Reducing opioid prescriptions decreases opioid use and related harms, but it takes time
Despite recent large-scale efforts to combat the opioid overdose epidemic, including reductions in opioid overprescribing, poisoning deaths continue to rise at unprecedented levels. This study examined whether a time lag between prescription reductions and lives saved is one potential reason for this discrepancy.
Efforts have been made to help combat the opioid overdose epidemic, including reducing the number of opioids prescribed. Since 2011, prescription opioids were reduced by over a third. However, opioid overdose deaths have continued to increase at unprecedented rates, with more than 100,000 people dying from overdoses in 2021. There have been major criticisms on policies that reduce opioid prescribing in the absence of systemic increases in addiction treatment access which, these experts suggest, have contributedto the increase in overdose deaths. The rise of the use of heroin and illicit fentanyl are also part of the reason for this discrepancy, but the beneficial impacts of reducing prescription opioids is unclear.
Given that opioid prescription reduction policies reduce the supply of opioids (i.e., availability), but not its demand (i.e., the conditions associated with opioid use disorder), one potential reason for the discrepancy is a possible lag between prescription reductions and downstream effects on lives saved. This study aimed to examine this possibility, as well as the impact of prescription reductions on cases of opioid use disorder. Such research can help shed light on the long-term impacts of opioid prescription reductions in the context of concerns about the harms of such policies in the short-term (e.g., that a reduction in prescription availability could turn people with opioid use disorder toward illicit supply).
HOW WAS THIS STUDY CONDUCTED?
The research team used statistical modeling to examine the cumulative impact of reducing the number of prescription opioids on lives saved and cases of opioid use disorder from 2011 to 2029. This model can help the researchers understand the relationship between the number of prescription opioids, other treatments, and lives saved across time, using observed and projected data. The model estimated populations in different stages of opioid use among individuals in the United States 12+ years old by drawing upon publicly available datasets (i.e., the United States Census Bureau, Centers for Disease Control and Prevention, National Survey on Drug Use and Health, National Health and Nutrition Examination Survey, and National Epidemiologic Survey on Alcohol and Related Conditions). The researchers used this data to incorporate changing levels of treatment based on data from 2001 to 2017, as well as a projected annual decline of 3% in opioid prescriptions from 2020 to 2029.
In the model, the researchers defined 3 categories of opioid use. Prescription opioid medical use was defined as opioid use as directed and prescribed by a licensed prescriber. Prescription opioid non-medical use was defined as the misuse of opioids, regardless of whether the misuse started with a prescription. Illicit opioid use was defined as the use of heroin, synthetic fentanyl, or other illicit opioids.
Individuals in these categories then had the potential to develop opioid use disorder, which the researchers also divided into 3 categories: (1) opioid use disorder from prescription use only, without prior or current illicit use; (2) opioid use disorder from illicit use with prior prescription non-medical use; and (3) opioid use disorder from illicit use without non-medical use of prescription opioids. Each of these three opioid use disorder categories include several subcategories of use, medication-assisted treatment, and detoxification or “detox” (defined as physiological detoxification and withdrawal, regardless of entering a treatment facility).
When the researchers programmed the model to estimate the number of people who died from an overdose in the United States, they included data from all three opioid use disorder categories. However, when estimating the impact of reducing the number of prescription opioids, they excluded data from the third one – opioid use disorder from illicit use without prior non-medical use of prescription opioids.
The researchers then ran 2 main statistical analyses. In their first analysis, they estimated the number of opioid overdose deaths averted by observed and future reductions in opioid prescribing. In their second analysis, they used a simulated cohort of individuals who initiated medical use of prescription opioids (i.e., taking as prescribed by a medical professional) to estimate the number of people who would go on to non-medical use of prescription opioids and, of those, the number that would develop prescription opioid use disorder and experience opioid overdose deaths.
WHAT DID THIS STUDY FIND?
There is a time lag between reductions in opioid prescriptions and decreases in opioid use disorder.
Between 2010 and 2019, the number of opioid prescriptions per 100 people decreased from 81.2 to 46.7, a reduction of 42.5%. This reduction coincided with a projected 8.5% increase in the number of active prescription opioid use disorder cases during the same time period.
Of the estimated 2.4 million individuals with an active opioid use disorder in 2019, 65% first used opioids for medical reasons prior to 2011. However, only 14% first used opioids for medical reasons between 2017 and 2019.
By 2029, it was projected that approximately 2.5 million people will have an active opioid use disorder, of whom 54% would have first used opioids for medical reasons prior to 2011, whereas 29% first used opioids for medical reasons between 2020 and 2029.
There is a time lag between reductions in opioid prescriptions and lives saved.
The 42.5% reduction in the rate of opioid prescriptions per 100 people between 2010 and 2019 coincided with a projected 103.2% increase in the number fatal opioid overdoses during the same time period.
Of the 78.3 million individuals who were first prescribed an opioid in 2011, 13,663 died from an opioid overdose (0.02%).
Of the projected 37,183 opioid overdose deaths that occurred in 2019 among those with non-medical use of prescription opioids, 64% first used opioids for medical reasons prior to 2011. However, only 17% occurred among people who first used opioids for medical reasons between 2017 and 2019.
By 2029, it was projected that 38,940 opioid overdose deaths will have occurred among people with non-medical use of prescription opioids, of whom 54% would have first used opioids for medical reasons prior to 2011, whereas 28% first used opioids between 2020 and 2029.
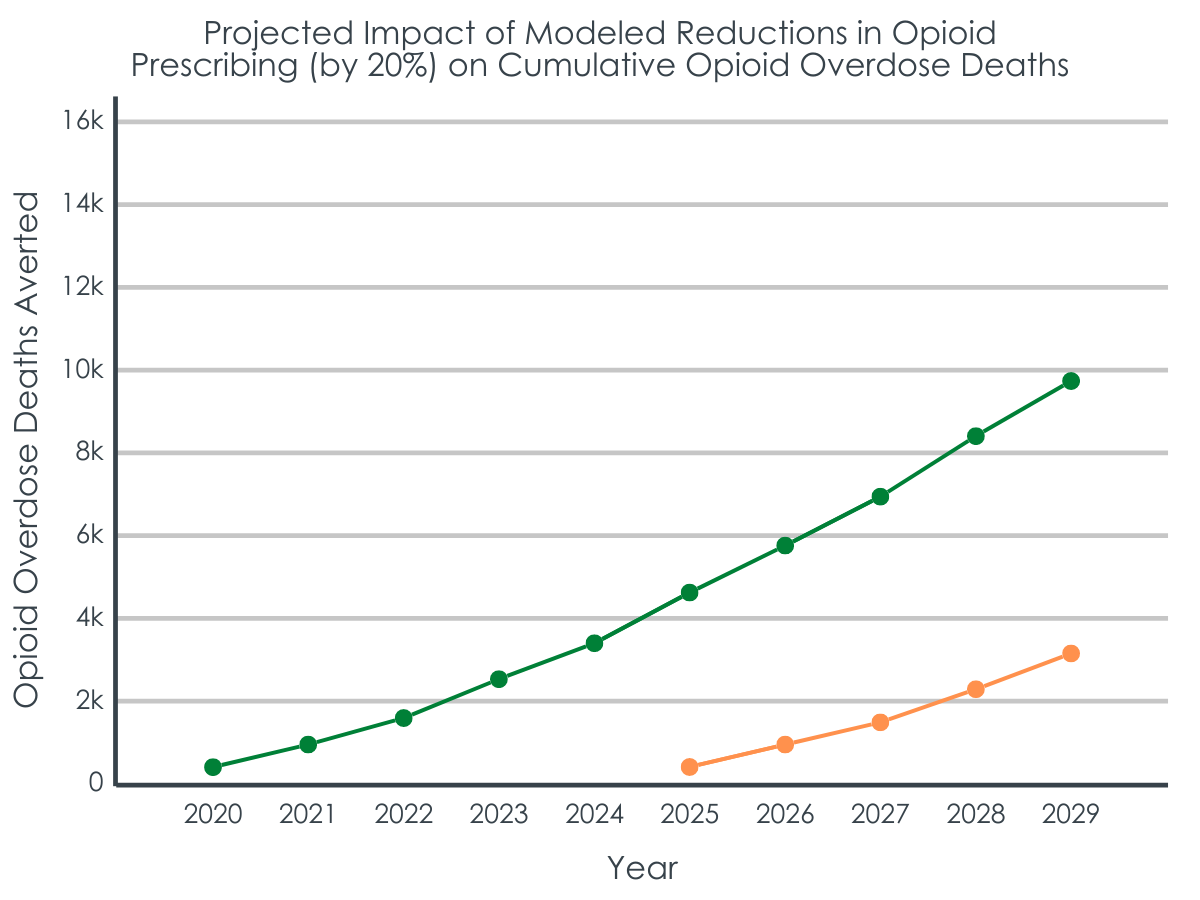
When compared to a hypothetical where the 2010 opioid prescription rate was maintained over time, reductions that occurred between 2010 and 2019 are estimated to have prevented 9600 opioid overdose deaths by 2019, and are projected to prevent another 50,918 deaths between 2020 and 2029. As such, only 18.9% of the impact of the prescription reductions was seen in the first decade (2010-2019) and the remaining 81% is projected in the second decade.
Several hypothetical prescription reduction scenarios further illustrated that larger reductions implemented earlier averted more opioid overdose deaths rather than smaller reductions implemented later.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study used computer modeling to show that reducing the number of prescription opioids saves lives and reduces cases of opioid use disorder, but with a time lag between opioid prescription reductions and downstream benefits. The largest public health benefits are not evident until the second decade of implementing the reductions.
The illustration of the lag period between prescription reductions and beneficial effects helps to resolve the discrepancy of opioid overdoses continuing to rise at unprecedented rates despite the reductions.
For instance, most of the cases of opioid use disorder and overdose deaths that occurred in 2019 were projected to have been among people who first used prescription opioids a decade or more earlier. The reductions were also projected to have already saved almost 10,000 lives and to have prevented more than 5 times as many overdose deaths in the next decade compared to a hypothetical where the number of prescriptions remained at 2010 levels. These delayed effects are similar to the lag observed between decreases in lung cancer cases and smoking cessation campaigns, since the decreases in lung cancer were not observed until decades after smoking rates began to decrease. This supports the policy change of prescription reductions.
Taken together, these results suggest that reducing the number of prescription opioids can have beneficial effects, but these effects take time to see. Accordingly, prescription reductions should be implemented as part of a larger, multi-level national public health strategy that includes expanding access to treatment,harm reduction,and recovery support services to have a more immediate impact on the opioid epidemic. Further, there are potential harms of reducing opioid medications for long-term pain patientsthat need to be considered, such that any reductions should be based on empirically-supported protocols and paired with linkages to substance use disorder treatment if needed.
Because the researchers used statistical modeling to predict results, the results should be viewed as projections rather than empirical observations. For instance, there is no direct data to determine the effect of any single intervention in isolation. Other outside factors that were not accounted for in the models could have affected the results. However, the data that were used to provide information to the models were based on the best available scientific data estimates.
The researchers programmed the models based on total opioid-related overdose deaths rather than opioid use disorder cases. Therefore, the estimates of the number of people with opioid use disorder may be underestimates since opioid use disorder cases that did not result in overdose deaths would have been missed. There are also limitations of the datasets used and changes in diagnostic criteria of opioid use disorder that may have further contributed to underestimates of opioid use disorder cases.
Since the researchers also programmed the models based on 2010 data, it is not possible to determine how effects prior to 2010 affected the results.
The model only accounted for potential secondary effects of some interventions. It was not possible to account for all of them. This may have resulted in an underestimation of the effects the prescription reductions have when implemented as part of a larger, comprehensive strategy to address the opioid epidemic.
The effects of other potential contributors to the discrepancy of opioid overdoses continuing to rise despite reductions in the number of opioid prescriptions, such as the rise of the use of illicit fentanyl, were not analyzed. Increases in fentanyl use have been associated with large increases in the number of overdose deaths.
BOTTOM LINE
Reducing the number of prescription opioids appears to have saved lives, prevented future deaths from opioid overdoses, and reduced opioid use disorder cases, although there is a decade-long time lag between the reductions and observed beneficial impacts. This suggests efforts to reduce opioid exposure by reducing opioid prescriptions enhances public health. However, given the paradoxical harms of reducing opioid prescriptions among certain population segments such as among pain patients, they should be used as part of other strategies to expand access to treatment and harm reduction services.
For individuals and families seeking recovery: Opioid prescription reductions can improve public health, but their beneficial effects take some time to be seen.In the meantime, individuals and families are encouraged to take advantage of currently available evidence-based treatments, such as medications and therapy. Individualscan also prevent opioid-related overdoses and other harms by engaging in harm reduction strategies, such as having ready availability of naloxone (Narcan) to reverse overdoses, and recovery services, such as peer support.
For treatment professionals and treatment systems: This prevention-focused study shows that public health benefits of opioid prescription reductions may take time to exert their most beneficial effects. In the meantime, there are risks to opioid prescription reductions that can be mitigatedby the use of empirically-supported tapering protocols and linkages to substance use disorder treatment (e.g., medications for opioid use disorder) and recovery supports.
For scientists:While the current study demonstrated the time lag between reductions in prescription opioids and lives saved, as well as reduced opioid use disorder cases, there are some limitations. If future research addressed these limitations, it could help to shed additional light on the impact of opioid prescription reductions. For instance, if scientists examined the effects of other treatment and harm reduction strategies for opioid use disorder not included in the current study, they could contribute to a greater understanding of how opioid prescription reductions impact opioid use disorder cases and overdose deaths. Further, additional research that uses data based on opioid use disorder cases rather than total overdose deaths to program statistical models could provide a more accurate estimate of the number of people with opioid use disorder.
For policy makers: Given the potential benefits of reducing the number of opioid prescriptions, continuing to support policies that limit opioid prescriptions could have important effects on lives saved from opioid overdoses and decreasing rates of opioid use disorder. Such policies, however, also need to consider the needs of certain population segments, such as people with chronic pain. Further, since there is a lag period between prescription reductions and beneficial impacts, support of policies that expand access to treatment and harm reduction services could have a more immediate impact on the opioid epidemic.
Efforts have been made to help combat the opioid overdose epidemic, including reducing the number of opioids prescribed. Since 2011, prescription opioids were reduced by over a third. However, opioid overdose deaths have continued to increase at unprecedented rates, with more than 100,000 people dying from overdoses in 2021. There have been major criticisms on policies that reduce opioid prescribing in the absence of systemic increases in addiction treatment access which, these experts suggest, have contributedto the increase in overdose deaths. The rise of the use of heroin and illicit fentanyl are also part of the reason for this discrepancy, but the beneficial impacts of reducing prescription opioids is unclear.
Given that opioid prescription reduction policies reduce the supply of opioids (i.e., availability), but not its demand (i.e., the conditions associated with opioid use disorder), one potential reason for the discrepancy is a possible lag between prescription reductions and downstream effects on lives saved. This study aimed to examine this possibility, as well as the impact of prescription reductions on cases of opioid use disorder. Such research can help shed light on the long-term impacts of opioid prescription reductions in the context of concerns about the harms of such policies in the short-term (e.g., that a reduction in prescription availability could turn people with opioid use disorder toward illicit supply).
HOW WAS THIS STUDY CONDUCTED?
The research team used statistical modeling to examine the cumulative impact of reducing the number of prescription opioids on lives saved and cases of opioid use disorder from 2011 to 2029. This model can help the researchers understand the relationship between the number of prescription opioids, other treatments, and lives saved across time, using observed and projected data. The model estimated populations in different stages of opioid use among individuals in the United States 12+ years old by drawing upon publicly available datasets (i.e., the United States Census Bureau, Centers for Disease Control and Prevention, National Survey on Drug Use and Health, National Health and Nutrition Examination Survey, and National Epidemiologic Survey on Alcohol and Related Conditions). The researchers used this data to incorporate changing levels of treatment based on data from 2001 to 2017, as well as a projected annual decline of 3% in opioid prescriptions from 2020 to 2029.
In the model, the researchers defined 3 categories of opioid use. Prescription opioid medical use was defined as opioid use as directed and prescribed by a licensed prescriber. Prescription opioid non-medical use was defined as the misuse of opioids, regardless of whether the misuse started with a prescription. Illicit opioid use was defined as the use of heroin, synthetic fentanyl, or other illicit opioids.
Individuals in these categories then had the potential to develop opioid use disorder, which the researchers also divided into 3 categories: (1) opioid use disorder from prescription use only, without prior or current illicit use; (2) opioid use disorder from illicit use with prior prescription non-medical use; and (3) opioid use disorder from illicit use without non-medical use of prescription opioids. Each of these three opioid use disorder categories include several subcategories of use, medication-assisted treatment, and detoxification or “detox” (defined as physiological detoxification and withdrawal, regardless of entering a treatment facility).
When the researchers programmed the model to estimate the number of people who died from an overdose in the United States, they included data from all three opioid use disorder categories. However, when estimating the impact of reducing the number of prescription opioids, they excluded data from the third one – opioid use disorder from illicit use without prior non-medical use of prescription opioids.
The researchers then ran 2 main statistical analyses. In their first analysis, they estimated the number of opioid overdose deaths averted by observed and future reductions in opioid prescribing. In their second analysis, they used a simulated cohort of individuals who initiated medical use of prescription opioids (i.e., taking as prescribed by a medical professional) to estimate the number of people who would go on to non-medical use of prescription opioids and, of those, the number that would develop prescription opioid use disorder and experience opioid overdose deaths.
WHAT DID THIS STUDY FIND?
There is a time lag between reductions in opioid prescriptions and decreases in opioid use disorder.
Between 2010 and 2019, the number of opioid prescriptions per 100 people decreased from 81.2 to 46.7, a reduction of 42.5%. This reduction coincided with a projected 8.5% increase in the number of active prescription opioid use disorder cases during the same time period.
Of the estimated 2.4 million individuals with an active opioid use disorder in 2019, 65% first used opioids for medical reasons prior to 2011. However, only 14% first used opioids for medical reasons between 2017 and 2019.
By 2029, it was projected that approximately 2.5 million people will have an active opioid use disorder, of whom 54% would have first used opioids for medical reasons prior to 2011, whereas 29% first used opioids for medical reasons between 2020 and 2029.
There is a time lag between reductions in opioid prescriptions and lives saved.
The 42.5% reduction in the rate of opioid prescriptions per 100 people between 2010 and 2019 coincided with a projected 103.2% increase in the number fatal opioid overdoses during the same time period.
Of the 78.3 million individuals who were first prescribed an opioid in 2011, 13,663 died from an opioid overdose (0.02%).
Of the projected 37,183 opioid overdose deaths that occurred in 2019 among those with non-medical use of prescription opioids, 64% first used opioids for medical reasons prior to 2011. However, only 17% occurred among people who first used opioids for medical reasons between 2017 and 2019.
By 2029, it was projected that 38,940 opioid overdose deaths will have occurred among people with non-medical use of prescription opioids, of whom 54% would have first used opioids for medical reasons prior to 2011, whereas 28% first used opioids between 2020 and 2029.
When compared to a hypothetical where the 2010 opioid prescription rate was maintained over time, reductions that occurred between 2010 and 2019 are estimated to have prevented 9600 opioid overdose deaths by 2019, and are projected to prevent another 50,918 deaths between 2020 and 2029. As such, only 18.9% of the impact of the prescription reductions was seen in the first decade (2010-2019) and the remaining 81% is projected in the second decade.
Several hypothetical prescription reduction scenarios further illustrated that larger reductions implemented earlier averted more opioid overdose deaths rather than smaller reductions implemented later.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study used computer modeling to show that reducing the number of prescription opioids saves lives and reduces cases of opioid use disorder, but with a time lag between opioid prescription reductions and downstream benefits. The largest public health benefits are not evident until the second decade of implementing the reductions.
The illustration of the lag period between prescription reductions and beneficial effects helps to resolve the discrepancy of opioid overdoses continuing to rise at unprecedented rates despite the reductions.
For instance, most of the cases of opioid use disorder and overdose deaths that occurred in 2019 were projected to have been among people who first used prescription opioids a decade or more earlier. The reductions were also projected to have already saved almost 10,000 lives and to have prevented more than 5 times as many overdose deaths in the next decade compared to a hypothetical where the number of prescriptions remained at 2010 levels. These delayed effects are similar to the lag observed between decreases in lung cancer cases and smoking cessation campaigns, since the decreases in lung cancer were not observed until decades after smoking rates began to decrease. This supports the policy change of prescription reductions.
Taken together, these results suggest that reducing the number of prescription opioids can have beneficial effects, but these effects take time to see. Accordingly, prescription reductions should be implemented as part of a larger, multi-level national public health strategy that includes expanding access to treatment,harm reduction,and recovery support services to have a more immediate impact on the opioid epidemic. Further, there are potential harms of reducing opioid medications for long-term pain patientsthat need to be considered, such that any reductions should be based on empirically-supported protocols and paired with linkages to substance use disorder treatment if needed.
Because the researchers used statistical modeling to predict results, the results should be viewed as projections rather than empirical observations. For instance, there is no direct data to determine the effect of any single intervention in isolation. Other outside factors that were not accounted for in the models could have affected the results. However, the data that were used to provide information to the models were based on the best available scientific data estimates.
The researchers programmed the models based on total opioid-related overdose deaths rather than opioid use disorder cases. Therefore, the estimates of the number of people with opioid use disorder may be underestimates since opioid use disorder cases that did not result in overdose deaths would have been missed. There are also limitations of the datasets used and changes in diagnostic criteria of opioid use disorder that may have further contributed to underestimates of opioid use disorder cases.
Since the researchers also programmed the models based on 2010 data, it is not possible to determine how effects prior to 2010 affected the results.
The model only accounted for potential secondary effects of some interventions. It was not possible to account for all of them. This may have resulted in an underestimation of the effects the prescription reductions have when implemented as part of a larger, comprehensive strategy to address the opioid epidemic.
The effects of other potential contributors to the discrepancy of opioid overdoses continuing to rise despite reductions in the number of opioid prescriptions, such as the rise of the use of illicit fentanyl, were not analyzed. Increases in fentanyl use have been associated with large increases in the number of overdose deaths.
BOTTOM LINE
Reducing the number of prescription opioids appears to have saved lives, prevented future deaths from opioid overdoses, and reduced opioid use disorder cases, although there is a decade-long time lag between the reductions and observed beneficial impacts. This suggests efforts to reduce opioid exposure by reducing opioid prescriptions enhances public health. However, given the paradoxical harms of reducing opioid prescriptions among certain population segments such as among pain patients, they should be used as part of other strategies to expand access to treatment and harm reduction services.
For individuals and families seeking recovery: Opioid prescription reductions can improve public health, but their beneficial effects take some time to be seen.In the meantime, individuals and families are encouraged to take advantage of currently available evidence-based treatments, such as medications and therapy. Individualscan also prevent opioid-related overdoses and other harms by engaging in harm reduction strategies, such as having ready availability of naloxone (Narcan) to reverse overdoses, and recovery services, such as peer support.
For treatment professionals and treatment systems: This prevention-focused study shows that public health benefits of opioid prescription reductions may take time to exert their most beneficial effects. In the meantime, there are risks to opioid prescription reductions that can be mitigatedby the use of empirically-supported tapering protocols and linkages to substance use disorder treatment (e.g., medications for opioid use disorder) and recovery supports.
For scientists:While the current study demonstrated the time lag between reductions in prescription opioids and lives saved, as well as reduced opioid use disorder cases, there are some limitations. If future research addressed these limitations, it could help to shed additional light on the impact of opioid prescription reductions. For instance, if scientists examined the effects of other treatment and harm reduction strategies for opioid use disorder not included in the current study, they could contribute to a greater understanding of how opioid prescription reductions impact opioid use disorder cases and overdose deaths. Further, additional research that uses data based on opioid use disorder cases rather than total overdose deaths to program statistical models could provide a more accurate estimate of the number of people with opioid use disorder.
For policy makers: Given the potential benefits of reducing the number of opioid prescriptions, continuing to support policies that limit opioid prescriptions could have important effects on lives saved from opioid overdoses and decreasing rates of opioid use disorder. Such policies, however, also need to consider the needs of certain population segments, such as people with chronic pain. Further, since there is a lag period between prescription reductions and beneficial impacts, support of policies that expand access to treatment and harm reduction services could have a more immediate impact on the opioid epidemic.
Efforts have been made to help combat the opioid overdose epidemic, including reducing the number of opioids prescribed. Since 2011, prescription opioids were reduced by over a third. However, opioid overdose deaths have continued to increase at unprecedented rates, with more than 100,000 people dying from overdoses in 2021. There have been major criticisms on policies that reduce opioid prescribing in the absence of systemic increases in addiction treatment access which, these experts suggest, have contributedto the increase in overdose deaths. The rise of the use of heroin and illicit fentanyl are also part of the reason for this discrepancy, but the beneficial impacts of reducing prescription opioids is unclear.
Given that opioid prescription reduction policies reduce the supply of opioids (i.e., availability), but not its demand (i.e., the conditions associated with opioid use disorder), one potential reason for the discrepancy is a possible lag between prescription reductions and downstream effects on lives saved. This study aimed to examine this possibility, as well as the impact of prescription reductions on cases of opioid use disorder. Such research can help shed light on the long-term impacts of opioid prescription reductions in the context of concerns about the harms of such policies in the short-term (e.g., that a reduction in prescription availability could turn people with opioid use disorder toward illicit supply).
HOW WAS THIS STUDY CONDUCTED?
The research team used statistical modeling to examine the cumulative impact of reducing the number of prescription opioids on lives saved and cases of opioid use disorder from 2011 to 2029. This model can help the researchers understand the relationship between the number of prescription opioids, other treatments, and lives saved across time, using observed and projected data. The model estimated populations in different stages of opioid use among individuals in the United States 12+ years old by drawing upon publicly available datasets (i.e., the United States Census Bureau, Centers for Disease Control and Prevention, National Survey on Drug Use and Health, National Health and Nutrition Examination Survey, and National Epidemiologic Survey on Alcohol and Related Conditions). The researchers used this data to incorporate changing levels of treatment based on data from 2001 to 2017, as well as a projected annual decline of 3% in opioid prescriptions from 2020 to 2029.
In the model, the researchers defined 3 categories of opioid use. Prescription opioid medical use was defined as opioid use as directed and prescribed by a licensed prescriber. Prescription opioid non-medical use was defined as the misuse of opioids, regardless of whether the misuse started with a prescription. Illicit opioid use was defined as the use of heroin, synthetic fentanyl, or other illicit opioids.
Individuals in these categories then had the potential to develop opioid use disorder, which the researchers also divided into 3 categories: (1) opioid use disorder from prescription use only, without prior or current illicit use; (2) opioid use disorder from illicit use with prior prescription non-medical use; and (3) opioid use disorder from illicit use without non-medical use of prescription opioids. Each of these three opioid use disorder categories include several subcategories of use, medication-assisted treatment, and detoxification or “detox” (defined as physiological detoxification and withdrawal, regardless of entering a treatment facility).
When the researchers programmed the model to estimate the number of people who died from an overdose in the United States, they included data from all three opioid use disorder categories. However, when estimating the impact of reducing the number of prescription opioids, they excluded data from the third one – opioid use disorder from illicit use without prior non-medical use of prescription opioids.
The researchers then ran 2 main statistical analyses. In their first analysis, they estimated the number of opioid overdose deaths averted by observed and future reductions in opioid prescribing. In their second analysis, they used a simulated cohort of individuals who initiated medical use of prescription opioids (i.e., taking as prescribed by a medical professional) to estimate the number of people who would go on to non-medical use of prescription opioids and, of those, the number that would develop prescription opioid use disorder and experience opioid overdose deaths.
WHAT DID THIS STUDY FIND?
There is a time lag between reductions in opioid prescriptions and decreases in opioid use disorder.
Between 2010 and 2019, the number of opioid prescriptions per 100 people decreased from 81.2 to 46.7, a reduction of 42.5%. This reduction coincided with a projected 8.5% increase in the number of active prescription opioid use disorder cases during the same time period.
Of the estimated 2.4 million individuals with an active opioid use disorder in 2019, 65% first used opioids for medical reasons prior to 2011. However, only 14% first used opioids for medical reasons between 2017 and 2019.
By 2029, it was projected that approximately 2.5 million people will have an active opioid use disorder, of whom 54% would have first used opioids for medical reasons prior to 2011, whereas 29% first used opioids for medical reasons between 2020 and 2029.
There is a time lag between reductions in opioid prescriptions and lives saved.
The 42.5% reduction in the rate of opioid prescriptions per 100 people between 2010 and 2019 coincided with a projected 103.2% increase in the number fatal opioid overdoses during the same time period.
Of the 78.3 million individuals who were first prescribed an opioid in 2011, 13,663 died from an opioid overdose (0.02%).
Of the projected 37,183 opioid overdose deaths that occurred in 2019 among those with non-medical use of prescription opioids, 64% first used opioids for medical reasons prior to 2011. However, only 17% occurred among people who first used opioids for medical reasons between 2017 and 2019.
By 2029, it was projected that 38,940 opioid overdose deaths will have occurred among people with non-medical use of prescription opioids, of whom 54% would have first used opioids for medical reasons prior to 2011, whereas 28% first used opioids between 2020 and 2029.
When compared to a hypothetical where the 2010 opioid prescription rate was maintained over time, reductions that occurred between 2010 and 2019 are estimated to have prevented 9600 opioid overdose deaths by 2019, and are projected to prevent another 50,918 deaths between 2020 and 2029. As such, only 18.9% of the impact of the prescription reductions was seen in the first decade (2010-2019) and the remaining 81% is projected in the second decade.
Several hypothetical prescription reduction scenarios further illustrated that larger reductions implemented earlier averted more opioid overdose deaths rather than smaller reductions implemented later.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study used computer modeling to show that reducing the number of prescription opioids saves lives and reduces cases of opioid use disorder, but with a time lag between opioid prescription reductions and downstream benefits. The largest public health benefits are not evident until the second decade of implementing the reductions.
The illustration of the lag period between prescription reductions and beneficial effects helps to resolve the discrepancy of opioid overdoses continuing to rise at unprecedented rates despite the reductions.
For instance, most of the cases of opioid use disorder and overdose deaths that occurred in 2019 were projected to have been among people who first used prescription opioids a decade or more earlier. The reductions were also projected to have already saved almost 10,000 lives and to have prevented more than 5 times as many overdose deaths in the next decade compared to a hypothetical where the number of prescriptions remained at 2010 levels. These delayed effects are similar to the lag observed between decreases in lung cancer cases and smoking cessation campaigns, since the decreases in lung cancer were not observed until decades after smoking rates began to decrease. This supports the policy change of prescription reductions.
Taken together, these results suggest that reducing the number of prescription opioids can have beneficial effects, but these effects take time to see. Accordingly, prescription reductions should be implemented as part of a larger, multi-level national public health strategy that includes expanding access to treatment,harm reduction,and recovery support services to have a more immediate impact on the opioid epidemic. Further, there are potential harms of reducing opioid medications for long-term pain patientsthat need to be considered, such that any reductions should be based on empirically-supported protocols and paired with linkages to substance use disorder treatment if needed.
Because the researchers used statistical modeling to predict results, the results should be viewed as projections rather than empirical observations. For instance, there is no direct data to determine the effect of any single intervention in isolation. Other outside factors that were not accounted for in the models could have affected the results. However, the data that were used to provide information to the models were based on the best available scientific data estimates.
The researchers programmed the models based on total opioid-related overdose deaths rather than opioid use disorder cases. Therefore, the estimates of the number of people with opioid use disorder may be underestimates since opioid use disorder cases that did not result in overdose deaths would have been missed. There are also limitations of the datasets used and changes in diagnostic criteria of opioid use disorder that may have further contributed to underestimates of opioid use disorder cases.
Since the researchers also programmed the models based on 2010 data, it is not possible to determine how effects prior to 2010 affected the results.
The model only accounted for potential secondary effects of some interventions. It was not possible to account for all of them. This may have resulted in an underestimation of the effects the prescription reductions have when implemented as part of a larger, comprehensive strategy to address the opioid epidemic.
The effects of other potential contributors to the discrepancy of opioid overdoses continuing to rise despite reductions in the number of opioid prescriptions, such as the rise of the use of illicit fentanyl, were not analyzed. Increases in fentanyl use have been associated with large increases in the number of overdose deaths.
BOTTOM LINE
Reducing the number of prescription opioids appears to have saved lives, prevented future deaths from opioid overdoses, and reduced opioid use disorder cases, although there is a decade-long time lag between the reductions and observed beneficial impacts. This suggests efforts to reduce opioid exposure by reducing opioid prescriptions enhances public health. However, given the paradoxical harms of reducing opioid prescriptions among certain population segments such as among pain patients, they should be used as part of other strategies to expand access to treatment and harm reduction services.
For individuals and families seeking recovery: Opioid prescription reductions can improve public health, but their beneficial effects take some time to be seen.In the meantime, individuals and families are encouraged to take advantage of currently available evidence-based treatments, such as medications and therapy. Individualscan also prevent opioid-related overdoses and other harms by engaging in harm reduction strategies, such as having ready availability of naloxone (Narcan) to reverse overdoses, and recovery services, such as peer support.
For treatment professionals and treatment systems: This prevention-focused study shows that public health benefits of opioid prescription reductions may take time to exert their most beneficial effects. In the meantime, there are risks to opioid prescription reductions that can be mitigatedby the use of empirically-supported tapering protocols and linkages to substance use disorder treatment (e.g., medications for opioid use disorder) and recovery supports.
For scientists:While the current study demonstrated the time lag between reductions in prescription opioids and lives saved, as well as reduced opioid use disorder cases, there are some limitations. If future research addressed these limitations, it could help to shed additional light on the impact of opioid prescription reductions. For instance, if scientists examined the effects of other treatment and harm reduction strategies for opioid use disorder not included in the current study, they could contribute to a greater understanding of how opioid prescription reductions impact opioid use disorder cases and overdose deaths. Further, additional research that uses data based on opioid use disorder cases rather than total overdose deaths to program statistical models could provide a more accurate estimate of the number of people with opioid use disorder.
For policy makers: Given the potential benefits of reducing the number of opioid prescriptions, continuing to support policies that limit opioid prescriptions could have important effects on lives saved from opioid overdoses and decreasing rates of opioid use disorder. Such policies, however, also need to consider the needs of certain population segments, such as people with chronic pain. Further, since there is a lag period between prescription reductions and beneficial impacts, support of policies that expand access to treatment and harm reduction services could have a more immediate impact on the opioid epidemic.