Simulating the impact of overdose prevention strategies
Research suggests overdose prevention strategies are cost-effective, though their real-world benefits may depend on where exactly they are implemented. This study used computer-intensive “machine-learning” models to evaluate the effects of individual and combined overdose-death prevention strategies on overdose death rates among individuals with opioid use disorder in the U.S. state of Connecticut.
Overdose death rates continue to be high throughout the United States. Of the 107,543 drug overdoses that were estimated to occur in 2023, 75% involved opioids. Preliminary data suggests downward trends in drug overdose death rates for the first time since 2018. Though more data are needed to determine whether this encouraging data point is indeed a trend, and to what degree some of these benefits may be due to harm reduction strategies, more work is needed to understand which strategies are best, in which contexts, and at what cost.
Distribution of the opioid overdose-reversal medication naloxone is a cost-effective strategy for overdose death prevention and prior research suggests scaling it up with more precision (i.e., in overdose “hotspots”) in the community might help to further reduce overdose death rates, warranting additional research. Medication treatments for opioid use disorder (buprenorphine, methadone, naltrexone) are also extremely useful in preventing overdose, and thus, also preventing death. Individuals with opioid use disorder are at increased risk of overdose and medication treatment can help reduce that risk. While studies have modeled the cost effectiveness of these overdose death prevention strategies, it is unclear to what extent stakeholders should be investing in each of these strategies and their combinations to maximally benefit individuals with opioid use disorder and decrease overdose death rates.
Determining the effects of these strategies on overdose death rates is essential to inform policy efforts in specific areas of the US that more adequately address overdose deaths and better tackle the opioid epidemic. This study used machine-learning models to evaluate individual and combined overdose-death prevention strategies on overdose death rates in the state of Connecticut, which has one of the highest overdose rates in the US.
HOW WAS THIS STUDY CONDUCTED?
This study used a machine-learning model to estimate the effects of overdose prevention strategies on overdose death rates in the state of Connecticut. One-hundred thousand simulated cases representative of the Connecticut population with opioid use disorder were included in the analysis.
Prevention strategies modeled included increasing distribution/access to (1) naloxone in the general community, (2) medication treatments for opioid use disorder among people in the general community, (3) medication treatments among people who are incarcerated. The researchers examined the 5-year impact of each policy, individually and in combination, on life expectancy, years with good quality health (called quality-adjusted life years, or QALYs – pronounced “quallies’), percentage/number of opioid overdose deaths prevented over a 5-year period and over the simulated cohort’s lifetime. Cost-effectiveness of each policy was also evaluated. Medication treatment included 4 medication types: (1) methadone, (2) oral buprenorphine (active ingredient in the brand-name medication Suboxone), (3) injectable extended-release buprenorphine (sometimes referred to by the brand name Sublocade), (4) injectable extended-release naltrexone (sometimes referred to by the brand name Vivitrol). Transitions on/off these medications were modeled using data that were medication specific.
Values entered into the model were based on data from studies in the scientific literature, expert opinion, and community organizations. As part of the virtual lifecycle, each simulated individual could transition between incarceration and the community and could fluctuate in their opioid use disorder status and treatment status. They could also experience a fatal or non-fatal overdose, and/or die from other causes. The researchers took sex, age, opioid use disorder status (current vs. remission), incarceration status, medication treatment status, and injection behaviors into consideration in their simulated models. Individuals in the model who received medication treatment during incarceration were all assumed to be in remission. Upon release from incarceration, modeled individuals could transition between 3 conditions: 1) receiving medication treatment (in remission and not in remission), 2) not receiving medication treatment and not in remission (assumed actively using illicit opioids), 3) not receiving medication treatment and in remission (assumed abstinent from illicit opioids). It was assumed that models with greater availability of medication treatment would result in greater prevalence of MOUD use among the simulated cohort. Fatal and non-fatal overdoses were possible among simulated individuals who used illicit opioids, with or without medication treatment. The model also assumed that increased naltrexone distribution in the community did not affect overdose rates but did reduce the risk of overdose deaths. Simulated individuals were able to shift between incarceration and the community and could have died from causes un-related to opioids in both environments.
To assess cost-effectiveness of different policies, the authors calculated incremental cost-effectiveness ratio – which is the change in cost of implementing a given policy, divided by the increase in beneficial outcomes from that policy (increase is relative to the next best policy), analyzed as costs per quality-adjusted life years. Costs were assessed from a healthcare perspective and from a societal perspective, and included costs associated with: (1) medication treatment; (2) naloxone; (3) community-based overdose services (e.g., emergency department); (4) incarceration and healthcare costs from a public-payor perspective; (5) crime and loss of productivity from incarceration and lack of treatment, from a societal perspective.
To study the effects of policy combinations, 3 scenarios were tested: (1) maximizing medication treatment during incarceration: all incarcerated people with opioid use disorder receive medication treatment regardless of whether or not they received it before incarceration; (2) maximizing medication treatment in the community: nearly all people with opioid use disorder in the general community (80%) receive medication treatment; (3) maximizing naloxone in the community: all individuals with opioid use disorder in the general community receive naloxone kits a minimum of once per year.
At the start of the study, the simulated sample was made up of adults (age 20 and older), with 14% previously incarcerated and 31% having a past overdose experience. About 4% of the simulated cohort had engaged in injection drug use.
WHAT DID THIS STUDY FIND?
Without a change, over 4,000 overdose deaths would occur every 5 years
If overdose prevention strategies in Connecticut were held constant at their current level, individuals in the simulated cohort would live an average of 33 additional years, with an accumulation of 26 quality-adjusted life years. Overdose deaths would occur at a rate of 4711 deaths over 5 years and 11,655 deaths during the entire study cohort’s lifetime.
Maximizing naloxone distribution would reduce overdose deaths by 20%
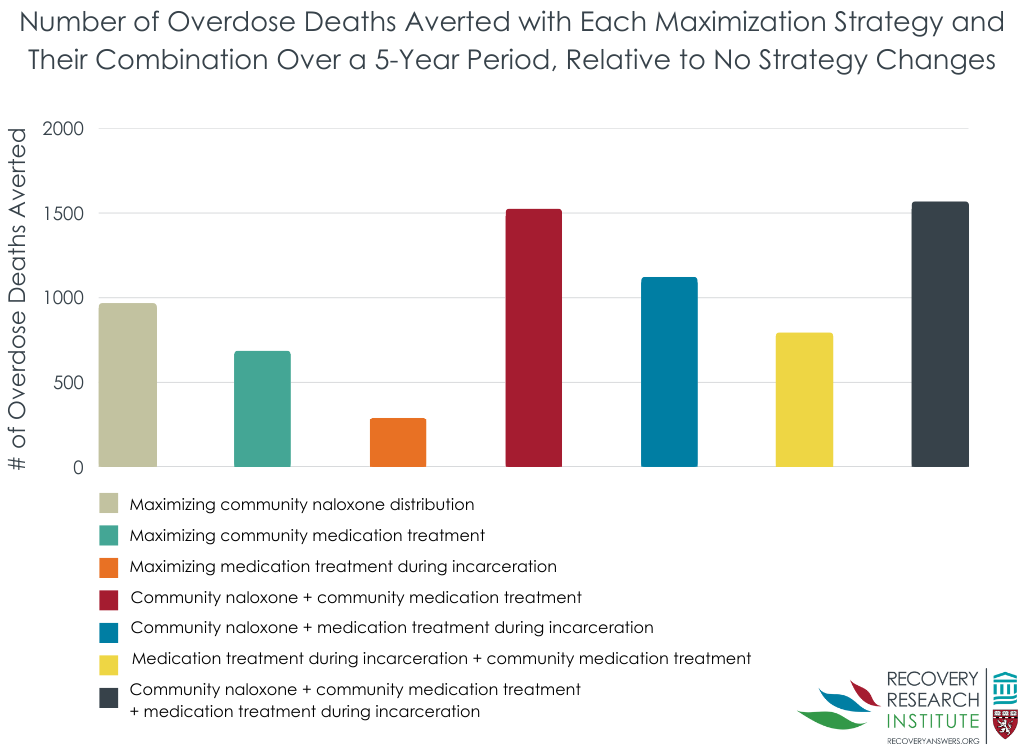
Distributing naloxone to all individuals with opioid use disorder at least once per year would reduce overdose death rates to 3744 deaths over 5 years (see Figure below). The simulated cohort would live an additional 0.4 life years, and 0.3 quality adjusted life years, over and above the years gained with no policy changes. The cost of maximizing naloxone distribution, taking the policy’s benefits into account, would be an additional $9000 spent per each quality adjusted life year gained.
Maximizing medication provision would reduce overdose deaths by about 10%
Providing medication treatment to nearly all people with opioid use disorder in the general community would reduce overdose death rates to 4029 deaths over 5 years (see Figure below). If all incarcerated people with opioid use disorder received medication treatment, overdose death rates would reduce to 4439 deaths over 5 years. The simulated community cohort would live an additional 1.5 life years (1.8 quality adjusted life years), and the incarcerated cohort would live an additional 0.2 life years (0.2 quality adjusted life years), over and above the years gained with no policy changes. The cost of maximizing medication treatment access in the community and during incarceration would be an additional $19,000 and $37,000 per quality adjusted life year, respectively.
Combining naloxone and medication treatment strategies was the most cost-effective option
Combining maximization strategies for community-based naloxone distribution and community-based medication treatment provision emerged as the best model when focusing on healthcare costs (see Figure below). This model would reduce overdose deaths by 32% (to 3193 deaths over 5 years). The simulated cohort would live an additional 1.8 life years (2.0 quality adjusted life years) over and above the years gained with no policy changes and would cost an additional $19,000 per each quality adjusted life year gained. From a societal perspective, this model saved society $333,000 per capita. Sensitivity analyses also suggested that this would be a cost-effective model even when varying important factors in the model (e.g., prior overdose or incarceration rates).
Combining all 3 maximization strategies (including incarceration-based medication treatment) resulted in 33% reduction of overdose death rates. This strategy was not considered as cost effective from the healthcare perspective (costing about $75,000 more than combining community strategies without incarceration strategies), but it was considered the best model when cost was assessed from a societal perspective, saving society $338,000 per capita.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help inform policies and strategies to address opioid overdose epidemic. This study, which focused on “best case scenario” strategies in the state of Connecticut, suggests that expanding and maximizing access to community-based medication treatment and naloxone distribution could prevent a third of overdose deaths over a 5-year period, and could result in 2 additional years of life expectancy per person. Such efforts would be cost effective from a healthcare perspective, costing only an additional $19,000 per adjusted life years gained, and from a societal perspective, saving society over $300,000 per capita in increased productivity and reduced crime.
One unsurprising but important note mentioned by the research team was that reduced death rates were largest among persons who inject drugs, highlighting the potential benefits of targeted naloxone distribution for individuals at increased risk of overdose, such as distribution through harm reduction programs. Nonetheless, few states have naloxone access that is broad enough to adequately achieve overdose death prevention. Additional investigation into the best venues for targeted and broad distribution of naloxone will help inform expanded access efforts.
Though the provision of medication treatment during incarceration reduced overdose deaths by 6% when assessed on its own, adding this strategy to those aimed at maximizing community medication treatment and naloxone provision did not substantially increase the overdose death rate (32% vs. 33%) and cost the healthcare system significantly more money. Yet, from a societal perspective the combination of all three strategies yielded the greatest cost savings, saving money through the prevention of crime and increased productivity. Developing and testing novel models of medication treatment for incarcerated individuals may be warranted to identify ways to reduce associated healthcare-related costs while maintaining high rates of overdose prevention. While this study only examined combinations of naloxone and medication treatment, future work may follow the lead of other computer-simulated studies that test even more combinations of strategies, including for example, recovery support services and fentanyl test strips.
Interestingly, maximizing the provision of naloxone alone was more effective at reducing overdose deaths than maximizing the provision of medication treatment alone. Though this may seem counterintuitive to what we hear about the benefits of medication treatment, it is important to remember that medication treatment can help reduce overdose risk but the most commonly used medication treatments like buprenorphine and methadone do not entirely prevent overdose and cannot reverse an overdose. To reverse an overdose, naloxone, the opioid overdose reversal drug, is needed. Still, studies examining patient-level effects of medication treatment provision suggest that medication treatment reduces drug-related deaths by ~60%. The reasons for discrepant findings here likely have to do with the methods (simulated models vs. patient data) and the focus of the studies, with this study focusing on population-level effects as opposed to patient-level effects. Other simulated research focused on population-level outcomes have found similar results, with naloxone emerging as the most effective strategy for overdose death prevention. Yet, findings are mixed, likely due to the various assumptions that go into a given simulated model. Real world data focusing on both individual and population level effects of overdose-death prevention strategies will help to clarify their individual and combined effects under different circumstances and with different sub-populations.
That said, additional research is needed to better understand the relationship between access to these strategies and uptake or use of these strategies among populations with opioid use disorder. If few people are willing to take medication treatment or carry naloxone, then efforts to expand access to these lifesaving strategies will not be maximally effective. Indeed, up to 87% of people with opioid use disorder in the US who would benefit from medication treatment do not receive it. Though barriers to treatment access (limited provider availability, financial & logistical barriers) contribute to inadequate treatment uptake, negative perceptions of medication treatment can also influence willingness to start medication treatment. Therefore, additional research examining attitudes toward medication treatment and initiatives to combat the influence of stigma on medication treatment will further inform efforts to address the opioid epidemic.
This study used a simulated model to estimate the outcomes of potential efforts to expand opioid use disorder treatment and overdose resources, warranting additional real-world research.
Maximal provision assumes that everyone in the model received the treatment or naloxone kit. This requires additional research, as a number of people may decline intervention efforts, including naloxone and medication treatment.
This study used model parameters that reflect a time when higher potency opioids like fentanyl and their use with sedatives like xylazine were not common, which might mute the theoretical benefits on overdose outcomes observed here.
The study only examined combinations of naloxone and medication treatment. Other computer-simulated studies like this one that included other approaches, such as recovery support services and fentanyl test strips, have shown these strategies to be life-saving as well.
BOTTOM LINE
Results from this Connecticut-based study show one-third of overdose deaths can be prevented by providing community-based medication treatment and naloxone distribution to nearly all individuals with opioid use disorder. Combined provision of these “best case scenario” strategies was cost effective from both healthcare and societal perspectives.
For individuals and families seeking recovery: Medication treatments for opioid use disorder and naloxone help prevent and reverse opioid overdose, and these often lifesaving medications are a good option for people who are looking to support their treatment and recovery goals. Individuals and families interested in these strategies are encouraged to speak with their healthcare providers about their treatment options to learn if these medications are right for them. Many states also now sell naloxone over the counter.
For treatment professionals and treatment systems: This study helps us better understand the influence of various policies/strategies for reducing opioid overdose deaths, which could ultimately help inform best methods for adequately addressing the opioid epidemic. Findings highlight the potential for the widespread community provision of opioid use disorder medication treatments and naloxone to prevent up to one-third of overdose deaths among individuals with opioid use disorder. Given the benefits and cost effectiveness of providing these services, providers are encouraged to provide naloxone to all patients with opioid use disorder and to consider increased provision of medication treatments like buprenorphine and extended-release naltrexone to better address the opioid overdose epidemic.
For scientists: Additional research is needed to examine the real-world longitudinal effects of medication treatment and naloxone provision, both in the community and among incarcerated individuals, on overdose death rates throughout different regions and patient populations in the US. Studies examining treatment attitudes, patient preferences, and barriers to treatment (e.g., financial, geographic) are needed to determine the influence of these factors on overdose, as well as other outcomes like recovery capital and quality of life. The influence of maximizing access to different types of medication treatments is also needed to identify potential differences in the impact of the breadth of treatment, recovery, and harm reduction services on community and individual patient outcomes. Future studies should also examine the influence of overdose and service-use histories, patient motivation for treatment/recovery, and additional treatment (public vs. private) and patient-level factors (e.g., change in mental/physical health symptoms) on study outcomes.
For policy makers: Studies like this help inform policies and strategies aimed at overcoming the opioid overdose epidemic. Leveraging existing strategies like the provision of medication treatment (e.g., buprenorphine) and naloxone, and scaling up the availability of these lifesaving medications in the community is likely to help prevent a substantial number of overdose deaths in a cost-effective and even cost-saving manner. Given that this study was a simulated study using a machine-learning model, additional funds are needed to study the direct real-world effects of expanding medication treatment and naloxone provision on overdose death risk and prevalence, accounting for patient, treatment, and community level factors not assessed in the current study.
CITATIONS
Scheidell, J. D., Townsend, T. N., Zhou, Q., Manandhar-Sasaki, P., Rodriguez-Santana, R., Jenkins, M., Buchelli, M., Charles, D. L., Frechette, J. M., I-Shin Su, J., & Braithwaite, R. S. (2024). Reducing overdose deaths among persons with opioid use disorder in Connecticut.Harm Reduction Journal, 21(103). doi: 10.1186/s12954-024-01026-6.
Overdose death rates continue to be high throughout the United States. Of the 107,543 drug overdoses that were estimated to occur in 2023, 75% involved opioids. Preliminary data suggests downward trends in drug overdose death rates for the first time since 2018. Though more data are needed to determine whether this encouraging data point is indeed a trend, and to what degree some of these benefits may be due to harm reduction strategies, more work is needed to understand which strategies are best, in which contexts, and at what cost.
Distribution of the opioid overdose-reversal medication naloxone is a cost-effective strategy for overdose death prevention and prior research suggests scaling it up with more precision (i.e., in overdose “hotspots”) in the community might help to further reduce overdose death rates, warranting additional research. Medication treatments for opioid use disorder (buprenorphine, methadone, naltrexone) are also extremely useful in preventing overdose, and thus, also preventing death. Individuals with opioid use disorder are at increased risk of overdose and medication treatment can help reduce that risk. While studies have modeled the cost effectiveness of these overdose death prevention strategies, it is unclear to what extent stakeholders should be investing in each of these strategies and their combinations to maximally benefit individuals with opioid use disorder and decrease overdose death rates.
Determining the effects of these strategies on overdose death rates is essential to inform policy efforts in specific areas of the US that more adequately address overdose deaths and better tackle the opioid epidemic. This study used machine-learning models to evaluate individual and combined overdose-death prevention strategies on overdose death rates in the state of Connecticut, which has one of the highest overdose rates in the US.
HOW WAS THIS STUDY CONDUCTED?
This study used a machine-learning model to estimate the effects of overdose prevention strategies on overdose death rates in the state of Connecticut. One-hundred thousand simulated cases representative of the Connecticut population with opioid use disorder were included in the analysis.
Prevention strategies modeled included increasing distribution/access to (1) naloxone in the general community, (2) medication treatments for opioid use disorder among people in the general community, (3) medication treatments among people who are incarcerated. The researchers examined the 5-year impact of each policy, individually and in combination, on life expectancy, years with good quality health (called quality-adjusted life years, or QALYs – pronounced “quallies’), percentage/number of opioid overdose deaths prevented over a 5-year period and over the simulated cohort’s lifetime. Cost-effectiveness of each policy was also evaluated. Medication treatment included 4 medication types: (1) methadone, (2) oral buprenorphine (active ingredient in the brand-name medication Suboxone), (3) injectable extended-release buprenorphine (sometimes referred to by the brand name Sublocade), (4) injectable extended-release naltrexone (sometimes referred to by the brand name Vivitrol). Transitions on/off these medications were modeled using data that were medication specific.
Values entered into the model were based on data from studies in the scientific literature, expert opinion, and community organizations. As part of the virtual lifecycle, each simulated individual could transition between incarceration and the community and could fluctuate in their opioid use disorder status and treatment status. They could also experience a fatal or non-fatal overdose, and/or die from other causes. The researchers took sex, age, opioid use disorder status (current vs. remission), incarceration status, medication treatment status, and injection behaviors into consideration in their simulated models. Individuals in the model who received medication treatment during incarceration were all assumed to be in remission. Upon release from incarceration, modeled individuals could transition between 3 conditions: 1) receiving medication treatment (in remission and not in remission), 2) not receiving medication treatment and not in remission (assumed actively using illicit opioids), 3) not receiving medication treatment and in remission (assumed abstinent from illicit opioids). It was assumed that models with greater availability of medication treatment would result in greater prevalence of MOUD use among the simulated cohort. Fatal and non-fatal overdoses were possible among simulated individuals who used illicit opioids, with or without medication treatment. The model also assumed that increased naltrexone distribution in the community did not affect overdose rates but did reduce the risk of overdose deaths. Simulated individuals were able to shift between incarceration and the community and could have died from causes un-related to opioids in both environments.
To assess cost-effectiveness of different policies, the authors calculated incremental cost-effectiveness ratio – which is the change in cost of implementing a given policy, divided by the increase in beneficial outcomes from that policy (increase is relative to the next best policy), analyzed as costs per quality-adjusted life years. Costs were assessed from a healthcare perspective and from a societal perspective, and included costs associated with: (1) medication treatment; (2) naloxone; (3) community-based overdose services (e.g., emergency department); (4) incarceration and healthcare costs from a public-payor perspective; (5) crime and loss of productivity from incarceration and lack of treatment, from a societal perspective.
To study the effects of policy combinations, 3 scenarios were tested: (1) maximizing medication treatment during incarceration: all incarcerated people with opioid use disorder receive medication treatment regardless of whether or not they received it before incarceration; (2) maximizing medication treatment in the community: nearly all people with opioid use disorder in the general community (80%) receive medication treatment; (3) maximizing naloxone in the community: all individuals with opioid use disorder in the general community receive naloxone kits a minimum of once per year.
At the start of the study, the simulated sample was made up of adults (age 20 and older), with 14% previously incarcerated and 31% having a past overdose experience. About 4% of the simulated cohort had engaged in injection drug use.
WHAT DID THIS STUDY FIND?
Without a change, over 4,000 overdose deaths would occur every 5 years
If overdose prevention strategies in Connecticut were held constant at their current level, individuals in the simulated cohort would live an average of 33 additional years, with an accumulation of 26 quality-adjusted life years. Overdose deaths would occur at a rate of 4711 deaths over 5 years and 11,655 deaths during the entire study cohort’s lifetime.
Maximizing naloxone distribution would reduce overdose deaths by 20%
Distributing naloxone to all individuals with opioid use disorder at least once per year would reduce overdose death rates to 3744 deaths over 5 years (see Figure below). The simulated cohort would live an additional 0.4 life years, and 0.3 quality adjusted life years, over and above the years gained with no policy changes. The cost of maximizing naloxone distribution, taking the policy’s benefits into account, would be an additional $9000 spent per each quality adjusted life year gained.
Maximizing medication provision would reduce overdose deaths by about 10%
Providing medication treatment to nearly all people with opioid use disorder in the general community would reduce overdose death rates to 4029 deaths over 5 years (see Figure below). If all incarcerated people with opioid use disorder received medication treatment, overdose death rates would reduce to 4439 deaths over 5 years. The simulated community cohort would live an additional 1.5 life years (1.8 quality adjusted life years), and the incarcerated cohort would live an additional 0.2 life years (0.2 quality adjusted life years), over and above the years gained with no policy changes. The cost of maximizing medication treatment access in the community and during incarceration would be an additional $19,000 and $37,000 per quality adjusted life year, respectively.
Combining naloxone and medication treatment strategies was the most cost-effective option
Combining maximization strategies for community-based naloxone distribution and community-based medication treatment provision emerged as the best model when focusing on healthcare costs (see Figure below). This model would reduce overdose deaths by 32% (to 3193 deaths over 5 years). The simulated cohort would live an additional 1.8 life years (2.0 quality adjusted life years) over and above the years gained with no policy changes and would cost an additional $19,000 per each quality adjusted life year gained. From a societal perspective, this model saved society $333,000 per capita. Sensitivity analyses also suggested that this would be a cost-effective model even when varying important factors in the model (e.g., prior overdose or incarceration rates).
Combining all 3 maximization strategies (including incarceration-based medication treatment) resulted in 33% reduction of overdose death rates. This strategy was not considered as cost effective from the healthcare perspective (costing about $75,000 more than combining community strategies without incarceration strategies), but it was considered the best model when cost was assessed from a societal perspective, saving society $338,000 per capita.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help inform policies and strategies to address opioid overdose epidemic. This study, which focused on “best case scenario” strategies in the state of Connecticut, suggests that expanding and maximizing access to community-based medication treatment and naloxone distribution could prevent a third of overdose deaths over a 5-year period, and could result in 2 additional years of life expectancy per person. Such efforts would be cost effective from a healthcare perspective, costing only an additional $19,000 per adjusted life years gained, and from a societal perspective, saving society over $300,000 per capita in increased productivity and reduced crime.
One unsurprising but important note mentioned by the research team was that reduced death rates were largest among persons who inject drugs, highlighting the potential benefits of targeted naloxone distribution for individuals at increased risk of overdose, such as distribution through harm reduction programs. Nonetheless, few states have naloxone access that is broad enough to adequately achieve overdose death prevention. Additional investigation into the best venues for targeted and broad distribution of naloxone will help inform expanded access efforts.
Though the provision of medication treatment during incarceration reduced overdose deaths by 6% when assessed on its own, adding this strategy to those aimed at maximizing community medication treatment and naloxone provision did not substantially increase the overdose death rate (32% vs. 33%) and cost the healthcare system significantly more money. Yet, from a societal perspective the combination of all three strategies yielded the greatest cost savings, saving money through the prevention of crime and increased productivity. Developing and testing novel models of medication treatment for incarcerated individuals may be warranted to identify ways to reduce associated healthcare-related costs while maintaining high rates of overdose prevention. While this study only examined combinations of naloxone and medication treatment, future work may follow the lead of other computer-simulated studies that test even more combinations of strategies, including for example, recovery support services and fentanyl test strips.
Interestingly, maximizing the provision of naloxone alone was more effective at reducing overdose deaths than maximizing the provision of medication treatment alone. Though this may seem counterintuitive to what we hear about the benefits of medication treatment, it is important to remember that medication treatment can help reduce overdose risk but the most commonly used medication treatments like buprenorphine and methadone do not entirely prevent overdose and cannot reverse an overdose. To reverse an overdose, naloxone, the opioid overdose reversal drug, is needed. Still, studies examining patient-level effects of medication treatment provision suggest that medication treatment reduces drug-related deaths by ~60%. The reasons for discrepant findings here likely have to do with the methods (simulated models vs. patient data) and the focus of the studies, with this study focusing on population-level effects as opposed to patient-level effects. Other simulated research focused on population-level outcomes have found similar results, with naloxone emerging as the most effective strategy for overdose death prevention. Yet, findings are mixed, likely due to the various assumptions that go into a given simulated model. Real world data focusing on both individual and population level effects of overdose-death prevention strategies will help to clarify their individual and combined effects under different circumstances and with different sub-populations.
That said, additional research is needed to better understand the relationship between access to these strategies and uptake or use of these strategies among populations with opioid use disorder. If few people are willing to take medication treatment or carry naloxone, then efforts to expand access to these lifesaving strategies will not be maximally effective. Indeed, up to 87% of people with opioid use disorder in the US who would benefit from medication treatment do not receive it. Though barriers to treatment access (limited provider availability, financial & logistical barriers) contribute to inadequate treatment uptake, negative perceptions of medication treatment can also influence willingness to start medication treatment. Therefore, additional research examining attitudes toward medication treatment and initiatives to combat the influence of stigma on medication treatment will further inform efforts to address the opioid epidemic.
This study used a simulated model to estimate the outcomes of potential efforts to expand opioid use disorder treatment and overdose resources, warranting additional real-world research.
Maximal provision assumes that everyone in the model received the treatment or naloxone kit. This requires additional research, as a number of people may decline intervention efforts, including naloxone and medication treatment.
This study used model parameters that reflect a time when higher potency opioids like fentanyl and their use with sedatives like xylazine were not common, which might mute the theoretical benefits on overdose outcomes observed here.
The study only examined combinations of naloxone and medication treatment. Other computer-simulated studies like this one that included other approaches, such as recovery support services and fentanyl test strips, have shown these strategies to be life-saving as well.
BOTTOM LINE
Results from this Connecticut-based study show one-third of overdose deaths can be prevented by providing community-based medication treatment and naloxone distribution to nearly all individuals with opioid use disorder. Combined provision of these “best case scenario” strategies was cost effective from both healthcare and societal perspectives.
For individuals and families seeking recovery: Medication treatments for opioid use disorder and naloxone help prevent and reverse opioid overdose, and these often lifesaving medications are a good option for people who are looking to support their treatment and recovery goals. Individuals and families interested in these strategies are encouraged to speak with their healthcare providers about their treatment options to learn if these medications are right for them. Many states also now sell naloxone over the counter.
For treatment professionals and treatment systems: This study helps us better understand the influence of various policies/strategies for reducing opioid overdose deaths, which could ultimately help inform best methods for adequately addressing the opioid epidemic. Findings highlight the potential for the widespread community provision of opioid use disorder medication treatments and naloxone to prevent up to one-third of overdose deaths among individuals with opioid use disorder. Given the benefits and cost effectiveness of providing these services, providers are encouraged to provide naloxone to all patients with opioid use disorder and to consider increased provision of medication treatments like buprenorphine and extended-release naltrexone to better address the opioid overdose epidemic.
For scientists: Additional research is needed to examine the real-world longitudinal effects of medication treatment and naloxone provision, both in the community and among incarcerated individuals, on overdose death rates throughout different regions and patient populations in the US. Studies examining treatment attitudes, patient preferences, and barriers to treatment (e.g., financial, geographic) are needed to determine the influence of these factors on overdose, as well as other outcomes like recovery capital and quality of life. The influence of maximizing access to different types of medication treatments is also needed to identify potential differences in the impact of the breadth of treatment, recovery, and harm reduction services on community and individual patient outcomes. Future studies should also examine the influence of overdose and service-use histories, patient motivation for treatment/recovery, and additional treatment (public vs. private) and patient-level factors (e.g., change in mental/physical health symptoms) on study outcomes.
For policy makers: Studies like this help inform policies and strategies aimed at overcoming the opioid overdose epidemic. Leveraging existing strategies like the provision of medication treatment (e.g., buprenorphine) and naloxone, and scaling up the availability of these lifesaving medications in the community is likely to help prevent a substantial number of overdose deaths in a cost-effective and even cost-saving manner. Given that this study was a simulated study using a machine-learning model, additional funds are needed to study the direct real-world effects of expanding medication treatment and naloxone provision on overdose death risk and prevalence, accounting for patient, treatment, and community level factors not assessed in the current study.
CITATIONS
Scheidell, J. D., Townsend, T. N., Zhou, Q., Manandhar-Sasaki, P., Rodriguez-Santana, R., Jenkins, M., Buchelli, M., Charles, D. L., Frechette, J. M., I-Shin Su, J., & Braithwaite, R. S. (2024). Reducing overdose deaths among persons with opioid use disorder in Connecticut.Harm Reduction Journal, 21(103). doi: 10.1186/s12954-024-01026-6.
Overdose death rates continue to be high throughout the United States. Of the 107,543 drug overdoses that were estimated to occur in 2023, 75% involved opioids. Preliminary data suggests downward trends in drug overdose death rates for the first time since 2018. Though more data are needed to determine whether this encouraging data point is indeed a trend, and to what degree some of these benefits may be due to harm reduction strategies, more work is needed to understand which strategies are best, in which contexts, and at what cost.
Distribution of the opioid overdose-reversal medication naloxone is a cost-effective strategy for overdose death prevention and prior research suggests scaling it up with more precision (i.e., in overdose “hotspots”) in the community might help to further reduce overdose death rates, warranting additional research. Medication treatments for opioid use disorder (buprenorphine, methadone, naltrexone) are also extremely useful in preventing overdose, and thus, also preventing death. Individuals with opioid use disorder are at increased risk of overdose and medication treatment can help reduce that risk. While studies have modeled the cost effectiveness of these overdose death prevention strategies, it is unclear to what extent stakeholders should be investing in each of these strategies and their combinations to maximally benefit individuals with opioid use disorder and decrease overdose death rates.
Determining the effects of these strategies on overdose death rates is essential to inform policy efforts in specific areas of the US that more adequately address overdose deaths and better tackle the opioid epidemic. This study used machine-learning models to evaluate individual and combined overdose-death prevention strategies on overdose death rates in the state of Connecticut, which has one of the highest overdose rates in the US.
HOW WAS THIS STUDY CONDUCTED?
This study used a machine-learning model to estimate the effects of overdose prevention strategies on overdose death rates in the state of Connecticut. One-hundred thousand simulated cases representative of the Connecticut population with opioid use disorder were included in the analysis.
Prevention strategies modeled included increasing distribution/access to (1) naloxone in the general community, (2) medication treatments for opioid use disorder among people in the general community, (3) medication treatments among people who are incarcerated. The researchers examined the 5-year impact of each policy, individually and in combination, on life expectancy, years with good quality health (called quality-adjusted life years, or QALYs – pronounced “quallies’), percentage/number of opioid overdose deaths prevented over a 5-year period and over the simulated cohort’s lifetime. Cost-effectiveness of each policy was also evaluated. Medication treatment included 4 medication types: (1) methadone, (2) oral buprenorphine (active ingredient in the brand-name medication Suboxone), (3) injectable extended-release buprenorphine (sometimes referred to by the brand name Sublocade), (4) injectable extended-release naltrexone (sometimes referred to by the brand name Vivitrol). Transitions on/off these medications were modeled using data that were medication specific.
Values entered into the model were based on data from studies in the scientific literature, expert opinion, and community organizations. As part of the virtual lifecycle, each simulated individual could transition between incarceration and the community and could fluctuate in their opioid use disorder status and treatment status. They could also experience a fatal or non-fatal overdose, and/or die from other causes. The researchers took sex, age, opioid use disorder status (current vs. remission), incarceration status, medication treatment status, and injection behaviors into consideration in their simulated models. Individuals in the model who received medication treatment during incarceration were all assumed to be in remission. Upon release from incarceration, modeled individuals could transition between 3 conditions: 1) receiving medication treatment (in remission and not in remission), 2) not receiving medication treatment and not in remission (assumed actively using illicit opioids), 3) not receiving medication treatment and in remission (assumed abstinent from illicit opioids). It was assumed that models with greater availability of medication treatment would result in greater prevalence of MOUD use among the simulated cohort. Fatal and non-fatal overdoses were possible among simulated individuals who used illicit opioids, with or without medication treatment. The model also assumed that increased naltrexone distribution in the community did not affect overdose rates but did reduce the risk of overdose deaths. Simulated individuals were able to shift between incarceration and the community and could have died from causes un-related to opioids in both environments.
To assess cost-effectiveness of different policies, the authors calculated incremental cost-effectiveness ratio – which is the change in cost of implementing a given policy, divided by the increase in beneficial outcomes from that policy (increase is relative to the next best policy), analyzed as costs per quality-adjusted life years. Costs were assessed from a healthcare perspective and from a societal perspective, and included costs associated with: (1) medication treatment; (2) naloxone; (3) community-based overdose services (e.g., emergency department); (4) incarceration and healthcare costs from a public-payor perspective; (5) crime and loss of productivity from incarceration and lack of treatment, from a societal perspective.
To study the effects of policy combinations, 3 scenarios were tested: (1) maximizing medication treatment during incarceration: all incarcerated people with opioid use disorder receive medication treatment regardless of whether or not they received it before incarceration; (2) maximizing medication treatment in the community: nearly all people with opioid use disorder in the general community (80%) receive medication treatment; (3) maximizing naloxone in the community: all individuals with opioid use disorder in the general community receive naloxone kits a minimum of once per year.
At the start of the study, the simulated sample was made up of adults (age 20 and older), with 14% previously incarcerated and 31% having a past overdose experience. About 4% of the simulated cohort had engaged in injection drug use.
WHAT DID THIS STUDY FIND?
Without a change, over 4,000 overdose deaths would occur every 5 years
If overdose prevention strategies in Connecticut were held constant at their current level, individuals in the simulated cohort would live an average of 33 additional years, with an accumulation of 26 quality-adjusted life years. Overdose deaths would occur at a rate of 4711 deaths over 5 years and 11,655 deaths during the entire study cohort’s lifetime.
Maximizing naloxone distribution would reduce overdose deaths by 20%
Distributing naloxone to all individuals with opioid use disorder at least once per year would reduce overdose death rates to 3744 deaths over 5 years (see Figure below). The simulated cohort would live an additional 0.4 life years, and 0.3 quality adjusted life years, over and above the years gained with no policy changes. The cost of maximizing naloxone distribution, taking the policy’s benefits into account, would be an additional $9000 spent per each quality adjusted life year gained.
Maximizing medication provision would reduce overdose deaths by about 10%
Providing medication treatment to nearly all people with opioid use disorder in the general community would reduce overdose death rates to 4029 deaths over 5 years (see Figure below). If all incarcerated people with opioid use disorder received medication treatment, overdose death rates would reduce to 4439 deaths over 5 years. The simulated community cohort would live an additional 1.5 life years (1.8 quality adjusted life years), and the incarcerated cohort would live an additional 0.2 life years (0.2 quality adjusted life years), over and above the years gained with no policy changes. The cost of maximizing medication treatment access in the community and during incarceration would be an additional $19,000 and $37,000 per quality adjusted life year, respectively.
Combining naloxone and medication treatment strategies was the most cost-effective option
Combining maximization strategies for community-based naloxone distribution and community-based medication treatment provision emerged as the best model when focusing on healthcare costs (see Figure below). This model would reduce overdose deaths by 32% (to 3193 deaths over 5 years). The simulated cohort would live an additional 1.8 life years (2.0 quality adjusted life years) over and above the years gained with no policy changes and would cost an additional $19,000 per each quality adjusted life year gained. From a societal perspective, this model saved society $333,000 per capita. Sensitivity analyses also suggested that this would be a cost-effective model even when varying important factors in the model (e.g., prior overdose or incarceration rates).
Combining all 3 maximization strategies (including incarceration-based medication treatment) resulted in 33% reduction of overdose death rates. This strategy was not considered as cost effective from the healthcare perspective (costing about $75,000 more than combining community strategies without incarceration strategies), but it was considered the best model when cost was assessed from a societal perspective, saving society $338,000 per capita.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help inform policies and strategies to address opioid overdose epidemic. This study, which focused on “best case scenario” strategies in the state of Connecticut, suggests that expanding and maximizing access to community-based medication treatment and naloxone distribution could prevent a third of overdose deaths over a 5-year period, and could result in 2 additional years of life expectancy per person. Such efforts would be cost effective from a healthcare perspective, costing only an additional $19,000 per adjusted life years gained, and from a societal perspective, saving society over $300,000 per capita in increased productivity and reduced crime.
One unsurprising but important note mentioned by the research team was that reduced death rates were largest among persons who inject drugs, highlighting the potential benefits of targeted naloxone distribution for individuals at increased risk of overdose, such as distribution through harm reduction programs. Nonetheless, few states have naloxone access that is broad enough to adequately achieve overdose death prevention. Additional investigation into the best venues for targeted and broad distribution of naloxone will help inform expanded access efforts.
Though the provision of medication treatment during incarceration reduced overdose deaths by 6% when assessed on its own, adding this strategy to those aimed at maximizing community medication treatment and naloxone provision did not substantially increase the overdose death rate (32% vs. 33%) and cost the healthcare system significantly more money. Yet, from a societal perspective the combination of all three strategies yielded the greatest cost savings, saving money through the prevention of crime and increased productivity. Developing and testing novel models of medication treatment for incarcerated individuals may be warranted to identify ways to reduce associated healthcare-related costs while maintaining high rates of overdose prevention. While this study only examined combinations of naloxone and medication treatment, future work may follow the lead of other computer-simulated studies that test even more combinations of strategies, including for example, recovery support services and fentanyl test strips.
Interestingly, maximizing the provision of naloxone alone was more effective at reducing overdose deaths than maximizing the provision of medication treatment alone. Though this may seem counterintuitive to what we hear about the benefits of medication treatment, it is important to remember that medication treatment can help reduce overdose risk but the most commonly used medication treatments like buprenorphine and methadone do not entirely prevent overdose and cannot reverse an overdose. To reverse an overdose, naloxone, the opioid overdose reversal drug, is needed. Still, studies examining patient-level effects of medication treatment provision suggest that medication treatment reduces drug-related deaths by ~60%. The reasons for discrepant findings here likely have to do with the methods (simulated models vs. patient data) and the focus of the studies, with this study focusing on population-level effects as opposed to patient-level effects. Other simulated research focused on population-level outcomes have found similar results, with naloxone emerging as the most effective strategy for overdose death prevention. Yet, findings are mixed, likely due to the various assumptions that go into a given simulated model. Real world data focusing on both individual and population level effects of overdose-death prevention strategies will help to clarify their individual and combined effects under different circumstances and with different sub-populations.
That said, additional research is needed to better understand the relationship between access to these strategies and uptake or use of these strategies among populations with opioid use disorder. If few people are willing to take medication treatment or carry naloxone, then efforts to expand access to these lifesaving strategies will not be maximally effective. Indeed, up to 87% of people with opioid use disorder in the US who would benefit from medication treatment do not receive it. Though barriers to treatment access (limited provider availability, financial & logistical barriers) contribute to inadequate treatment uptake, negative perceptions of medication treatment can also influence willingness to start medication treatment. Therefore, additional research examining attitudes toward medication treatment and initiatives to combat the influence of stigma on medication treatment will further inform efforts to address the opioid epidemic.
This study used a simulated model to estimate the outcomes of potential efforts to expand opioid use disorder treatment and overdose resources, warranting additional real-world research.
Maximal provision assumes that everyone in the model received the treatment or naloxone kit. This requires additional research, as a number of people may decline intervention efforts, including naloxone and medication treatment.
This study used model parameters that reflect a time when higher potency opioids like fentanyl and their use with sedatives like xylazine were not common, which might mute the theoretical benefits on overdose outcomes observed here.
The study only examined combinations of naloxone and medication treatment. Other computer-simulated studies like this one that included other approaches, such as recovery support services and fentanyl test strips, have shown these strategies to be life-saving as well.
BOTTOM LINE
Results from this Connecticut-based study show one-third of overdose deaths can be prevented by providing community-based medication treatment and naloxone distribution to nearly all individuals with opioid use disorder. Combined provision of these “best case scenario” strategies was cost effective from both healthcare and societal perspectives.
For individuals and families seeking recovery: Medication treatments for opioid use disorder and naloxone help prevent and reverse opioid overdose, and these often lifesaving medications are a good option for people who are looking to support their treatment and recovery goals. Individuals and families interested in these strategies are encouraged to speak with their healthcare providers about their treatment options to learn if these medications are right for them. Many states also now sell naloxone over the counter.
For treatment professionals and treatment systems: This study helps us better understand the influence of various policies/strategies for reducing opioid overdose deaths, which could ultimately help inform best methods for adequately addressing the opioid epidemic. Findings highlight the potential for the widespread community provision of opioid use disorder medication treatments and naloxone to prevent up to one-third of overdose deaths among individuals with opioid use disorder. Given the benefits and cost effectiveness of providing these services, providers are encouraged to provide naloxone to all patients with opioid use disorder and to consider increased provision of medication treatments like buprenorphine and extended-release naltrexone to better address the opioid overdose epidemic.
For scientists: Additional research is needed to examine the real-world longitudinal effects of medication treatment and naloxone provision, both in the community and among incarcerated individuals, on overdose death rates throughout different regions and patient populations in the US. Studies examining treatment attitudes, patient preferences, and barriers to treatment (e.g., financial, geographic) are needed to determine the influence of these factors on overdose, as well as other outcomes like recovery capital and quality of life. The influence of maximizing access to different types of medication treatments is also needed to identify potential differences in the impact of the breadth of treatment, recovery, and harm reduction services on community and individual patient outcomes. Future studies should also examine the influence of overdose and service-use histories, patient motivation for treatment/recovery, and additional treatment (public vs. private) and patient-level factors (e.g., change in mental/physical health symptoms) on study outcomes.
For policy makers: Studies like this help inform policies and strategies aimed at overcoming the opioid overdose epidemic. Leveraging existing strategies like the provision of medication treatment (e.g., buprenorphine) and naloxone, and scaling up the availability of these lifesaving medications in the community is likely to help prevent a substantial number of overdose deaths in a cost-effective and even cost-saving manner. Given that this study was a simulated study using a machine-learning model, additional funds are needed to study the direct real-world effects of expanding medication treatment and naloxone provision on overdose death risk and prevalence, accounting for patient, treatment, and community level factors not assessed in the current study.
CITATIONS
Scheidell, J. D., Townsend, T. N., Zhou, Q., Manandhar-Sasaki, P., Rodriguez-Santana, R., Jenkins, M., Buchelli, M., Charles, D. L., Frechette, J. M., I-Shin Su, J., & Braithwaite, R. S. (2024). Reducing overdose deaths among persons with opioid use disorder in Connecticut.Harm Reduction Journal, 21(103). doi: 10.1186/s12954-024-01026-6.