leaders, rather than federal and state governments, to meet their needs.
However, the finding that these racially segregated counties also distributed fewer syringes and naloxone doses suggests that these communities may lack the resources to be able to adequately staff their programs and scale harm reduction distribution efforts for successful implementation. These deficits in resources may be explained by long-standing structural inequities. Also of note, many of these programs operate in brick-and-mortar physical locations, limiting their capacity to scale. Then, when examining per capita distribution, syringe programs reach a smaller proportion of these more populous counties compared to programs in rural areas which may reach a larger proportion simply because they have fewer overall people to serve. Future studies can examine whether strategies to extend access beyond physical locations – e.g., mobile syringe distribution vans, etc. – can help to redress these difficulties with distribution. Overall, addressing these community level factors may help to improve the ability of syringe service programs to achieve greater levels of syringe and naloxone distribution, thereby helping to prevent overdoses and infectious diseases.
There may have been syringe service programs operating in the United States that were not included in the analyses. The impact this could have had on the results is unclear and may have depended on the area the programs were operating in.
Data on harm reduction services was collected by self-report, which is known to be subject to response biases, such as recall or social desirability. People may, for example, be more likely to report higher rates of syringe and naloxone distributions because they think it is a desirable outcome for the researchers. Of note, however, county level data were derived from US census and related rigorously collected, publicly available data.
Most of the counties in the US, and thus in the study, are not urban, which is where the racial segregation measures are more precise given larger populations.
BOTTOM LINE
Counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses. This suggests that racially segregated counties are aiming to meet the needs of the community by implementing a syringe service program but may lack the resources to be able to adequately scale harm reduction distribution efforts.
For individuals and families seeking recovery: This study found that counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses. The presence of a syringe service program reflects the resilience and culture of care for others that racially segregated communities display, while the low distribution rates may reflect a lack of resources for successful implementation. Accordingly, people in these communities may similarly rely on grassroots efforts for fundraising to improve the distribution rates of harm reduction supplies. Individuals may also advocate for local and federal policymakers to address structural inequities and provide greater investments in these communities.
For treatment professionals and treatment systems: This study showed that counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses. Low distribution rates may reflect a lack of resources for successful implementation due to structural barriers and disinvestment, but the presence of syringe service programs reflects the communities’ ability and willingness meet its needs as a grassroots level. Treatment professionals may help to boost these programs’ resources by holding fundraisers or advocating at the local and federal levels. Such efforts may improve the distribution rates of harm reduction supplies, thereby preventing overdoses and infectious disease.
For scientists: This study showed that counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses. Future studies might test whether strategies can help extend the reach of brick-and-mortar harm reduction programs – e.g., mobile vans to distribute syringes – to improve distribution.
For policy makers: This study demonstrated that counties with higher levels of racial segregation were more likely to have a syringe service program operating but distributed fewer syringes and naloxone doses. These results reflect the desire and willingness of communities to implement a syringe service program, but also suggest that they may lack the necessary resources to scale such efforts across their respective counties. Such challenges to scaling harm reduction may be explained by structural inequities; thus, policies that help address these barriers and invest in disadvantaged communities may improve these programs’ ability to achieve greater rates of harm reduction supply distribution, which can lead to fewer overdoses and reduced rates of infectious disease.