
Rolling the Dice! Brief Interventions for Problem Gambling in Substance Use Disorder Treatment
Up to 20% of those in substance use disorder treatment also have a problem with gambling.
This article compared three gambling treatments for individuals in two types of outpatient treatment programs – methadone maintenance and standard psychosocial treatment.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
For individuals with substance use disorder (SUD), it is not uncommon to struggle with other mental health and behavioral difficulties. Data from the Substance Abuse and Mental Health Services Administration (SAMHSA) shows:
- 33% of individuals admitted to addiction treatment also have another current psychiatric disorder. Gambling disorder is one particular co-occurring problem that has not been researched as often as psychiatric disorders like depression and anxiety.
- 23% of individuals who seek substance use disorder (SUD) treatment have gambling disorder or gambling that does not quite meet the threshold for diagnosis, but has a negative impact on someone’s life nevertheless, often called problem gambling.
This study by Nancy Petry and colleagues tested three brief interventions for individuals in substance use disorder (SUD) treatment that also had gambling problems. The findings provide important information for clinicians and treatment programs looking for evidence-based strategies to address gambling problems in their patients that are receiving help primarily for an substance use disorder.
HOW WAS THIS STUDY CONDUCTED?
Study authors randomly assigned individuals receiving outpatient treatment either at a methadone clinic (for patients with opioid use disorder) or a standard substance use disorder (SUD) treatment program (for individuals with a range of SUDs) to one of three interventions for gambling problems:
- Motivational Enhancement Therapy and Cognitive Behavioral Therapy (MET/CBT; n = 82), a 4-session intervention
- Brief Advice, a 10-15 minute intervention (n = 66)
- Brief Psychoeducation, a 10-15 minute intervention (n = 69)
It is worth noting they balanced the random assignment so that the groups were roughly equivalent in terms their gambling problem severity, the percent who were in methadone maintenance treatment, and the study therapist to which they were matched. They also weighted the random assignment toward MET/CBT, to account for anticipated drop-out from the 4-session intervention, leading to slightly more individuals in that group.
In terms of content in each group:
- Motivational Enhancement Therapy and Cognitive Behavioral Therapy (MET/CBT) included one session focused on patients’ motivation, such as rewards and consequences of gambling, as well as their life goals, and how gambling fit with those goals. This was followed by three sessions of CBT, focused on identifying the function of gambling (e.g., to cope with unpleasant feelings) and outlining other, healthier ways to meet those patient’s individual needs
- Brief Advice included education about how gambling problems are connected to SUD and mood difficulties, as well as four tips to curb their gambling problems (e.g., finding other fun activities to replace gambling)
- Brief Psycho-education included only the educational component; no advice to address the gambling problem was offered. To be considered for the study, patients had to have gambled on 4 or more days and at least $100 in the past 2 months, and needed to obtain a score of 4 or greater on a 20-item gambling screening assessment
Questions on this screening assessment, which was also used to measure gambling problem severity over time included, for example:
- When you gamble, how often do you go back another day to win back money you have lost? (Answers of “Most of the time I lose” or “Yes, most of the time” get 1 point)
- Did you ever gamble more than you intended to?
- Have you ever hidden betting slips, lottery tickets, gambling money, IOUs, or other signs of betting or gambling from your spouse, children, or other important people in your life?
- Have you ever borrowed from someone and not paid them back as a result of your gambling?
- Have you ever lost time from work (or school) due to betting money or gambling?
- GROUP SAMPLES
-
- Overall, groups entered the study having risked $240-300 in the past month, on average, and 84-88% met DSM-IV criteria for pathological gambling (the percentage range reflects percentages for the 3 groups).
- About one-third had a problem with purchasing scratch/instant lottery tickets, 18-29% with card games, 17-24% with traditional lottery tickets, and others with gambling problems related to sports wagers, slot machines, and other casino games.
- Very few had prior gambling treatment.
- Regarding substance use disorders (SUDs), patients most commonly met criteria for a cocaine use disorder (57-64%), alcohol use disorder (50-54%), opioid use disorder (39-46%), and marijuana use disorder (17-28%).
- The groups were similar at baseline (i.e., when entering the study), including their demographic characteristics (e.g., gender) and these key clinical characteristics.
Motivational Enhancement Therapy and Cognitive Behavioral Therapy (MET/CBT) was compared to Brief Advice, and Brief Advice was compared to Brief Psychoeducation on number of days gambled, dollar amount risked, and perceived severity of gambling problem during the past 30 days at several points in time over a 2 year period. Separate comparisons such as these are typical when authors have very specific hypotheses about how groups will perform against one another.
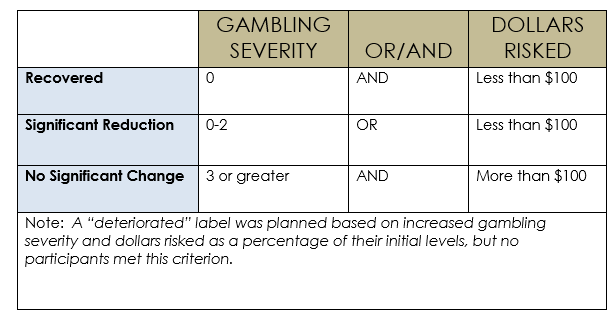
In this case, they anticipated the more intensive Motivational Enhancement Therapy and Cognitive Behavioral Therapy (MET/CBT) would outperform Brief Advice, which would outperform Brief Psychoeducation because the advice condition offered specific suggestions to address their gambling problem. Authors also categorized individuals with the labels below to make it easier to interpret improvement and apply study results to real-world behavior:
WHAT DID THIS STUDY FIND?
NOTABLY FROM THIS STUDY:
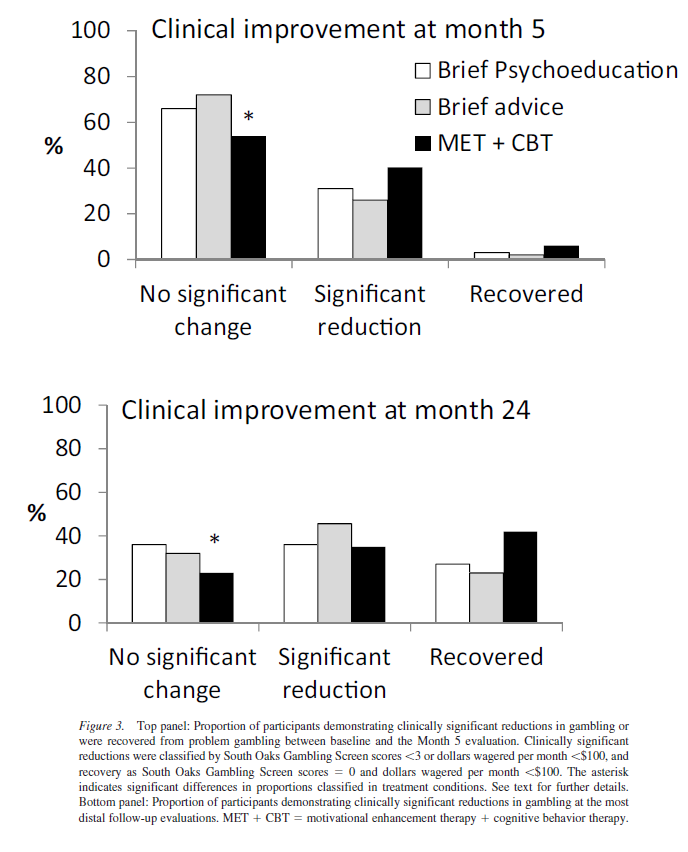
- Mostly in line with their expectations, by 5 months after beginning the study, Motivational Enhancement Therapy and Cognitive Behavioral Therapy (MET/CBT) patients did have greater reductions in money risked and gambling problem severity compared to Brief Advice patients, but they were not different on number of days gambled.
- They also had further reduction in money risked from the 5-month follow-up all the way through the 2-year follow-up.
- Counter to their expectations, Brief Advice patients had a greater reduction in the number of days they gambled, but were not different from the Brief Psychoeducation patients on money risked, and gambling problem severity at the 5-month follow-up. Groups also had similar reductions up through the 2-year follow-up.
- When comparing groups by the improvement categories (see table above), Motivational Enhancement Therapy and Cognitive Behavioral Therapy (MET/CBT) patients were more likely to be improved than Brief Advice patients both at the 5-month and the 2-year follow-ups. Brief Advice and Brief Psychoeducation patients were equally likely to show improvement.
It is important to note, here, that the word “significant” is not used like “statistically significant”, as is often the case in other research studies.
Overall, the study results demonstrate that the more intensive Motivational Enhancement Therapy and Cognitive Behavioral Therapy (MET/CBT) patients had the best gambling outcomes both short-term and long-term, and the two less intensive, 10-15 minute conditions were mostly similar to one another.
Although study authors were not targeting patients’ substance use disorder (SUD) with the gambling interventions, it is important to see whether the gambling interventions had differential effects on substance use. The Motivational Enhancement Therapy and Cognitive Behavioral Therapy (MET/CBT) patients had improved drinking, but not other drug use at the 5-month follow-up, and this advantage disappeared by the 2-year follow-up. One last note that we will discuss more below is that nearly 40% of MET/CBT patients did not go to any Cognitive Behavioral Therapy (CBT) sessions whatsoever, and only 28% completed all three.
WHY IS THIS STUDY IMPORTANT
This study is important for two major reasons:
-
First, it shows that for individuals in substance use disorder (SUD) treatment with gambling problems, they are likely to reduce their gambling over time. By the end of the study (2 year follow-up), all three groups, on average, were risking very small amounts each month ($1-3).
-
Second, it shows that a targeted intervention with tried-and-true motivational and cognitive-behavioral strategies promotes greater improvements that are sustained over time.
- LIMITATIONS
-
- Study authors did not measure gambling and substance use outcomes in a group receiving no gambling intervention (i.e., only substance use disorder (SUD) treatment). Therefore it is unclear whether the Brief Psychoeducation condition is better than doing nothing at all. That said a 10-15 minute intervention is very minimal. Given that the Motivational Enhancement Therapy and Cognitive Behavioral Therapy (MET/CBT) group had substance use outcomes as good as, or better than, the Brief Advice and Brief Psychoeducation conditions, it is unlikely that receiving a gambling disorder intervention will negatively affect substance use outcomes.
- Also, as the study authors pointed out, the MET/CBT condition, was four sessions long as opposed to one session each for the comparison conditions. Based just on this study, then, it is unclear whether the better outcomes related to MET/CBT are due to greater therapeutic contact or something inherent in the specifics of the MET/CBT intervention.
- NEXT STEPS
-
Since the study was conducted in two programs in one region of the country, it would be helpful to see if Motivational Enhancement Therapy and Cognitive Behavioral Therapy (MET/CBT) is an effective intervention in other types of treatment programs located in other areas. In addition, it might be important to determine if the intervention works equally well for individuals with different primary gambling problems. This type of investigation could be particularly important because while different forms of gambling could produce similar feelings of reward, gambling behaviors that may necessarily occur in particular settings (e.g., casinos) could lead to stronger pairing with alcohol and other drug use.
In other words, it could be that both the feelings produced by the gambling behavior – playing a card game like “blackjack” for example – as well as the setting where the gambling behavior occurs – the casino – are triggers for alcohol and other drug use, and vice versa. In this way, gambling treatment for individuals whose gambling problem manifests in gambling-specific settings like casinos would be even more beneficial than for individuals whose problem does not necessarily depend on a particular setting (e.g., those who buy scratch off tickets).
Next, it will be important to test Motivational Enhancement Therapy and Cognitive Behavioral Therapy (MET/CBT)in some other research designs to increase confidence in its true effectiveness. For example, nearly 40% of individuals did not go to any of the three Cognitive Behavioral Therapy (CBT) sessions whatsoever. It could be that a single motivational enhancement session is sufficient to help. Study authors suggest that those with more severe problems may require the CBT sessions and those with less severe problems may only need the motivational session. This is certainly a possibility and can be tested in future studies.
Finally, it will be important to determine if the Motivational Enhancement Therapy and Cognitive Behavioral Therapy (MET/CBT) is helpful due to the specific therapeutic “ingredients” in the intervention (the motivational and cognitive-behavioral strategies), or simply because of the benefits of spending four sessions with a therapist. The non-specific benefits from spending time with a therapist (e.g., feeling listened to and accepted) has been shown to explain as much as, if not more, of the improvement patients experience when receiving treatments for substance use disorder compared to the therapeutic techniques themselves.
BOTTOM LINE
- For individuals & families seeking recovery: More than 20% of people who enroll in substance use disorder treatment also have a gambling problem. This study shows that there are helpful gambling treatments that can be added to substance use disorder treatment. A treatment that combines motivational and cognitive-behavioral approaches to target the gambling problem is likely to provide the most help, the quickest. At this point, however, the research testing the addition of gambling problem interventions is in early stages, and it is not clear how many treatment programs actually offer such interventions.
- For Scientists: This rigorous randomized controlled trial provides an excellent model for testing treatments for additional problems like gambling disorder, that may co-occur with substance use disorder. One interesting piece of the results is that nearly 40% of Motivational Enhancement Therapy and Cognitive Behavioral Therapy (MET/CBT) patients did not go to any Cognitive Behavioral Therapy (CBT) sessions whatsoever, and only 28% completed all three. To maximize resources allocated to gambling treatments, in light of limited treatment resources, it will be important to design studies that determine the relative contributions of the motivational versus the cognitive-behavioral components. In addition, because MET/CBT was four sessions compared to one, future work should compare MET/CBT to a non-MET/CBT treatment (e.g., brief advice plus psychoeducation) that lasts four sessions. This will help disentangle specific effects due to the treatment “ingredients” for gambling problems vs. non-specific effects from talk therapy more generally (i.e., “common factors”).
- For Policy makers: Policies that help fund a) ongoing research related to problem gambling among individuals with substance use disorder, and b) implementation and evaluation of motivational enhancement/cognitive behavioral therapy for gambling problems in substance use disorder treatment settings could help address the multitude of problems faced by individuals in addiction treatment.
- For Treatment professionals and treatment systems: This study shows that a four-session treatment combining motivational and cognitive-behavioral approaches is helpful for individuals with gambling problems in substance use disorder treatment. While more research needs to be done on the cost-effectiveness of such treatments, if adequate resources are available, consider delivering the motivational/cognitive behavioral treatment as appropriate.
CITATIONS
Petry, N. M., Rash, C. J., & Alessi, S. M. (2016). A Randomized Controlled Trial of Brief Interventions for Problem Gambling in Substance Abuse Treatment Patients. Journal of Consulting and Clinical Psychology, Vol 84(10), Oct 2016, 874-886.
